
Housing Insecurity and Other Syndemic Factors Experienced by Black and Latina Cisgender Women in Austin, Texas: A Qualitative Study

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
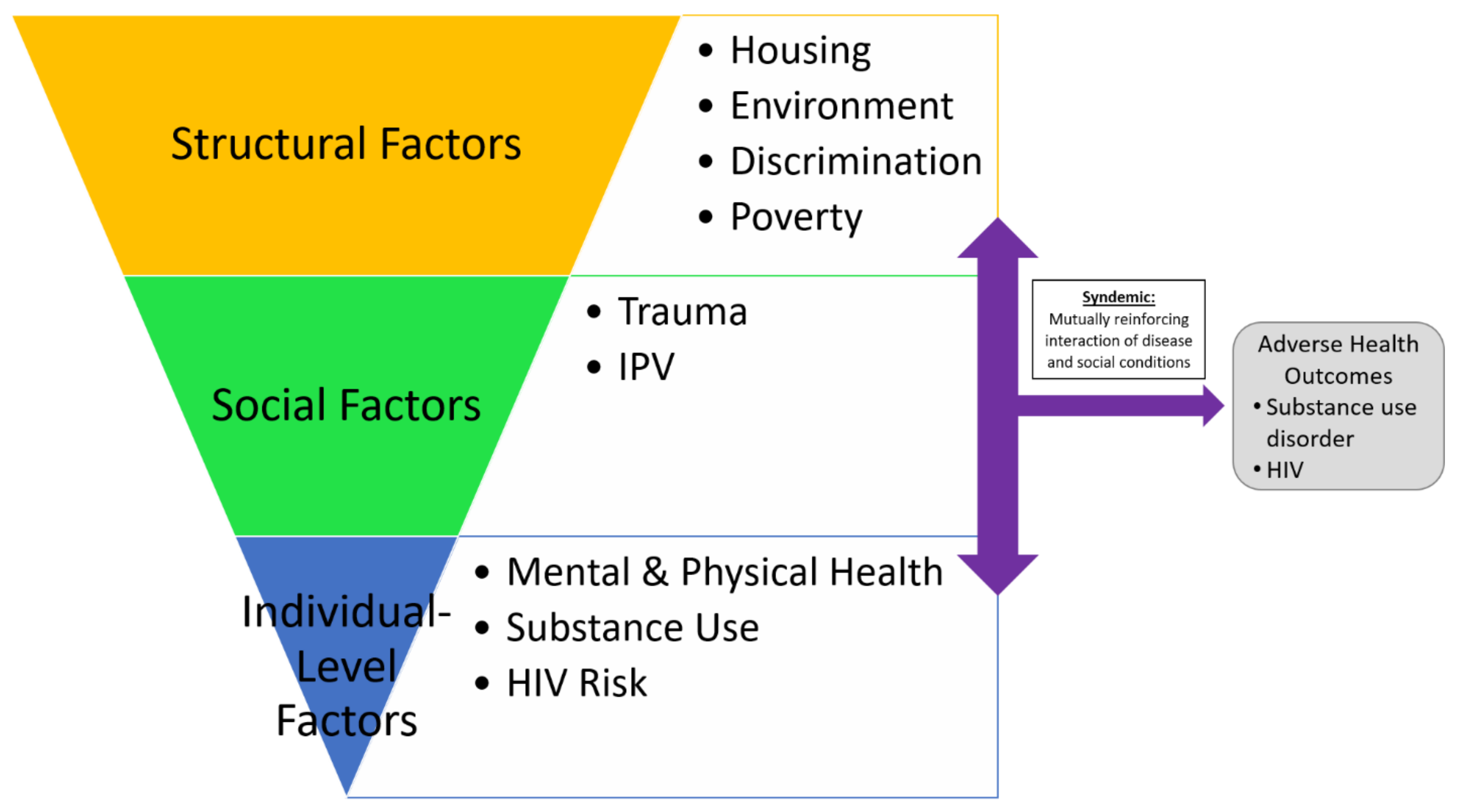
1.1. Syndemic Model
1.2. Study Purpose
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Structural Factors: Housing, Environment, Discrimination, and Poverty
3.1.1. Very Unstable Housing
Cause me and my first son, while I was pregnant, we were homeless and we were sleeping in my car and my car had broke down… After that [family] told me I couldn’t stay with them… [my sister] dropped us off over here [shelter/transitional housing] with all of our bags and stuff.(218, Prior to Interview 1, Very Unstable, 22 yo, Black)
3.1.2. Unstable Housing
Housing should be coming through pretty soon. I applied on different waiting lists and I’m like 50 [on the list]… they made a mistake and they took me off [the list] and put me back on the [bottom] of the list but I got the papers to show that I was already on the list.(212, Interview 1, Unstable, 46 yo, Afro-Latina)
3.1.3. Stable Substandard Housing
At first it was good… It was like a last [minute] temporary thing because we have a voucher you have to hurry up, they give you a certain amount of months to find somewhere to stay before your voucher [expires]… It was all right, and then until recently, people’s cars have been getting broken into, so now I got to watch outside for my car… But it’s like 10 cars got broken into in two weeks. 10 cars.(244, Interview 2, Stable Substandard, 30 yo, Black)
3.1.4. Stable Costly Housing
It’s expensive here and I don’t think it’s worth it, like I don’t. Like if you look at these apartments, if you look at the cabinets and stuff, it’s not worth it. And it’s super small…They’re way overpriced. So, I’ve been really thinking about, once I figure out like a job that I’m secure, I really been thinking about going to [town over 1 h north of Austin] because I’m like for what I’m paying here, I could have a house.(224, Interview 3, Stable Costly, 34 yo, Black)
3.2. Social Factors: IPV and Trauma
3.2.1. Emotional Abuse
It’s like he just try to start stuff, or it’s just like when we go out… So his grandma came up there, because we live on the second floor, she came up there with [boyfriend’s] brother and his uncle. So everyone’s sitting around talking, and every time his uncle and his brother… The dudes in his family, the males, [boyfriend says] “you put your head down”. So I say “hello”. “Oh, you didn’t have your head down”. And it’s like his little brother. I’m like this is your… He’s 22, but I’m like this is your little brother, like come on.(244, Interview 2, Stable Substandard, 30 yo, Black)
3.2.2. Physical IPV
Participant 216: He slapped, he just, he just slapped me. My face hurts. Because he have a heavy hand.
