
A Community-Engaged Approach to Understanding Suicide in a Small Rural County in Georgia: A Two-Phase Content Analysis of Individual and Focus Group Interviews

 , ,
, ,  ,
,
Abstract
:1. Introduction
Role of Community-Based Suicide Research
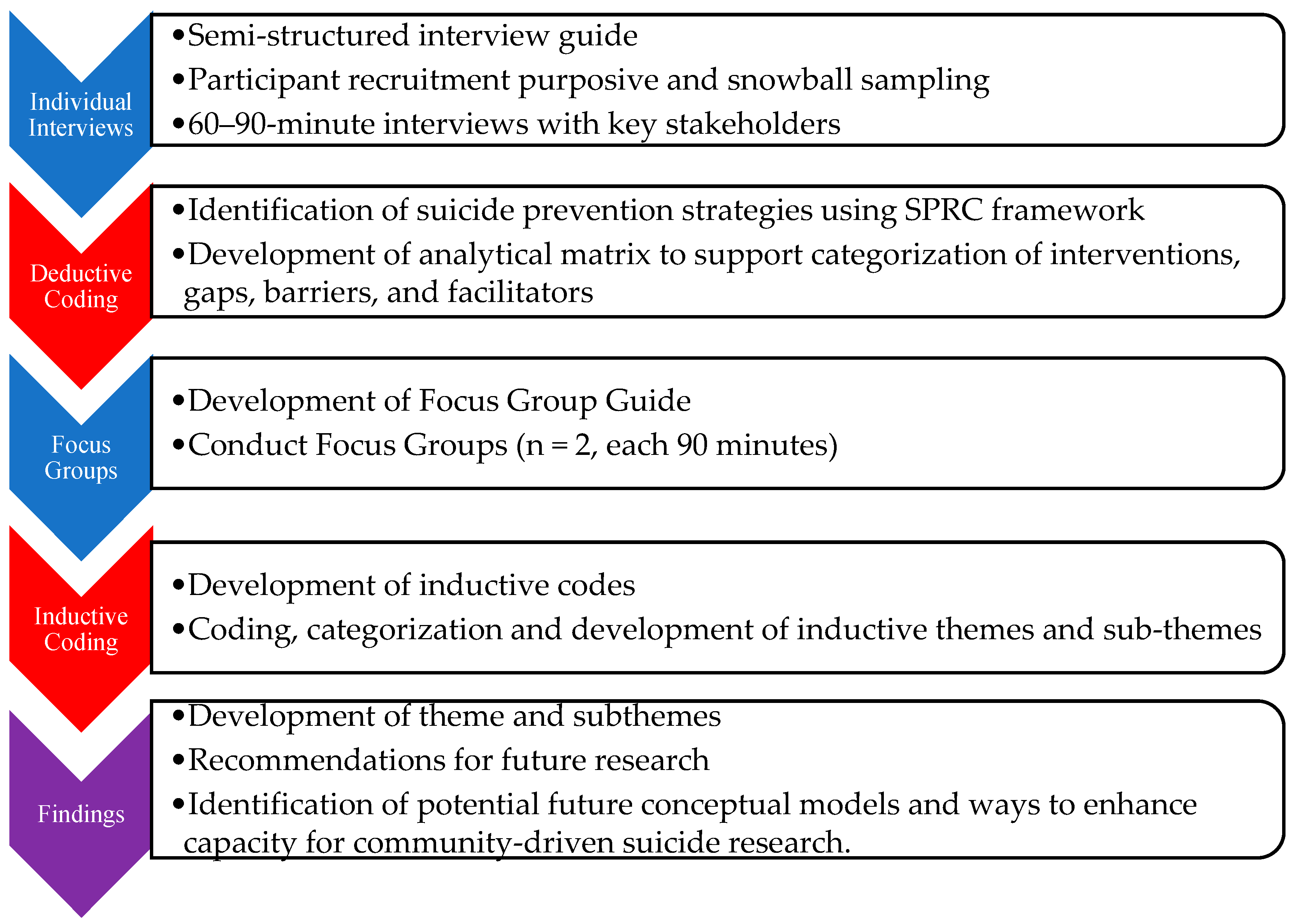
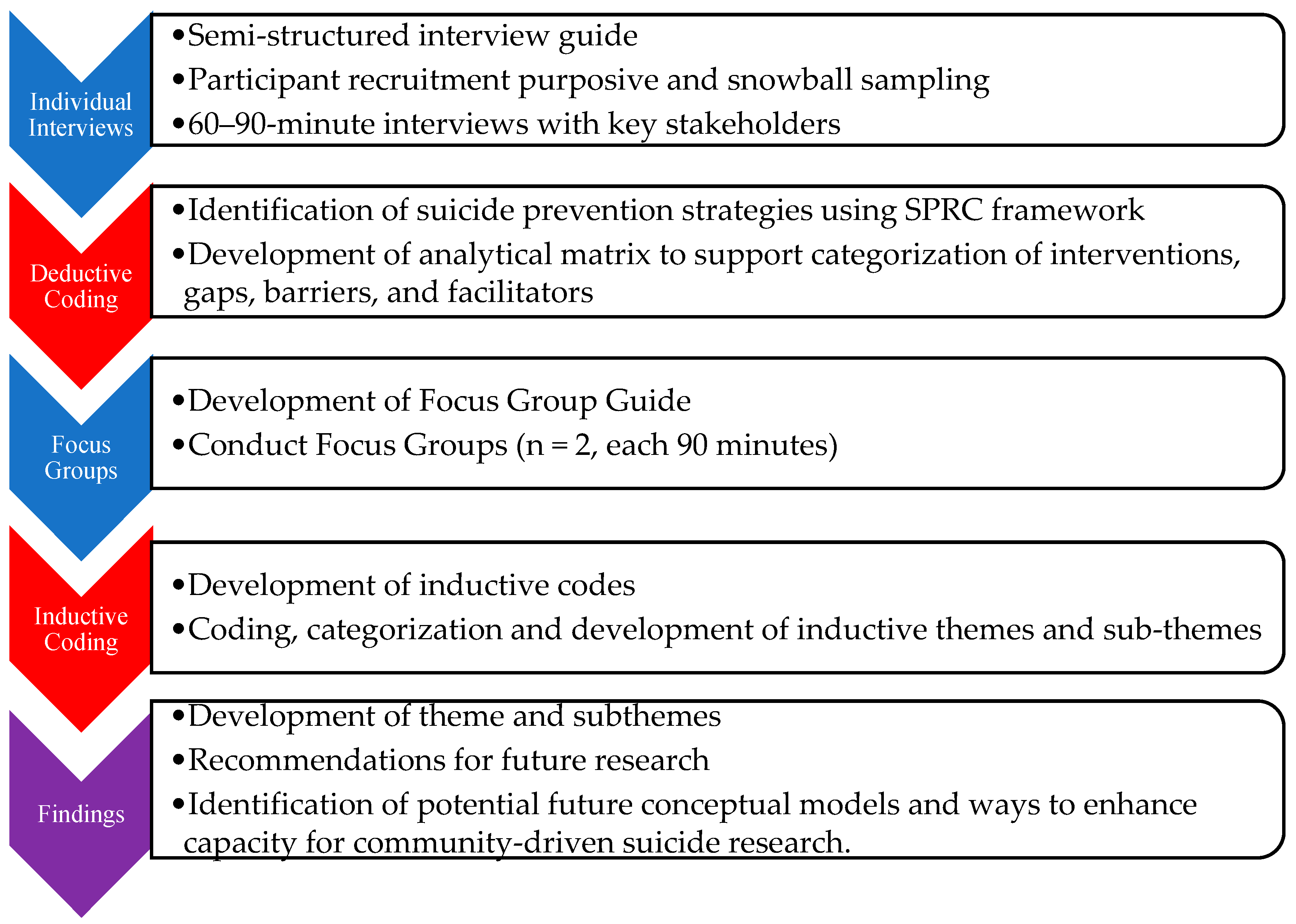
2. Materials and Methods
2.1. Setting
2.2. Participants and Data Collection
Ethical Considerations
2.3. Data Analysis
3. Results
3.1. Theme 1: Cumulative Trauma and Isolation
3.1.1. Subtheme 1.1: Community Crisis
“Matter of fact, we’ve coined a phrase here in our practice…It’s just something we’ve used specifically, not just for [county name] County but the surrounding area, and we’ve called it “CUTI”. And we just—it’s one of those code words. We know what we’re talking about in-house. But it’s “Cumulative Unresolved Trauma Isolation.””—ID 113. Mental health provider.
