1. Introduction
High-intensity interval training (HIIT) was initially developed for middle- and long-distance (track) runners with the aim of training at intensities close to competition speed and enhancing aerobic and anaerobic fitness [
1]. High-intensity interval training (HIIT) is defined as ‘near maximal’ efforts generally performed at an intensity that elicits at least 80% of the maximum oxygen consumption (VO
2max) or 90% of the maximum heart rate (HR
max), separated by periods of passive or active rest [
2,
3]. There is a growing consensus concerning the metabolic responses and physiological adaptations to HIIT. For instance, increased activity of mitochondrial enzymes is evident, and there is enhanced fat oxidation in the skeletal muscle [
4]. As a result, this training modality has gained popularity, also reaching individuals who exercise for health purposes and seek an activity with a good time–efficiency ratio.
There are HIIT protocols that manipulate the effort–pause relationship and that are performed in different formats (e.g., running in the sand, jumping, and body work) to facilitate the involvement in exercise, as opposed to the restrictions of the traditional ergometers, for example, on treadmills and bicycles [
5,
6]. Furthermore, a recent study used elastic resistance in HIIT and demonstrated that this modality can be potentially favorable for the development of cardiorespiratory fitness [
7]. Although elastic resistance can be used to perform HIIT, the ideal dimensions for prescribing HIIT using elastic resistance (i.e., prescription of intensity) remain unknown. In order to understand the prescription of HIIT using elastic resistance (EL-HIIE), it is necessary to better understand the acute cardiopulmonary responses to this exercise modality.
Researchers point out that rest intervals, intensity, and duration of work are variables that can be manipulated to prescribe different HIIT sessions [
8,
9]. Intensity can be controlled and individualized by specific running speed, percentage of HR
max, percentage of VO
2max, and rate of perceived exertion scale (RPE) [
8]. However, cardiopulmonary indicators should result from a cardiopulmonary exercise test (CPx) performed on a treadmill or cycle ergometer due to their objectivity, precision, and effectiveness in determining these physiological parameters for exercise prescription [
8]. The CPx is a gold-standard method that allows the determination of maximum physiological parameters (e.g., VO
2max, HR
max, maximum velocity, vVO
2max, and respiratory exchange ratio) and submaximal (e.g., ventilatory thresholds one and two) which are used in the determination of exercise intensity.
The VO
2max is dependent on the ergometer used due to the specificity of the movement [
10,
11]; in that regard, for a more accurate prescription of the intensity in the EL-HIIE, the cardiopulmonary test of exercise with elastic resistance can be used (CPxEL). The CPxEL has good reproducibility in evaluating maximal and submaximal cardiopulmonary parameters [
12]; however, it is important to check whether the cardiopulmonary parameters of the prescription are really equivalent to those found in the EL-HIIE session. Therefore, this study aims to evaluate the agreement between the cardiopulmonary parameters of the exercise session and the prescription parameters, based on a new proposal for a maximum incremental test, the CPxEL.
2. Materials and Methods
2.1. Subjects
The sample size was calculated using the G Power software program (version 3.1.4), by which a total number of 19 individuals was suggested, with statistical power (1-β) of 0.95 for the t test between two dependent means (corresponding pair), with an α-type error of 0.05 and a large effect size of 0.8. Twenty-two participants, including ten women and twelve men, participated in all experimental procedures (
Table 1). The procedures were approved by the Human Research Ethics Committee of the Federal University of Espírito Santo (CAAE 09109319200005542). The participants were required to read and sign an online informed-consent form containing all information about the study procedures, risks, and benefits. This study adopted as inclusion criteria a BMI (≥18 and ≤25 kg·m
−2), an age between 18 and 35 years, and physical independence (physical activity ≥150 min/week). Participants were excluded when there was cardiometabolic disease, use of dietary supplements or anabolic steroids, or suspected respiratory tract infections (for example, COVID-19). Participant characteristics are presented in
Table 1 and
Table 2.