Interviewer: Doesn’t [domestic violence shelter] have an emergency shelter for situations like that?
Participant 216: Yes, but it’s full.(216, Interview 2, Very Unstable, 24 yo, Black)
3.2.3. Sexual IPV
I stayed with ex-boyfriend. I stayed with him. This is why I say I want someone to be respectful, is because I told him, I wanted to come and stay at his place, be friends only and I’ll pay for rent. I’ll find a job and I’ll pay for rent and stuff. If you need help watching your son on days that I’m not working, I can do that. That didn’t happen. I went there. He’s like, “You either be my girlfriend or you get out”. I said, “What the hell?” … I was forced into a relationship that I didn’t want to be in… I had to leave. I got tired of it.(230, Interview 1, Very Unstable, 30 yo, Latina)
3.2.4. Economic IPV
I was financially dependent on him… He was selling drugs and stuff. And doing a lot of stuff he shouldn’t have been doing. He made me lose my job… Because he would call up to my job. He tried to change my life insurance to his name. That’s why I was like, but I still stayed with him so I don’t know. But at that point I felt like he was going to kill me or something.(212, Interview 1, Unstable, 46 yo, Afro-Latina)
3.2.5. Social Isolation
I wasn’t myself. I lost my personality. I lost my bubbliness. I lost everything about me so I was basically like a church mouse in the house. I couldn’t go anywhere. He was controlling. Couldn’t go nowhere. He made me drop out of school the first time. He would take my car so I wouldn’t go anywhere. And if I wouldn’t, like if I would have my car keys he would slice my tires so that I couldn’t go anywhere, yeah it was bad, it was bad.(210, Interview 1, Unstable, 31 yo, Black)
3.3. Individual-Level Factors: Substance Use, Mental and Physical Health, and HIV Risk
3.3.1. Substance Use
I’ve been lately just drinking left and right. I’ve been drinking whatever I can get my hands on. Budweiser, Coronas… I’m drinking when [the kids are] asleep, because I don’t want them to see me… And I’m still getting up and going to work. Which is horrible, because I’m just… I know I’m not supposed to be drinking but it kind of numbs that feeling that I’m dealing with. But it’s not good. It’s not good because it just makes it… numb. And it just makes me stop thinking of him for a while but then reality really sinks in… And kind of let it out and cry and then by the time I find out I’m like, in bed already… Somehow my subconscious knows that I have to get off the couch, that I can’t leave the bottles on the floor because like, the kids… So I find myself waking up the next morning, and the living room’s clean and like, there’s no sign of me drinking. But I know I drank.(235, Interview 2, Stable Substandard, 29 yo, Latina)
I started smoking because my head felt like it was gonna to blow up. And then I went to the hospital. They gave me stuff there but it wore off… Next week, on Wednesday I’m going to call and schedule an appointment [with a psychiatrist] if I can get in this week fine. If I can get in next month I get meds. I’m going to stop smoking again. But until I get meds I’m going to keep smoking.(212, Interview 2, Unstable, 46 yo, Afro-Latina)
Last week I almost had a heart attack. I was on the couch laying down and I felt like pain in my heart. I’m like, “I need to stop”.
No. They put me in a cold shower. [Boyfriend] and his friend put me in a cold shower. Then I blacked out after that I don’t know what happened. Like, [interviewer name], I’m so serious, the last thing I heard from him was “sex stimulation”.
