
Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Certainty of Evidence
3. Results
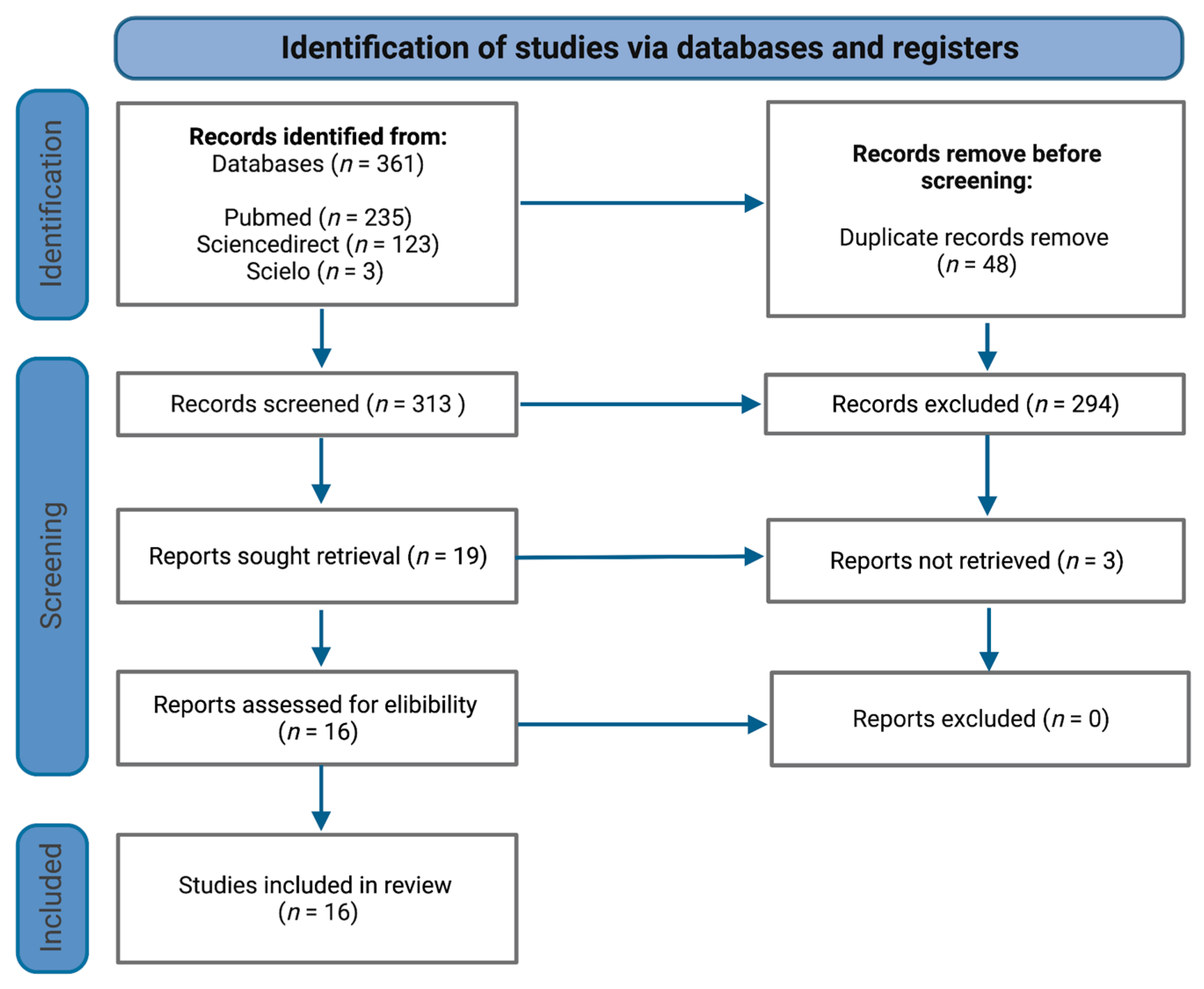
3.1. Search Results
3.2. Phase Angle as a Potential Screening Tool in Metabolic Diseases
3.2.1. Overweight and Obesity
3.2.2. Malnutrition
3.2.3. Cardiovascular and Chronic Kidney Diseases
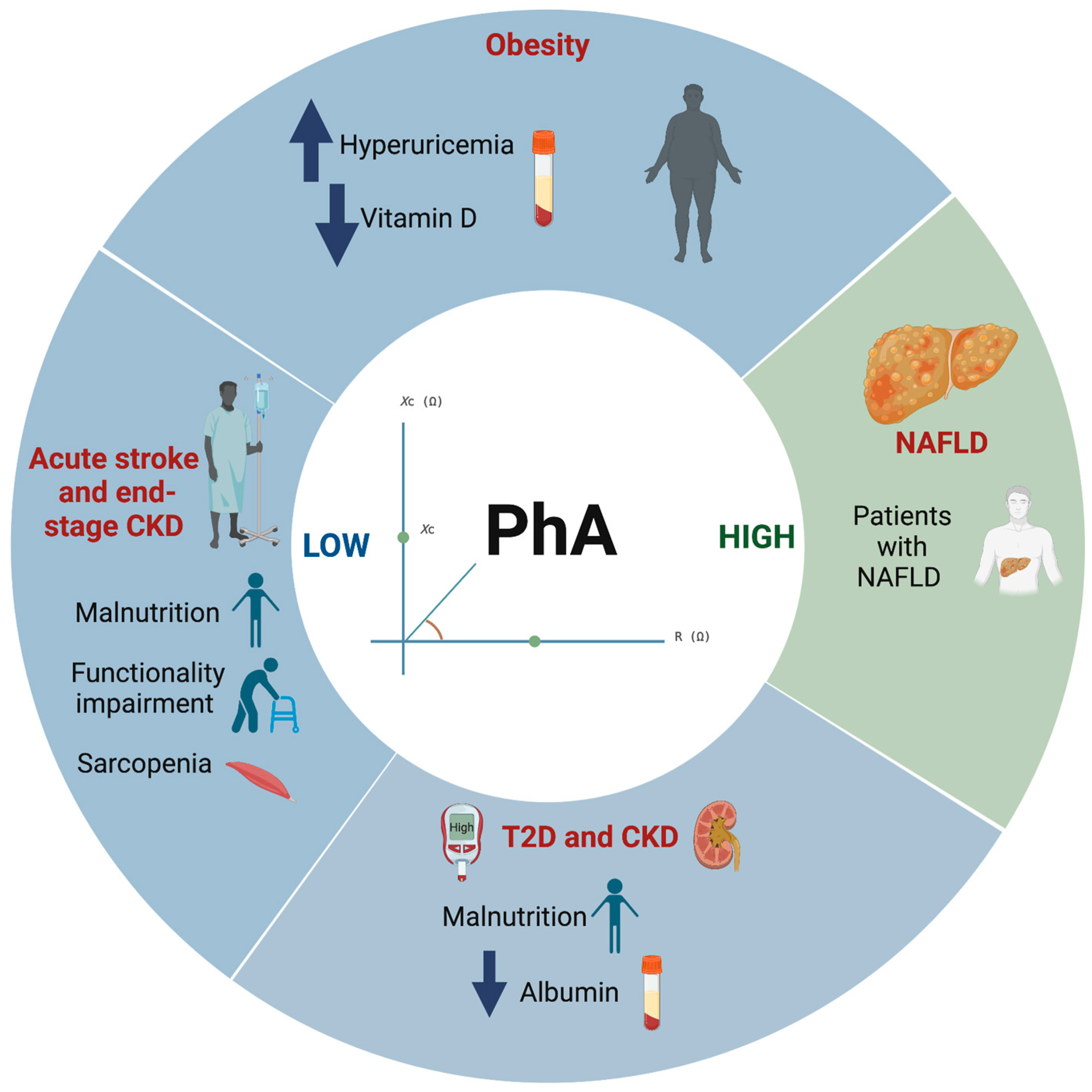
3.3. Differences on PhA Values in Several Health Conditions
3.4. Factors That Influence PhA Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noncommunicable Diseases. Available online: https://www.who.int/health-topics/noncommunicable-diseases (accessed on 17 November 2022).
- Garlini, L.M.; Alves, F.D.; Ceretta, L.B.; Perry, I.S.; Souza, G.C.; Clausell, N.O. Phase angle and mortality: A systematic review. Eur. J. Clin. Nutr. 2019, 73, 495–508. [Google Scholar] [CrossRef]
- de Borba, E.L.; Ceolin, J.; Ziegelmann, P.K.; Bodanese, L.C.; Gonçalves, M.R.; Cañon-Montañez, W.; Mattiello, R. Phase angle of bioimpedance at 50 kHz is associated with cardiovascular diseases: Systematic review and meta-analysis. Eur. J. Clin. Nutr. 2022, 76, 1366–1373. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis—Clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Iragorri, N.; Spackman, E. Assessing the value of screening tools: Reviewing the challenges and opportunities of cost-effectiveness analysis. Public Health Rev. 2018, 39, 17. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- What Is GRADE?|BMJ Best Practice. Available online: https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/ (accessed on 17 November 2022).