2.2. Study Design
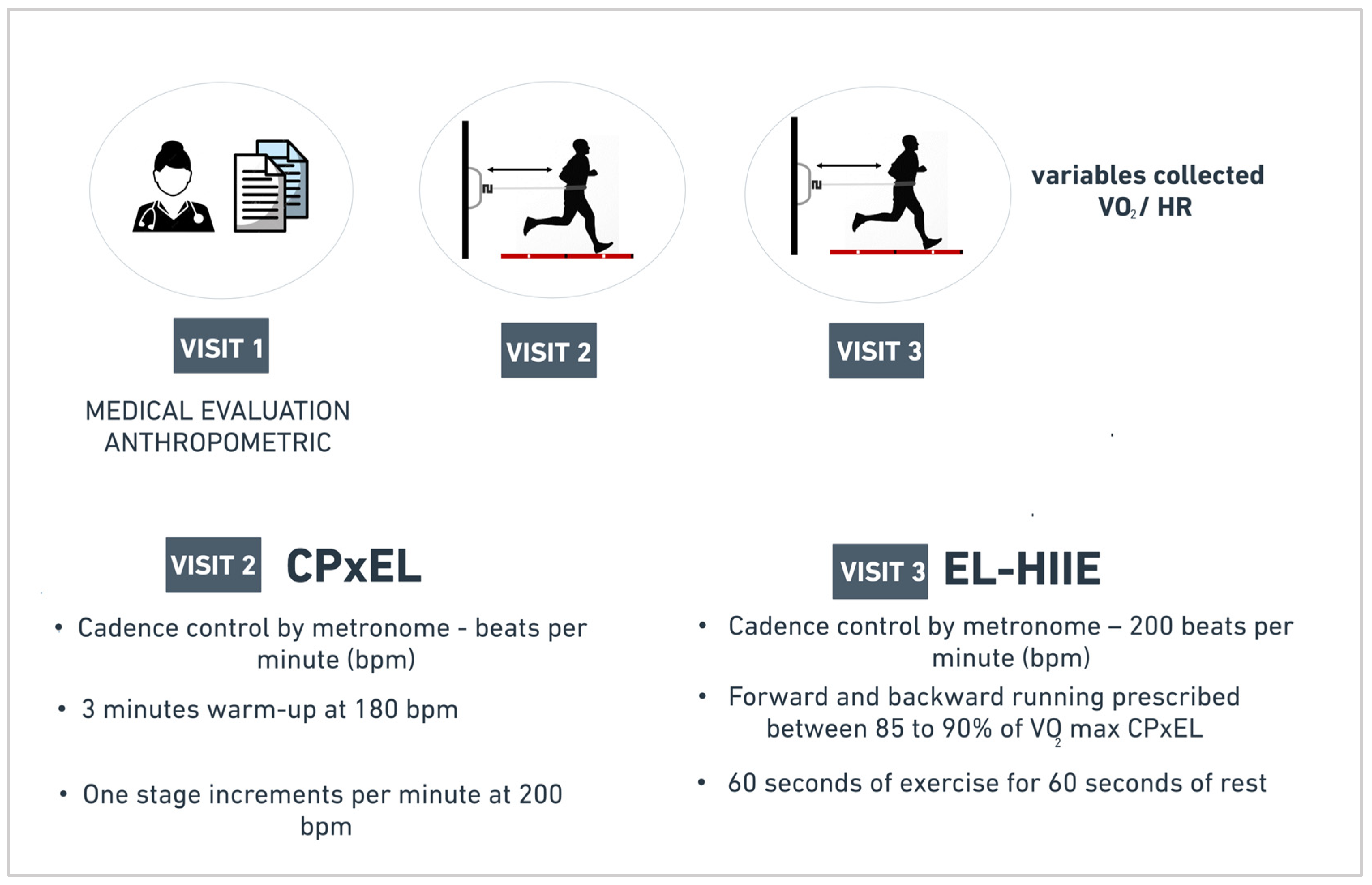
Participants visited the laboratory three times, with each visit separated by an interval of seven days, during morning hours (7:00 a.m. and 10:30 a.m.). Medical and anthropometric assessment were performed on the first visit. On the second visit, all participants performed the CPxEL until exhaustion to assess the maximal oxygen consumption and prescribed intensity of EL-HIIE. On the third visit, participants performed the EL-HIIE session (
Figure 1).
