1. Introduction
Climate change is a concept that is well-known and well-researched across the world, especially in high-income countries such as the United States [
1,
2]. However, climate change literacy rates vary substantially across the world. In low- and middle-income countries (LMICs), climate literacy rates tend to be much lower compared with high-income nations [
3,
4]. In a 2015 study published in Nature Climate Change, which assessed the results of a 2007–2008 World Gallup poll, participants across 119 countries were asked about their knowledge of global warming or climate change [
3,
4]. This study found that participants from high-income countries were more likely to say they were aware of climate change, with awareness rates of over 90% across North America and Europe [
3]. Conversely, many LMICs had climate change awareness rates of 50% or below [
3]. In Africa, LMICs like Tunisia and Mozambique have climate literacy rates as low as 23% and 25%, respectively [
5].
Although inadequate in several parts of the world, climate change literacy is important for several reasons. Widespread climate education is essential to help the general population better understand and relate to climate change issues and can allow them to make better-informed personal and community health decisions to reduce their climate impact and undertake adaptive behaviors [
6,
7]. Improved knowledge of climate change and the associated consequences is also an important driver for the successful implementation of individual pro-climatic behaviors, especially among younger populations [
8].
At present, there are little to no assessments on climate change literacy for populations living in LMICs and even less so in the Caribbean. In our prior review [
9], we found a limited number of knowledge, attitude, and practice (KAP) studies in LMICs; only one study focused on climate change literacy in the Caribbean, specifically in Jamaica [
10]. Small-island developing states like those in the Caribbean are increasingly susceptible to changes in temperature and precipitation patterns, paving the way for increases in extreme weather events such as heatwaves, cyclones, tropical storms, droughts, sea level rises, and flooding [
6,
11,
12]. Climate change will not only make these events more frequent, but will also intensify them, causing widespread environmental and human health impacts such as increases in infectious diseases, heat-related morbidity and mortality, flood- and storm-induced infrastructure damage, and water and food scarcity [
11]. Infectious diseases are a particular concern with regards to climate change. Because of increased temperatures and changes in precipitation patterns, vector-borne disease incidence has risen as vector ranges have expanded or vector reproduction has increased [
11]. These concerns are even more evident in the Caribbean region, which has experienced rapid increases in mosquito-borne disease outbreaks (namely, dengue, Zika, and chikungunya) over the past 30 years [
13]. At present, infectious disease literacy is also limited and does not effectively evaluate VBD and climate change interactions, particularly in more affected regions such as the Caribbean [
9].
Our current study aims to rectify the limited availability of current climate change and infectious disease literacy assessments in the Caribbean region through the development of a comprehensive literacy scale evaluating knowledge, attitudes, and behaviors of women currently enrolled in the Caribbean Consortium for Research in Environmental and Occupational Health (CCREOH) cohort [
14] with regards to climate change and infectious disease dynamics in Suriname. Utilizing the expertise obtained from our prior scoping review [
9], we created a scale that covered topics such as food and water availability, droughts and heatwaves, hurricanes and extreme weather events, sea level rises and flooding, mosquito ecology and transmission, preventive actions against mosquito-borne diseases, and government and media influence. Our central goal in the creation of this literacy scale was to provide an effective and generalizable instrument to evaluate current climate change and infectious disease knowledge, attitudes, and behaviors that could be applied across a variety of populations in the Caribbean region. We hope to utilize our findings from this work to strengthen future vector-borne disease interventions at both the individual and community levels.
4. Discussion
The goal of this study was to develop a validated scale of climate change and VBD constructs to adequately assess literacy about these issues among women enrolled in the CCREOH cohort based in Suriname. Our survey instrument utilized five-point Likert scales to evaluate current participant knowledge, attitudes, and behaviors towards climate change and climate–VBD interactions. Our final scale contained both a general climate change section as well as a VBD-specific section and had a total of 20 items that were created through our EFA and CFA results.
