
Health Economic Evaluation of an Online-Based Motivational Program to Reduce Problematic Media Use and Promote Treatment Motivation for Internet Use Disorder—Results of the OMPRIS Study

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AICA-S | Scale for the Assessment of Internet and Computer Game Addiction |
| CEA | cost-effectiveness analysis |
| CUA | cost-utility analysis |
| DDD | defined daily dose |
| DiD | difference-in-difference |
| EBM | German doctor’s fee scale |
| ICER | incremental cost-effectiveness ratio |
| IG | intervention group |
| IUD | Internet Use Disorders |
| PRC | Persons with Reliable Change |
| QALYs | quality-adjusted life years |
| RC | Reliable Change |
| RCI | Reliable Change Index |
| SHI | statutory health insurance |
| WCG | waiting control group |
References
- Wölfling, K.; Beutel, M.E.; Bengesser, I.; Müller, K.W. Computerspiel- und Internetsucht: Ein Kognitiv-Behaviorales Behandlungsmanual; W. Kohlhammer GmbH: Mainz, Germany, 2012. [Google Scholar]
- World Health Organization. Addictive Behaviours: Gaming Disorder. Available online: https://www.who.int/news-room/questions-and-answers/item/addictive-behaviours-gaming-disorder (accessed on 13 December 2022).
- Pan, Y.C.; Chiu, Y.C.; Lin, Y.H. Systematic review and meta-analysis of epidemiology of internet addiction. Neurosci. Biobehav. Rev. 2020, 118, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.W.; Glaesmer, H.; Brähler, E.; Woelfling, K.; Beutel, M.E. Prevalence of internet addiction in the general population: Results from a German population-based survey. Behav. Inf. Technol. 2014, 33, 757–766. [Google Scholar] [CrossRef]
- Wartberg, L.; Kriston, L.; Thomasius, R. The Prevalence and Psychosocial Correlates of Internet Gaming Disorder. Dtsch. Arztebl. Int. 2017, 114, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Hofmarcher, T.; Romild, U.; Spangberg, J.; Persson, U.; Hakansson, A. The societal costs of problem gambling in Sweden. BMC Public Health 2020, 20, 1921. [Google Scholar] [CrossRef] [PubMed]
- Effertz, T.; Bischof, A.; Rumpf, H.J.; Meyer, C.; John, U. The effect of online gambling on gambling problems and resulting economic health costs in Germany. Eur. J. Health Econ. 2018, 19, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Dieris-Hirche, J.; Bottel, L.; Pape, M.; Te Wildt, B.T.; Wolfling, K.; Henningsen, P.; Timmesfeld, N.; Neumann, A.; Neusser, S.; Beckers, R.; et al. Effects of an online-based motivational intervention to reduce problematic internet use and promote treatment motivation in internet gaming disorder and internet use disorder (OMPRIS): Study protocol for a randomised controlled trial. BMJ Open 2021, 11, e045840. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.O.; Brettschneider, C.; Seidl, H.; Bowles, D.; Holle, R.; Greiner, W.; Konig, H.H. Calculation of standardised unit costs from a societal perspective for health economic evaluation. Gesundheitswesen 2015, 77, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Grupp, H.; König, H.-H.; Konnopka, A. Calculation of Standardised Unit Costs for the Economic Evaluation of Mental Disorders. Gesundheitswesen 2017, 79, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Scholz, S.; Biermann-Stallwitz, J.; Brettschneider, C.; Damm, O.; Freytag, A.; Greiner, W.; Icks, A. Standardisierte Kostenberechnungen im deutschen Gesundheitswesen: Bericht der Arbeitsgruppe “Standardkosten” des Ausschusses “ökonomische Evaluation” der dggö. Gesundheitsökonomie Qual. 2020, 25, 52–59. [Google Scholar] [CrossRef]
- Schwalm, A.; Neusser, S.; Mostardt, S.; Kunigkeit, C.; Biermann-Stallwitz, J.; Wasem, J.; Neumann, A. Methoden der Kostenberechnung von Arzneimitteln im deutschen Gesundheitssystem: Bericht der Arbeitsgruppe “Standardkosten” des Ausschusses “ökonomische Evaluation” der dggö. Gesundheitsökonomie Qual. 2020, 25, 44–51. [Google Scholar] [CrossRef]
- Kassenärztliche Bundesvereinigung. Einheitlicher Bewertungsmaßstab (EBM). Stand: 1. Quartal 2022. Available online: https://www.kbv.de/media/sp/EBM_Gesamt_-_Stand_1._Quartal_2022.pdf (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Entgeltatlas. Available online: https://web.arbeitsagentur.de/entgeltatlas/ (accessed on 16 November 2022).