2.3. Cardiopulmonary Exercise Test with Elastic Resistance (CPxEL)
The CPxEL followed the protocol Gasparini Neto et al. (2022) validated; additional details are available in that source [
12]. The CPxEL was carried out to evaluate the maximum parameters and define the stage for the performance of the EL-HIIE. The test consisted of performing alternating steps back and forth against elastic resistance (Thera-band
® Tubing, Kuala Lumpur, Malaysia). The elastic resistance was attached to a polyamide military tactical belt (5 cm × 140 cm) inserted at the hip. Furthermore, the elastic resistance was attached to a load cell for force monitoring (200 kg; EMG System of Brazil, SP Ltd., Sao Paulo, Brazil). Force signals were collected by software (EMG Lab, version 1.03) at a sampling frequency of 1000 Hz. Data were analyzed using MatLab (MatLab; R2015a
®, MathWorks, Natick, MA, USA). The results of the strength values were represented by the average strength in kilograms (kg) in the last 30 s of each stage.
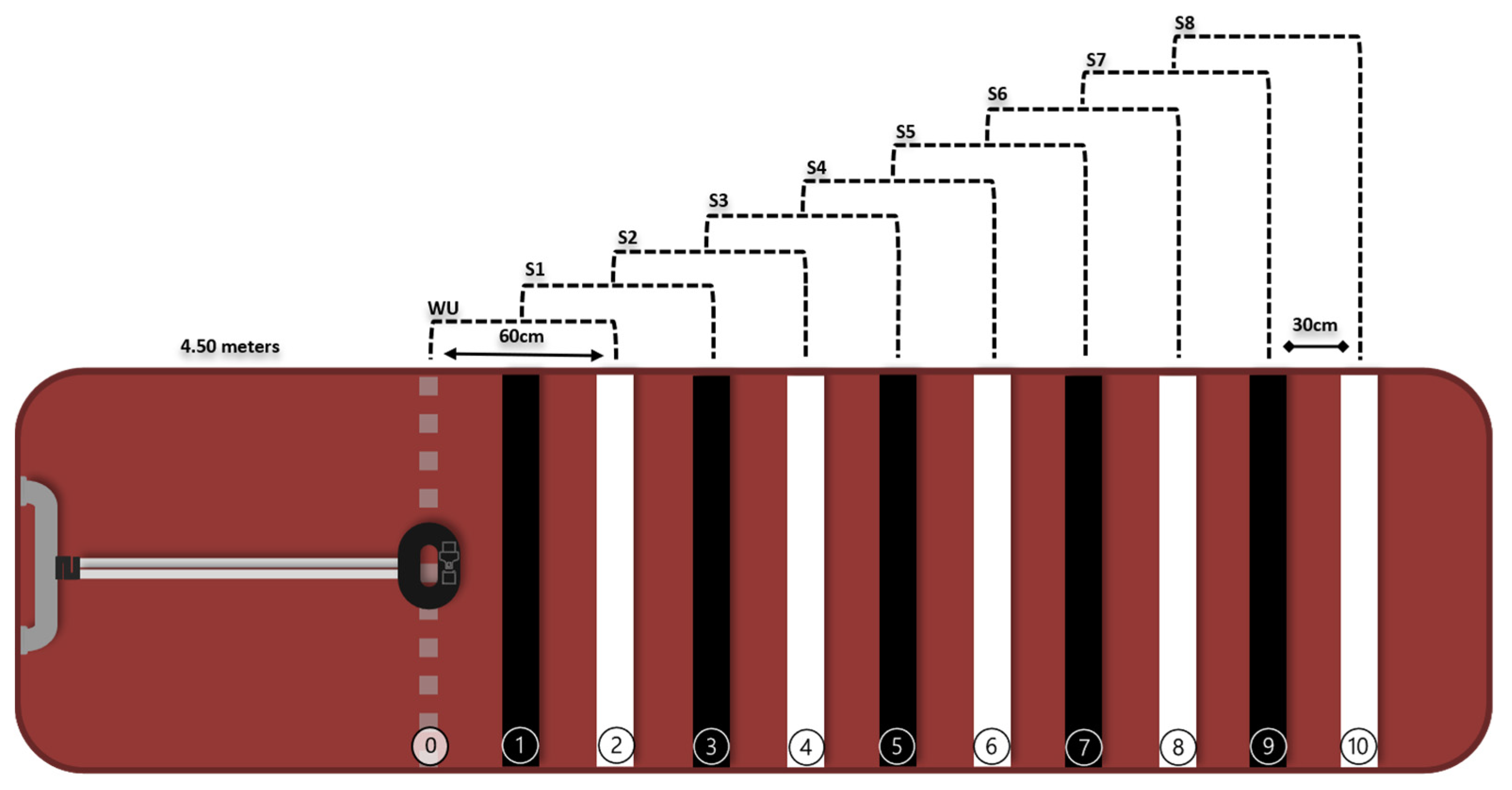
Initially, the participants performed a brief familiarization with the protocol. Then, the silicone face mask for gas collection and the T31 coded™ heart rate sensor (Polar Electro Oy, Kempele, Finland) were adjusted. The movements in the CPxEL stages were performed until the participant reached the stage that corresponded to his maximum. A 3-min warm-up was performed, from line zero to line 2, at a cadence of 180 bpm (beats per minute). Afterward, the protocol consisted of increments of 1 stage per minute, following a cadence of 200 bpm on an 8-stage rubber mat (