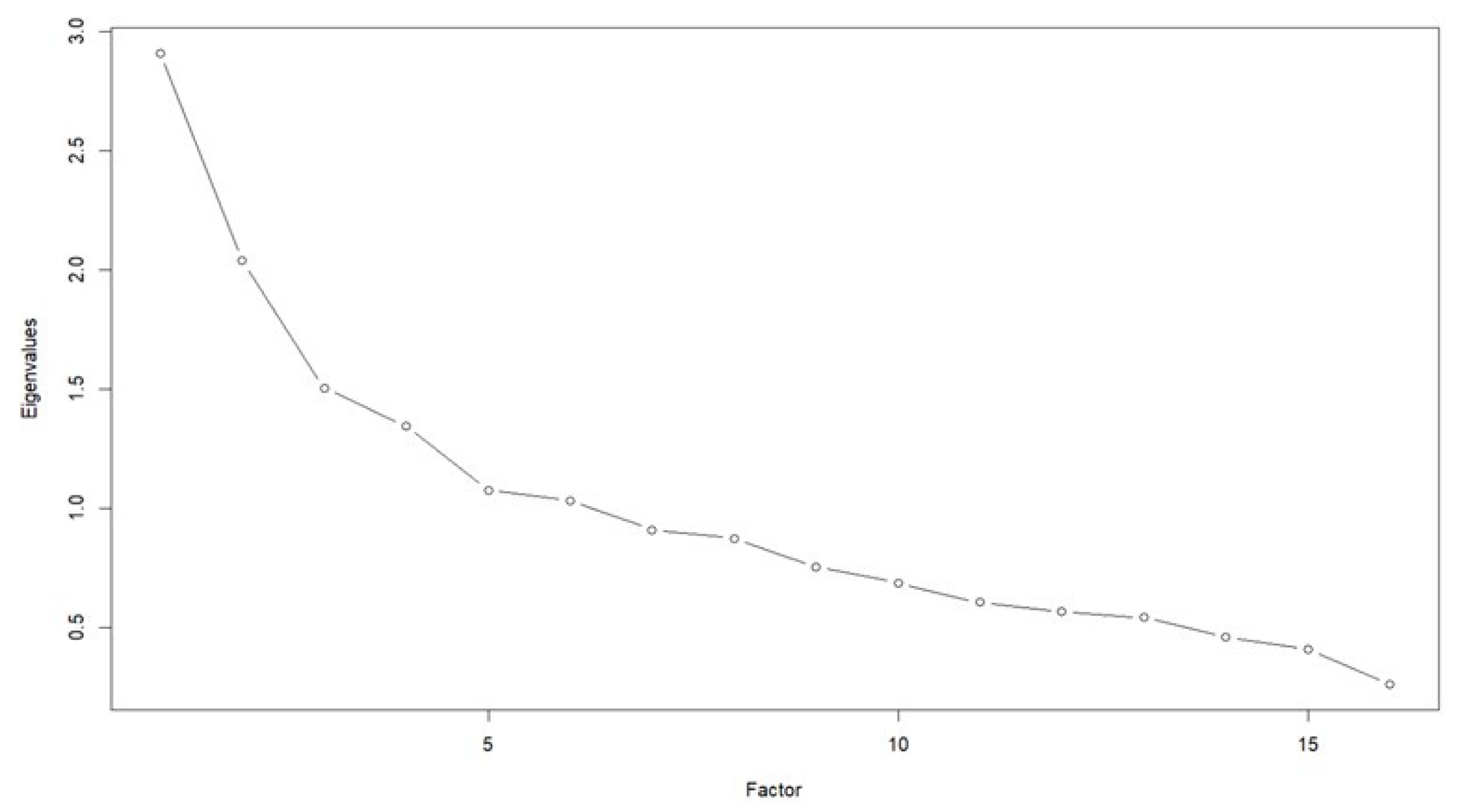
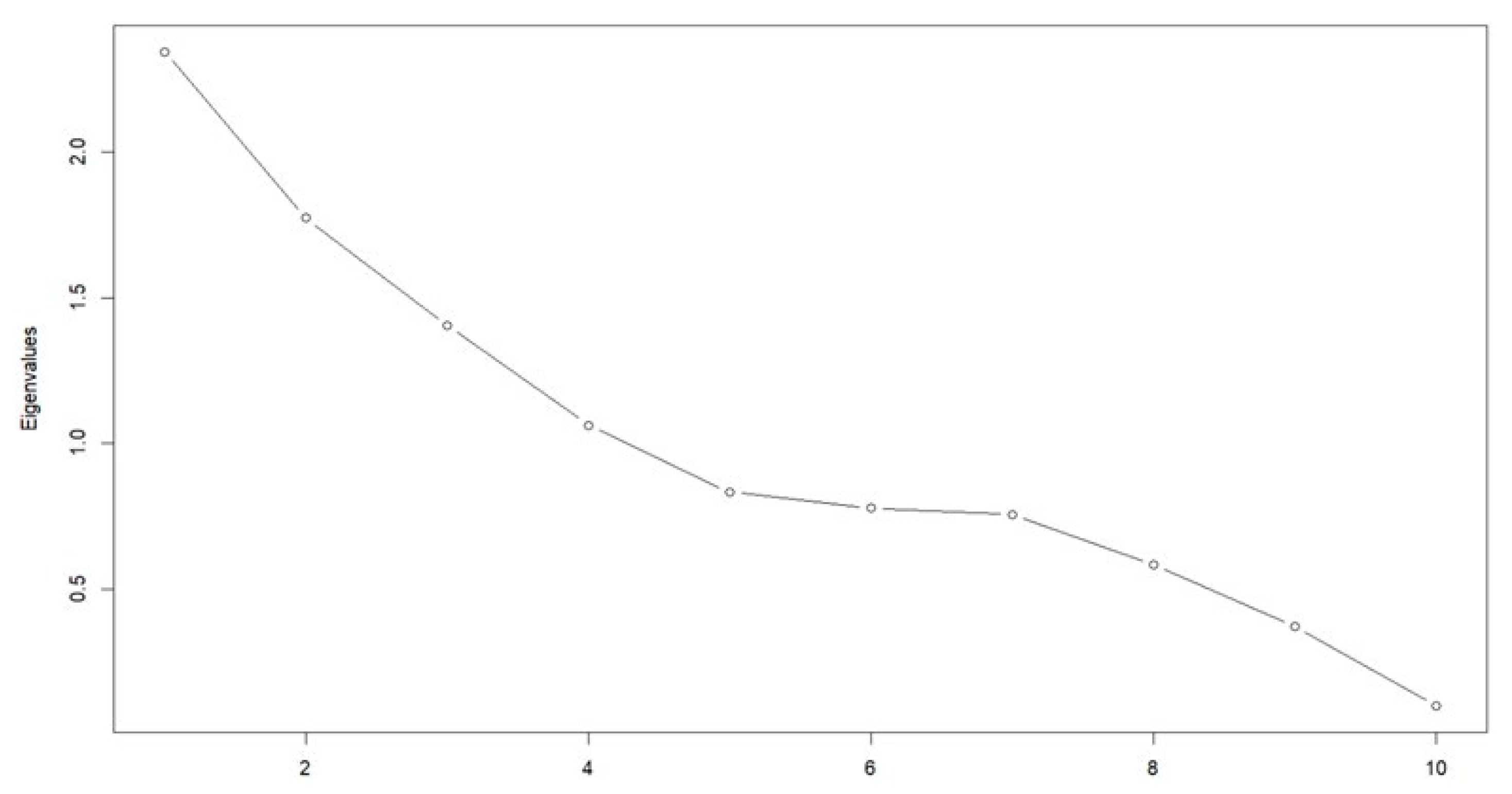
Our 11-item Climate Change Scale described a four-construct solution as follows: general climate change effects, containing three items; heat effects, containing four items; staying indoors/household cooling, containing two items; and ocean warming, containing two items. Together, these factors explained 37.2% of the total variability. Internal reliability was measured using Cronbach’s alpha, which was 0.47 and below our cutoff of 0.7. A calculation of Cronbach’s alpha for individual factors yielded slightly improved results, although our second and third factors still produced alpha values below our 0.7 cutoff. Our nine-item Infectious Disease Scale described a four-construct solution as follows: disease transmission, containing three items; temperature effects, containing two items; viruses, containing two items; and water-holding containers, containing two items. These four factors explained 28.5% of the total variability. Cronbach’s alpha for our Infectious Disease Scale was 0.45, which was also below our cutoff of 0.7. Individual Cronbach’s alpha values for these factors greatly improved, although the alpha value for Factor 1 (disease transmission) was much lower than the overall alpha value calculated. Both scales had otherwise good-fit statistics (
Appendix A,
Table A3) and good absolute model fits (RMSEA = 0.015 for the Climate Change Scale; RMSEA = 0.00 for the Infectious Disease Scale).