- IQWiG. Allgemeine Methoden. Version 6.1 vom 24.1.2022. Available online: https://www.iqwig.de/methoden/allgemeine-methoden-v6-1.pdf (accessed on 16 November 2022).
- Statistisches Bundesamt (Destatis). Verbraucherpreisindex: Deutschland, Jahre. Verfügbarer Zeitraum 1991–2021. Available online: https://www-genesis.destatis.de/genesis/online?sequenz=tabelleErgebnis&selectionname=61111-0001&startjahr=1991#abreadcrumb (accessed on 16 November 2022).
- Statistisches Bundesamt (Destatis). Lohnnebenkosten in Deutschland in Euro. Available online: https://www.destatis.de/DE/Themen/Arbeit/Arbeitskosten-Lohnnebenkosten/Tabellen/lohnkosten-deutschland.html (accessed on 16 November 2022).
- LAUER-FISCHER GmbH. LAUER-TAXE® Online 4.0. Fürth, Germany. Available online: https://portal.cgmlauer.cgm.com/LF/Seiten/Verwaltung/Kundencenter/1.aspx (accessed on 8 November 2022).
- Fricke, U.; Günther, J.; Niepraschk-von Dollen, K.; Zawinell, A. Anatomisch-Therapeutisch-Chemische Klassifikation mit Tagesdosen für den Deutschen Arzneimittelmarkt. ATC-Index mit DDD-Angaben. Available online: https://www.wido.de/publikationen-produkte/arzneimittel-klassifikation/ (accessed on 4 April 2022).
- Ludwig, W.-D.; Mühlbauer, B.; Seifert, R. Arzneimittelverordnung—Report 2021; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Bundesministerium der Finanzen. AfA-Tabelle für die Allgemein Verwendbaren Anlagegüter (Afa-Tabelle„AV“). Available online: https://www.bundesfinanzministerium.de/Content/DE/Standardartikel/Themen/Steuern/Weitere_Steuerthemen/Betriebspruefung/AfA-Tabellen/Ergaenzende-AfA-Tabellen/AfA-Tabelle_AV.pdf?__blob=publicationFile&v=3 (accessed on 7 June 2022).
- Wölfling, K.; Beutel, M.E.; Müller, K.W. OSV-S—Skala zum Onlinesuchtverhalten. In Diagnostische Verfahren in der Psychotherapie; Geue, K., Strauß, B., Brähler, E., Eds.; Hogrefe: Göttingen, Germany, 2016; pp. 362–366. [Google Scholar]
- Wölfling, K.; Müller, K.W.; Beutel, M. Reliabilität und Validität der Skala zum Computerspielverhalten (CSV-S). Psychother. Psych. Med. 2011, 61, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.W.; Dreier, M.; Beutel, M.E.; Duven, E.; Giralt, S.; Wölfling, K. A hidden type of internet addiction? Intense and addictive use of social networking sites in adolescents. Comput. Hum. Behav. 2016, 55, 172–177. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- EuroQol Group. EQ-5D-5L. German. Germany. Self-Complete. Digital. Available online: https://euroqol.org/eq-5d-instruments/all-eq-5d-versions/ (accessed on 22 July 2020).
