


Examination of Preferences for COVID-19 Vaccines in Hungary Based on Their Properties—Examining the Impact of Pandemic Awareness with a Hybrid Choice Approach

 ,
,  ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Process of the Research
- (1)
- country of origin (USA/European Union/Hungary/Russia/China);
- (2)
- type of technology used in the production (old/new);
- (3)
- the effectiveness of the vaccine (60–70%/71–90%/more than 90%);
- (4)
- the type of possible side effect (according to the package leaflet/long-term);
- (5)
- duration of protection provided by the vaccine (6 months/12 months/lifelong);
- (6)
- the number of doses required to develop protection (1 dose/2 dose);
- (7)
- the price of the vaccine (HUF 2000/HUF 6000/HUF 10,000/HUF 14,000).
2.2. Methodology
- −
- Since the existence of the pandemic, he has avoided personal contact with friends and acquaintances and group gatherings;
- −
- Since the end of the pandemic, wash your hands thoroughly (for at least 20 s) with running water or clean your hands with an alcoholic hand sanitizer several times a day;
- −
- Since the end of the pandemic, always wear a mask and maintain a protective distance of 1.5 m as required;
- −
- Routinely cleans/disinfects frequently touched surfaces (such as tables, door handles, light switches, handles, desks, toilets, taps, sinks, and cell phones) since the pandemic has occurred;
- −
- Avoid large crowds, and crowded, confined spaces (e.g., public transportation, shopping malls) since the pandemic;