In assessing our raw survey data, we found that most participants agreed that climate change was primarily anthropogenic and unavoidable, while approximately 28% of those surveyed were unsure or did not agree that climate change would affect future generations. Preventive measures among this population were also inconsistent. Fewer than half of all participants reported frequently or always staying indoors during heatwaves, although 70.7% affirmed frequently or always keeping their homes as cool as possible during heatwaves. This specific result may have had a higher agreement due to the fact that Suriname has a hot, tropical climate and consistently experiences temperatures between 70 and 90 degrees Fahrenheit [
37,
38], and people are more likely to keep their homes cooled regardless of their level of climate change literacy. There was a high agreement for the two ocean-warming items included (88.1% and 87.7%, respectively, for items 10 and 11 in the Climate Change Scale (
Table 2). Commercial fishing in Suriname is incredibly important for the livelihoods of many individuals as it can provide income through the export of fish and other marine animals such as shrimp [
39]. Previous research has shown that increased ocean temperatures are likely to negatively impact fish populations by reducing reproductive output and thus limiting their ability to successfully repopulate [
40,
41], which poses real problems for both local and commercial fishers.
Our Infectious Disease Scale retained constructs surrounding disease transmission, higher temperatures, viruses, and prolonged water storage. Survey respondents were somewhat aware of the association between temperature and VBDs, with approximately 55% of participants agreeing that warmer temperatures would also increase VBD transmission. The association between precipitation and VBDs was much more pronounced, with over 80% of participants reporting that changes in precipitation would increase VBD transmission. In addition, 81.1% of participants agreed that VBD outbreaks occur more often during rainy seasons. Precipitation projections for Suriname specifically predict less-frequent rainfall but more severe episodes of precipitation over the next several decades [
42]. It is imperative to note that these future episodes are much more likely to increase mosquito habitats in and around water-holding containers. Our respondents tended to already be very aware of these water-storage risks with regards to VBDs as over 75% of the participants surveyed frequently or always removed water from open storage containers and/or removed open storage containers themselves. However, participants were less likely to believe that they personally had increased VBD risks compared with the rest of their community, and most reported seeing no recent change in VBD outbreaks within their areas.
Additional climate change and infectious disease constructs that were evaluated using our survey instrument but not ultimately retained for our final scales included sea level rise, extreme weather, access to food, preventive measures and activities, mosquito ecology, and access to information and media sources. The items that described these constructs (20 of 31 for the Climate Change Scale; 12 of 21 for the Infectious Disease Scale) were all dropped during the EFA. We found that these items either did not load highly (<0.4) onto any factor during our EFA iterations or could not provide an interpretable factor solution. It could be that these concepts were not retained due to poorly worded items or items that may have been too specific in their wording, which was highlighted in the fact that our EFA was unable to identify an underlying KAP structure as expected and thus our scales were instead defined by these narrowly defined constructs, which limited our analyses.