“It’s the ones that are living in a trailer, living in a pop-up camper with a tarp over the roof cuz there’s holes. And then they got to push it up. It’s causing a lot of depression. And then the money comes in that’s supposed to go for the kids and it’s going to alcohol. So, parents are shoving their kids out at 18. And, I mean, we had a 19-year-old that shot himself in the face because he wasn’t ready for the world.”—ID 105. First responder.
“… we have the Georgia crisis line, but in many cases, they have three or four hours of travel time to send a crisis team. So, it really puts the people that are the boots on the ground, dealing with these individuals on a daily basis, in a quandary.”—ID 110. Fire department member.
3.1.2. Subtheme 1.2: Survivors of Suicide Loss
“I’ve dealt myself in the last two years with 21 area suicides. Families after the fact. Of those 21, half were in [this] county.”—ID 113. Mental health provider.
“70,000 people in this town. Everybody’s related to somebody, and everybody’s related to somebody who’s killed themselves, and it matters…When you’re looking at numbers and statistics, it doesn’t matter. When you’re sitting there and you’re looking at the list, and you’re reading down the list and realize, “Oh my gosh. There’s my cousin’s daughter.””—ID 120. Grassroots organization founder.
3.2. Theme 2: Support Networks and Systems
3.2.1. Subtheme 2.1: Connections to Formal Systems
“I don’t know, I think it depends on if their motivation, their support network and systems—It’s hard to give kind of a blanket response. I think that’s kind of, for each individual, it’s probably a kind of different, and dependent on a lot of factors as well. Folks who are more connected to formal organizations, such as military personnel, and because they didn’t report to duty or something they—it may become more known, have probably a greater chance of accessing help than some others or a child who confides in a peer at school, who reaches out to a counselor or teacher…”—ID 117. Non-profit staff.
“We as a district—all of our counselors just went through a suicide first aid training. …of course, all of us are trained in suicide prevention in and of itself, just from the credentials we have to have to do the job. But just from the recent deaths by suicide that we have had, there was definitely a need to say, “Okay, what else can we do?” And so, we just went through an intensive training to refresh our skills…just so that we could be more prepared to deal with our students as they are dealing with their issues…”—ID 106. School counselor.
As stated by another school counselor: ““And that may be because a lot of what I’m dealing with is military, and they’ve got the services. And they’ve got the insurance. And they’ve got an avenue. I would say that’s probably the biggest difference.” According to key stakeholders, some of these services included increased awareness campaigns, emergency department and inpatient beds on military bases, and family counseling.”—ID 102. School counselor.
3.2.2. Subtheme 2.2: Barriers to Help-Seeking: Family Resources and Stigma
“Now, my parents wouldn’t—but I know there’s people that I grew up around them that are their age [60s], that would probably not know what to do if they had an adult child tells them that they were having a problem. It’s just something that they wouldn’t talk about. It’s almost kind of like, not the southern, that kind of southern way of like not talking about things that make people uncomfortable.”—ID118. Counselor.
“So, I think access to mental health is a big deal whether they know if it’s okay, the stigma piece, or whether they can afford it and whether they just can’t get here and looking for alternatives to try and help them to access the help that is here. So, you asked me three reasons, I would say access to mental health treatment, economic life you know just financial concerns.”—ID112. Counselor.