- Ludwig, K.; Graf von der Schulenburg, J.M.; Greiner, W. German Value Set fort he EQ-5D-5L. Pharmacoeconomics 2018, 36, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt (Destatis). Verdienste und Arbeitskosten. Arbeitnehmerverdienste Jahr 2021. Fachserie 16. Reihe 2.3. Available online: https://www.destatis.de/DE/Themen/Arbeit/Verdienste/Verdienste-Branche-Berufe/Publikationen/Downloads/arbeitnehmerverdienste-jahr-2160230217004.pdf?__blob=publicationFile (accessed on 20 March 2023).
- Bundesagentur für Arbeit. Entgeltatlas. Helfer/in—Hauswirtschaft. Available online: https://web.arbeitsagentur.de/entgeltatlas/beruf/90128 (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Entgeltatlas. Kinderbetreuer/in. Available online: https://web.arbeitsagentur.de/entgeltatlas/beruf/14335 (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Entgeltatlas. Rechtliche/r Betreuer/in. Available online: https://web.arbeitsagentur.de/entgeltatlas/beruf/59085 (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Entgeltatlas. Sozialarbeiter/in/Sozialpädagoge/-pädagogin. Available online: https://web.arbeitsagentur.de/entgeltatlas/beruf/58775 (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Entgeltatlas. Erzieher/in—Jugend- und Heimerziehung. Available online: https://web.arbeitsagentur.de/entgeltatlas/beruf/9101 (accessed on 16 November 2022).
- Bundesagentur für Arbeit. Berichte: Blickpunkt Arbeitsmarkt—Der Arbeitsmarkt in Deutschland 2021. Available online: https://statistik.arbeitsagentur.de/Statistikdaten/Detail/202112/ama/heft-arbeitsmarkt/arbeitsmarkt-d-0-202112-pdf.pdf?__blob=publicationFile&v=2 (accessed on 4 May 2023).