Further exploration of these topics is required, although the scales presented in this study provide a strong pilot tool for researchers. First, the overall small sample size was a limiting factor in our analyses. We estimated that about 300 participants would be required, based on a prior guideline suggesting that 10 participants per item should be included in a scale for factor analysis [
17,
18]. Although we met this criterion overall, we had to split this sample for the exploratory and confirmatory analyses, leaving 180 observations for the EFA and 121 for the CFA. Further, several of our constructs among both scales retained only two items after the EFA, whereas a minimum of three items per factor is recommended for optimal analyses [
31,
32,
33]. An overall larger sample size may have yielded different results and given us a higher number of items retained per scale. Additionally, our current sample only included women as our sample was obtained from CCREOH, an existing maternal and child cohort. Thus, our sample was limited to responses from one specific population and will need to be rectified in future iterations. Our Cronbach’s alpha values for both the Climate Change and Infectious Disease Scales were also lower than expected, with low internal consistency. This could indicate that our scales may have had several items that were less highly interrelated; however, this was considered to be a minor problem when conducting our EFAs and when trying to load items to specific factors. This was mitigated by calculating Cronbach’s alpha values per individual factors. Because of the timeframe, information on some important variables could not be collected and so we could not measure divergent and convergent validity. We were also unable to obtain a three-factor solution based on our initial domains (knowledge, attitudes, and behaviors). The preliminary EFA on the Climate Change Scale gave a solution with three factors but had no high item loadings for ‘behavior’ on any factor and could not be used. Many of the ‘behavior’ items had negative loadings on our factors. We hypothesized that since some of the ‘behavior’ concepts that we included were not widely known or practiced within the community surveyed, this may potentially explain why none of our ‘behavior’ items were able to highly load onto one factor. In particular, ‘behavior’ items pertaining to water-saving strategies, emergency preparedness, and mosquito intervention methods were the items most likely to have very low practice rates. A cultural adaptation of the literacy scale is likely to resolve these challenges.
Through the development and implementation of these scales, we noted that climate change and infectious disease literacy, in particular with regards to prevention measures and the dissemination of information, is deficient in LMICs such as Suriname. Our survey data indicated that at least half of the respondents were aware that climate change played a role in infectious disease transmission and were able to associate temperature and precipitation with increased VBDs but did not know exactly how they were spread. We also noted that many participants reported rarely or never participating in basic safety measures to reduce VBD risk, although they agreed that climate change was directly linked to VBD transmission. It is abundantly clear that climate change and VBD literacy should be a more pertinent issue for vulnerable populations as nearly all women in our study population agreed that greater climate change and infectious disease education was needed in their communities (99.7% and 98%, respectively).
Very few climate change and VBD literacy studies have focused their efforts in the Caribbean. We noted from our prior review that the only climate change literacy survey we found that was conducted in the Caribbean came from Jamaica and was very specific to that country [
10]. For this reason, we focused our initial efforts on Suriname, with plans to expand our efforts into other Caribbean and South American countries as well as parts of the southern United States. These areas are some of the most affected by climate change and VBDs [
43]. Evident changes in the response to climate change in areas of the Caribbean include more intense weather and precipitation patterns, more droughts, more frequent temperature extremes, and increases in sea levels [
43]. These changes, if left unmitigated, will very likely continue to impact VBDs through longer transmission seasons as well as increased geographical ranges [
44]. In South America specifically, climate suitability for infectious diseases is at an all-time high, with a 35.3% increase in dengue transmission between 2012 and 2021 compared with the 1950–1961 baseline [
45].
The creation of a comprehensive climate literacy scale such as ours that expressly addresses important interactions between climate change effects and vector-borne diseases is important for future global health education; there is currently no standardized climate change literacy scale available to researchers to adequately assess climate change and VBD literacy as related topics. At present, many prior studies focus on either climate change or VBD literacy [
9] but do not necessarily evaluate increased VBD transmission or vector ranges as consequences of climate change, although these issues are highly correlated. Additionally, previous research has trended towards evaluations of climate change literacy among more highly educated groups such as medical students or healthcare workers, but not always among more vulnerable or high-risk populations such as those living in LMICs [
9]. The adaptation of these surveys to the general population will allow us to assess the level of climate change literacy that currently exists within the rest of the population. These scales have the potential to advance climate change and VBD literacy through improving community engagement projects as well as building capacity for climate change and VBD preventive practices in highly vulnerable regions. The scales developed here demonstrate an important step in the advancement of global climate change and VBD literacy not only in the Caribbean, but also in other parts of the world that are also highly affected by climate change and related VBD effects.
Future research includes the cultural adaptation of the scale for implementation in other Caribbean countries such as the Bahamas and Trinidad and Tobago. We also plan to deploy the scale among a larger general population of both men and women in Suriname in order to generate responses from a more representative sample of the population. Lastly, with an entirely female sample, gender differences were not possible to analyze at this point. Sociodemographic outcomes, including gender differences, would be important to assess with the next iteration of scale implementation.



 ,
, 

{kind=link}
{kind=link}