That’s the last thing I heard. I’m like what the fu….then my sister, my sister called my phone and was like “Dude you need to get away from this dude, you really do”. And I’m like, “I don’t know how to”.(216, Interview 3, Very Unstable, 24 yo, Black)
3.3.2. Risk of Acquiring HIV
Yes [I did want to use a condom]… I didn’t ask him, because I knew he didn’t want to… I wasn’t afraid to ask. I just knew he didn’t want to.(218, Interview 3, Unstable, 22 yo, Black)
I’ve had, oh God. I’ve had about maybe three casuals.(228, Interview 1, Very Unstable, 32 yo, Black)
I just stopped answering [partner 1′s] phone call. I got a call blocker for text messages and stuff and then with [partner 2] I just told him at school, like, “Hey, work on your marriage… cause it’s not fair to me. I’m always gonna be a secret. I can’t go in public with you”. I didn’t like that. And then with [partner 3], he was a whore so I don’t think it really phased him that I stopped talking to him. I didn’t even give him a reason. I just walked passed him like I didn’t see him. Granted, both these guys [partners 2 and 3] go to my school.(228, Interview 2, Very Unstable, 32 yo, Black)
[Ex-husband’s] like, “I’m going to try to work things out with you,” and I’m like, okay, let’s see how it works… So that night, I remember we kind of just let it go, I don’t really think much of it… And then [ex-husband says] “I find out that I need to make an appointment because it’s really hurting, it’s being discomfort when I use the restroom”. I got him a doctor’s appointment at the local clinic. He goes in. They test him for STDs. The following day he calls me and tells me, “You know what? I need you to help me go pick up medication,” because he didn’t have a car… I go pick it up, in the back of my head I’m like, “what type of medication did they give him?” I read it. Google what the medication is, and it’s for chlamydia… I go back and the timeline puts him in Mexico. If that’s what it is, it puts him in Mexico, because I had my Pap smear done in early [month] and nothing came back. Nothing came back, so he exposed me to that.(235, Interview 2, Stable Substandard, 29 yo, Latina)
I had this re-evaluation after my [first] interview… I’m like, “You’re very carefree for someone so [sexually] active”.… I was making some really poor decision, like sometimes I wouldn’t use a condom, sometimes I would. I’m just like, “No, if you are STD-free, stay that way”.(228, Interview 2, Very Unstable, 32 yo, Black)
4. Discussion
4.1. Limitations
4.2. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Census Bureau. Annual Estimates of the Resident Population: April 1, 2010 to July 1, 2019 in Austin, Texas. Available online: https://data.census.gov/table/peppop2019.pepannres?g=310xx00us12420 (accessed on 24 October 2023).
- City of Austin. Austin Is Now the 10th Largest City in the U.S. Available online: https://www.austintexas.gov/news/austin-now-10th-largest-city-us (accessed on 24 October 2023).
- Iyanda, A.E.; Lu, Y. ‘Gentrification is not improving my health’: A mixed-method investigation of chronic health conditions in rapidly changing urban neighborhoods in Austin, Texas. J. Hous. Built Environ. 2022, 37, 77–100. [Google Scholar] [CrossRef] [PubMed]
- Kushel, M.B.; Gupta, R.; Gee, L.; Haas, J.S. Housing instability and food insecurity as barriers to health care among low-income Americans. J. Gen. Intern. Med. 2006, 21, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Frederick, T.J.; Chwalek, M.; Hughes, J.; Karabanow, J.; Kidd, S. How stable is stable? Defining and measuring housing stability. J. Community Psychol. 2014, 42, 964–979. [Google Scholar] [CrossRef]
- Macrotrends. Austin Metro Area Population 1950–2023. Available online: https://www.macrotrends.net/cities/22926/austin/population# (accessed on 9 October 2023).
- World Population Review. Austin, Texas Population 2023. Available online: https://worldpopulationreview.com/us-cities/austin-tx-population (accessed on 14 August 2023).
- United States Census Bureau. QuickFacts: Austin City, Texas. Available online: https://www.census.gov/quickfacts/fact/table/austincitytexas/lnd110210 (accessed on 14 August 2023).
- Ending Community Homelessness Coalition. Homelessness in Austin. Available online: https://www.austinecho.org/about-echo/homelessness-in-austin/ (accessed on 23 July 2021).
- Salazar, M. Homelessness in Austin: Current Needs and Gaps Report; Ending Community Homelessness Coalition (ECHO): Austin, TX, USA, 2017; Available online: https://www.thn.org/wp-content/uploads/2017/10/austin-homelessness-needs-and-gaps3-2016.pdf (accessed on 10 July 2017).
- Henry, M.; de Sousa, T.; Roddey, C.; Gayen, S.; Bednar, T.J.; Abt Associates. The 2020 Annual Homeless Assessment Report (AHAR) to Congress; US Department of Housing and Urban Development: Washington, DC, USA, 2021. Available online: https://www.huduser.gov/portal/sites/default/files/pdf/2020-ahar-part-1.pdf (accessed on 28 October 2021).
- Ending Community Homelessness Coalition. Emergency Housing Voucher Program. Available online: https://www.austinecho.org/arpa-ehv/ (accessed on 28 November 2023).
- Travis County. Housing Referral List. Available online: https://www.traviscountytx.gov/health-human-services/cdbg/housing-referral-list (accessed on 28 November 2023).
- Housing Authority of the City of Austin. Housing Choice Voucher Program (Section 8). Available online: https://www.hacanet.org/resident/assisted-housing/#:~:text=read%20more-,how%20the%20hcv%20program%20works,than%206%2c000%20units%20of%20housing (accessed on 28 November 2023).