- Klauber, J.; Geraedts, M.; Friedrich, J.; Wasem, J. Krankenhaus-Report 2016 „Ambulant im Krankenhaus“. Auszug Seite 63–84. Available online: https://www.wido.de/fileadmin/Dateien/Dokumente/Publikationen_Produkte/Buchreihen/Krankenhausreport/2016/Kapitel%20mit%20Deckblatt/wido_khr2016_kap04.pdf (accessed on 20 March 2023).
- Gesetzliche Krankenversicherung. Vorläufige Rechnungsergebnisse 1.-4. Quartal 2014. Available online: https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Statistiken/GKV/Finanzergebnisse/KV45_4Q2014.pdf (accessed on 16 November 2022).
- Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG). Burnout—Kann Yoga bei der Bewältigung Helfen? Available online: https://www.iqwig.de/download/ht21-02_yoga-bei-burnout_vorlaeufiger-hta-bericht_v1-0.pdf (accessed on 11 July 2023).
- Dieris-Hirche, J.; Bottel, L.; Basten, J.; Pape, M. Efficacy of a short-term, webcam-based telemedicine treatment of internet use disorders (OMPRIS): A multicentre, prospective, single-blind, randomised, clinical trial. eClinicalMedicine 2023, 64, 102216. [Google Scholar] [CrossRef] [PubMed]
- Devlin, N.J.; Brooks, R. EQ-5D and the EuroQol Group: Past, Present and Future. Appl. Health Econ. Health Policy 2017, 15, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Elliott, S.A.; Brown, J.S. What are we doing to waiting list controls? Behav. Res. Ther. 2002, 40, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Andersson, G.; Li, J.; Mergl, R.; Hegerl, U. The effects of blinding on the outcomes of psychotherapy and pharmacotherapy for adult depression: A meta-analysis. Eur. Psychiatry 2015, 30, 685–693. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | Total (n = 169) | IG (n = 81) | WCG (n = 88) |