- −
- You have been keeping over-the-counter medications at home since the pandemic that may help you get through the virus (such as painkillers and antipyretics).
3. Results
3.1. Descriptive Statistics of the Sample, the Evaluation Statements Examined and the Other Issues Related to the COVID-19 Situation
3.2. Discrete Choice Model Estimates in Preference Space
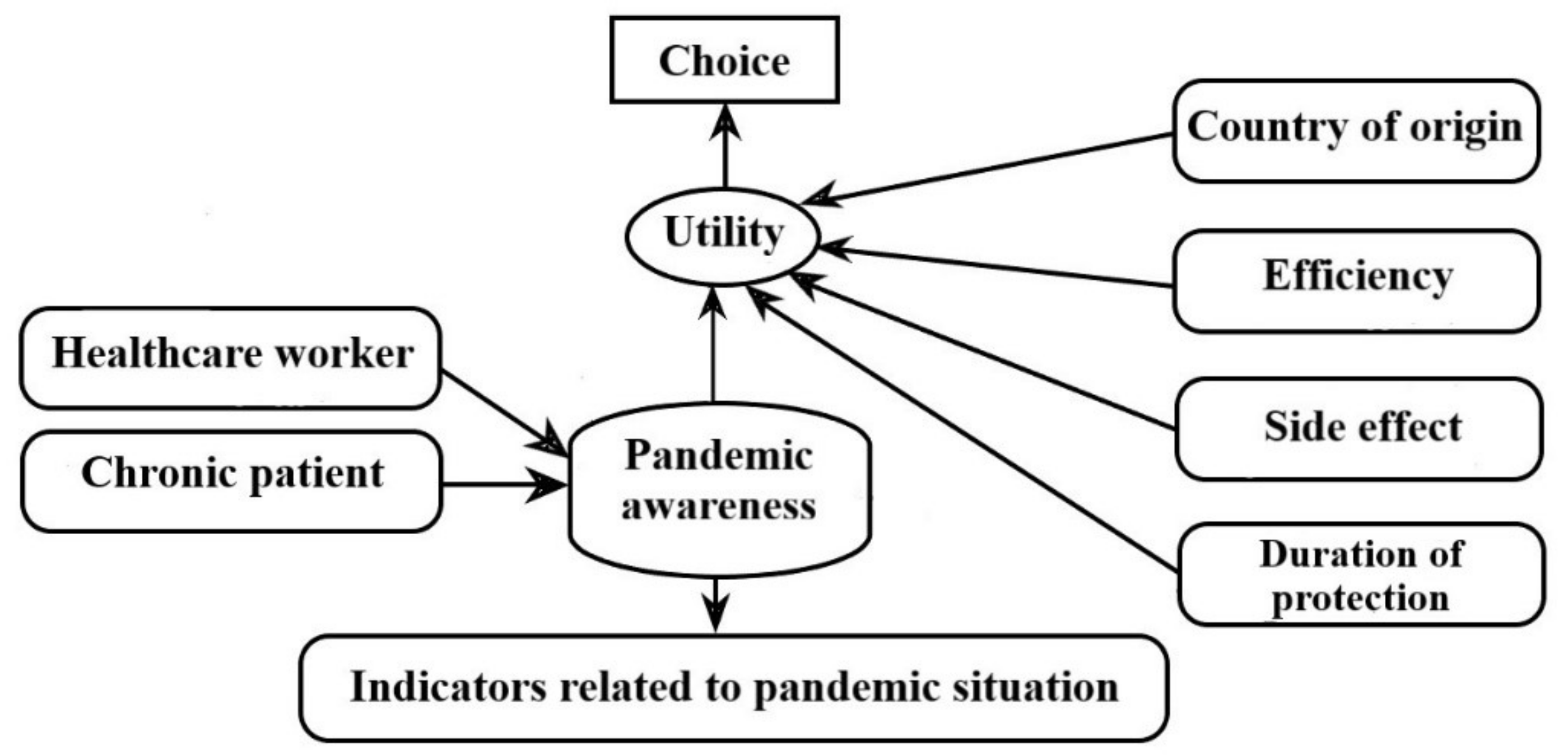
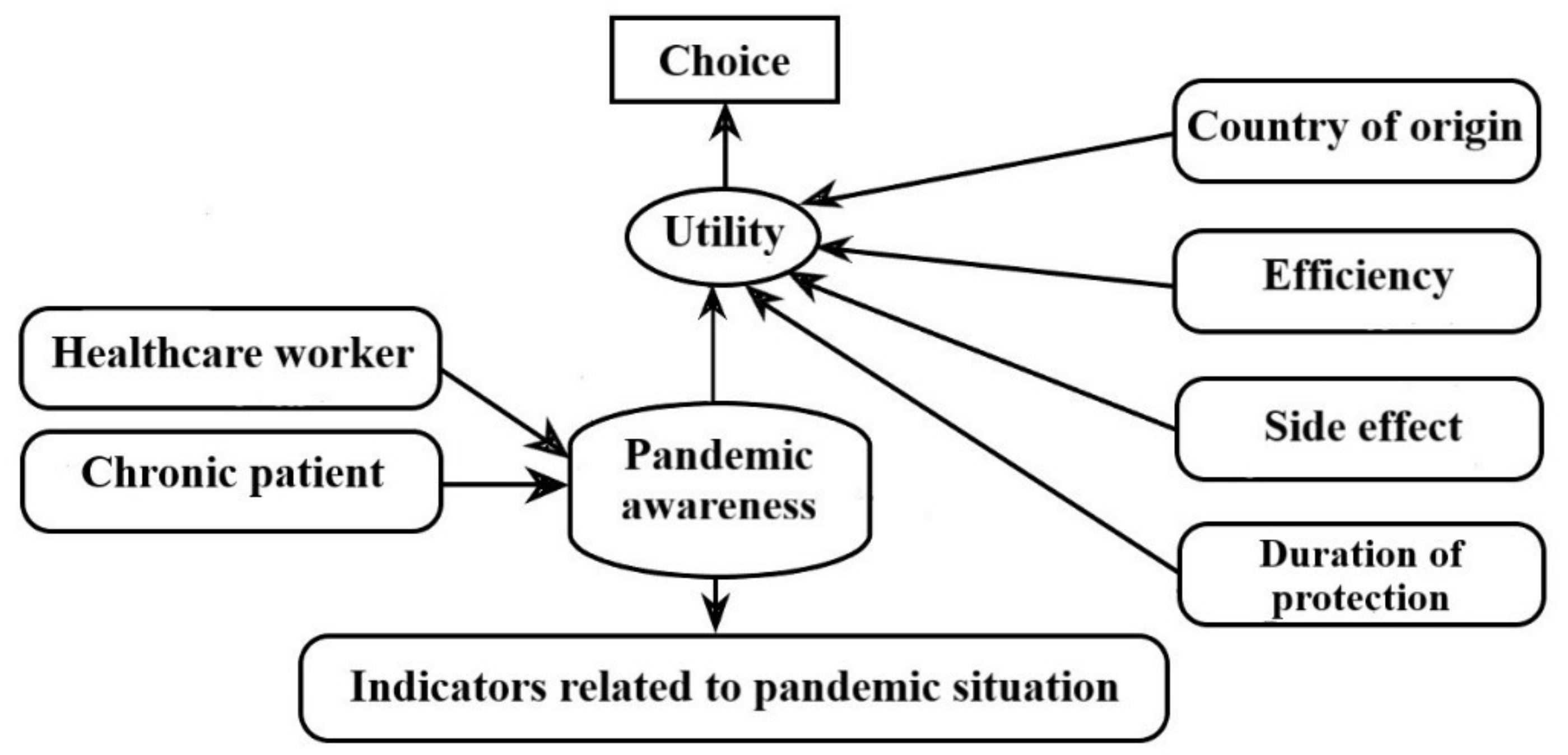
3.3. Parameter Estimates of the Structural and Measurement Equations for the Hybrid Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Measurement Equation Threshold Parameters | HRPL Model | |
|---|---|---|
| Estimates | t-Ratio | |
| −1.54 * | −23.01 | |
| −0.95 * | −17.80 | |
| 0.11 * | 2.35 | |
| 0.94 * | 17.30 | |
| −2.21 * | −21.90 | |
| −1.74 * | −23.00 | |
| −1.00 * | −18.14 | |
| −0.21 * | −4.54 | |
| −2.67 * | −18.68 | |
| −2.12 * | −22.20 | |
| −1.29 * | −20.78 | |
| −0.26 * | −5.43 | |
| −1.96 * | −23.26 | |
| −1.24 * | −21.95 | |
| −0.47 * | −10.40 | |
| 0.40 * | 8.78 | |
| −2.02 * | −22.84 | |
| −1.38 * | −21.70 | |
| −0.48 * | −9.87 | |
| 0.32 * | 6.66 | |
| −1.17 * | −21.75 | |
| −0.71 * | −15.34 | |
| −0.18 * | −4.31 | |
| 0.30 * | 6.84 | |
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 16 October 2022).
