
Trends of Exclusive Breastfeeding Practices and Its Determinants in Tanzania from 1999 to 2016

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Area
2.3. Data Source
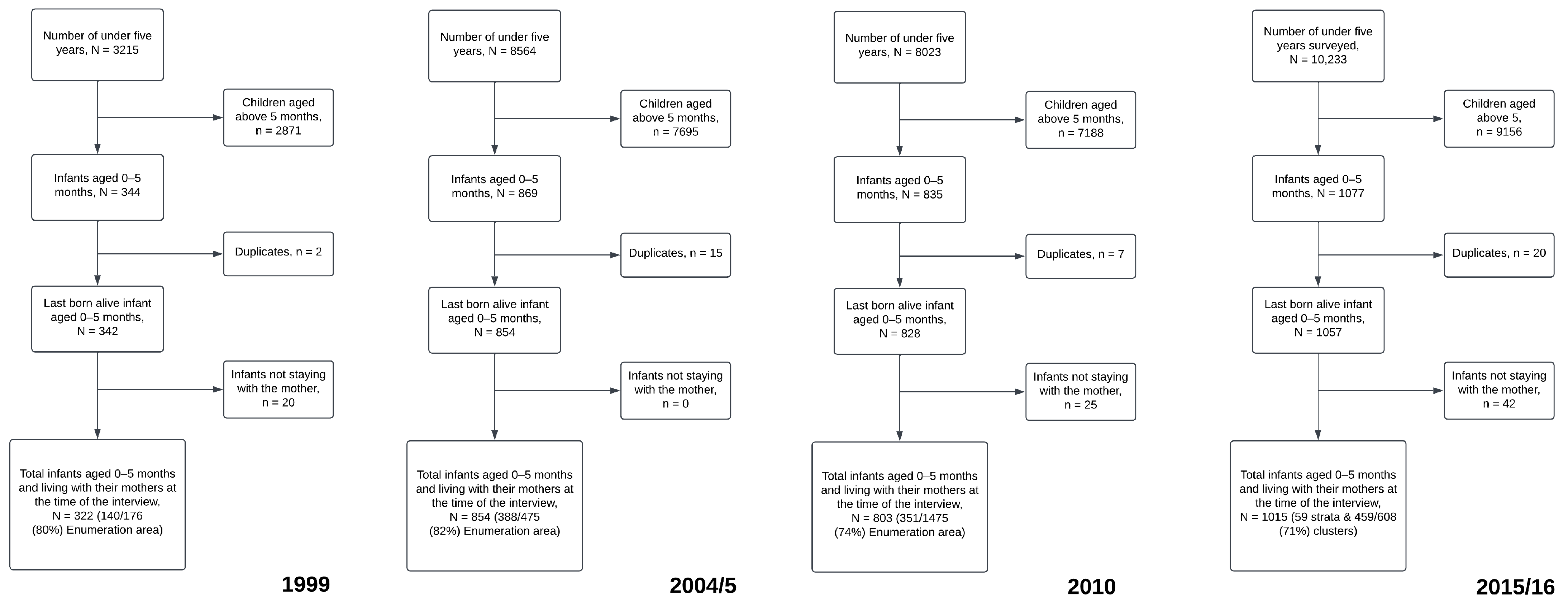
2.4. Study Participants and Sampling Procedure
2.5. Study Variables
2.5.1. Dependent Variable
2.5.2. Exposure Variables
2.6. Statistical Methods
2.6.1. Background Characteristics
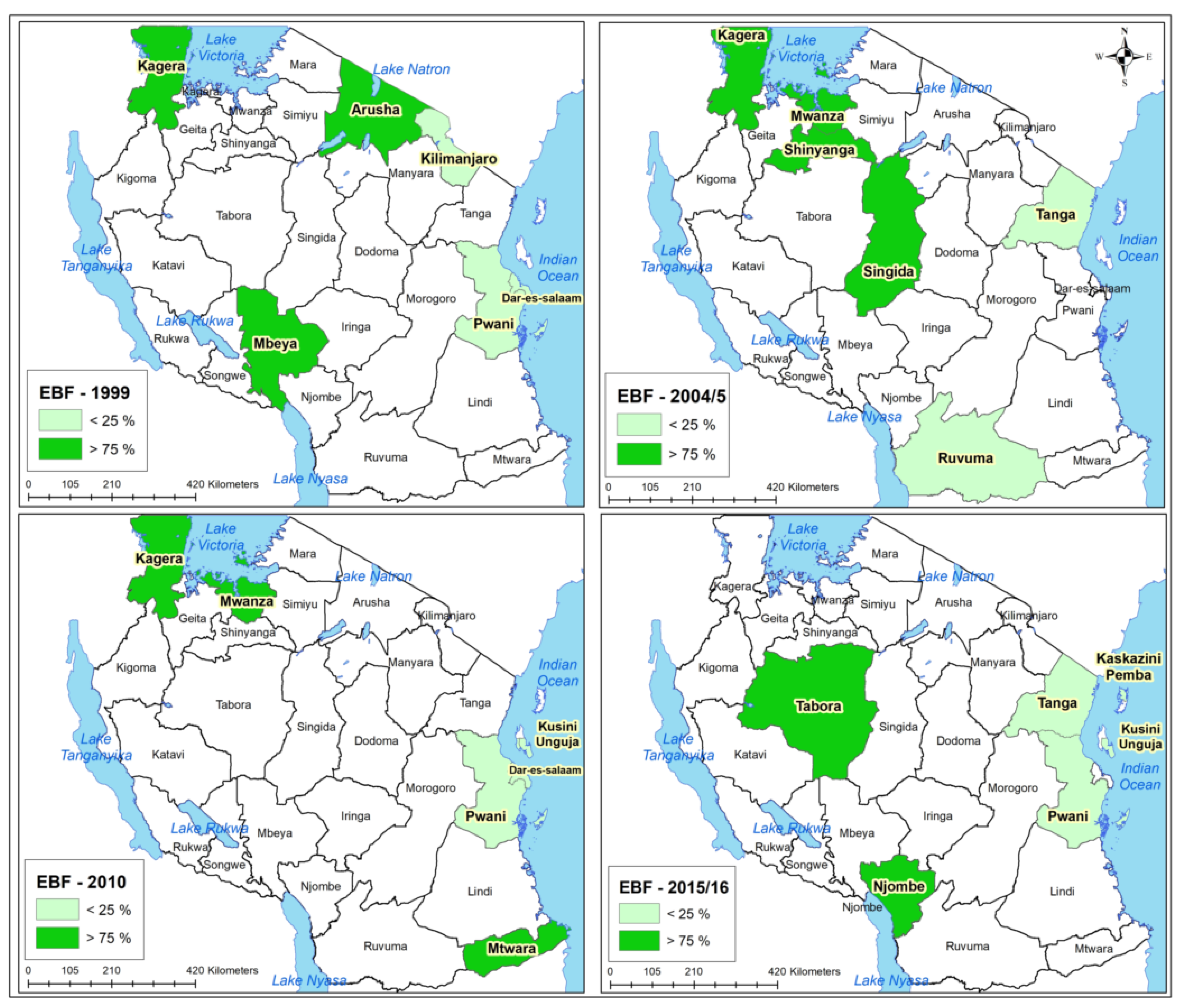
2.6.2. Maps Development
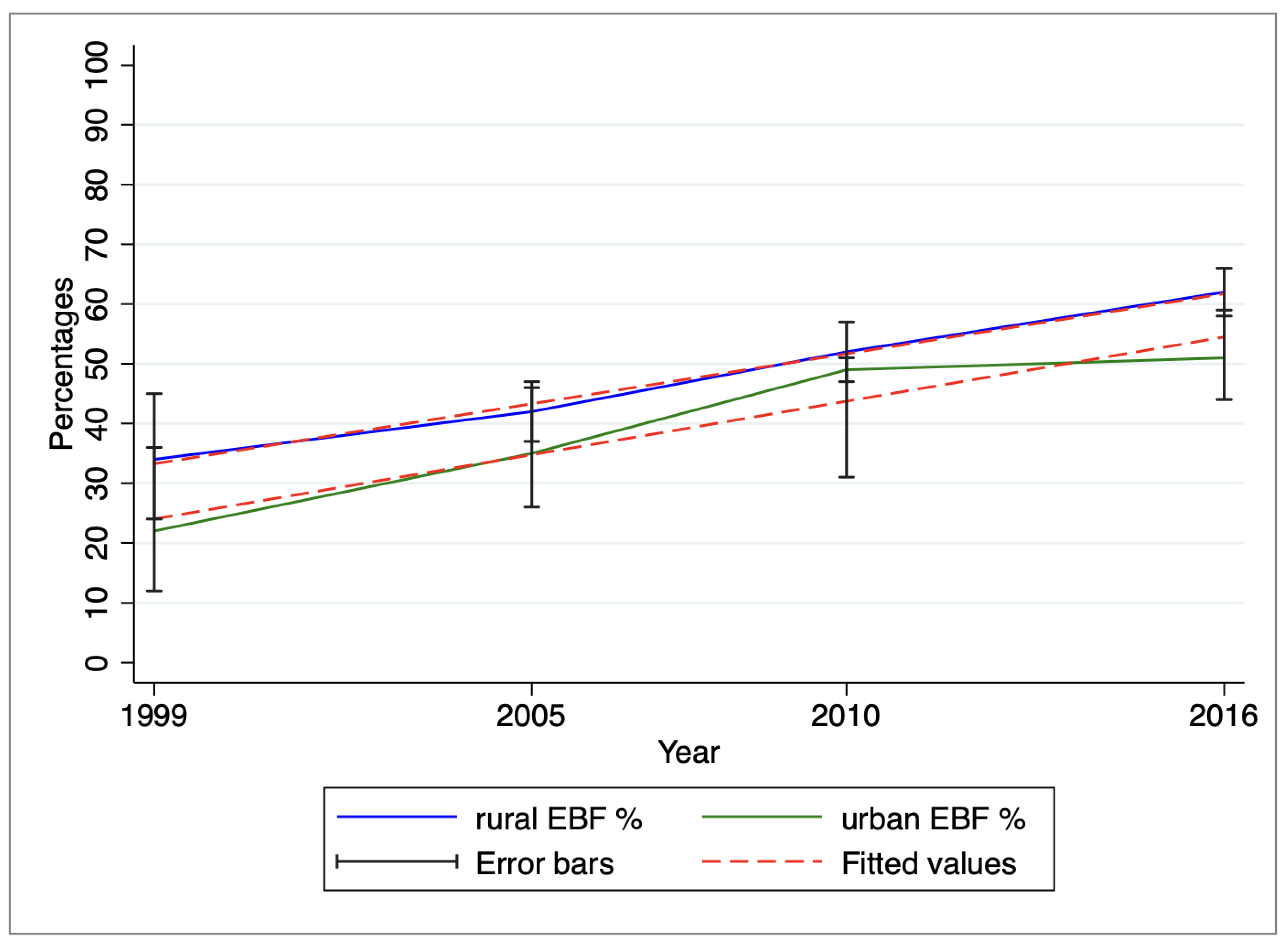
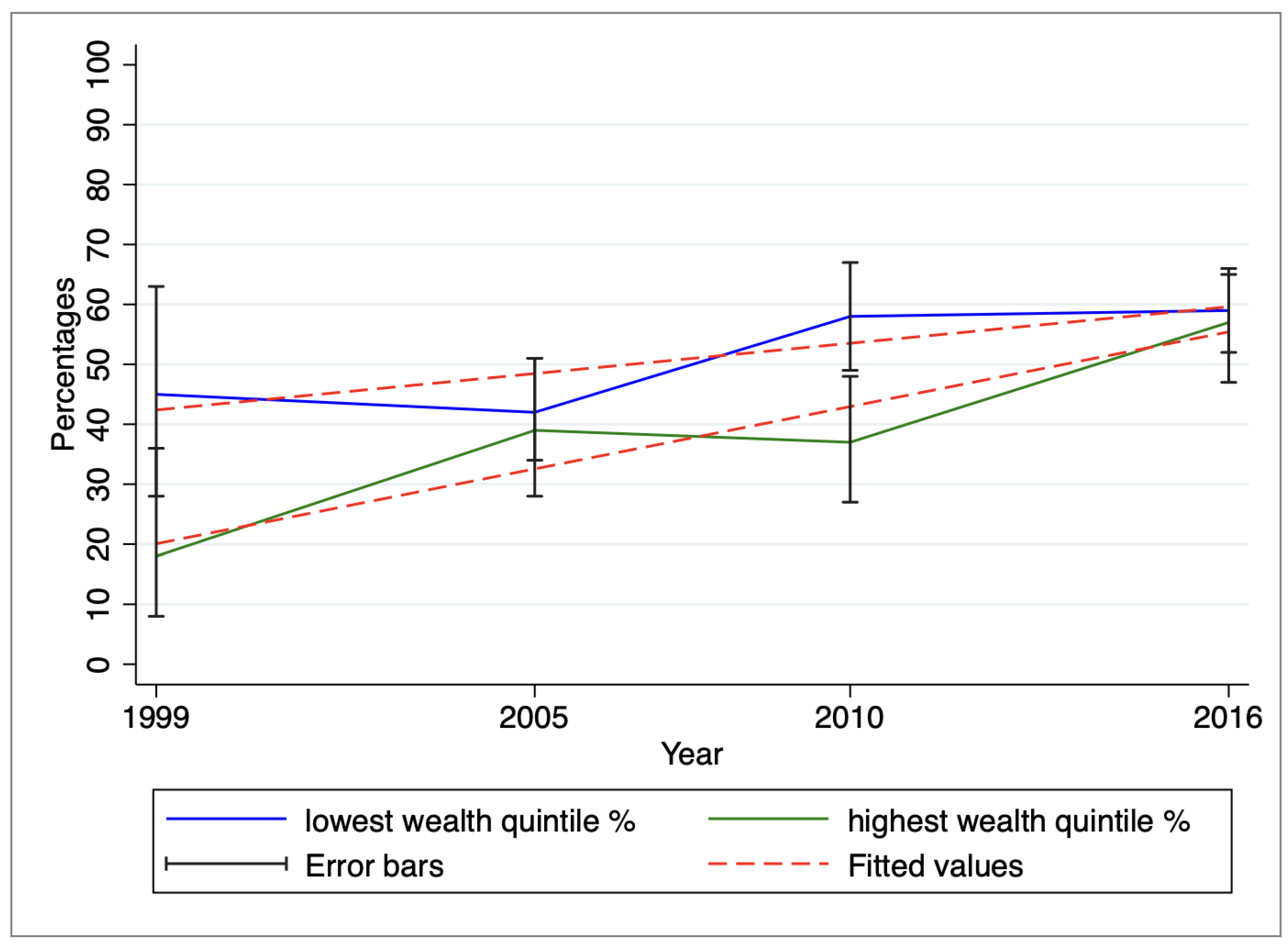
2.6.3. The Trend of EBF Practices by Area of Residence and by Wealth Quintile
2.6.4. Model Selection for the Determinants of EBF across Surveys and Its Validation
- i.
- Classical logistic regression with the age of an infant as a categorical variable;
- ii.
- Classical logistic regression with the age of an infant as a continuous variable;
- iii.
- Generalized linear mixed model accounting for clustering at regional level with infant’s age treated as a categorical variable;
- iv.
- Generalized linear mixed model accounting for clustering at regional level with infant’s age as a continuous variable;
- v.
- Generalized linear mixed model accounting for enumeration area nested in regions with infant’s age treated as categorical;
- vi.
- Generalized linear mixed model accounting for enumeration area nested in regions with infant’s age as a continuous variable.
3. Results
3.1. Background Characteristics of the Participants from the Surveys
3.2. The Trend of EBF by Region across the Surveys