|---|---|---|---|
| Age in years [MV (SD)] | 31.93 (12.08) | 32.11 (12.77) | 31.76 (11.48) |
| Gender [n (%)] | |||
| male | 127 (75.1) | 63 (77.8) | 64 (7.7) |
| female | 39 (23.1) | 18 (22.2) | 21 (23.9) |
| divers | 3 (1.8) | 0 | 3 (3.4) |
| Nationality [n (%)] | |||
| German | 163 (96.4) | 77 (95.1) | 86 (97.7) |
| other | 6 (3.6) | 4 (4.9) | 2 (2.3) |
| Highest school degree [n (%)] | |||
| currently at school | 6 (3.6) | 4 (4.9) | 2 (2.3) |
| secondary school (usually 9 to 10 years of schooling) | 3 (1.8) | 0 | 3 (3.4) |
| secondary school (usually 10 years of schooling) | 12 (7.1) | 3 (3.7) | 9 (10.2) |
| subject-related university entrance qualification | 16 (9.5) | 7 (8.6) | 9 (10.2) |
| general qualification for university entrance | 132 (78.1) | 67 (82.7) | 65 (73.9) |
| Current occupation [n (%)] | |||
| full-time employment | 55 (32.5) | 29 (35.8) | 26 (29.5) |
| part-time employment | 17 (10.1) | 7 (8.6) | 10 (11.4) |
| school | 6 (3.6) | 4 (4.9) | 2 (2.3) |
| vocational training/apprenticeship | 2 (1.2) | 0 | 2 (2.3) |
| studying at a university | 60 (35.5) | 27 (33.3) | 33 (37.5) |
| unemployed | 15 (8.9) | 6 (7.4) | 9 (10.2) |
| housewife/househusband | 1 (0.6) | 1 (1.2) | 0 |
| disability pension | 2 (1.2) | 0 | 2 (2.3) |
| retirement pension | 3 (1.8) | 2 (2.5) | 1 (1.1) |
| other | 8 (4.7) | 5 (6.2) | 3 (3.4) |