- Nydegger, L.A.; Kidane, H.; Benitez, S.; Yuan, M.; Claborn, K.R. A qualitative exploration of PrEP interests, barriers, and interventions among Black and Latina cisgender women in the U.S. Arch. Sex. Behav. 2023. [Google Scholar] [CrossRef]
- Nydegger, L.A.; Claborn, K.R. Exploring patterns of substance use among highly vulnerable Black women at-risk for HIV through a syndemics framework: A qualitative study. PLoS ONE 2020, 15, e0236247. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.C. Introduction to Syndemics: A Critical Systems Approach to Public and Community Health; John Wiley and Sons: San Francisco, CA, USA, 2009. [Google Scholar]
- Fedina, L.; Ashwell, L.; Bright, C.; Backes, B.; Newman, M.; Hafner, S.; Rosay, A.B. Racial and gender inequalities in food, housing, and healthcare insecurity associated with intimate partner and sexual violence. J. Interpers. Violence 2022, 37, NP23202–NP23221. [Google Scholar] [CrossRef] [PubMed]
- Fraga Rizo, C.; Klein, L.B.; Chesworth, B.; Macy, R.J.; Dooley, R. Intimate partner violence survivors’ housing needs and preferences: A brief report. J. Interpers. Violence 2022, 37, 958–972. [Google Scholar] [CrossRef]
- Wilson, P.R.; Thorpe, R.J.; Sharps, P.; Laughon, K. The relationship between housing instability and intimate partner violence: A retrospective study. Public Health Nurs. 2021, 38, 32–39. [Google Scholar] [CrossRef]
- Edwards, K.M.; Wheeler, L.; Siller, L.; Murphy, S.B.; Ullman, S.E.; Harvey, R.; Palmer, K.; Lee, K.; Marshall, J. Outcomes associated with participation in a sober living home for women with histories of domestic and sexual violence victimization and substance use disorders. Traumatology 2023, 29, 191–201. [Google Scholar] [CrossRef]
- Nicholls, M.J.; Urada, L.A. Homelessness and polysubstance use: A qualitative study on recovery and treatment access solutions around an urban library in Southern California, USA. Health Soc. Care Community 2022, 30, e175–e193. [Google Scholar] [CrossRef]
- Bowen, E.A.; Mitchell, C.G. Homelessness and residential instability as covariates of HIV risk behavior among residents of single room occupancy housing. J. HIV AIDS Soc. Serv. 2016, 15, 269–283. [Google Scholar] [CrossRef]
- Groves, A.K.; Niccolai, L.M.; Keene, D.E.; Rosenberg, A.; Schlesinger, P.; Blankenship, K.M. Housing instability and HIV risk: Expanding our understanding of the impact of eviction and other landlord-related forced moves. AIDS Behav. 2021, 25, 1913–1922. [Google Scholar] [CrossRef]
- Santa Maria, D.; Hernandez, D.; Arlinghaus, K.; Gallardo, K.; Maness, S.; Kendzor, D.; Reitzel, L.; Businelle, M. Current age, age at first sex, age at first homelessness, and HIV risk perceptions predict sexual risk behaviors among sexually active homeless adults. Int. J. Environ. Res. Public Health 2018, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.L.; Rhoades, H.; Harris, T.; Winetrobe, H.; Rice, E.; Henwood, B. Risk behavior and access to HIV/AIDS prevention services in a community sample of homeless persons entering permanent supportive housing. AIDS Care 2017, 29, 570–574. [Google Scholar] [CrossRef]
- Moses, J.; Janosko, J.; Homelessness Research Institute. Demographic Data Project Part II: Gender and Individual Homelessness; National Alliance to End Homelessness: Washington, DC, USA, 2019; Available online: https://endhomelessness.org/wp-content/uploads/2019/09/ddp-gender-brief-09272019-byline-single-pages.pdf (accessed on 28 November 2023).
- National Health Care for the Homeless Council. Homelessness & Health: What’s the Connection? 2019. Available online: https://nhchc.org/wp-content/uploads/2019/08/homelessness-and-health.pdf (accessed on 28 November 2023).
- Straus, M.A.; Douglas, E.M. A short form of the Revised Conflict Tactics Scales, and typologies for severity and mutuality. Violence Vict. 2004, 19, 507–520. [Google Scholar] [CrossRef]
- Lehmann, P.; Simmons, C.A.; Pillai, V.K. The validation of the Checklist of Controlling Behaviors (CCB): Assessing coercive control in abusive relationships. Violence Against Women 2012, 18, 913–933. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Drug Abuse. Seek, Test, Treat and Retain for Vulnerable Populations: Data Harmonization Measure: HIV Risk Behaviors; National Institute on Drug Abuse: Rockville, MD, USA, 2013. Available online: http://www.drugabuse.gov/sites/default/files/sttrfiles/hivriskbehaviorsvp.pdf (accessed on 30 September 2015).
- Johnson, M.E.; Fisher, D.G.; Montoya, I.; Booth, R.; Rhodes, F.; Andersen, M.; Zhuo, Z.; Williams, M. Reliability and validity of not-in-treatment drug users’ follow-up self-reports. AIDS Behav. 2000, 4, 373–380. [Google Scholar] [CrossRef]
- National Institute on Alcohol Abuse and Alcoholism. Drinking Levels Defined. Available online: http://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (accessed on 9 October 2015).