3.3. Variation of EBF Based on the Area of Residence and the Wealth Quintile
3.4. Determinants of EBF across the Surveys
4. Discussion
- Region-specific interventions: Given the disparities in EBF practices across regions, it’s crucial to design region-specific interventions to address the lagging regions, particularly those along the coast. These interventions should be tailored to the cultural and socioeconomic contexts of each region, focusing on raising awareness about the benefits of EBF and providing adequate support to mothers. This calls for localized studies to understand the unique factors influencing EBF adoption. This will enable the development of targeted interventions that consider specific local dynamics;
- Age-Specific EBF Support: Addressing the consistent drop in EBF proportions as infants age requires age-specific support mechanisms. Establish comprehensive educational programs that provide mothers, and society in general, with knowledge and skills to sustain EBF as infants grow, tackling challenges such as milk insufficiency perceptions and infant fussiness. The education program should be integrated into the extended program of immunization, as it often provides an opportunity for mothers and caregivers to visit healthcare facilities or interact with healthcare providers;
- Urban EBF Promotion: Urban areas are also experiencing challenges in EBF adoption. Policy efforts should target urban populations with campaigns emphasizing the importance of EBF, dispelling misconceptions, and providing accessible resources for urban mothers to facilitate EBF practices amidst busy lifestyles;
- Wealth-Targeted Programs: While wealthier mothers are catching up with EBF adoption, efforts should be made to prevent the reversal of this pattern. Targeted programs should be implemented that ensure accessibility to EBF information, counseling, and support for mothers across all income levels. This can prevent a scenario where wealthier mothers breastfeed for longer durations, leaving economically disadvantaged mothers at a disadvantage;
- Sustaining EBF with Economic Growth: As Tanzania’s economy advances, efforts should be made to prevent the decline in EBF adoption observed in some wealthier segments. There is a need to establish breastfeeding-friendly workplaces, ensuring that working mothers have the support and facilities needed to continue EBF while pursuing their careers;
- Quality Healthcare Facilities: The positive association between EBF and delivering at health facilities suggests the need for strengthening healthcare facilities’ role in EBF promotion. Healthcare providers should receive consistent training on EBF counseling to ensure accurate and reliable guidance to mothers. Enhancing the quality and accessibility of healthcare facilities can contribute to higher EBF rates.
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington DC, USA; WHO: Geneva, Switzerland, 2008; Volume 2007, Available online: https://apps.who.int/iris/bitstream/handle/10665/43895/9789241596664_eng.pdf;sequence=1 (accessed on 1 June 2023).