| AICA-S Score | T0 | T2 | ||||
|---|---|---|---|---|---|---|
| Total | IG | WCG | Total | IG | WCG | |
| Mean value | 12.46 | 12.36 | 12.53 | 8.98 | 6.79 | 11.00 |
| Standard deviation | 4.78 | 4.52 | 5.04 | 5.67 | 5.15 | 5.39 |
| Median | 12.50 | 13.00 | 12.00 | 8.00 | 5.00 | 10.25 |
| Mode | 12.50 | 12.50 | 10.50 | 5.50 | 2.00 | 6.00 |
| Minimum | 2.50 | 2.50 | 3.00 | 2.00 | 2.00 | 2.00 |
| Maximum | 27.00 | 23.00 | 27.00 | 27.00 | 22.50 | 27.00 |
| EQ-5D-5L Index Value | T0 | T2 | ||||
|---|---|---|---|---|---|---|
| Total | IG | WCG | Total | IG | WCG | |
| Mean value | 0.839 | 0.847 | 0.831 | 0.860 | 0.884 | 0.838 |
| Standard deviation | 0.161 | 0.143 | 0.176 | 0.154 | 0.122 | 0.176 |
| Median | 0.882 | 0.892 | 0.874 | 0.913 | 0.913 | 0.911 |
| Minimum | 0.130 | 0.300 | 0.130 | 0 | 0.460 | 0 |
| Maximum | 1 | 1 | 1 | 1 | 1 | 1 |
| Cost Categories | T0 | T2 | ||||||
|---|---|---|---|---|---|---|---|---|
| /Day Total [EUR] | /Day IG [EUR] | /Day WCG [EUR] | p-Value | /Day Total [EUR] | /Day IG [EUR] | /Day WCG [EUR] | p-Value | |
| Sickness benefits | 0.33 | 0 | 0.63 | 0.174 | 1.32 | 0 | 2.54 | 0.174 |
| Outpatient physician contacts | 1.68 | 1.67 | 1.69 | 0.609 | 1.75 | 1.89 | 1.62 | 0.867 |
| Hospital treatments | 2.64 | 2.22 | 3.02 | 0.366 | 1.29 | 0.39 | 2.12 | 0.601 |
| Medications | 0.75 | 0.12 | 1.34 | 0.200 | 2.37 | 3.31 | 1.50 | 0.910 |
| Remedies | 0.28 | 0.24 | 0.31 | 0.976 | 1.33 | 0.17 | 0.10 | 0.613 |
| Intervention costs | 0 | 0 | 0 | 0 | 0 | 11.11 | 0 | <0.001 |
| Sum | 5.67 | 4.25 | 6.98 | 0.953 | 12.19 | 16.88 | 7.88 | <0.001 |