- Curvello-Silva, K.; Ramos, L.B.; Sousa, C.; Daltro, C. Phase angle and metabolic parameters in severely obese patients. Nutr. Hosp. 2020, 37, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Laudisio, D.; Di Somma, C.; Salzano, C.; Pugliese, G.; De Alteriis, G.; Colao, A.; Savastano, S. Phase Angle: A Possible Biomarker to Quantify Inflammation in Subjects with Obesity and 25(OH)D Deficiency. Nutrients 2019, 11, 1747. [Google Scholar] [CrossRef] [PubMed]
- Shin J ho Kim, C.R.; Park, K.H.; Hwang, J.H.; Kim, S.H. Predicting clinical outcomes using phase angle as assessed by bioelectrical impedance analysis in maintenance hemodialysis patients. Nutrition 2017, 41, 7–13. [Google Scholar] [CrossRef]
- Fernández-Jiménez, R.; Dalla-Rovere, L.; García-Olivares, M.; Abuín-Fernández, J.; Sánchez-Torralvo, F.J.; Doulatram-Gamgaram, V.K.; Hernández-Sanchez, A.M.; García-Almeida, J.M. Phase Angle and Handgrip Strength as a Predictor of Disease-Related Malnutrition in Admitted Patients: 12-Month Mortality. Nutrients 2022, 14, 1851. [Google Scholar] [CrossRef]
- Abe, T.; Yoshimura, Y.; Imai, R.; Yoneoka, Y.; Tsubaki, A.; Sato, Y. Impact of Phase Angle on Physical Function in Patients with Acute Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105941. [Google Scholar] [CrossRef]
- Shin, J.; Hwang, J.H.; Han, M.; Cha, R.H.; Kang, S.H.; An, W.S.; Kim, J.C.; Kim, S.H. Phase angle as a marker for muscle health and quality of life in patients with chronic kidney disease. Clin. Nutr. 2022, 41, 1651–1659. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Clinical Significance of Phase Angle in Non-Dialysis CKD Stage 5 and Peritoneal Dialysis Patients. Nutrients 2018, 10, 1331. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Decreased Bioimpedance Phase Angle in Patients with Diabetic Chronic Kidney Disease Stage 5. Nutrients 2019, 11, 2874. [Google Scholar] [CrossRef]
- Silva TK da Perry, I.D.S.; Brauner, J.S.; Wender, O.C.B.; Souza, G.C.; Vieira, S.R.R. Performance evaluation of phase angle and handgrip strength in patients undergoing cardiac surgery: Prospective cohort study. Aust. Crit. Care 2018, 31, 284–290. [Google Scholar] [CrossRef]
- Oliveira Filho, J.M.; de Bernardes, P.S.; Serpa, G.H.C.; Siquiera, G.D.d.J.; Noll, M.; Venâncio, P.E.M.; Soares, V. Bioelectrical vector analysis in obese adolescents. Rev. Paul. Pediatr. 2020, 38, e2019017. [Google Scholar] [CrossRef] [PubMed]
- Jun, M.H.; Ku, B.; Kim, J.; Kim, K.H.; Kim, J.U. Mediation effect of the duration of diabetes mellitus on the decrease in bioimpedance phase angles in ethnically Korean people: A multicenter clinical study. J. Diabetes Investig. 2021, 12, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Lv, Y.; Ni, W.; Shi, Q.; Xiang, X.; Li, S.; Song, C.; Xiao, M.; Jin, S. Associations between Phase Angle Values Obtained by Bioelectrical Impedance Analysis and Nonalcoholic Fatty Liver Disease in an Overweight Population. Can. J. Gastroenterol. Hepatol. 2020, 2020, e8888405. [Google Scholar] [CrossRef]
- Fu, L.; Ren, Z.; Liu, X.; Wu, N.; Zhao, K.; Luo, G.; Yang, H.; Zhang, Y.; Yan, T.; Liu, Y.; et al. Reference Data of Phase Angle Using Bioelectrical Impedance Analysis in Overweight and Obese Chinese. Front. Endocrinol. 2022, 13, 924199. [Google Scholar] [CrossRef] [PubMed]
- Streb, A.R.; Hansen, F.; Gabiatti, M.P.; Tozetto, W.R.; Del Duca, G.F. Phase angle associated with different indicators of health-related physical fitness in adults with obesity. Physiol. Behav. 2020, 225, 113104. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.d.S.; Barreto Silva, M.I.; da Costa, M.S.; Pontes, K.S.d.S.; Castro, F.G.; Antunes, V.P.; de Carvalho Rosina, K.T.; Menna Barreto, A.P.M.; Souza, E.; Klein, M.R.S.T. High abdominal adiposity and low phase angle in overweight renal transplant recipients. Clin. Transplant 2019, 33, e13654. [Google Scholar] [CrossRef] [PubMed]
