

Feasibility and Outcomes of Meta Salud Diabetes Behavioral Health Intervention: A Pilot Study of a Community Health Worker-Administered Educational Intervention to Prevent Cardiovascular Disease and Its Complications among Hispanic Patients with Type-2 Diabetes

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sites
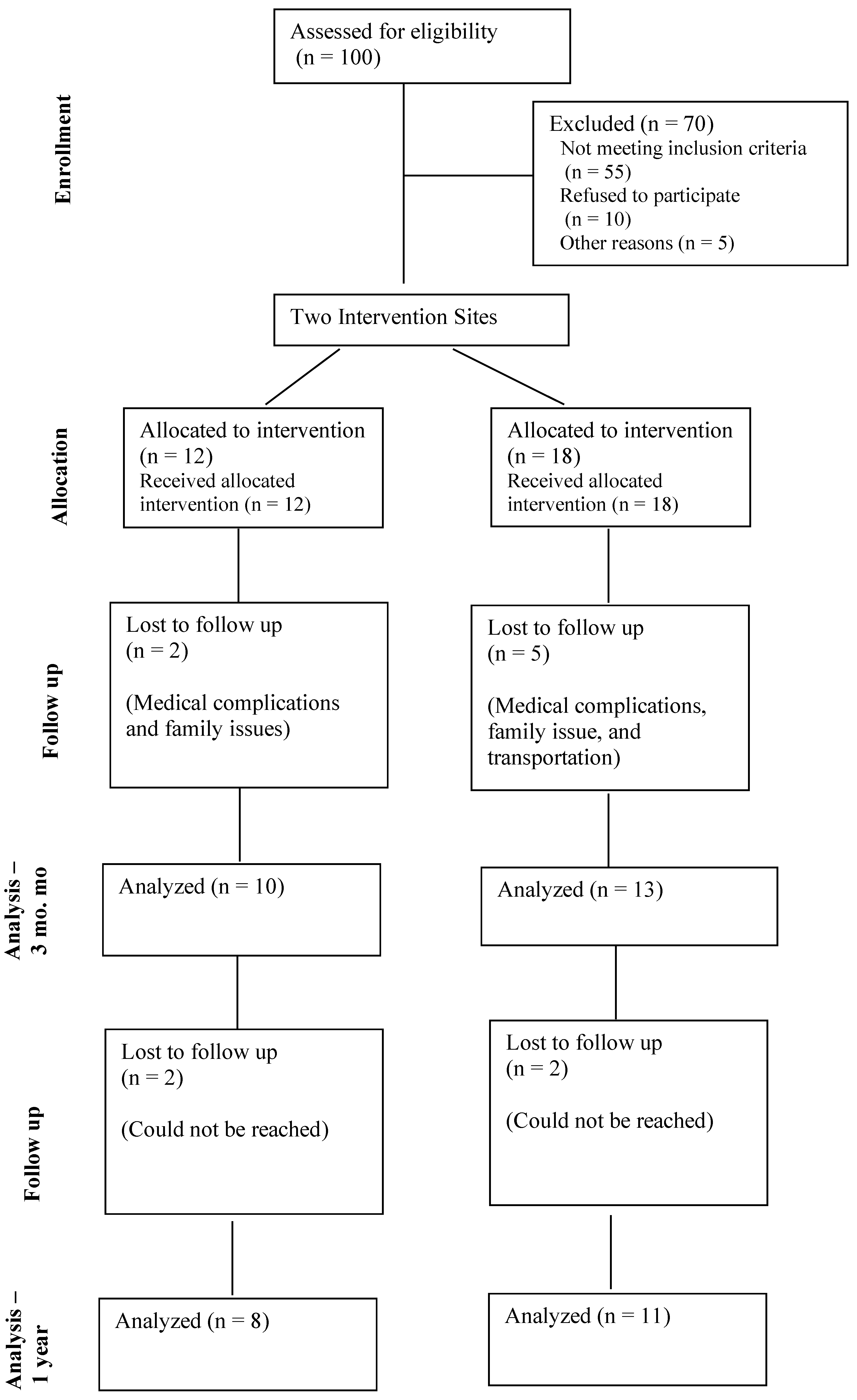
2.2. Participant Eligibility and Recruitment
2.3. Intervention and Curriculum
2.4. Outcomes and Measures
2.4.1. Implementation Science Outcome
2.4.2. Clinical Outcomes
2.4.3. Data Collection and Management
2.4.4. Statistical Analyses
3. Results
4. Discussion
Limitation and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.Y.M.; Carlsson, N.P.; Colditz, G.A.; Chang, S.-H. The Burden of Obesity on Diabetes in the United States: Medical Expenditure Panel Survey, 2008 to 2012. Value Health 2017, 20, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.J.; Kanaya, A.M.; Araneta, M.R.G.; Saydah, S.H.; Kahn, H.S.; Gregg, E.W.; Fujimoto, W.Y.; Imperatore, G. Prevalence of Diabetes by Race and Ethnicity in the United States, 2011–2016. JAMA 2019, 322, 2389–2398. [Google Scholar] [CrossRef] [PubMed]
- Mendola, N.D.; Chen, T.-C.; Gu, Q.; Eberhardt, M.S.; Saydah, S. Prevalence of Total, Diagnosed, and Undiagnosed Diabetes Among Adults: United States, 2013–2016. NCHS Data Brief 2018, 319, 1–8. [Google Scholar]
- Mansour, O.; Golden, S.H.; Yeh, H.-C. Disparities in mortality among adults with and without diabetes by sex and race. J. Diabetes Complicat. 2020, 34, 107496. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Data and Statistics. 2018. Available online: https://www.cdc.gov/diabetes/data/ (accessed on 15 August 2022).
- Schneiderman, N.; Llabre, M.; Cowie, C.C.; Barnhart, J.; Carnethon, M.; Gallo, L.C.; Giachello, A.L.; Heiss, G.; Kaplan, R.C.; LaVange, L.M.; et al. Prevalence of diabetes among Hispanics/Latinos from diverse backgrounds: The Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Diabetes Care 2014, 37, 2233–2239. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Pirzada, A.; Talavera, G.A. Cardiovascular disease risk factors in the Hispanic/Latino population: Lessons from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prog. Cardiovasc. Dis. 2014, 57, 230–236. [Google Scholar] [CrossRef]