Figure 2). Participants were encouraged to follow a rhythm of 180 bpm (~90 steps/min) during the warm-up and 200 bpm (~100 steps/min) during the stages, following sounds emitted by a metronome app (Cifraclub
®, Belo Horizonte, Brazil) plugged into a speaker. Constant verbal encouragement was applied to maintain the rhythm during stages. If the participant reached the last stage, an increase of 10 (ten) bpm was incrementally added every minute until exhaustion.
The ventilatory variables, oxygen consumption (VO2), and carbon dioxide output (VCO2) were collected using a metabolic gas analyzer (model: Cortex Metamax 3B, Germany), and measured breath-by-breath and analyzed at 20 s averages by Metasoft™. Heart rate was monitored continuously and collected using the T31 coded™ heart-rate sensor (Polar Electro Oy, Kempele, Finland). Afterward, 20 s averages were extracted using the Metasoft program.
The criteria for defining the maximum test were voluntary exhaustion, reaching at least 90% of the maximum heart rate predicted by the formula (220-age), RER above 1.05, or BORG-CR10 rate of perceived exertion scale (RPE) value at the ‘very difficult’ intensity (7 onwards) [
13].
The ventilatory threshold 2 (VT2) was determined to verify how close the EL-HIIE session was to this intensity. Visual criteria were used, based on the response of ventilatory equivalents (VE/VO
2 and VE/VCO
2) and carbon dioxide tension (P
ETCO
2). Three evaluators independently and blindly evaluated the results, and the study employs the limit of agreement of at least two evaluators (ICC, 0.93). Identification of VT2 was based on the following criterion: the moment of the lowest point of the VE/VCO
2 with subsequent elevation beyond the moment of the gradual decline of the end-tidal carbon dioxide tension (P
ETCO
2) was considered [
14].