- Sarmento-Dias, M.; Santos-Araújo, C.; Poínhos, R.; Oliveira, B.; Sousa, M.; Simões-Silva, L.; Correia, F.; Pestana, M. Phase Angle Predicts Arterial Stiffness and Vascular Calcification in Peritoneal Dialysis Patients. Perit. Dial. Int. 2017, 37, 451–457. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar]
- Nigatu, Y.D.; Gebreyesus, S.H.; Allard, J.P.; Endris, B.S. The effect of malnutrition at admission on length of hospital stay among adult patients in developing country: A prospective cohort study. Clin. Nutr. ESPEN 2021, 41, 217–224. [Google Scholar] [CrossRef]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef] [PubMed]
- Leão, L.L.; Engedal, K.; Monteiro-Junior, R.S.; Tangen, G.G.; Krogseth, M. Malnutrition is associated with impaired functional status in older people receiving home care nursing service. Front. Nutr. 2021, 8, 684438. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, W.; Du, Y.; Zhang, J.; Zhang, Y.; Li, W.; Hu, W.; Zong, L.; Liu, Y.; Qin, H.; et al. A simple assessment model based on phase angle for malnutrition and prognosis in hospitalized cancer patients. Clin. Nutr. 2022, 41, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- González-Arellanes, R.; Urquidez-Romero, R.; Rodríguez-Tadeo, A.; Esparza-Romero, J.; Méndez-Estrada, R.O.; Ramírez-López, E.; Robles-Sardin, A.-E.; Pacheco-Moreno, B.-I.; Alemán-Mateo, H. High Hydration Factor in Older Hispanic-American Adults: Possible Implications for Accurate Body Composition Estimates. Nutrients 2019, 11, 2897. [Google Scholar] [CrossRef]
- Ritz, P.; Vol, S.; Berrut, G.; Tack, I.; Arnaud, M.J.; Tichet, J. Influence of gender and body composition on hydration and body water spaces. Clin. Nutr. 2008, 27, 740–746. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors and Year | Study Design | BIA Device and PhA Equation | Scientific Evidence |
|---|---|---|---|
| Curvello-Silva et al., 2020 [8] | Cross-sectional study |
| C |
| Barrea et al., 2019 [9] | Cross-sectional study |
| C |
| Shin et al., 2017 [10] | Retrospective observational study |
| C |
| Fernández-Jiménez et al., 2022 [11] | Retrospective observational study |
| C |
| Abe et al., 2021 [12] | Observational cohort study |
| B |
| Shin et al., 2022 [13] | Retrospective observational study |
| B |
| Han et al., 2018 [14] | Cross-sectional study |
| C |
| Han et al., 2019 [15] | Retrospective observational study |
| B |
| Silva et al., 2018 [16] | Prospective cohort study |
| B |
| de Oliveira-Filho et al., 2020 [17] | Cross-sectional study |
| C |
| Jun et al., 2021 [18] | Multicenter clinical study |
| B |
| Chen et al., 2020 [19] | Cross-sectional study |
| C |
| Fu et al., 2022 [20] | Observational retrospective study |
| C |
| Streb et al., 2020 [21] | Cross-sectional study |
| C |
| Ferreira et al., 2018 [22] | Cross-sectional study |
| C |
| Sarmento-Dias et al., 2017 [23] | Cross-sectional study |
| C |
| Authors and Year |
Sample Characteristics
| Main Outcomes |
|---|---|---|
| Curvello-Silva et al., 2020 [8] |
| Association between low PhA (<5°) and presence of hyperuricemia, adjusted by waist circumference, dysglycemia, and arterial hypertension (p = 0.018). |
| Barrea et al., 2019 [9] |