“Yeah, I think one is cost. I think culture, because you’re viewed as weak—in the black community especially. And I think in some of the other communities if you are talking about harming yourself. And I think another barrier is there’s no facilities! There’s no real place to go. I mean, there’s a place for drug and alcohol abuse, sexual abuse. There’s no real place for people who are feeling like they want to end it all, to go and have a group meeting, and talk about it. Not to my knowledge.”—ID101. Government official.
3.3. Theme 3: Treatment Gaps and Community Response
3.3.1. Subtheme 3.1: Linkage Gaps in Mental Health Care
“Like, the patient I told you, they’d been bringing him here for—because he lives in a group home. And they can’t even get them to give him his shot… I think the doctor that used to be there a lot, he kind of left, and they have problems getting personnel to run the place, to be efficient, to be open all the time.”—ID 119. Primary care provider
ID 123 (school counselor): “[The ER] is our point of entry usually. A lot of times we’re going to the ER in the medical… We’re going with students or advising parents to go to the ER… And also the telehealth sometimes. We have used that before…”
ID 110 (EMS provider): “It flabbergasts me to hear that our school system has access to telehealth, but our emergency responders don’t. Cuz if you think about the school systems are open for this short window of the day, but we’re responding to calls 24 h a day and we don’t have that, especially for the EMS side. The fire service doesn’t, but with that EMS history and background. It blows my mind that that’s not…”
3.3.2. Subtheme 3.2: Community Response
“And [the state suicide prevention specialist] gave me a lot of trainings or list of trainings, and then I had the other death. And then I had another one. And so, at that point, I reached out to her and I was like, “Hey, something’s really, really not right going on here.” … And at that point, she suggested that we maybe start up a coalition for our community. And with that—it’s a lot of work…. And now it’s just the part of trying to get everybody together is where I’m kind of stuck at… And so, that’s where I kind of am at this point.”—ID 104. School administrator.
ID 121 (pastor): “…we need to know what the medical resources are, [healthcare director], because most of the people that are counseling. They don’t know what to do. I mean, I get it all the time. They call me all the time that they call me, “Pastor. Do I send them to [mental health facility 1] or do I send them to [mental health facility 2]? They’re both full. What do I do?” And I’m like, well—”
ID 116 (counselor): “There needs to be somebody that binds that bit.”
ID 121 (pastor): “Yeah, and we don’t know where to go, and we don’t know what to do.”
ID 128 (healthcare director): “And see, that’s what we’re living in too, because when we’re sending somebody, we’re usually trying to find a place where to admit them, and there’s such limited places…”
ID 121 (pastor): “But I think the team that we develop needs to have an understanding of how that works, because if we have a better understanding of how the healthcare side of it works, if we have that education, then we become better equipped, and we might even also be able to take some of the pressure of off the ER on a cold night.”
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention, National Center for Health. Statistics 1999–2018 Wide Ranging Online Data for Epidemiological Research (WONDER); Multiple Cause of Death Files [Data File]; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020.
- Hedegaard, H.; Curtin, S.C.; Warner, M. Increase in Suicide Mortality in the United States, 1999–2018; National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- Substance Abuse and Mental Health Services Administration (SAMHSA). Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health; NSDUH Series H-56; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021.
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-Based Injury Statistics Query and Reporting System (WISQARS). 2019. Available online: https://www.cdc.gov/injury/wisqars/index.html (accessed on 21 September 2023).
- Suicide Prevention Resource Center. Suicide by Age. Available online: https://www.sprc.org/scope/age (accessed on 26 May 2021).