2.4. High-Intensity Interval Exercise with Elastic Resistance (EL-HIIE)
The session was prescribed at the stage corresponding to an intensity of 85–90% of the VO2max, as determined by the CPxEL. In EL-HIIE, the following were performed: 10 × 1 min (work):1 min (passive rest) (60 s protocol—adapted from Little et al. (2011)). The series consisted of alternating forward and backward movements against elastic resistance (Theraband® Tubing, Malaysia) at a cadence of 200 bpm, monitored by a metronome app (Cifraclub®, Brazil). Participants, as in the CPxEL, used the belt attached to the elastic tube (Silver tube, Thera-band® Tubing, Malaysia), the silicone face mask, and the T31 coded™ heart rate sensor (Polar Electro Oy, Kempele, Finland). Ventilatory variables (VO2 and VCO2) were collected using a metabolic gas analyzer (model Cortex Metamax 3B, Weil am Rhein, Germany) and measured breath-by-breath. Afterward, VO2peak (average of the last 10 s for each bout) and VO2average (average of the 60 s for each bout) were calculated.
Heart rate was monitored continuously by the T31 coded™ heart rate sensor (Polar Electro Oy, Kempele, Finland). Then, the HRpeak (average of the last 10 s for each bout) and HRaverage (average of the 60 s for each bout) were calculated.
2.5. Statistical Analysis
Data were expressed as mean and standard deviation (SD) and analyzed for normality (Shapiro–Wilk test) using the GraphPad Prism 9 software. To compare and evaluate the agreement between the cardiopulmonary responses (VO
2 and HR) elicited by EL-HIIE and those prescribed by CPxEL, we employed the paired
t-test and Bland–Altman analysis. One-way repeated-measures ANOVA and Tukey’s multiple comparison tests were employed to ascertain the distinctions between the peak and average values of VO
2 and HR during EL-HIIE, compared with the corresponding values obtained from the prescription provided by CPxEL. The
p values were exact, and statistical significance was defined as
p < 0.05. Cohen’s d effect size from an arbitrary scale was calculated and classified as trivial (0–0.19), small (0.20–0.49), moderate (0.50–0.79), or large (≥0.8) to determine the magnitude of differences [
15].
3. Results
3.1. CPxEL vs. EL-HIIE (Peak Values)
Prescription values for the CPxEL and peak values for the EL-HIIE are shown in
Table 3. The average stage performed during the EL-HIIE was stage 3, with an external load applied through elastic force averaging 66.6 ± 3.2% of the maximum load determined in the CPxEL. There was a statistical difference between the VO
2CPxEL and the VO
2session, with a small effect size (ES). The VO
2session was 5% higher than the VO
2CPxEL. Over the 10 min bout in the EL-HIIE, VO
2 remained at 147.6 s (2.46 min) in the prescription target range (≥85% VO
2max), in the following proportions: bout 1, 5.4 s; bout 2, 14.0 s; bout 3, 15.4 s; bout 4, 18.1 s; bout 5, 15.5 s; bout 6, 15.9 s; bout 7, 15.4 s; bout 8, 15.4 s; bout 9, 16.3 s; and bout 10, 17.2 s.
There was no statistical difference between the HR value of the prescription and that of the EL-HIIE. Over the 10 min bout in the EL-HIIE, HR remained at 125.3 s (2.08 min) in the prescription target range (≥85% VO2max), in the following proportions: bout 1, 2.2 s; bout 2, 5.4 s; bout 3, 10.0 s; bout 4, 12.7 s; bout 5, 14.3 s; bout 6, 15.9 s; bout 7, 17.7 s; bout 8, 18.6 s; bout 9, 19.0 s; and bout 10, 22.2 s.