- UNICEF; WHO. Complementary Feeding of Young Children in Developing Countries: A Review of Current Scientific Knowledge; Emergency Nutrition Network (ENN): Kidlington, UK, 1998. [Google Scholar]
- Matare, C.R.; Craig, H.C.; Martin, S.L.; Kayanda, R.A.; Chapleau, G.M.; Kerr, R.B.; Dearden, K.A.; Nnally, L.P.; Dickin, K.L. Barriers and Opportunities for Improved Exclusive Breast-Feeding Practices in Tanzania: Household Trials With Mothers and Fathers. Food Nutr. Bull. 2019, 40, 308–325. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Tomori, C.; Hernández-Cordero, S.; Baker, P.; Barros, A.J.; Bégin, F.; Chapman, D.J.; Grummer-Strawn, L.M.; McCoy, D.; Menon, P.; et al. Series Breastfeeding 1 Breastfeeding: Crucially important, but increasingly challenged in a market-driven world. Lancet 2023, 401, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Huffman, S.L.; Zehner, E.R.; Victora, C. Can improvements in breast-feeding practices reduce neonatal mortality in developing countries? Midwifery 2001, 17, 80–92. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Mwiru, R.S.; Spiegelman, D.; Duggan, C.; Peterson, K.; Liu, E.; Msamanga, G.; Aboud, S.; Fawzi, W.W. Relationship of exclusive breast-feeding to infections and growth of Tanzanian children born to HIV-infected women. Public Health Nutr. 2011, 14, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Community Development, Gender, Elderly and Children—MoHCDGEC/Tanzania Mainland; Ministry of Health—MoH/Zanzibar; National Bureau of Statistics—NBS/Tanzania; Office of Chief Government Statistician—OCGS/Zanzibar; ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16; MoHCDGEC, MoH, NBS, OCGS, ICF: Dar es Salaam, Tanzania, 2016. [Google Scholar]
- Afnan-Holmes, H.; Magoma, M.; John, T.; Levira, F.; Msemo, G.; Armstrong, C.E.; Martínez-Álvarez, M.; Kerber, K.; Kihinga, C.; Makuwani, A.; et al. Tanzania’s Countdown to 2015: An analysis of two decades of progress and gaps for reproductive, maternal, newborn, and child health, to inform priorities for post-2015. Lancet Glob. Health 2015, 3, e396–e409. [Google Scholar] [CrossRef]
- Bhattacharjee, N.V.; Schaeffer, L.E.; Marczak, L.B.; Ross, J.M.; Swartz, S.J.; Albright, J.; Gardner, W.M.; Shields, C.; Sligar, A.; Schipp, M.F.; et al. Mapping exclusive breastfeeding in Africa between 2000 and 2017. Nat. Med. 2019, 25, 1205–1212. [Google Scholar] [CrossRef]
- Dede, K.S.; Bras, H. Exclusive breastfeeding patterns in Tanzania: Do individual, household, or community factors matter? Int. Breastfeed. J. 2020, 15, 32. [Google Scholar] [CrossRef]
- Yalçin, S.S.; Berde, A.S.; Yalçin, S. Determinants of Exclusive Breast Feeding in sub-Saharan Africa: A Multilevel Approach. Paediatr. Perinat. Epidemiol. 2016, 30, 439–449. [Google Scholar] [CrossRef]
- Agho, K.E.; Dibley, M.J.; Odiase, J.I.; Ogbonmwan, S.M. Determinants of exclusive breastfeeding in Nigeria. BMC Pregnancy Childbirth 2011, 11, 2. [Google Scholar] [CrossRef]
- Kazaura, M. Exclusive breastfeeding practices in the Coast Region, Tanzania. Afr. Health Sci. 2016, 16, 44–50. [Google Scholar] [CrossRef]
- Chandhiok, N.; Singh, K.J.; Sahu, D.; Singh, L.; Pandey, A. Changes in exclusive breastfeeding practices and its determinants in India, 1992–2006: Analysis of national survey data. Int. Breastfeed. J. 2015, 10, 34. [Google Scholar] [CrossRef]
- Labbok, M.H.; Wardlaw, T.; Blanc, A.; Clark, D.; Terreri, N. Trends in Exclusive Breastfeeding: Findings from the 1990s. J. Hum. Lact. 2006, 22, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Parizoto, G.M.; Parada, C.M.G.D.L.; Venâncio, S.I.; Carvalhaes, M.A.D.B.L. Trends and patterns of exclusive breastfeeding for under-6-month-old children. J. Pediatr. 2009, 85, 201–208. [Google Scholar] [CrossRef]
- Khanal, V.; Sauer, K.; Zhao, Y. Exclusive breastfeeding practices in relation to social and health determinants: A comparison of the 2006 and 2011 Nepal Demographic and Health Surveys. BMC Public Health 2013, 13, 958. [Google Scholar] [CrossRef] [PubMed]
- Shirima, R.; Greiner, T.; Kylberg, E.; Gebre-Medhin, M. Exclusive breast-feeding is rarely practised in rural and urban Morogoro, Tanzania. Public Health Nutr. 2001, 4, 147–154. [Google Scholar] [CrossRef]
- National Institute of Statistics of Rwanda (NISR) [Rwanda]; Ministry of Health (MOH) [Rwanda]; ICF International. Rwanda Demographic and Health Survey 2014-15; NISR, MOH, ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Ekholuenetale, M.; Barrow, A.; Arora, A. Skin-to-skin contact and breastfeeding practices in Nigeria: A study of socioeconomic inequalities. Int. Breastfeed. J. 2022, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- Matanda, D.J.; Mittelmark, M.B.; Kigaru, D.M.D. Breast-, complementary and bottle-feeding practices in Kenya: Stagnant trends were experienced from 1998 to 2009. Nutr. Res. 2014, 34, 507–517. [Google Scholar] [CrossRef]
- Kenya Ministry of Health. Rapid Qualitative Assessment: Beliefs and Attitudes around Infant and Young Child Feeding in Kenya. 2011, pp. 1–45. Available online: http://www.iycn.org/files/FINAL-Beliefs_and_Attitudes_Around_IYCF_in_Kenya-032311.pdf (accessed on 1 June 2023).