- Anand, P.; Stahel, V.P. Review the safety of COVID-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, COVID-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- Vanaparthy, R.; Mohan, G.; Vasireddy, D.; Atluri, P. Review of COVID-19 viral vector-based vaccines and COVID-19 variants. Infez. Med. 2021, 29, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, H.; Lv, J.; Huang, T.; Zhang, R.; Zhang, D.; Luo, L.; Wei, S.; Liu, X.; Zhang, S.; et al. Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus. Vaccines 2022, 10, 1020. [Google Scholar] [CrossRef]
- Heinz, F.X.; Stiasny, K. Profiles of current COVID-19 vaccines. Wien. Klin. Wochenschr. 2021, 133, 271–283. [Google Scholar] [CrossRef]
- Nizigiyimana, A.; Acharya, D.; Morillon, G.F.; Poder, T.G. Predictors of Vaccine Acceptance, Confidence, and Hesitancy in General, and COVID-19 Vaccination Refusal in the Province of Quebec, Canada. Patient Prefer. Adherence 2022, 16, 2181–2202. [Google Scholar] [CrossRef]
- Kutasi, K.; Koltai, J.; Szabo-Morvai, A.; Rost, G.; Karsai, M.; Biro, P.; Lengyel, B. Understanding hesitancy with revealed preferences across COVID-19 vaccine types. Sci. Rep. 2022, 12, 13293. [Google Scholar] [CrossRef]
- Coronavirus Vaccines to be Voluntary and Free of Charge. Available online: https://abouthungary.hu/news-in-brief/coronavirus-vaccines-to-be-voluntary-and-free-of-charge (accessed on 28 December 2022).
- Debrecen Népessége. Available online: http://nepesseg.com/hajdu-bihar/debrecen (accessed on 16 October 2022).
- Ngene 1.2 User Manual & Reference Guide. Available online: http://www.choice-metrics.com/NgeneManual120.pdf (accessed on 16 October 2022).