In EL-HIIE, two participants reached a VO2 of VT2 as determined by CPxEL, six were 5.7% above VT2, and fourteen were 8.3% below VT2. In addition, one participant reached the HR of VT2 determined by CPxEL, seventeen were 6.8% below VT2, and four were 1.7% above VT2.
3.2. CPxEL vs. EL-HIIE (Average Values)
Prescription values of CpxEL and average values of 60 s EL-HIIE are shown in
Table 4. The VO
2 of the EL-HIIE average value was 30.4 ± 4.4 mL·kg
−1·min
−1, 74.8 ± 15.3% of the VO
2max. The VO
2session was 15% less than the VO
2CpxEL. There was a propensity of VO
2 stabilization from bout 3 onward.
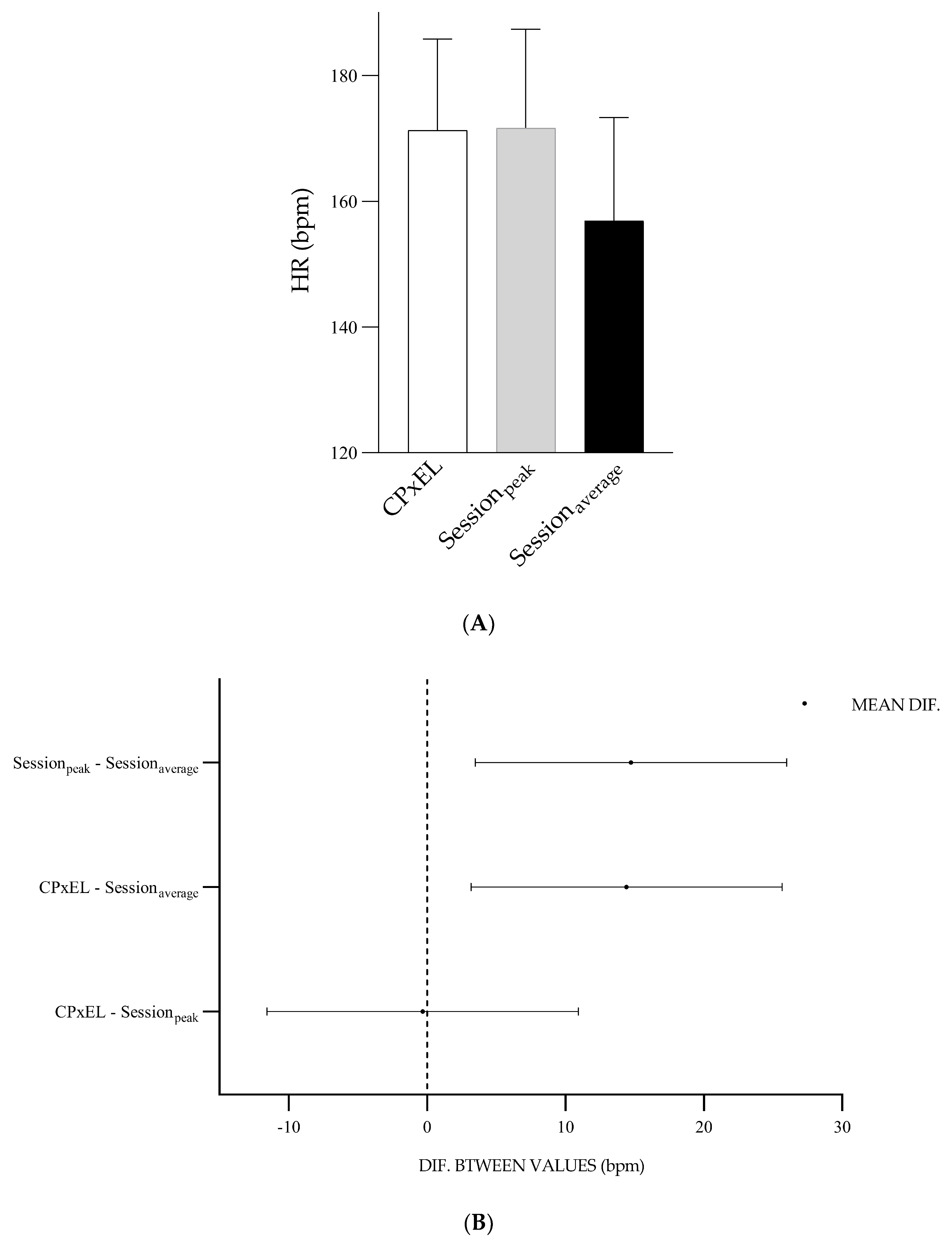
The average HR of the session was 157 ± 16 bpm, 84 ± 53.7% of HRmax. The HRsession was 8.4% less than the HRCpxEL. From bout 3, the average HR of the session showed a percentage of 82.3% of HRmax, increasing at the end of bout 10 to 89% of HRmax.