- Croft, T.N.; Marshall, A.M.; Allen, C.K.; Arnold, F.; Assaf, S.; Balian, S. Guide to DHS Statistics; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Tanzania Commission for AIDS (TACAIDS); Zanzibar AIDS Commission (ZAC); National Bureau of Statistics (NBS); Office of the Chief Government Statistician (OCGS); ICF International. Tanzania HIV/AIDS and Malaria Indicator Survey 2011-12; TACAIDS, ZAC, NBS, OCGS, ICF International: Dar es Salaam, Tanzania, 2013. [Google Scholar]
- Chale, L.E.; Fenton, T.R.; Kayange, N. Predictors of knowledge and practice of exclusive breastfeeding among health workers in Mwanza city, northwest Tanzania. BMC Nurs. 2016, 15, 72. [Google Scholar] [CrossRef]
- Lorri, W.; Svanberg, U. An overview of the use of fermented foods for child feeding in tanzania. Ecol. Food Nutr. 1995, 34, 65–81. [Google Scholar] [CrossRef]
- Hadley, C. Ethnic expansions and between-group differences in children’s health: A case study from the Rukwa Valley, Tanzania. Am. J. Phys. Anthropol. 2005, 128, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Mgongo, M.; Mosha, M.V.; Uriyo, J.G.; Msuya, S.E.; Stray-pedersen, B. Prevalence and predictors of exclusive breastfeeding among women in Kilimanjaro region, Northern Tanzania: A population based cross-sectional study. Int. Breastfeed. J. 2013, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwaz, E.G.; Richter, L.M.; Victora, C.G. Breastfeeding Series Group, Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar]
- Semega-Janneh, I.J.; Bøhler, E.; Holm, H.; Matheson, I.; Holmboe-Ottesen, G. Promoting breastfeeding in rural Gambia: Combining traditional and modern knowledge. Health Policy Plan. 2001, 16, 199–205. [Google Scholar] [CrossRef]
- Khanal, V.; Lee, A.H.; Scott, J.A.; Karkee, R.; Binns, C.W. Implications of methodological differences in measuring the rates of exclusive breastfeeding in Nepal: Findings from literature review and cohort study. BMC Pregnancy Childbirth 2016, 16, 389. [Google Scholar] [CrossRef] [PubMed]
- Agnarsson, I.; Mpello, A.; Gunnlaugsson, G.; Hofvander, Y.; Greiner, T. Infant feeding practices during the first six months of life in a rural area in Tanzania. East Afr. Med. J. 2001, 78, 9–13. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Eshton Nkala, T.; Msuya, S.E. Prevalence and Predictors of Exclusive Breastfeeding among Women in Kigoma Region, Western Tanzania: A Community Based Cross-Sectional Study. 2011. Available online: http://www.internationalbreastfeedingjournal.com/content/6/1/17 (accessed on 1 August 2020).
- Schulze, P.A.; Carlisle, S.A. What research does and doesn’t say about breastfeeding: A critical review. Early Child Dev. Care 2010, 180, 703–718. [Google Scholar] [CrossRef]
- Oyelana, O.; Kamanzi, J.; Richter, S. A critical look at exclusive breastfeeding in Africa: Through the lens of diffusion of innovation theory. Int. J. Afr. Nurs. Sci. 2021, 14, 100267. [Google Scholar] [CrossRef]
- Husain Rasheed, M.; Philemon, R.; Damas Kinabo, G.; Maxym, M.; Mamuu Shayo, A.; Theophil Mmbaga, B. Adherence to Exclusive Breastfeeding and Associated Factors in Mothers of HIV-Exposed Infants Receiving Care at Kilimanjaro Christian Medical Centre, Tanzania. East Afr. Health Res. J. 2018, 2, 33–42. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1999 (N = 322) | 2004/5 (N = 854) | 2010 (N = 803) | 2015/16 (N = 1015) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall Total (a) | Yes EBF (b) | Overall Total (a) | Yes EBF (b) | Overall Total (a) | Yes EBF (b) | Overall Total (a) | Yes EBF (b) | |||||||||
| n | % | Row % | 95% CI | n | % | Row % | 95% CI | n | % | Row % | 95% CI | n | % | Row % | 95% CI | |
| Characteristics | ||||||||||||||||
| EBF Proportion | 31.80% | (22.5–39.3) | 41 | [36.8, 45.4] | 49.9 | [45.6, 54.2] | 59.2 | [55.7, 62.7] | ||||||||
| Infant’s characteristics | ||||||||||||||||
| Sex of an infant | ||||||||||||||||
| Male | 161 | 50 | 25.5 | [17.2, 36.0] | 417 | 48.8 | 42.5 | [36.4, 48.9] | 398 | 49.6 | 50.2 | [44.4, 56.0] | 507 | 50 | 59 | [54.2, 63.7] |
| Female | 161 | 50 | 38 | [26.5, 51.1] | 437 | 51.2 | 39.6 | [34.1, 45.3] | 405 | 50.4 | 49.6 | [43.5, 55.7] | 508 | 50 | 59.4 | [54.4, 64.3] |
| Infant’s age (month) | ** | ** | ** | ** | ||||||||||||
| 0 | 37 | 11.5 | 53.9 | [31.7, 74.7] | 83 | 9.7 | 76.5 | [65.2, 85.0] | 80 | 10 | 86.2 | [75.1, 92.9] | 194 | 19.1 | 89.4 | [83.7, 93.3] |