| Cost Categories | T0 | T2 | ||||||
|---|---|---|---|---|---|---|---|---|
| /Day Total [EUR] | /Day IG [EUR] | /Day WCG [EUR] | p-Value | /Day Total [EUR] | /Day IG [EUR] | /Day WCG [EUR] | p-Value | |
| Incapacity to work | 3.07 | 1.11 | 4.88 | 0.288 | 2.94 | 0.48 | 5.21 | 0.177 |
| Reduction in earning capacity | 1.17 | 0.00 | 2.25 | 0.174 | 1.81 | 0.57 | 2.95 | 0.601 |
| Outpatient physician contacts | 1.76 | 1.75 | 1.77 | 0.609 | 1.83 | 1.98 | 1.69 | 0.959 |
| Hospital treatments | 2.78 | 3.03 | 2.55 | 0.361 | 0.96 | 0.29 | 1.57 | 0.606 |
| Rehabilitation | 1.01 | 1.37 | 0.69 | 0.279 | 0.92 | 1.91 | 0.0 | 0.139 |
| Medications | 0.85 | 0.18 | 1.46 | 0.095 | 4.06 | 6.09 | 2.20 | 0.900 |
| Remedies | 0.30 | 0.26 | 0.33 | 0.976 | 0.14 | 0.18 | 0.11 | 0.613 |
| Intervention costs | - | - | - | - | - | 11.11 | - | <0.001 |
| Sum | 10.94 | 7.68 | 13.93 | 0.532 | 17.99 | 22.61 | 13.73 | <0.001 |
| ICER | Perspective | |
|---|---|---|
| Statutory Health Insurance | Society | |
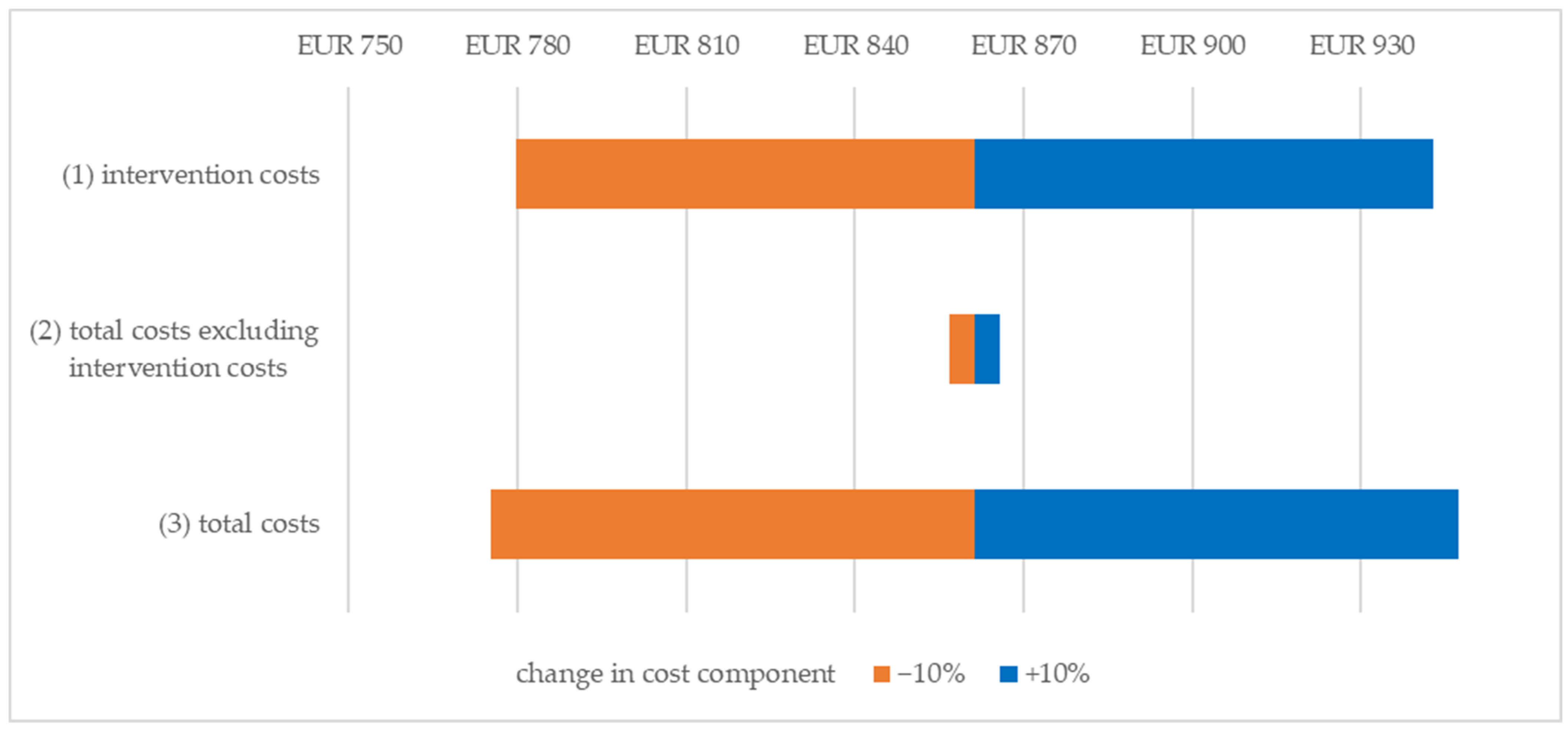
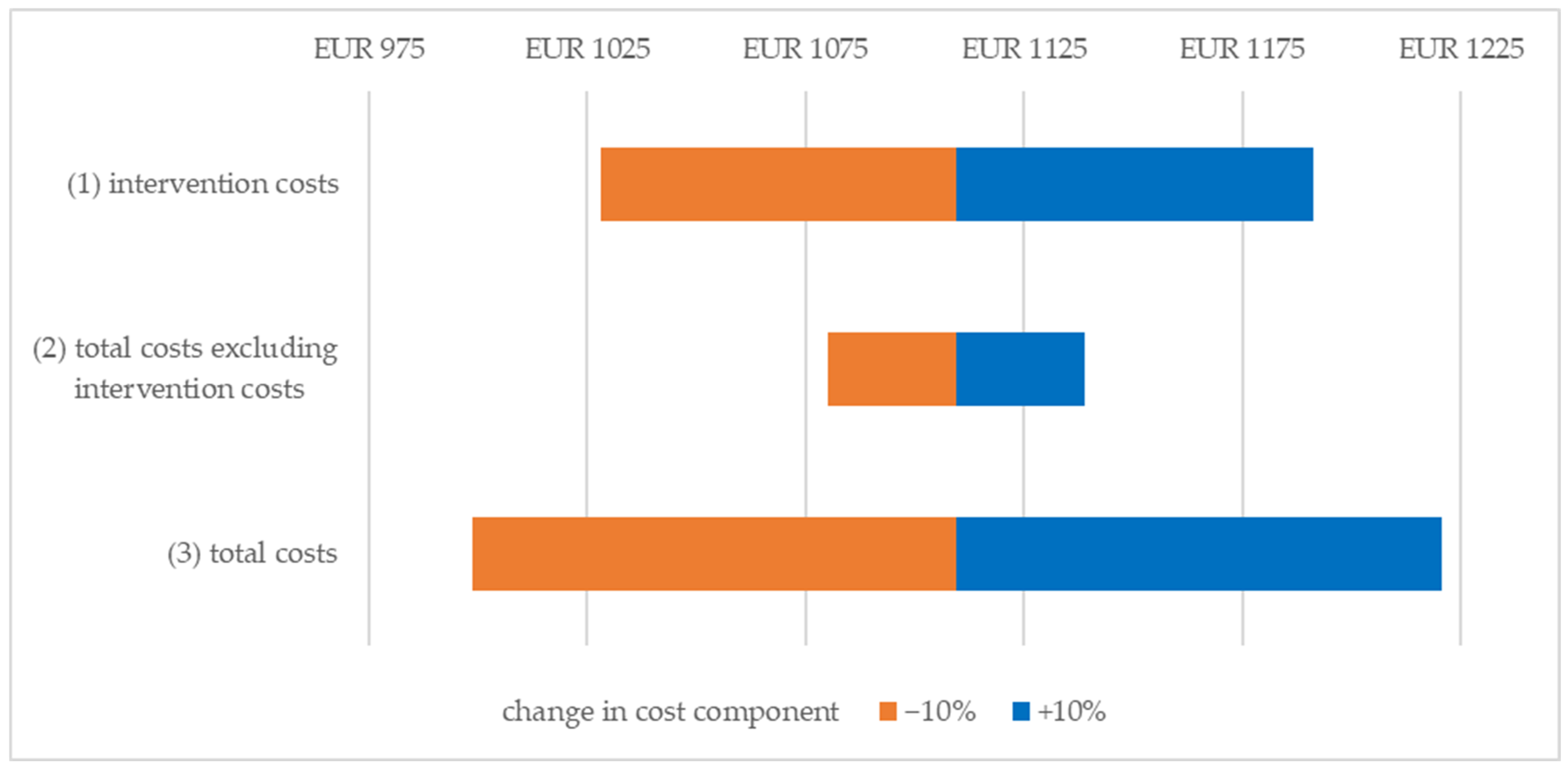
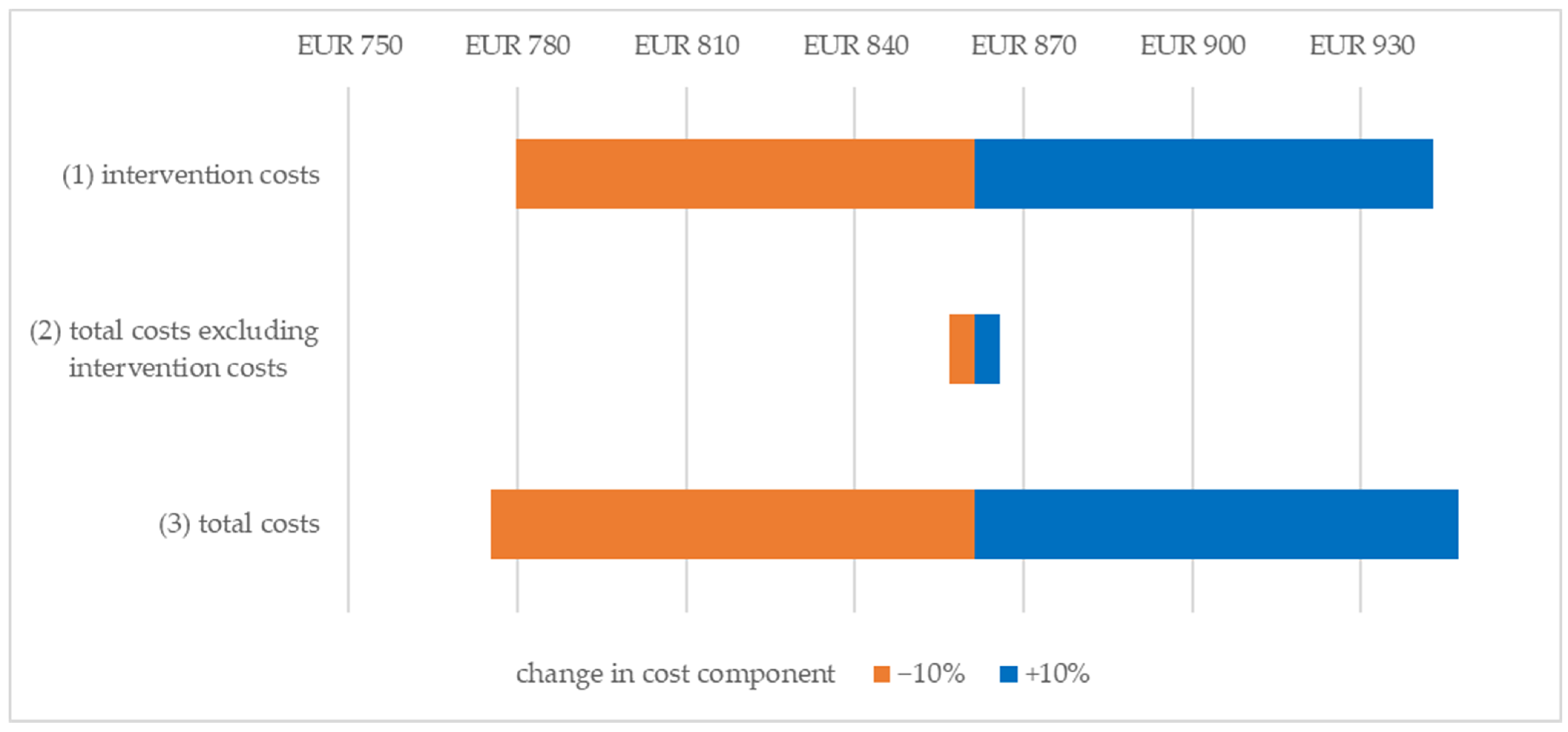
| Base case | EUR 861.30/PRC | EUR 1109.57/PRC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemann, A.; Hillerich, V.; Wasem, J.; Dieris-Hirche, J.; Bottel, L.; Pape, M.; Herpertz, S.; Timmesfeld, N.; Basten, J.; te Wildt, B.T.; et al. Health Economic Evaluation of an Online-Based Motivational Program to Reduce Problematic Media Use and Promote Treatment Motivation for Internet Use Disorder—Results of the OMPRIS Study. Int. J. Environ. Res. Public Health 2023, 20, 7144. https://doi.org/10.3390/ijerph20247144