- Rose, J.M.; Bliemer, M.C. Constructing efficient stated choice experimental designs. Transp. Rev. 2009, 29, 587–617. [Google Scholar]
- Bliemer, M.C.; Rose, J.M.; Hess, S. Approximation of Bayesian efficiency in experimental choice designs. J. Choice Model. 2008, 1, 98–126. [Google Scholar] [CrossRef]
- McFadden, D. Conditional logit analysis of qualitative choice behavior. Front. Econom. 1974, 105–142. [Google Scholar]
- Ben-Akiva, M.E.; Lerman, S.R.; Lerman, S.R. Discrete Choice Analysis: Theory and Application to Travel Demand; MIT Press: Cambridge, MA, USA, 1985; Volume 9. [Google Scholar]
- McFadden, D.; Train, K. Mixed MNL Models for Discrete Response. J. Appl. Econom. 2000, 15, 447–470. [Google Scholar] [CrossRef]
- Ben-Akiva, M.; McFadden, D.; Train, K.; Walker, J.; Bhat, C.; Bierlaire, M.; Bolduc, D.; Boersch-Supan, A.; Brownstone, D.; Bunch, D.S.; et al. Hybrid Choice Models: Progress and Challenges. Mark. Lett. 2002, 13, 163–175. [Google Scholar] [CrossRef] [Green Version]
- Ben-Akiva, M.; Walker, J.; Bernardino, A.T.; Gopinath, D.A.; Morikawa, T.; Polydoropoulou, A. Integration of choice and latent variable models. In Perpetual Motion: Travel Behaviour Research Opportunities and Application Challenges; Transportation Research Board: Oxford, UK, 2002; Volume 2002, pp. 431–470. [Google Scholar]
- Bolduc, D.; Ben-Akiva, M.; Walker, J.; Michaud, A. Hybrid Choice Models. In Integrated Land-Use and Transportation Models; Lee-Gosselin, M.E.H., Doherty, S.T., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2005; pp. 275–302. [Google Scholar]
- Webpage of the National Public Health Center: ‘General Precautions against New Coronavirus Infections’. Available online: https://www.nnk.gov.hu/index.php/koronavirus-tajekoztato/540-altalanos-ovintezkedesek-az-uj-koronavirus-fertozessel-kapcsolatban (accessed on 28 December 2022).
- Hess, S.; Palma, D. Apollo: A flexible, powerful and customisable freeware package for choice model estimation and application. J. Choice Model. 2019, 32, 100170. [Google Scholar] [CrossRef]
- Hess, S.; Palma, D. Apollo Version 0.2.8, User Manual. Available online: www.ApolloChoiceModelling.com (accessed on 6 January 2023).
- RC Team. R: A Language and Environment for Statistical Computing; RC Team: Firminy, France, 2020. [Google Scholar]
- De Terwangne, C.; Laouni, J.; Jouffe, L.; Lechien, J.R.; Bouillon, V.; Place, S.; Capulzini, L.; Machayekhi, S.; Ceccarelli, A.; Saussez, S.; et al. Predictive Accuracy of COVID-19 World Health Organization (WHO) Severity Classification and Comparison with a Bayesian-Method-Based Severity Score (EPI-SCORE). Pathogens 2020, 9, 880. [Google Scholar] [CrossRef]
- Clinical Spectrum of SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 28 December 2022).
- Train, K.; Hess, S.; Polak, J. On the Use of a Modified Latin Hypercube Sampling (MLHS) Method in the Estimation of a Mixed Logit Model for Vehicle Choice. Transp. Res. Part B Methodol. 2006, 40, 147–163. [Google Scholar] [CrossRef] [Green Version]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Roy, D.N.; Biswas, M.; Islam, E.; Azam, M.S. Potential factors influencing COVID-19 vaccine acceptance and hesitancy: A systematic review. PLoS ONE 2022, 17, e0265496. [Google Scholar] [CrossRef]
- Biro-Nagy, A.; Szaszi, A.J. The roots of COVID-19 vaccine hesitancy: Evidence from Hungary. J. Behav. Med. 2022. [Google Scholar] [CrossRef]
- EU’s Vaccine Portfolio. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/safe-covid-19-vaccines-europeans_en#eus-vaccine-portfolio (accessed on 16 October 2022).