| 1 | 60 | 18.6 | 59.6 | [42.6, 74.6] | 161 | 18.9 | 63.8 | [54.9, 71.9] | 162 | 20.2 | 78.3 | [68.9, 85.4] | 184 | 18.1 | 78.4 | [71.1, 84.2] |
| 2 | 56 | 17.4 | 29.6 | [17.0, 46.4] | 173 | 20.3 | 49.4 | [40.5, 58.3] | 146 | 18.2 | 57.9 | [47.9, 67.2] | 175 | 17.2 | 63.4 | [54.9, 71.2] |
| 3 | 63 | 19.6 | 21.3 | [10.9, 37.5] | 149 | 17.4 | 33.4 | [24.5, 43.7] | 128 | 15.9 | 44.2 | [34.4, 54.5] | 159 | 15.7 | 53.4 | [44.5, 62.0] |
| 4 | 57 | 17.7 | 15.3 | [5.0, 38.1] | 142 | 16.6 | 17.6 | [11.1, 27.0] | 145 | 18.1 | 26.3 | [18.6, 35.8] | 181 | 17.8 | 33 | [25.1, 41.9] |
| 5 | 49 | 15.2 | 15.7 | [4.4, 42.9] | 146 | 17.1 | 10 | [5.4, 17.8] | 142 | 17.7 | 20 | [14.0, 27.7] | 122 | 12 | 18.1 | [11.5, 27.3] |
| Mother’s characteristics | ||||||||||||||||
| Mother’s age (years) | ||||||||||||||||
| Less than 18 | 18 | 5.6 | 40.1 | [15.7, 70.6] | 37 | 4.3 | 42.2 | [24.5, 62.2] | 39 | 4.9 | 57 | [41.8, 70.9] | 49 | 4.8 | 49.6 | [32.7, 66.6] |
| 18–24 | 110 | 34.2 | 27.8 | [18.1, 40.0] | 297 | 34.8 | 35.1 | [28.6, 42.2] | 283 | 35.2 | 49.5 | [42.7, 56.3] | 411 | 40.5 | 58.4 | [52.8, 63.9] |
| 25+ | 194 | 60.2 | 33.6 | [22.9, 46.3] | 520 | 60.9 | 44.6 | [39.2, 50.2] | 481 | 59.9 | 49.5 | [44.1, 54.9] | 555 | 54.7 | 60.8 | [55.7, 65.7] |
| Current marital status | ||||||||||||||||
| Never in union/widowed/divorced/no longer living together | 46 | 14.3 | 23.3 | [11.0, 42.7] | 90 | 10.5 | 31.1 | [21.3, 43.0] | 108 | 13.4 | 43.4 | [33.6, 53.8] | 147 | 14.5 | 57.7 | [48.4, 66.5] |
| Married/living with partner | 276 | 85.7 | 33.4 | [24.0, 44.3] | 764 | 89.5 | 42.3 | [37.7, 47.0] | 695 | 86.6 | 51 | [46.0, 56.0] | 868 | 85.5 | 59.5 | [55.7, 63.2] |
| Wealth quintile | * | |||||||||||||||
| Lowest | 89 | 27.6 | 45.1 | [28.4, 63.0] | 176 | 20.6 | 42 | [33.8, 50.7] | 156 | 19.4 | 58.3 | [49.2, 66.8] | 258 | 25.4 | 58.9 | [51.6, 65.8] |
| Low | 39 | 12.1 | 20.9 | [7.4, 46.4] | 154 | 18 | 45.2 | [36.5, 54.3] | 190 | 23.7 | 54 | [44.8, 63.0] | 209 | 20.6 | 63 | [54.5, 70.8] |
| Middle | 57 | 17.7 | 31.9 | [19.0, 48.3] | 187 | 21.9 | 37.7 | [30.6, 45.4] | 178 | 22.2 | 51.5 | [42.3, 60.6] | 179 | 17.6 | 58.7 | [50.5, 66.4] |
| High | 54 | 16.8 | 39 | [24.1, 56.3] | 192 | 22.5 | 41.8 | [32.6, 51.6] | 177 | 22 | 42.5 | [33.8, 51.6] | 214 | 21.1 | 58.1 | [49.3, 66.3] |
| Highest | 83 | 25.8 | 17.9 | [8.0, 35.2] | 145 | 17 | 38.9 | [28.5, 50.5] | 102 | 12.7 | 37 | [26.7, 48.7] | 155 | 15.3 | 56.8 | [47.2, 65.9] |
| Mother’s residence | * | * | ||||||||||||||
| Urban | 77 | 23.9 | 21.9 | [12.4, 35.7] | 145 | 17 | 35.3 | [25.9, 46.0] | 135 | 16.8 | 40.3 | [30.9, 50.4] | 243 | 23.9 | 51.4 | [44.0, 58.7] |
| Rural | 245 | 76.1 | 34 | [24.3, 45.2] | 709 | 83 | 42.3 | [37.6, 47.1] | 668 | 83.2 | 52.2 | [47.3, 57.0] | 772 | 76.1 | 62.2 | [58.2, 66.1] |
| Education attainment | ||||||||||||||||
| No education | 92 | 28.6 | 39.7 | [21.8, 60.8] | 210 | 24.6 | 41 | [32.4, 50.2] | 207 | 25.8 | 50.6 | [41.9, 59.3] | 201 | 19.8 | 55.6 | [47.9, 63.1] |
| Incomplete primary | 50 | 15.5 | 28.7 | [15.2, 47.6] | 161 | 18.9 | 34.5 | [25.1, 45.4] | 138 | 17.2 | 50.1 | [39.7, 60.6] | 135 | 13.3 | 49.2 | [40.4, 58.1] |
| Complete primary/incomplete secondary | 178 | 55.3 | 28.3 | [20.3, 38.0] | 469 | 54.9 | 41.7 | [36.6, 47.0] | 453 | 56.4 | 49.7 | [44.0, 55.5] | 574 | 56.6 | 61.5 | [56.5, 66.3] |
| Complete secondary/higher | 2 | 0.6 | 0 | 14 | 1.6 | 79.9 | [50.9, 93.9] | 5 | 0.6 | 21.7 | [2.8, 73.0] | 105 | 10.3 | 65.8 | [54.7, 75.5] | |
| Who respondent works for | * | |||||||||||||||
| For family member/Someone else | 131 | 40.7 | 27.8 | [18.9, 38.8] | 592 | 69.3 | 43.9 | [39.3, 48.5] | 228 | 28.4 | 48.4 | [40.8, 56.0] | 362 | 35.7 | 62 | [56.0, 67.6] |
| Self-employed | 97 | 30.1 | 39.3 | [26.9, 53.4] | 125 | 14.6 | 27.6 | [17.7, 40.3] | 435 | 54.2 | 48.9 | [43.0, 54.9] | 410 | 40.4 | 61.5 | [55.6, 67.0] |
| Not working | 94 | 29.2 | 32.7 | [16.3, 54.9] | 137 | 16 | 33.3 | [22.4, 46.3] | 140 | 17.4 | 57.7 | [47.2, 67.6] | 243 | 23.9 | 51.3 | [43.7, 58.9] |
| Frequency of listening to radio | ||||||||||||||||
| Not at all | 110 | 34.2 | 40.3 | [30.3, 51.2] | 206 | 24.1 | 49.8 | [42.1, 57.5] | 263 | 32.8 | 55.8 | [48.6, 62.7] | 276 | 27.2 | 60.7 | [53.8, 67.2] |
| Less than once a week | 125 | 38.8 | 23 | [13.5, 36.4] | 105 | 12.3 | 35.8 | [26.4, 46.4] | 124 | 15.4 | 48.5 | [37.4, 59.8] | 359 | 35.4 | 58.5 | [52.2, 64.6] |