Niemann A, Hillerich V, Wasem J, Dieris-Hirche J, Bottel L, Pape M, Herpertz S, Timmesfeld N, Basten J, te Wildt BT, et al. Health Economic Evaluation of an Online-Based Motivational Program to Reduce Problematic Media Use and Promote Treatment Motivation for Internet Use Disorder—Results of the OMPRIS Study. International Journal of Environmental Research and Public Health. 2023; 20(24):7144. https://doi.org/10.3390/ijerph20247144
Chicago/Turabian StyleNiemann, Anja, Vivienne Hillerich, Jürgen Wasem, Jan Dieris-Hirche, Laura Bottel, Magdalena Pape, Stephan Herpertz, Nina Timmesfeld, Jale Basten, Bert Theodor te Wildt, and et al. 2023. "Health Economic Evaluation of an Online-Based Motivational Program to Reduce Problematic Media Use and Promote Treatment Motivation for Internet Use Disorder—Results of the OMPRIS Study" International Journal of Environmental Research and Public Health 20, no. 24: 7144. https://doi.org/10.3390/ijerph20247144
APA StyleNiemann, A., Hillerich, V., Wasem, J., Dieris-Hirche, J., Bottel, L., Pape, M., Herpertz, S., Timmesfeld, N., Basten, J., te Wildt, B. T., Wölfling, K., Beckers, R., Henningsen, P., Neusser, S., & Neumann, A. (2023). Health Economic Evaluation of an Online-Based Motivational Program to Reduce Problematic Media Use and Promote Treatment Motivation for Internet Use Disorder—Results of the OMPRIS Study. International Journal of Environmental Research and Public Health, 20(24), 7144. https://doi.org/10.3390/ijerph20247144