3.3. Bland–Altman Analysis
The mean (peak) difference between VO
2session and VO
2CpxEL was −1.7 mL·kg
−1·min
−1 with concordance limits of +4.8 to −8.3 mL·kg
−1. The mean (average) difference between VO
2CpxEL and VO
2session was 5.4 mL·kg
−1·min
−1 with concordance limits of +11.8 to −0.9 mL·kg
−1·min
−1 (
Figure 3).
The mean (peak) difference between HR
CpxEL and HR
session was 0.3 bpm with concordance limits of +16.3 to −16.9 bpm. The mean (average) difference between HR
CpxEL and HR
session was 14.4 bpm with concordance limits of +33.1 to −4.1 bpm (
Figure 3).
3.4. Difference between Prescription Parameters and Exercise Session Parameters
The VO
2CpxEL represented 88.1% of VO
2max, the VO
2session (peak), 92.6% of VO
2max, and the VO
2session (average), 74.8% of VO
2max. The distinction between the VO
2CPxEL and the VO
2session (peak) was −1.7 mL·kg
−1·min
−1,
p = 0.47. The distinction between VO
2CPxEL and VO
2session (average) was 5.4 mL·kg
−1·min
−1,
p = 0.00. The distinction between VO
2session (peak) and VO
2session (average) was 7.1 mL·kg
−1·min
−1,
p = 0.00 (
Figure 4).
The HR
CPxEL represented 91.9% of HR
max, the HR
session (peak), 92.1% of HR
max, and HR
session (average), 78.4% of HR
max. The distinction between HR
CPxEL and HR
session (peak) was −0.3 bpm,
p = 0.99. The distinction between HR
CPxEL and HR
session (average) was 14.4 bpm,
p = 0.005. The distinction between HR
session (peak) and HR
session (average) was 14.7 bpm,
p = 0.00 (
Figure 5).
4. Discussion
The present study aimed to assess the agreement between the cardiopulmonary variables of the EL-HIIE and the values used in a prescription based on the CPxEL. The significance of movement specificity in prescribing exercise intensity is well-recognized, as the measurement of VO
2 relies on factors such as the type of equipment (treadmill, cycle ergometer), the protocol employed, and the nature of effort exerted during the testing [
10].
Our main findings demonstrated a good agreement between the cardiopulmonary parameters of the EL-HIIE and the prescription parameters determined by the CPxEL. CPxEL was initially proposed to determine VO2max and ventilatory thresholds in healthy individuals, and our results highlight the importance of its use in prescribing correctly a 10 × 1:1 min protocol in the EL-HIIE at an intensity of 88.1 ± 5.8% of VO2max.
This study defined the exercise intensity prescription parameter according to the reference already used in the literature (≥85% of VO
2max) [
16,
17]. In these previously mentioned studies, the individuals exercised within a workload corresponding to the submaximal fraction of the VO
2max, while the HR, lactate production, speed, power, and classification of the perceived exertion during the execution of the exercise were monitored. Given the few data sources available in the literature, our study directly monitored VO
2 in EL-HIIE. Therefore, it was possible to confirm the good agreement between the VO
2session (peak) of EL-HIIE and the VO
2 prescribed by CPxEL.