- Kegler, S.R.; Stone, D.M.; Holland, K.M. Trends in Suicide by Level of Urbanization—United States, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Steelesmith, D.L.; Fontanella, C.A.; Campo, J.V.; Bridge, J.A.; Warren, K.L.; Root, E.D. Contextual Factors Associated with County-Level Suicide Rates in the United States, 1999 to 2016. JAMA Netw/Open 2019, 2, e1910936. [Google Scholar] [CrossRef] [PubMed]
- Ivey-Stephenson, A.Z.; Crosby, A.E.; Jack, S.P.D.; Haileyesus, T.; Kresnow-Sedacca, M. Suicide Trends Among and Within Urbanization Levels by Sex, Race/Ethnicity, Age Group, and Mechanism of Death—United States, 2001–2015. MMWR Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, H.; Curtin, S.C.; Warner, M. Suicide Mortality in the United States, 1999–2017; U.S. Department of Health and Human Services, National Institutes of Health: Research Triangle Park, NC, USA, 2018.
- Barnhorst, A.; Gonzales, H.; Asif-Sattar, R. Suicide Prevention Efforts in the United States and Their Effectiveness. Curr. Opin. Psychiatry 2021, 34, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Georgia Department of Public Health. Online Analytical Statistical Information System (OASIS). Mortality Web Query. Available online: https://oasis.state.ga.us/oasis/webquery/qryMortality.aspx (accessed on 8 December 2022).
- Center for Behavioral Health Statistics and Quality. 2018 National Survey on Drug Use and Health: Detailed Tables; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2019.
- Butterworth, S.E.; Daruwala, S.E.; Anestis, M.D. The Role of Reason for Firearm Ownership in Beliefs about Firearms and Suicide, Openness to Means Safety, and Current Firearm Storage. Suicide Life Threat. Behav. 2020, 50, 617–630. [Google Scholar] [CrossRef] [PubMed]
- Rural Health Information Hub. Barriers to Mental Health Treatment in Rural Areas. Available online: https://www.ruralhealthinfo.org/toolkits/mental-health/1/barriers (accessed on 7 June 2021).
- Gamm, L.; Stone, S.; Pittman, S. Mental Health and Mental Disorders—A Rural Challenge: A Literature Review. In Rural Healthy People 2010: A Companion Document to Healthy People 2010; The Texas A&M University System Health Science Center, School of Rural Public Health, Southwest Rural Health Research Center: College Station, TX, USA, 2003; Volume 2. [Google Scholar]
- Goldstein, E.V.; Prater, L.C.; Wickizer, T.M. Behavioral Health Care and Firearm Suicide: Do States with Greater Treatment Capacity Have Lower Suicide Rates? Health Aff. 2019, 38, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.G.; Branas, C.C.; Metlay, J.P.; Sullivan, A.F.; Camargo, C.A. Access to Emergency Care in the United States. Ann. Emerg. Med. 2009, 54, 261–269. [Google Scholar] [CrossRef]
- Hjelmeland, H.; Knizex, B.L. Why We Need Qualitative Research in Suicidology. Suicide Life-Threat. Behav. 2010, 40, 74–80. [Google Scholar] [CrossRef]
- Epp, D.; Rauch, K.; Waddell-Henowitch, C.; Ryan, K.D.; Herron, R.V.; Thomson, A.E.; Mullins, S.; Ramsey, D. Maintaining Safety While Discussing Suicide: Trauma Informed Research in an Online Focus Groups. Int. J. Qual. Methods 2022, 21, 16094069221135973. [Google Scholar] [CrossRef]
- Kohlbeck, S.A.; Quinn, K.; deRoon-Cassini, T.; Hargarten, S.; Nelson, D.; Cassidy, L. “I’ve given up”: Biopsychosocial factors preceding farmer suicide in Wisconsin. Am. J. Orthopsychiatry 2023, 93, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Varia, S.G.; Ebin, J.; Stout, E.R. Suicide prevention in rural communities: Perspectives from a Community of Practice. J. Rural Ment. Health 2014, 38, 109–115. [Google Scholar] [CrossRef]
- Grattidge, L.; Hoang, H.; Mond, J.; Lees, D.; Visentin, D.; Auckland, S. Exploring Community-Based Suicide Prevention in the Context of Rural Australia: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 2644. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979; ISBN 978-0-674-02884-5. [Google Scholar]
- Suicide Prevention Resource Center. A Comprehensive Approach to Suicide Prevention. Available online: https://www.sprc.org/effective-prevention/comprehensive-approach (accessed on 27 May 2021).