- McCurley, J.L.; Gutierrez, A.P.; Gallo, L.C. Diabetes Prevention in U.S. Hispanic Adults: A Systematic Review of Culturally Tailored Interventions. Am. J. Prev. Med. 2017, 52, 519–529. [Google Scholar] [CrossRef]
- Viramontes, O.; Swendeman, D.; Moreno, G. Efficacy of Behavioral Interventions on Biological Outcomes for Cardiovascular Disease Risk Reduction among Latinos: A Review of the Literature. J. Racial Ethn. Health Disparities 2017, 4, 418–424. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases, 2013–2020; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]
- Rosales, C.B.; Denman, C.A.; Bell, M.L.; Cornejo, E.; Ingram, M.; Del Carmen Castro Vásquez, M.; Gonzalez-Fagoaga, J.E.; Aceves, B.; Nuño, T.; Anderson, E.J.; et al. Meta Salud Diabetes for cardiovascular disease prevention in Mexico: A cluster-randomized behavioural clinical trial. Int. J. Epidemiol. 2021, 50, 1272–1282. [Google Scholar] [CrossRef]
- Staten, L.K.; Scheu, L.L.; Bronson, D.; Peña, V.; Elenes, J. Pasos Adelante: The effectiveness of a community-based chronic disease prevention program. Prev. Chronic Dis. 2005, 2, A18. [Google Scholar] [PubMed]
- Denman, C.A.; Rosales, C.; Cornejo, E.; Bell, M.L.; Munguía, D.; Zepeda, T.; Carvajal, S.; Guernsey de Zapien, J. Evaluation of the community-based chronic disease prevention program Meta Salud in Northern Mexico, 2011–2012. Prev. Chronic Dis. 2014, 11, E154. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sabo, S.; Denman Champion, C.; Bell, M.L.; Cornejo Vucovich, E.; Ingram, M.; Valenica, C.; Castro Vasquez, M.D.C.; Gonzalez-Fagoaga, E.; Geurnsey de Zapien, J.; Rosales, C.B. Meta Salud Diabetes study protocol: A cluster-randomised trial to reduce cardiovascular risk among a diabetic population of Mexico. BMJ Open 2018, 8, e020762. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. American Community Survey 2017-2021 5-Year Data Release. Available online: https://www.census.gov/newsroom/press-kits/2022/acs-5-year.html (accessed on 1 September 2022).