- Konstantopoulos, W.L.M.; Dreifuss, J.A.; McDermott, K.A.; Parry, B.A.; Howell, M.L.; Mander, R.N.; Fitzmaurice, G.M.; Bogenschutz, M.P.; Weiss, R.D. Identifying patients with problematic drug use in the emergency department: Results of a multisite study. Ann. Emerg. Med. 2014, 64, 15–19. [Google Scholar] [CrossRef]
- Johnson, M.E.; Pratt, D.K.; Neal, D.B.; Fisher, D.G. Drug users’ test-retest reliability of self-reported alcohol use on the risk behavior assessment. Subst. Use Misuse 2010, 45, 925–935. [Google Scholar] [CrossRef]
- McDaniel, G.; Akinwunmi, S.; Brenya, V.; Kidane, H.; Nydegger, L.A. Superwoman schema: Uncovering repercussions of coping strategies used among Black women at high risk for HIV. Ethn. Health 2023, 28, 874–894. [Google Scholar] [CrossRef]
- Nydegger, L.A.; Dickson-Gomez, J.; Ko Ko, T. A longitudinal, qualitative exploration of perceived HIV risk, healthcare experiences, and social support as facilitators and barriers to PrEP adoption among Black women. AIDS Behav 2021, 25, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Nydegger, L.A.; Dickson-Gomez, J.; Ko Ko, T. Structural and syndemic barriers to PrEP adoption among Black women at high risk for HIV: A qualitative exploration. Cult. Health Sex. 2021, 23, 659–673. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- National Domestic Violence Hotline. What Is Emotional Abuse? Available online: https://www.thehotline.org/resources/what-is-emotional-abuse/ (accessed on 11 September 2023).
- National Domestic Violence Hotline. What Is Gaslighting? Available online: https://www.thehotline.org/resources/what-is-gaslighting/ (accessed on 11 September 2023).
- Centers for Disease Control and Prevention. What Is Intimate Partner Violence? Available online: https://www.cdc.gov/violenceprevention/intimatepartnerviolence/fastfact.html (accessed on 11 September 2023).
- Johnson, L.; Chen, Y.; Stylianou, A.; Arnold, A. Examining the impact of economic abuse on survivors of intimate partner violence: A scoping review. BMC Public Health 2022, 22, 1014. [Google Scholar] [CrossRef] [PubMed]
- National Domestic Violence Hotline. Power and Control. Available online: https://www.thehotline.org/identify-abuse/power-and-control/ (accessed on 11 September 2023).
- National Institute on Alcohol Abuse and Alcoholism. Rethinking Drinking: Alcohol and Your Health; National Institutes of Health: Rockville, MD, USA, 2022. Available online: https://www.niaaa.nih.gov/sites/default/files/publications/niaaa_rethinkingdrinking.pdf (accessed on 9 October 2023).
- Substance Abuse and Mental Health Services. Key Substance Use and Mental Health Indicators in the United States: Results from the 2021 National Survey on Drug Use and Health; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2022. Available online: https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report (accessed on 29 September 2023).
- National Alliance to End Homelessness. Racial Disparities in Homelessness Persist: A Data Snapshot. 2023. Available online: https://endhomelessness.org/resource/racial-disparities-in-homelessness-persist-a-data-snapshot/ (accessed on 7 December 2023).
- Chinchilla, M.; Moses, J.; Visotzky, A.; National Alliance to End Homelessness. Increasing Latino Homelessness—What’s Happening, Why, and What to Do About It. Available online: https://endhomelessness.org/wp-content/uploads/2023/01/latino-homelessness_researchbrief_01242023_final.pdf (accessed on 7 December 2023).
- National Alliance to End Homelessness. Children and Families. 2023. Available online: https://endhomelessness.org/homelessness-in-america/who-experiences-homelessness/children-and-families/ (accessed on 7 December 2023).
- Hepburn, P.; Louis, R.; Desmond, M. Racial and gender disparities among evicted Americans. Sociol. Sci. 2020, 7, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Bullock, H.E.; Reppond, H.A.; Truon, S.V.; Singh, M.R. An intersectional analysis of the feminization of homelessness and mothers’ housing precarity. J. Soc. Issues 2020, 76, 835–858. [Google Scholar] [CrossRef]
- City of Austin. Strategic Housing Blueprint. 2023. Available online: https://www.austintexas.gov/sites/default/files/files/Blueprint_Overview.pdf (accessed on 23 November 2023).
- City of Austin. Displacement Mitigation Strategy. In Austin Strategic Housing Blueprint Implementation; City of Austin: Austin, TX, USA, 2023; pp. 57–69. Available online: https://www.austintexas.gov/sites/default/files/files/housing/displacement_mitigation_strategy_blueprint_chapter__002_.pdf (accessed on 28 November 2023).
- Project Transitions. Supportive Housing. Available online: https://www.projecttransitions.org/housing (accessed on 27 November 2023).