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N.; Wensing, M.; Fiander, M.; Eccles, M.P.; et al. Tailored Interventions to Address Determinants of Practice. Cochrane Database Syst. Rev. 2015, 4, CD005470. [Google Scholar] [CrossRef] [PubMed]
- Georgia Department of Public Health. Online Analytical Statistical Information System (OASIS). Available online: https://oasis.state.ga.us/oasis/webquery/qryDrugOverdose.aspx (accessed on 8 December 2022).
- Wreally. Transcribe. [Software]. Available online: https://transcribe.wreally.com/ (accessed on 1 August 2021).
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Sandström, B.; Willman, A.; Svensson, B.; Borglin, G. Perceptions of National Guidelines and Their (Non) Implementation in Mental Healthcare: A Deductive and Inductive Content Analysis. Implement. Sci. 2015, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Schreier, M. Qualitative Content Analysis. In The SAGE Handbook of Qualitative Data Analysis; Flick, U., Ed.; SAGE Publications Ltd.: London, UK, 2014; pp. 170–183. ISBN 978-1-4462-8224-3. [Google Scholar]
- Dedoose. Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data. 2021. [Software]. Available online: https://www.dedoose.com/ (accessed on 8 December 2022).
- Graneheim, U.H.; Lundman, B. Qualitative Content Analysis in Nursing Research: Concepts, Procedures and Measures to Achieve Trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Birks, M.; Chapman, Y.; Francis, K. Memoing in Qualitative Research: Probing Data and Processes. J. Res. Nurs. 2008, 13, 68–75. [Google Scholar] [CrossRef]
- Pitman, A.; Osborn, D.; King, M.; Erlangsen, A. Effects of Suicide Bereavement on Mental Health and Suicide Risk. Lancet Psychiatry 2014, 1, 86–94. [Google Scholar] [CrossRef]
- LoMurray, M. Sources of Strength Facilitators Guide: Suicide Prevention Peer Gatekeeper Training; The North Dakota Suicide Prevention Project: Bismarck, ND, USA, 2005. [Google Scholar]
- LivingWorks ASIST. Suicide Prevention Training Program. Available online: https://www.livingworks.net/asist (accessed on 3 August 2023).
- Quinnett, P. QPR: Ask a Question, Save a Life; QPR Institute and Suicide Awareness/Voices of Education: Spokane, WA, USA, 1995. [Google Scholar]
- American Foundation for Suicide Prevention [AFSP]. Out of the Darkness Walks. Available online: https://supporting.afsp.org/?fuseaction=cms.page&id=1370 (accessed on 25 May 2023).