- Karsh, B.-T. Beyond usability: Designing effective technology implementation systems to promote patient safety. Qual. Saf. Health Care 2004, 13, 388–394. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Revicki, D.A.; Kleinman, L.; Cella, D. A history of health-related quality of life outcomes in psychiatry. Dialogues Clin. Neurosci. 2014, 16, 127–135. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Anderson, B.J.; Lohrer, P.A.; Welch, G.; Jacobson, A.M.; Aponte, J.E.; Schwartz, C.E. Assessment of diabetes-related distress. Diabetes Care 1995, 18, 754–760. [Google Scholar] [CrossRef]
- Hildebrand, J.A.; Billimek, J.; Lee, J.A.; Sorkin, D.H.; Olshansky, E.F.; Clancy, S.L.; Evangelista, L.S. Effect of diabetes self-management education on glycemic control in Latino adults with type 2 diabetes: A systematic review and meta-analysis. Patient Educ. Couns. 2020, 103, 266–275. [Google Scholar] [CrossRef]
- Whittemore, R. Culturally competent interventions for Hispanic adults with type 2 diabetes: A systematic review. J. Transcult. Nurs. 2007, 18, 157–166. [Google Scholar] [CrossRef]
- Flores-Luevano, S.; Pacheco, M.; Shokar, G.S.; Dwivedi, A.K.; Shokar, N.K. Impact of a Culturally Tailored Diabetes Education and Empowerment Program in a Mexican American Population Along the US/Mexico Border: A Pragmatic Study. J. Clin. Med. Res. 2020, 12, 517–529. [Google Scholar] [CrossRef]
- McEwen, M.M.; Pasvogel, A.; Gallegos, G.; Barrera, L. Type 2 diabetes self-management social support intervention at the U.S.-Mexico border. Public Health Nurs. 2010, 27, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Joachim-Célestin, M.; Gamboa-Maldonado, T.; Dos Santos, H.; Montgomery, S.B. Delivering the Same Intervention to Hispanic/Latinos with Pre-diabetes and Diabetes. Early Evidence of Success in a Longitudinal Mixed Method Study. Inquiry 2021, 58, 1–19. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Sr.; Grundy, S.; Sullivan, L.M.; Wilson, P.; CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA 2001, 286, 180–187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Participant Characteristics | All (N = 30) |
|---|---|
| Age (years), mean (SD) | 61.2 (8.2) |
| Gender, n (%) | |
| Female | 21 (70.0) |
| Males | 9 (30.0) |
| Education (years), mean (SD) | 11.6 (4.4) |
| Birth Place, n (%) | |
| Arizona | 3 (10.0) |
| Other state/country | 27 (90.0) |
| Civil Status, n (%) | |
| Married or partnered | 19 (63.3) |
| Nonmarried/partnered | 11 (36.7) |
| Annual Income, n (%) | |
| ≤12,000 | 11 (36.7) |
| 12,001–20,000 | 7 (23.3) |
| 20,001–50,000 | 7 (23.3) |
| ≥60,001 | 2 (7.4) |
| Diabetes Status, n (%) | |
| Diabetes | 26 (86.7) |
| Prediabetes | 4 (13.3) |
| Previously Diagnosed with CVD, n (%) | |
| Yes | 8 (26.7) |
| No | 22 (73.3) |
| Medication for diabetes as prescribed, n (%) | |
| Yes | 28 (93.3) |
| No | 2 (6.7) |
| Insured, n (%) | |
| Yes | 29 (96.7) |
| No | 1 (3.3) |
| Current Drinking, n (%) | |
| None | 19 (63.3) |
| 1–4 times/week | 3 (10.0) |
| 1–3 times/month | 4 (13.3) |
| 1–11 times/year | 4 (13.3) |