| At least once a week | 14 | 4.3 | 8.8 | [1.6, 36.1] | 172 | 20.1 | 36.1 | [27.9, 45.3] | 156 | 19.4 | 43.6 | [34.4, 53.3] | 380 | 37.4 | 58.8 | [52.6, 64.7] |
| Almost everyday | 73 | 22.7 | 39.3 | [20.4, 62.1] | 371 | 43.4 | 39.3 | [32.9, 46.1] | 260 | 32.4 | 47.7 | [39.8, 55.7] | ||||
| Frequency of watching television | * | * | ||||||||||||||
| Not at all | 249 | 77.3 | 33.6 | [24.1, 44.6] | 677 | 79.3 | 44 | [39.3, 48.7] | 617 | 76.8 | 52.6 | [47.7, 57.5] | 597 | 58.8 | 60.1 | [55.5, 64.5] |
| Less than once a week | 54 | 16.8 | 25.3 | [9.9, 51.2] | 77 | 9 | 17.8 | [10.0, 29.8] | 89 | 11.1 | 46.4 | [33.8, 59.6] | 240 | 23.6 | 59.2 | [51.7, 66.3] |
| At least once a week | 2 | 0.6 | 0 | 63 | 7.4 | 32.2 | [18.7, 49.5] | 42 | 5.2 | 27.6 | [14.9, 45.2] | 178 | 17.5 | 56 | [47.4, 64.2] | |
| Almost everyday | 17 | 5.3 | 1.2 | [0.1, 9.0] | 37 | 4.3 | 53.3 | [28.4, 76.7] | 55 | 6.8 | 39.5 | [23.2, 58.5] | ||||
| Place of delivery | * | |||||||||||||||
| Home | 193 | 59.9 | 40.3 | [30.5, 50.9] | 456 | 53.4 | 41.2 | [35.5, 47.1] | 398 | 49.6 | 50.6 | [43.8, 57.5] | 358 | 35.3 | 59 | [53.2, 64.7] |
| Health facility | 129 | 40.1 | 20.2 | [11.5, 33.0] | 398 | 46.6 | 40.8 | [34.4, 47.4] | 405 | 50.4 | 49.2 | [44.2, 54.2] | 657 | 64.7 | 59.3 | [54.7, 63.8] |
| 1999 | 2004/5 | 2010 | 2015/16 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| COR (95% CI) | p-Value | AOR (95% CI) | p-Value | COR (95% CI) | p-Value | AOR (95% CI) | p-Value | COR (95% CI) | p-Value | AOR (95% CI) | p-Value | COR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Characteristics | ||||||||||||||||
| Infant’s characteristics | ||||||||||||||||
| Sex of an infant | ||||||||||||||||
| female | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| male | 0.7 (0.4, 1.4) | 0.358 | 0.6 (0.2, 1.4) | 0.203 | 1.1 (0.8, 1.6) | 0.45 | 1.3 (0.8, 1.9) | 0.267 | 1.1 (0.8, 1.6) | 0.483 | 1.2 (0.8, 1.8) | 0.483 | 1.03 (0.8, 1.4) | 0.869 | 0.9 (0.6, 1.3) | 0.607 |
| Infant’s age (month) | 0.4 (0.3, 0.5) | <0.001 | 0.3 (0.2, 0.5) | <0.001 | 0.4 (0.4, 0.5) | <0.001 | 0.4 (0.3, 0, 5) | <0.001 | 0.4 (0.3, 0.5) | <0.0001 | 0.4 (0.3, 0.4) | <0.001 | 0.4 (0.3, 0.4) | <0.0001 | 0.4 (0.3, 0.4) | <0.0001 |
| Mother’s characteristics | ||||||||||||||||
| Mother’s age (years) | ||||||||||||||||
| less than 18 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| 18–24 | 0.5 (0.1, 1.97) | 0.323 | 0.3 (0.03, 2.2) | 0.218 | 0.7 (0.3, 1.5) | 0.321 | 0.9 (0.3, 2.7) | 0.833 | 0.4 (0.2, 0.9) | 0.022 | 0.4 (0.2, 1.2) | 0.096 | 1.8 (0.9, 3.5) | 0.106 | 1.3 (0.5, 3.2) | 0.549 |
| 25+ | 0.6 (0.2, 2.3) | 0.441 | 0.3 (0.03, 2.0) | 0.198 | 1 (0.4, 2.2) | 0.956 | 1.5 (0.5, 4.4) | 0.481 | 0.4 (0.2, 0.9) | 0.027 | 0.5 (0.2, 1.4) | 0.187 | 2 (1, 3.9) | 0.047 | 2.0 (0.8, 4.9) | 0.114 |
| Wealth quintile | ||||||||||||||||
| lowest | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| low | 0.3 (0.1, 0.8) | 0.018 | 0.2 (0.04, 0.9) | 0.04 | 1.03 (0.6, 1.8) | 0.908 | 0.7 (0.4, 1.4) | 0.361 | 1 (0.6, 1.6) | 0.868 | 0.7 (0.4, 1.4) | 0.359 | 1.3 (0.8, 2) | 0.311 | 1 (0.6, 1.9) | 0.905 |
| middle | 0.7 (0.31.6) | 0.396 | 0.4 (0.1, 1.6) | 0.222 | 0.6 (0.4, 1) | 0.047 | 0.5 (0.3, 0.9) | 0.034 | 0.8 (0.5, 1.3) | 0.321 | 0.7 (0.4, 1.5) | 0.366 | 1.2 (0.7, 1.9) | 0.541 | 1.3 (0.7, 2.5) | 0.415 |
| high | 0.9 (0.4, 2.4) | 0.913 | 1.3 (0.3, 5.1) | 0.695 | 1.1 (0.6, 1.8) | 0.842 | 0.8 (0.4, 1.8) | 0.725 | 0.5 (0.3, 0.9) | 0.014 | 0.5 (0.2, 1.2) | 0.125 | 1.3 (0.8, 2.1) | 0.331 | 1.4 (0.7, 3) | 0.317 |
| highest | 0.4 (0.1, 1.1) | 0.085 | 0.8 (0.1, 5.5) | 0.797 | 0.9 (0.5, 1.7) | 0.725 | 1.03 (0.4, 2.9) | 0.941 | 0.4 (0.2, 0.9) | 0.02 | 0.5 (0.1, 1.5) | 0.196 | 1.4 (0.8, 2.7) | 0.232 | 1.4 (0.5, 3.9) | 0.581 |
| Mother’s residence | ||||||||||||||||
| urban | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| rural | 0.6 (0.2, 1.6) | 0.288 | 0.9 (0.1, 5.3) | 0.875 | 0.8 (0.4, 1.3) | 0.299 | 1.6 (0.8, 3.5) | 0.211 | 1.6 (0.9, 2.7) | 0.093 | 1.5 (0.6, 3.6) | 0.364 | 0.7 (0.5, 1.1) | 0.165 | 2.1 (0.1, 4.2) | 0.035 |
| Education attainment | ||||||||||||||||
| no education | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| incomplete primary | 0.4 (0.1, 1.1) | 0.063 | 0.1 (0.03, 0.7) | 0.017 | 0.7 (0.4, 1.3) | 0.294 | 0.7 (0.4, 1.5) | 0.395 | 0.7 (0.4, 1.2) | 0.202 | 0.5 (0.3, 1.1) | 0.088 | 0.8 (0.5, 1.4) | 0.477 | 1.1 (0.5, 2.2) | 0.834 |