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; First Touchstone; Simon and Schuster: New York, NY, USA, 1986; ISBN 978-1-4391-8833-0. [Google Scholar]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of All-Cause and Suicide Mortality in Mental Disorders: A Meta-Review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and Suicidal Behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.K.; Cukrowicz, K.C. Suicide in Rural Areas: An Updated Review of the Literature. J. Rural Ment. Health 2014, 38, 65–78. [Google Scholar] [CrossRef]
- Barry, R.; Rehm, J.; de Oliveira, C.; Gozdyra, P.; Kurdyak, P. Rurality and Risk of Suicide Attempts and Death by Suicide among People Living in Four English-Speaking High-Income Countries: A Systematic Review and Meta-Analysis. Can. J. Psychiatry 2020, 65, 441–447. [Google Scholar] [CrossRef]
- Elnour, A.A.; Harrison, J. Lethality of Suicide Methods. Inj. Prev. 2008, 14, 39–45. [Google Scholar] [CrossRef]
- Aguirre, R.T.P.; Slater, H. Suicide Postvention as Suicide Prevention: Improvement and Expansion in the United States. Death Stud. 2010, 34, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.R. Postvention Is Prevention—The Case for Suicide Postvention. Death Stud. 2017, 41, 614–621. [Google Scholar] [CrossRef]
- Hill, S.K.; Cantrell, P.; Edwards, J.; Dalton, W. Factors Influencing Mental Health Screening and Treatment Among Women in a Rural South Central Appalachian Primary Care Clinic. J. Rural Health 2016, 32, 82–91. [Google Scholar] [CrossRef]
- Hoge, C.W.; Castro, C.A. Preventing Suicides in US Service Members and Veterans: Concerns After a Decade of War. JAMA 2012, 308, 671. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Stein, M.B.; Heeringa, S.G.; Ursano, R.J.; Colpe, L.J.; Fullerton, C.S.; Hwang, I.; Naifeh, J.A.; Sampson, N.A.; Schoenbaum, M.; et al. Prevalence and Correlates of Suicidal Behavior Among Soldiers: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry 2014, 71, 514. [Google Scholar] [CrossRef] [PubMed]
- Chaskin, R.J. Building Community Capacity: A Definitional Framework and Case Studies from a Comprehensive Community Initiative. Urban Aff. Rev. 2001, 36, 291–323. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration [SAMHSA]. Crisis Intercept Mapping for SMVF Suicide Prevention. Available online: https://www.samhsa.gov/smvf-ta-center/activities/crisis-intercept-mapping (accessed on 25 May 2023).


{kind=link}
{kind=link}
| Themes | Subthemes |
|---|---|
| 1. Cumulative trauma and isolation | 1.1. Community crisis 1.2. Survivors of suicide loss |
| 2. Support networks and systems | 2.1. Evidence-based practices: Connections to formal systems 2.2. Barriers: Family resources and help-seeking |
| 3. Treatment gaps and community response | 3.1. Linkage gaps in mental health care 3.2. Lack of formalized postvention services |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roth, K.B.; Gaveras, E.; Ghiathi, F.; Shaw, E.K.; Shoemaker, M.S.; Howard, N.A.; Dhir, M.; Caiza, G.R.; Szlyk, H.S. A Community-Engaged Approach to Understanding Suicide in a Small Rural County in Georgia: A Two-Phase Content Analysis of Individual and Focus Group Interviews. Int. J. Environ. Res. Public Health 2023, 20, 7145. https://doi.org/10.3390/ijerph20247145
Roth KB, Gaveras E, Ghiathi F, Shaw EK, Shoemaker MS, Howard NA, Dhir M, Caiza GR, Szlyk HS. A Community-Engaged Approach to Understanding Suicide in a Small Rural County in Georgia: A Two-Phase Content Analysis of Individual and Focus Group Interviews. International Journal of Environmental Research and Public Health. 2023; 20(24):7145. https://doi.org/10.3390/ijerph20247145
Chicago/Turabian StyleRoth, Kimberly Beth, Eleni Gaveras, Fatima Ghiathi, Eric Kendall Shaw, Melanie Shanlin Shoemaker, Nicholas Adam Howard, Meena Dhir, Genesis Rebeca Caiza, and Hannah Selene Szlyk. 2023. "A Community-Engaged Approach to Understanding Suicide in a Small Rural County in Georgia: A Two-Phase Content Analysis of Individual and Focus Group Interviews" International Journal of Environmental Research and Public Health 20, no. 24: 7145. https://doi.org/10.3390/ijerph20247145
APA StyleRoth, K. B., Gaveras, E., Ghiathi, F., Shaw, E. K., Shoemaker, M. S., Howard, N. A., Dhir, M., Caiza, G. R., & Szlyk, H. S. (2023). A Community-Engaged Approach to Understanding Suicide in a Small Rural County in Georgia: A Two-Phase Content Analysis of Individual and Focus Group Interviews. International Journal of Environmental Research and Public Health, 20(24), 7145. https://doi.org/10.3390/ijerph20247145