| Variable | Time | Unadjusted Mean (SD) | p-Value a | Adjusted b Mean (SD) | p-Value |
|---|---|---|---|---|---|
| CVD Risk | Baseline | 20.3(12.1) | |||
| 3 months | 18.7 (12.8) | ||||
| Difference (95% CI) | −1.8 (−4.4, 0.8) | 0.17 | −2.5 (−5.3, 0.1) | 0.06 | |
| HbA1c, (%) | Baseline | 7.06(0.3) | |||
| 3 months | 6.8(0.3) | - | |||
| Difference a (95% CI) | −0.3 (−0.6, 0.1) | 0.17 | −0.4 (−0.8, 0.1) | 0.09 | |
| 12 months | 6.3(0.3) | ||||
| Difference b (95% CI) | −0.5 (−0.9, −0.1) | 0.02 | −0.5 (−0.1, −0.0) | 0.05 | |
| Blood Glucose, (mg/dL) | Baseline | 158.1(10.6) | - | ||
| 3 months | 159.2(12.3) | - | |||
| Difference a (95% CI) | 1.1 (−23.7 25.9) | 0.93 | 4.9 (−22.9, 32.7) | 0.73 | |
| 12 months | 145.1(13.2) | ||||
| Difference b (95% CI) | −14.0 (−41.9, 13.8) | 0.32 | −18.9 (−50.4, 12.7) | 0.24 | |
| Average Systolic Pressure c, (mmHg) | Baseline | 132.1(2.5) | - | ||
| 3 months | 126.0(2.9) | - | |||
| Difference a (95% CI) | −6.1 (−12.0, −0.22) | 0.04 | −6.7 (−13.1, −0.4) | 0.04 | |
| 12 months | 122.6(3.2) | ||||
| Difference b (95% CI) | −3.4 (−10.1, 3.3) | 0.32 | −1.8 (−9.1, 5.4) | 0.62 | |
| Average Diastolic Pressure c (mmHg) | Baseline | 82.9(1.5) | - | ||
| 3 months | 79.6(1.7) | - | |||
| Difference (95% CI) | −3.3 (−6.4, −0.1) | 0.04 | −3.0 (−6.6, 0.6) | 0.1 | |
| 12 months | 77.6(1.9) | ||||
| Difference b (95% CI) | −2.0 (−5.5, 1.6) | 0.28 | −1.8 (−5.9, 2.4) | 0.4 | |
| Total Cholesterol, (mg/dL) | Baseline | 159.7(6.2) | - | ||
| 3 months | 158.7(6.8) | - | |||
| Difference a (95% CI) | −1.0 (−11.6, 9.6) | 0.85 | −3.9 (−15.1, 7.3) | 0.5 | |
| 12 months | 153.9(7.2) | ||||
| Difference b (95% CI) | −4.7 (−16.5, 7.0) | 0.43 | −8.1 (−20.7, 4.5) | 0.21 | |
| HDL Cholesterol, (mg/dL) | Baseline | 44.3(1.9) | |||
| 3 months | 44.3(2.1) | ||||
| Difference (95% CI) | −0.06 (−3.2, 3.4) | 0.97 | −0.4 (−3.9, 3.1) | 0.81 | |
| 12 months | 44.1(2.2) | ||||
| Difference b (95% CI) | −0.2 (−3.6, 3.3) | 0.92 | −0.04 (−3.9, 3.9) | 0.99 | |
| LDL Cholesterol, (mg/dL) | Baseline | 71.8(6.0) | |||
| 3 months | 71.3(6.5) | ||||
| Difference (95% CI) | −0.5 (−9.7, 8.7) | 0.91 | −1.5 (−12.2, 9.2) | 0.79 | |
| 12 months | 73.7(6.8) | ||||
| Difference (95% CI) | 2.4 (−8.1, 12.9) | 0.66 | 0.2 (−12.4, 12.7) | 0.98 | |
| Triglycerides, (mg/dL) | Baseline | 214.6(18.4) | |||
| 3 months | 241.4(21.2) | ||||
| Difference (95% CI) | 26.7 (−15.0, 68.5) | 0.21 | 18.8 (−27.0, 64.6) | 0.42 | |
| 12 months | 184.2(22.8) | ||||
| Difference (95% CI) | −57.1 (−104.0, −10.3) | 0.02 | −71.4 (−123.1, −19.7) | 0.01 | |
| Anthropometrics | |||||
| BMI, (kg/m2) | Baseline | 32.1(1.0) | |||
| 3 months | 32.8(1.1) | ||||
| Difference (95% CI) | 0.7 (−0.9, 2.3) | 0.39 | 0.8 (−1.0, 2.7) | 0.36 | |
| 12 months | 32.7(1.1) | ||||
| Difference (95% CI) | −0.1 (−1.9, 1.6) | 0.88 | −0.1 (−2.2, 1.9) | 0.9 | |
| Average Weight c, (lbs) | Baseline | 189.1(7.3) | |||
| 3 months | 194.1(7.7) | ||||
| Difference (95% CI) | 5.0 (−4.0 13.9) | 0.28 | 4.5 (−5.9, 14.8) | 0.4 | |
| 12 months | 193.4(7.9) | ||||
| Difference (95% CI) | −0.6 (−10.5, 9.2) | 0.90 | −0.4 (−12.0, 11.2) | 0.95 | |