- Peitzmeier, S.M.; Fedina, L.; Ashwell, L.; Herrenkohl, T.I.; Tolman, R. Increases in intimate partner violence during COVID-19: Prevalence and correlates. J. Interpers. Violence 2022, 37, NP20482–NP20512. [Google Scholar] [CrossRef]
- Pavao, J.; Alvarez, J.; Baumrind, N.; Induni, M.; Kimerling, R. Intimate partner violence and housing instability. Am. J. Prev. Med. 2007, 32, 143–146. [Google Scholar] [CrossRef]
- Klein, L.B.; Chesworth, B.R.; Howland-Myers, J.R.; Rizo, C.F.; Macy, R.J. Housing interventions for intimate partner violence survivors: A systematic review. Trauma Violence Abus. 2021, 22, 249–264. [Google Scholar] [CrossRef]
- Willie, T.C.; Linton, S.L.; Whittaker, S.; Martinez, I.; Sharpless, L.; Kershaw, T. “There’s no place like home”: Examining the associations between state eviction defense protections and indicators of biopsychosocial stress among survivors of intimate partner violence. Soc. Sci. Med. 2021, 279, 113957. [Google Scholar] [CrossRef]
- Breiding, M.J.; Basile, K.C.; Klevens, J.; Smith, S.G. Economic insecurity and intimate partner and sexual violence victimization. Am. J. Prev. Med. 2017, 53, 457–464. [Google Scholar] [CrossRef]
- O’Campo, P.; Daoud, N.; Hamilton-Wright, S.; Dunn, J. Conceptualizing housing instability: Experiences with material and psychological instability among women living with partner violence. Hous. Stud. 2016, 31, 1–19. [Google Scholar] [CrossRef]
- Manning, W.D.; Longmore, M.A.; Giordano, P.C. Cohabitation and intimate partner violence during emerging adulthood: High constraints and low commitment. J. Fam. Issues 2018, 39, 1030–1055. [Google Scholar] [CrossRef] [PubMed]
- Jewkes, R. Intimate partner violence: Causes and prevention. Lancet 2002, 359, 1423–1429. [Google Scholar] [CrossRef]
- North, C.S.; Eyrich-Garg, K.M.; Pollio, D.E.; Thirthalli, J. A prospective study of substance use and housing stability in a homeless population. Soc. Psychiatr. Epidemiol. 2010, 45, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.R.; Anthony, N.; Quesinberry, D.; Delcher, C. Evidence of housing instability identified by addresses, clinical notes, and diagnostic codes in a real-world population with substance use disorders. J. Clin. Trans. Sci. 2023, 7, e196. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Wood, E.; Nguyen, P.; Kerr, T.; DeBeck, K. Increases and decreases in drug use attributed to housing status among street-involved youth in a Canadian setting. Harm Reduct. J. 2014, 11, 12. [Google Scholar] [CrossRef]
- Johnson, T.P.; Freels, S.A.; Parsons, J.A.; Vangeest, J.B. Substance abuse and homelessness: Social selection or social adaptation? Addiction 1997, 92, 437–445. [Google Scholar] [CrossRef]
- Johnson, G.; Chamberlain, C. Homelessness and substance abuse: Which comes first? Aust. Soc. Work. 2008, 61, 342–356. [Google Scholar] [CrossRef]
- Gibbs, K.D.; Jones, J.T.; LaMark, W.; Abdulmooti, S.; Bretz, L.; Kearney, K.D.; Narendorf, S.C.; Santa Maria, D.M. Coping during the COVID-19 pandemic among young adults experiencing homelessness and unstable housing: A qualitative study. Public Health Nurs. 2023, 40, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.P.; Hunter, S.B.; Osilla, K.C.; Maksabedian, E.; Golinelli, D.; Tucker, J.S. A computer-assisted motivational social network intervention to reduce alcohol, drug and HIV risk behaviors among housing first residents. Addict. Sci. Clin. Pract. 2016, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Dickson-Gomez, J.; McAuliffe, T.; Quinn, K. The effects of housing status, stability and the social contexts of housing on drug and sexual risk behaviors. AIDS Behav. 2017, 21, 2079–2092. [Google Scholar] [CrossRef] [PubMed]
- Willie, T.; Linton, S.; Whittaker, S.; Phillips, K.; Knight, D.; Gray, M.; Gardner, G.; Overstreet, N. Housing insecurity among Black women surviving intimate partner violence during the COVID-19 pandemic: An intersectional qualitative approach. Res. Sq. 2023, rs.3.rs-2662616. [Google Scholar] [CrossRef]
- Walsh, C.A.; Lorenzetti, L.; St-Denis, N.; Murwisi, P.; Lewis, T.R. Community voices: Insights on social and human services from people with lived experiences of homelessness. Rev. Soc. Sci. 2016, 1, 27–41. [Google Scholar] [CrossRef][Green Version]
- Office of Disease Prevention and Health Promotion. Housing Instability. 2020. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health/literature-summaries/housing-instability (accessed on 10 December 2023).
- Pagaduan, J.; National Alliance to End Homelessness. Millions of Americans are Housing Insecure: Rent Relief and Eviction Assistance Continue to be Critical. 2021. Available online: https://endhomelessness.org/resource/housing-insecurity-rent-relief-eviction-assistance/ (accessed on 10 December 2023).