- Dror, A.A.; Daoud, A.; Morozov, N.G.; Layous, E.; Eisenbach, N.; Mizrachi, M.; Rayan, D.; Bader, A.; Francis, S.; Kaykov, E.; et al. Vaccine hesitancy due to vaccine country of origin, vaccine technology, and certification. Eur. J. Epidemiol. 2021, 36, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. E Clin. Med. 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open. 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Steinert, J.I.; Sternberg, H.; Prince, H.; Fasolo, B.; Galizzi, M.M.; Buthe, T.; Veltri, G.A. COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci. Adv. 2022, 8, eabm9825. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, 2021726118. [Google Scholar] [CrossRef]
- Pires, C. Global Predictors of COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 1349. [Google Scholar] [CrossRef]
| Vaccine 1 | Vaccine 2 | Vaccine 3 | No Choice | |
|---|---|---|---|---|
| Country of origin | USA | China | Russia | |
| Type of technology | Old | New | Old | |
| Efficiency (%) | More than 90 | 60–70 | 71–90 | |
| Side effect | According to the package leaflet | According to the package leaflet | Long-term | |
| Duration of protection | Lifelong | 12 months | 12 months | |
| Number of the dose required | 2 doses | 1 dose | 2 doses | |
| Price (HUF) | 6000 | 6000 | 2000 | |
| Your choice (X): |
| Vaccine Attribute | Description of the Attribute | Levels of the Attribute |
|---|---|---|
| Country of origin | Production country of the vaccine. | USA European Union Hungary Russia China |
| Efficiency (%) | Efficiency level of the vaccine against the COVID-19 virus is expressed as a percentage. | 60–70 71–90 More than 90 |
| Side effect | Type of potential side effect after vaccination. | According to the package leaflet Long-term |
| Duration of protection | The duration of the period of protection is guaranteed by the producer after vaccination. | 6 months 12 months Lifelong |
| Vaccine 1 | Vaccine 2 | Vaccine 3 | No Choice | |
|---|---|---|---|---|
| Country of origin | China | European Union | USA | |
| Efficiency (%) | More than 90 | 71–90 | 60–70 | |
| Side effect | Long-term | According to the package leaflet | According to the package leaflet | |
| Duration of protection | 12 months | Lifelong | 12 months | |
| Your choice (X): |
| Characteristic | Sample ( n= 1011) | |
|---|---|---|
| Count | Percentage | |
| Gender | ||
| Male | 447 | 44.2 |
| Female | 564 | 55.8 |
| Age category | ||
| 18–29 | 383 | 37.9 |
| 30–45 | 393 | 38.9 |
| 46–60 | 210 | 20.8 |
| 61–75 | 25 | 2.4 |
| Highest level of education | ||
| Primary | 62 | 6.1 |
| Secondary | 553 | 54.7 |
| Higher (minimum BSc) | 396 | 39.2 |
| Residence category | ||
| Debrecen | 685 | 67.8 |
| Another town in Hajdú-Bihar county | 221 | 21.8 |
| Another township in Hajdú-Bihar county | 84 | 8.3 |
| Other | 21 | 2.1 |
| Statement * | 1 (%) | 2 (%) | 1 + 2 (%) | 3 (%) | 4 (%) | 5 (%) | 4 + 5 (%) |
|---|---|---|---|---|---|---|---|
| Statement 1 | 8.3 | 11.5 | 19.8 | 34.2 | 26.0 | 20.0 | 46.0 |
| Statement 2 | 2.4 | 3.5 | 5.9 | 12.7 | 24.1 | 57.3 | 81.4 |
| Statement 3 | 0.9 | 2.1 | 3.0 | 9.7 | 28.3 | 59.0 | 87.3 |
| Statement 4 | 3.4 | 8.9 | 12.3 | 20.8 | 31.3 | 35.6 | 66.9 |
| Statement 5 | 3.7 | 7.3 | 11.0 | 22.6 | 27.5 | 38.9 | 66.4 |
| Statement 6 | 13.4 | 11.7 | 25.1 | 18.1 | 17.9 | 38.9 | 56.8 |
| Question | |
|---|---|
| Have you been infected with COVID-19? (%) | |
| Yes | 21.4 |
| No | 78.6 |
| If so, how severe your symptoms were? (1–10) | |
| Mean (standard deviation) | 4.9 (2.5) |
| Do you have a chronic illness? (%) | |
| Yes | 19.5 |
| No | 80.5 |
| Are you a healthcare worker? (%) | |
| Yes | 17.3 |
| No | 82.7 |
| Have you already received any vaccine against COVID-19? (%) | |
| I got a vaccine | 37.8 |
| I received both vaccinations | 62.2 |
| If so, which vaccine did you receive? (%) | |