| Average Waist c, (in) | Baseline | 43.9(1.0) | |||
| 3 months | 43.5(1.0) | ||||
| Difference (95% CI) | −0.4 (−1.8, 1.0) | 0.55 | −0.1 (−1.5, 1.3) | 0.88 | |
| 12 months | 43.8(1.0) | ||||
| Difference (95% CI) | 0.3 (−1.1, 1.7) | 0.66 | 0.3 (−1.2, 1.9) | 0.66 |
| Variable | Time | Unadjusted Mean (SD) | p-Value a | Adjusted b Mean (SD) | p-Value |
|---|---|---|---|---|---|
| Physical Activity | |||||
| Moderate Physical Activity (min/week) | Baseline | 492.2(112.0) | |||
| 3 months | 525.7(133.8) | ||||
| Difference (95% CI) | 33.5 (−228.6, 295.8) | 0.80 | 39.5 (−260.0, 339.0) | 0.80 | |
| Time Seated (min/day) | Baseline | 229(30.0) | |||
| 3 months | 194.9(36.0) | ||||
| Difference (95% CI) | −34.1 (−104.3, 36.1) | 0.34 | −9.4 (−86.7, 68.0) | 0.81 | |
| Diet | |||||
| Sweet Beverages (portions in mL) | Baseline | 0.9(0.2) | |||
| 3 months | 0.1(0.3) | ||||
| Difference (95% CI) | −0.8 (−1.5, −0.1) | 0.01 | −0.5 (−0.9, −0.2) | 0.002 | |
| Vegetable Consumption (portions per day) | Baseline | 1.7(0.3) | |||
| 3 months | 1.7(0.3) | ||||
| Difference (95% CI) | 0.01 (−0.6, 0.7) | 0.93 | −0.2 (−0.9, 0.6) | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuño, T.; Torres, M.R.; Soto, S.; Sepulveda, R.; Aceves, B.; Rosales, C.B. Feasibility and Outcomes of Meta Salud Diabetes Behavioral Health Intervention: A Pilot Study of a Community Health Worker-Administered Educational Intervention to Prevent Cardiovascular Disease and Its Complications among Hispanic Patients with Type-2 Diabetes. Int. J. Environ. Res. Public Health 2023, 20, 6968. https://doi.org/10.3390/ijerph20216968
Nuño T, Torres MR, Soto S, Sepulveda R, Aceves B, Rosales CB. Feasibility and Outcomes of Meta Salud Diabetes Behavioral Health Intervention: A Pilot Study of a Community Health Worker-Administered Educational Intervention to Prevent Cardiovascular Disease and Its Complications among Hispanic Patients with Type-2 Diabetes. International Journal of Environmental Research and Public Health. 2023; 20(21):6968. https://doi.org/10.3390/ijerph20216968
Chicago/Turabian StyleNuño, Tomas, Maria Rocio Torres, Sheila Soto, Refugio Sepulveda, Benjamin Aceves, and Cecilia Ballesteros Rosales. 2023. "Feasibility and Outcomes of Meta Salud Diabetes Behavioral Health Intervention: A Pilot Study of a Community Health Worker-Administered Educational Intervention to Prevent Cardiovascular Disease and Its Complications among Hispanic Patients with Type-2 Diabetes" International Journal of Environmental Research and Public Health 20, no. 21: 6968. https://doi.org/10.3390/ijerph20216968
APA StyleNuño, T., Torres, M. R., Soto, S., Sepulveda, R., Aceves, B., & Rosales, C. B. (2023). Feasibility and Outcomes of Meta Salud Diabetes Behavioral Health Intervention: A Pilot Study of a Community Health Worker-Administered Educational Intervention to Prevent Cardiovascular Disease and Its Complications among Hispanic Patients with Type-2 Diabetes. International Journal of Environmental Research and Public Health, 20(21), 6968. https://doi.org/10.3390/ijerph20216968