{kind=link}
{kind=link}
| Variable | Total (n = 18) | Previous (n = 18) | T1 (n = 18) | T2 (n = 15) | T3 (n = 14) | |
|---|---|---|---|---|---|---|
| Age (years) (M (SD)) | 31.8 (7.55) | - | - | - | - | |
| Number of children (M (SD)) | 2.92 (1.44) | - | - | - | - | |
| Race/ethnicity | ||||||
| Black/African American | 10 (55.56) | - | - | - | - | |
| Latina/Hispanic | 6 (33.33) | - | - | - | - | |
| Afro-Latina a | 2 (11.11) | - | - | - | - | |
| Housing experiences b | ||||||
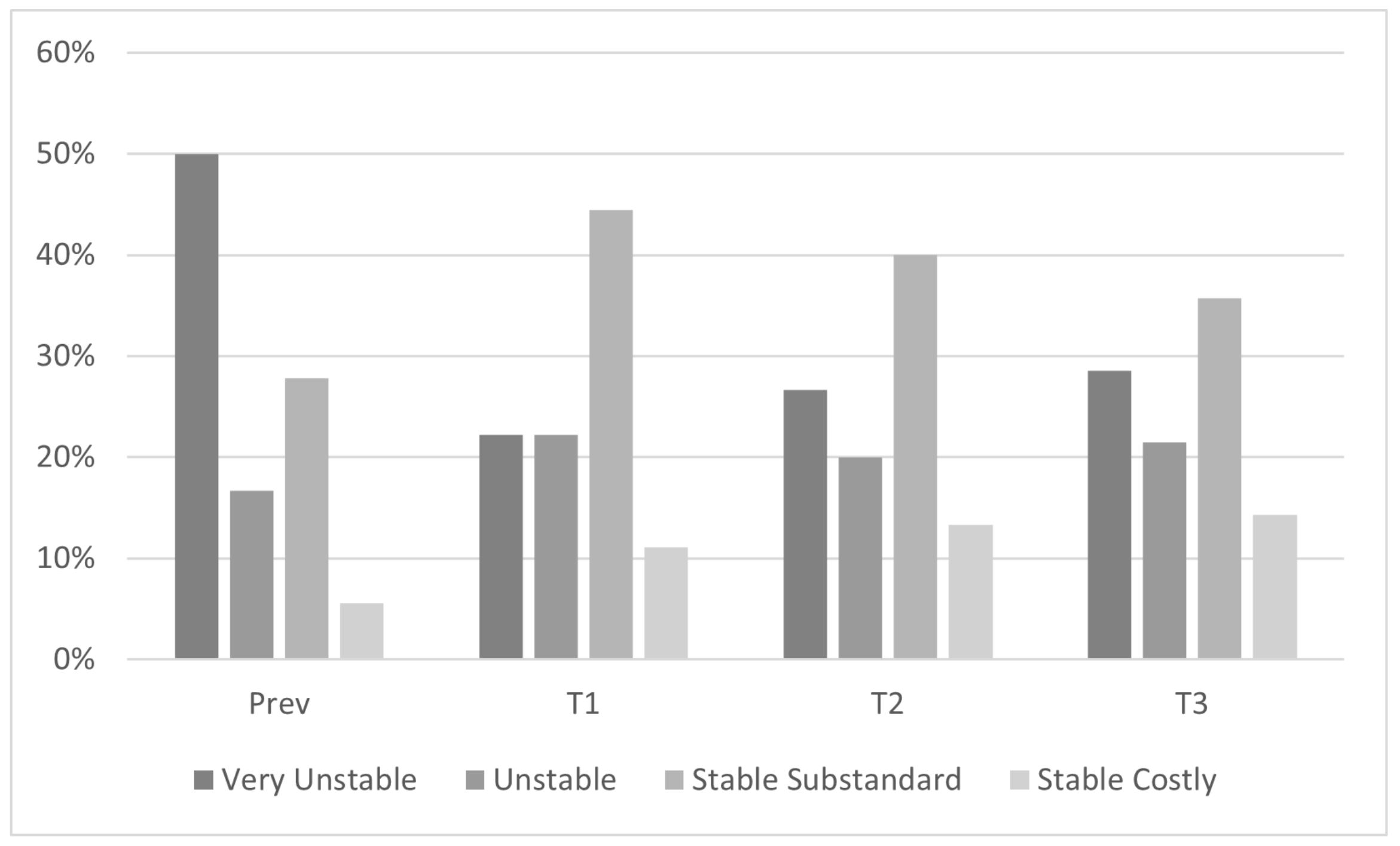
| Very unstable | 9 (50.00) | 9 (50.00) | 4 (22.22) | 4 (26.67) | 4 (28.57) | |
| Unstable | 6 (33.33) | 3 (16.67) | 4 (22.22) | 3 (20.00) | 3 (21.43) | |
| Stable substandard | 9 (50.00) | 5 (27.78) | 8 (44.44) | 6 (40.00) | 5 (35.71) | |
| Stable costly | 2 (11.11) | 1 (5.56) | 2 (11.11) | 2 (13.33) | 2 (14.29) | |
| IPV b | ||||||
| Emotional | 16 (88.89) | - | 16 (88.89) | 8 (53.33) | 6 (42.86) | |
| Physical | 11 (61.11) | - | 11 (61.11) | 1 (6.67) | 1 (7.14) | |
| Sexual | 12 (66.67) | - | 10 (55.56) | 4 (26.67) | 3 (21.43) | |
| Economic | 10 (55.56) | - | 8 (44.44) | 3 (20.00) | 2 (14.29) | |
| Social isolation | 11 (61.11) | - | 10 (55.56) | 2 (13.33) | 2 (14.29) | |
| Substance misuse b | ||||||
| Alcohol | 10 (55.56) | - | 9 (50.00) | 4 (26.67) | 2 (14.29) | |
| Marijuana | 7 (38.89) | - | 7 (38.89) | 3 (20.00) | 1 (7.14) | |
| Illicit drugs | 6 (33.33) | - | 6 (33.33) | 2 (13.33) | 2 (14.29) | |
| Increased risk for contracting HIV b | ||||||
| Condomless sex | 18 (100.00) | - | 18 (100.00) | 7 (46.67) | 4 (28.57) | |
| Multiple sex partners | 8 (44.44) | - | 7 (38.89) | 3 (20.00) | 3 (21.43) | |
| Partner has multiple sex partners | 14 (77.78) | - | 13 (72.22) | 5 (33.33) | 5 (35.71) | |
| Syndemic Variable | Very Unstable | Unstable | Stable Substandard | Stable Costly | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 n = 4 | T2 n = 4 | T3 n = 4 | T1 n = 4 | T2 n = 3 | T3 n = 3 | T1 n = 8 | T2 n = 6 | T3 n = 5 | T1 n = 2 | T2 n = 2 | T3 n = 2 | ||
| IPV | |||||||||||||
| Emotional | 100.0 | 100.0 | 100.0 | 75.0 | 33.3 | 33.3 | 87.5 | 33.3 | 20.0 | 100.0 | 50.0 | 0.0 | |
| Physical | 75.0 | 25.0 | 25.0 | 50.0 | 0.0 | 0.0 | 62.5 | 0.0 | 0.0 | 50.0 | 0.0 | 0.0 | |
| Sexual | 75.0 | 50.0 | 25.0 | 50.0 | 0.0 | 66.7 | 50.0 | 33.3 | 0.0 | 50.0 | 0.0 | 0.0 | |