The present study, in addition, monitored HR during EL-HIIE. In sports practice, the use of this metric is frequent, although the literature points out that there may be limitations, mainly due to the delay in changes in the heart rate at the beginning of the exercise [
18]. Our findings demonstrated good agreement between the HR
session (peak) of the exercise session and the HR CPxEL prescription. Therefore, this evidence points out that monitoring HR
session (peak) in EL-HIIE ensured that participants were at an intensity equivalent to the specific test prescription (CPxEL).
Although the main focus of prescribing and monitoring in the EL-HIIE was not the external load, it was possible to identify the average load used during the exercise execution (66.6% of the peak force reached in the CPxEL), as continuously measured via a load cell. The load used in the EL-HIIE is similar to the prescription parameters established in the literature. In the study by Hood et al. (2011), a HIIT exercise session was performed on a cycle ergometer, prescribed at ∼60% of the peak power reached during the VO
2peak test. The bouts in this study provoked a cardiopulmonary effort corresponding to ∼80% to 95% of HR reserve [
19]. The cardiopulmonary results found in EL-HIIE (∼84% to 92% HR
max), from 66.6% of peak force, confirm that the exercise protocol of our study was performed at high intensity.
Our findings, moreover, indicated lower values of HR and VO
2 in the average values compared to the peak values. This result was expected, since lower average values of HR and VO
2 can be attributed to the passive recovery interval of our protocol. The present study agrees with a previous study that observed higher average values of HR and VO
2 in active intervals in HIIT with an effort–pause ratio of 1:1 [
20].
In EL-HIIE, participants remained for approximately 24.6% of the total exercise time within the prescription target zone (≥85% VO
2max). Comparing our results with the literature is difficult, since the intensity and duration of HIIT exercise differ significantly. In addition, few studies show how long participants remain in the prescription target zone. Furthermore, to the best of our knowledge, this was the first study to investigate the agreement between the CPxEL prescription’s cardiopulmonary parameters and the EL-HIIE session’s parameters. On the other hand, future research with EL-HIIE can manipulate the duration of bouts and recovery intervals, such as the high-intensity decreasing interval training (HIDIT) protocol performed by cyclists [
21]. This protocol is characterized by bout intervals varying between long and short, starting with 3 min and ending with 30 s. The HIDIT performed in cyclists showed a longer time of high-intensity exercise, which could be a strategy for EL-HIIE. The 60 s:60 s protocol performed in the present study was a strategy to ensure an exercise intervention capable of being performed by healthy individuals and clinical populations [
22].
Some limitations need to be pointed out: our study evaluated only healthy and eutrophic young individuals, and these findings cannot represent the behavior of subjects with different levels of physical conditioning, like obese and sedentary individuals. Another limitation was the mixed sample (men and women), because men and women can have up to a 30% difference for VO2max, but another side of the question is that a mixed sample increases the ecological validity of results. Despite these limitations, it is essential to highlight that our proposal was safe and presented good agreement between CPxEL and EL-HIIE. Thus, we encourage studies to apply our protocol to different populations and on a large scale to understand the better application of these findings in daily life and in longitudinal exercise prescription of physical exercise in different intensity domains.
Although it is not the primary outcome of this research, there is interest in the scientific literature on multicomponent training modalities. This modality offers a combination of physical capabilities (muscle strength, cardiorespiratory endurance, balance, and flexibility) in the same exercise session [
23,
24]. Considering that EL-HIIE can be a potential stimulus for developing cardiorespiratory fitness and lower-limb strength in young, active individuals [
7], future research may investigate whether EL-HIIE can be a multicomponent exercise strategy applied in different populations.


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}