| complete primary/incomplete secondary | 0.5 (0.2, 0.99) | 0.048 | 0.2 (0.1, 0.7) | 0.011 | 1.2 (0.8, 1.8) | 0.364 | 1.7 (0.9, 2.9) | 0.05 | 0.8 (0.6, 1.3) | 0.404 | 0.9 (0.5, 1.6) | 0.748 | 1.5 (1, 2.3) | 0.038 | 1.8 (1.03, 3.2) | 0.038 |
| complete secondary/higher | 9 (1.8, 46.3) | 0.008 | 12.2 (1.4, 103.1) | 0.022 | 0.3 (0.02, 5.1) | 0.416 | 1.3 (0.02, 80.3) | 0.9 | 1.9 (1, 3.5) | 0.059 | 2.6 (1.03, 6.3) | 0.043 | ||||
| Working status | ||||||||||||||||
| For family member/Someone else | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| Self-employed | 2.2 (0.99, 4.7) | 0.054 | 3.5 (1.2, 10.5) | 0.025 | 0.5 (0.3, 1) | 0.046 | 0.7 (0.3, 1.6) | 0.393 | 1.2 (0.8, 1.8) | 0.419 | 1.4 (0.8, 2.4) | 0.223 | 0.7 (0.5, 1.1) | 0.178 | 1.1 (0.7, 1.7) | 0.742 |
| Not working | 0.99 (0.4, 2.3) | 0.979 | 0.8 (0.2, 3) | 0.792 | 1.1 (0.6, 2) | 0.742 | 1.5 (0.7, 3.2) | 0.276 | 1.9 (1, 3.7) | 0.044 | 2.7 (1.2, 6.4) | 0.022 | 1.03 (0.7, 1.5) | 0.881 | 0.7 (0.4, 1.3) | 0.258 |
| Frequency of listening to radio | ||||||||||||||||
| not at all | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| less than once a week | 0.4 (0.2, 0.8) | 0.015 | 0.2 (0.1, 0.6) | 0.004 | 0.7 (0.5, 1.1) | 0.12 | 0.6 (0.3, 1.0) | 0.07 | 0.7 (0.4, 1.2) | 0.206 | 0.5 (0.3, 1) | 0.068 | 1.1 (0.7, 1.6) | 0.699 | 1.1 (0.6, 1.9) | 0.779 |
| At least once a week | 0.2 (0.03, 1.8) | 0.164 | 0.2 (0.01, 3.3) | 0.245 | 0.5 (0.3, 0.9) | 0.016 | 0.4 (0.2, 0.7) | 0.003 | 0.6 (0.4, 0.9) | 0.048 | 0.6 (0.3, 1.1) | 0.079 | 1 (0.7, 1.5) | 0.977 | 0.7 (0.4, 1.3) | 0.297 |
| Almost everyday | 1.7 (0.7, 4.3) | 0.236 | 0.7 (0.2, 3) | 0.603 | 0.7 (0.4, 1.2) | 0.206 | 1 (0.5, 2) | 0.939 | 0.6 (0.4, 1) | 0.052 | 0.6 (0.4, 1.2) | 0.173 | ||||
| Frequency of watching television | ||||||||||||||||
| not at all | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| less than once a week | 1.1 (0.4, 2.8) | 0.871 | 2.7 (0.6, 11.9) | 0.204 | 0.3 (0.1, 0.5) | <0.001 | 0.2 (0.1, 0.6) | 0.001 | 0.6 (0.4, 1.1) | 0.11 | 1.2 (0.6, 2.5) | 0.639 | 1.01 (0.7, 1.5) | 0.927 | 1 (0.6, 1.7) | 0.984 |
| At least once a week | 0.7 (0.4, 1.5) | 0.366 | 0.8 (0.3, 2) | 0.571 | 0.2 (0.1, 0.6) | 0.001 | 0.4 (0.1, 1.2) | 0.105 | 1.2 (0.7, 1.9) | 0.523 | 1.3 (0.6, 2.7) | 0.565 | ||||
| Almost everyday | 0.02 (9.2 × 10−6, 52.6) | 0.336 | 0.02 (6.3 × 10−6, 77.4) | 0.36 | 1.7 (0.6, 4.9) | 0.292 | 1.5 (0.3, 6.4) | 0.587 | 0.8 (0.3, 1.9) | 0.607 | 0.96 (0.3, 3.2) | 0.953 | ||||
| Place of delivery | ||||||||||||||||
| Health facility | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||
| Home | 2.8 (1.3, 6) | 0.011 | 2.7 (0.8, 9) | 0.098 | 0.9 (0.6, 1.2) | 0.426 | 0.7 (0.4, 1.1) | 0.08 | 0.9 (0.6, 1.3) | 0.671 | 0.6 (0.4, 1) | 0.069 | 0.8 (0.6, 1.2) | 0.271 | 0.7 (0.4, 1.1) | 0.135 |
| Random factors (p-value) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||||||||||||
| Intracluster correlation (ICC) Regional | 41.5% (95% CI: 19.3%, 67.9%) | 26% (14%, 43%) | 18% (8%, 36%) | 20% (10%, 36%) | ||||||||||||
| ICC EA | 58.5% (31.7%, 81.1%) | 40% (25%, 57%) | 45% (31%, 60%) | 46% (33%, 60%) | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahanpour, O.F.; Todd, J.; Mwambi, H.; Okango, E.L.; Mahande, M.J. Trends of Exclusive Breastfeeding Practices and Its Determinants in Tanzania from 1999 to 2016. Int. J. Environ. Res. Public Health 2023, 20, 6904. https://doi.org/10.3390/ijerph20206904
Jahanpour OF, Todd J, Mwambi H, Okango EL, Mahande MJ. Trends of Exclusive Breastfeeding Practices and Its Determinants in Tanzania from 1999 to 2016. International Journal of Environmental Research and Public Health. 2023; 20(20):6904. https://doi.org/10.3390/ijerph20206904
Chicago/Turabian StyleJahanpour, Ola Farid, Jim Todd, Henry Mwambi, Elphas Luchemo Okango, and Michael J. Mahande. 2023. "Trends of Exclusive Breastfeeding Practices and Its Determinants in Tanzania from 1999 to 2016" International Journal of Environmental Research and Public Health 20, no. 20: 6904. https://doi.org/10.3390/ijerph20206904
APA StyleJahanpour, O. F., Todd, J., Mwambi, H., Okango, E. L., & Mahande, M. J. (2023). Trends of Exclusive Breastfeeding Practices and Its Determinants in Tanzania from 1999 to 2016. International Journal of Environmental Research and Public Health, 20(20), 6904. https://doi.org/10.3390/ijerph20206904