| Economic | 25.0 | 25.0 | 50.0 | 50.0 | 0.0 | 0.0 | 62.5 | 33.3 | 0.0 | 0.0 | 0.0 | 0.0 | |
| Social Isolation | 50.0 | 25.0 | 50.0 | 25.0 | 0.0 | 0.0 | 75.0 | 16.7 | 0.0 | 50.0 | 0.0 | 0.0 | |
| Drugs | |||||||||||||
| Alcohol | 0.0 | 0.0 | 25.0 | 25.0 | 33.3 | 0.0 | 75.0 | 50.0 | 20.0 | 100.0 | 0.0 | 0.0 | |
| Marijuana | 50.0 | 50.0 | 25.0 | 50.0 | 33.3 | 0.0 | 37.5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | |
| Illicit | 25.0 | 25.0 | 25.0 | 25.0 | 0.0 | 0.0 | 37.5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | |
| Risk of acquiring HIV | |||||||||||||
| Condomless sex | 100.0 | 50.0 | 75.0 | 100.0 | 33.3 | 33.3 | 100.0 | 50.0 | 0.0 | 100.0 | 50.0 | 0.0 | |
| Multiple sex partners | 50.0 | 25.0 | 0.0 | 50.0 | 33.3 | 66.7 | 37.5 | 16.7 | 20.0 | 0.0 | 0.0 | 0.0 | |
| Partner with multiple sex partners | 100.0 | 25.0 | 25.0 | 100.0 | 66.7 | 66.7 | 50.0 | 16.7 | 20.0 | 50.0 | 50.0 | 50.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nydegger, L.A.; Benton, E.N.; Hemingway, B.; Fung, S.; Yuan, M.; Phung, C.; Claborn, K.R. Housing Insecurity and Other Syndemic Factors Experienced by Black and Latina Cisgender Women in Austin, Texas: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 7177. https://doi.org/10.3390/ijerph20247177
Nydegger LA, Benton EN, Hemingway B, Fung S, Yuan M, Phung C, Claborn KR. Housing Insecurity and Other Syndemic Factors Experienced by Black and Latina Cisgender Women in Austin, Texas: A Qualitative Study. International Journal of Environmental Research and Public Health. 2023; 20(24):7177. https://doi.org/10.3390/ijerph20247177
Chicago/Turabian StyleNydegger, Liesl A., Erin N. Benton, Bree Hemingway, Sarah Fung, Mandy Yuan, Chau Phung, and Kasey R. Claborn. 2023. "Housing Insecurity and Other Syndemic Factors Experienced by Black and Latina Cisgender Women in Austin, Texas: A Qualitative Study" International Journal of Environmental Research and Public Health 20, no. 24: 7177. https://doi.org/10.3390/ijerph20247177
APA StyleNydegger, L. A., Benton, E. N., Hemingway, B., Fung, S., Yuan, M., Phung, C., & Claborn, K. R. (2023). Housing Insecurity and Other Syndemic Factors Experienced by Black and Latina Cisgender Women in Austin, Texas: A Qualitative Study. International Journal of Environmental Research and Public Health, 20(24), 7177. https://doi.org/10.3390/ijerph20247177