| BMI, sex and age were associated with PhA (β = −0.54, −0.32, −0.11, respectively; p ≤ 0.004). The lowest values of PhA were significantly associated with obesity (OR = 0.3) and 25(OH)D deficiency (OR = 0.2). The specific cut-off for 25(OH)D levels to predict the PhA above the median was >14 ng/mL (p < 0.001). |
| Shin et al., 2017 [10] |
| A positive correlation of PhA with albumin, BUN, creatinine, uric acid, and phosphorus (r = 0.37, 0.31, 0.50, 0.46, and 0.20; p < 0.05). A negative correlation of PhA with glucose and TCO2 (r = −0.22 and −0.19; p = 0.009 and 0.025). |
| Fernández-Jiménez et al., 2022 [11] |
| PhA cut-off for malnutrition diagnosis was 5.4°, 5.4° and 5.3°, in total sample, men and women, respectively. |
| Abe et al., 2021 [12] |
| Independent association between low PhA (<5.62° in men and <4.54° in women) and physical function (β = 0.201, p < 0.017), after adjustment. |
| Shin et al., 2022 [13] |
| Low PhA values were associated with the presence of sarcopenia, independent of age, sex, comorbidity index, eGFR, and uPCR (OR: 0.12; p = 0.001). |
| Han et al., 2018 [14] |
| Association between PhA and nutritional status (GNRI > 98 score, β = 0.152, p = 0.037). |
| Han et al., 2019 [15] |
| Albumin level (OR: 0.131; p < 0.001) was significantly associated with undernutrition (PhA < 4.17°) in the DMCKD5 group. |
| Silva et al., 2018 [16] |
| The mechanical ventilation time and European system for cardiac operative risk (EuroSCORE) were inversely associated with PhA in all three assessments (p = 0.05). |
| de Oliveira-Filho et al., 2020 [17] |
| Obese subjects had a higher PhA in comparison with eutrophic subjects (6.9 ± 0.9° vs. 6.5 ± 0.8°; p = 0.003). |
| Jun et al., 2021 [18] |
| Decrease in PhA with respect to age in DMT2 vs. control group. Decrease in PhA in patients with DMT2, and the changes were exacerbated over the disease duration. |
| Chen et al., 2020 [19] |
| NAFLD subjects had a higher PhA in comparison with non-NAFLD subjects (5.53 ± 0.66° vs. 5.43 ± 0.60°; p = 0.04). Association between PhA and the risk of NAFLD, after adjustment (OR = 1.40, p = 0.03). |
| Fu et al., 2022 [20] |
| BMI, sex, and age were associated with PhA (β = 0.006, 0.629, −0.014, respectively; p < 0.05). |
| Streb et al., 2020 [21] |
| An increase of 1% point in body fat representing a reduction of 0.065° in PhA, after adjustment (p < 0.001). |
| Ferreira et al., 2018 [22] |
| PhA was inversely and significantly correlated with waist-to-height ratio and body shape index, r = −0.22, −0.21, respectively; p < 0.05. |
| Sarmento-Dias et al., 2017 [23] |
| Low PhA (<6°) had higher CRP, AI, and SCS values, and lower serum albumin and fetuin-A levels compared with patients with high PhA (≥6°). Association between PhA and arterial stiffness, after adjustment (β = −0.266, p = 0.088). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Praget-Bracamontes, S.; González-Arellanes, R.; Aguilar-Salinas, C.A.; Martagón, A.J. Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1608. https://doi.org/10.3390/ijerph20021608
Praget-Bracamontes S, González-Arellanes R, Aguilar-Salinas CA, Martagón AJ. Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(2):1608. https://doi.org/10.3390/ijerph20021608
Chicago/Turabian StylePraget-Bracamontes, Samantha, Rogelio González-Arellanes, Carlos A. Aguilar-Salinas, and Alexandro J. Martagón. 2023. "Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 2: 1608. https://doi.org/10.3390/ijerph20021608
APA StylePraget-Bracamontes, S., González-Arellanes, R., Aguilar-Salinas, C. A., & Martagón, A. J. (2023). Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review. International Journal of Environmental Research and Public Health, 20(2), 1608. https://doi.org/10.3390/ijerph20021608