| Vaxzevria (AstraZeneca) | 4.6 |
| Spikevax (Moderna) | 3.5 |
| SARS-CoV-2/Vero Cell inactivated (Sinopharm) | 32.0 |
| Sputnik (Russian Gamaleja) | 17.8 |
| Comirnaty (Pfizer) | 42.1 |
| Why did you decide to vaccinate yourself (select only one option)? (%) | |
| Media/News | 2.8 |
| Healthcare professional | 12.9 |
| Family/Acquaintance | 11.8 |
| Workplace | 8.1 |
| My own decision | 61.6 |
| Other | 2.8 |
| What was the main reason for choosing COVID-19 vaccination (select only one option)? (%) | |
| Protecting your health | 36.4 |
| Protecting family/acquaintance | 33.6 |
| Vaccine passport (security certificate) | 20.9 |
| Workplace | 6.9 |
| Other | 2.2 |
| Attributes and Descriptive Data of the Model | RPL Model | HRPL Model | ||
|---|---|---|---|---|
| Estimates | t-Ratio | Estimates | t-Ratio | |
| ASC (reference category: Choice of a vaccine alternative) | ||||
| No choice | −1.70 * | −21.62 | −3.18 * | −12.22 |
| Country of origin (reference category: China) | ||||
| USA | 0.52 * | 5.41 | 0.69 * | 7.39 |
| USA (standard deviation) | 1.80 * | 15.99 | 1.60 * | 14.51 |
| European Union | 1.36 * | 14.10 | 1.29 * | 14.28 |
| European Union (standard deviation) | 1.92 * | 19.15 | 1.86 * | 17.76 |
| Hungary | 1.28 * | 12.12 | 1.27 * | 12.98 |
| Hungary (standard deviation) | 2.14 * | 19.08 | 1.94 * | 17.04 |
| Russia | 0.40 * | 4.09 | 0.41 * | 4.67 |
| Russia (standard deviation) | 1.75 * | 15.90 | 1.51 * | 13.56 |
| Efficiency (reference category: More than 90%) | ||||
| 60–70% | −1.48 * | −19.96 | −1.47 * | −20.14 |
| 60–70% (Standard deviation) | 1.24 * | 13.57 | 1.04 * | 12.13 |
| 71–90% | −0.64 * | −10.59 | −0.60 * | −11.07 |
| 71–90% (Standard deviation) | 0.86 * | 10.25 | 0.50 * | 4.93 |
| Side effect (reference category: Long-term) | ||||
| In accordance with the package leaflet | 1.17 * | 15.11 | 1.08 * | 15.01 |
| In accordance with the package leaflet (Standard deviation) | 1.77 * | 21.98 | 1.69 * | 20.85 |
| Duration of protection (reference category: Lifelong) | ||||
| 6 months | −2.91 * | −27.17 | −2.84 * | −27.09 |
| 6 months (Standard deviation) | 1.55 * | 13.84 | 1.49 * | 14.12 |
| 12 months | −1.73 * | −23.71 | −1.65 * | −23.48 |
| 12 months (Standard deviation) | 1.28 * | 16.43 | 1.20 * | 15.22 |
| λ | - | - | −2.96 * | −12.31 |
| Individuals | 1009 | |||
| Observations | 8072 | |||
| Parameters | 19 | 20 | ||
| Log-likelihood (0) (for choice model) | −11,190.17 | −11,190.17 | ||
| Log-likelihood (final) (for choice model) | −8301.26 | −7905.16 | ||
| 0.26 | 0.29 | |||
| AIC | 16,640.51 | 31,627.91 | ||
| BIC | 16,773.44 | 31,991.71 | ||
| Structural Equation Parameters | HRPL Model | |
|---|---|---|
| Estimates | t-Ratio | |
| −0.39 * | −4.22 | |
| 0.34 * | 3.44 | |
| Measurement Equation Parameters | Estimates | t-Ratio |
| 0.51 * | 9.97 | |
| 0.51 * | 8.71 | |
| 0.53 * | 9.00 | |
| 0.40 * | 8.02 | |
| 0.54 * | 9.95 | |
| 0.34 * | 6.98 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blaga, Z.; Czine, P.; Takacs, B.; Szilagyi, A.; Szekeres, R.; Wachal, Z.; Hegedus, C.; Buchholcz, G.; Varga, B.; Priksz, D.; et al. Examination of Preferences for COVID-19 Vaccines in Hungary Based on Their Properties—Examining the Impact of Pandemic Awareness with a Hybrid Choice Approach. Int. J. Environ. Res. Public Health 2023, 20, 1270. https://doi.org/10.3390/ijerph20021270
Blaga Z, Czine P, Takacs B, Szilagyi A, Szekeres R, Wachal Z, Hegedus C, Buchholcz G, Varga B, Priksz D, et al. Examination of Preferences for COVID-19 Vaccines in Hungary Based on Their Properties—Examining the Impact of Pandemic Awareness with a Hybrid Choice Approach. International Journal of Environmental Research and Public Health. 2023; 20(2):1270. https://doi.org/10.3390/ijerph20021270
Chicago/Turabian StyleBlaga, Zsanett, Peter Czine, Barbara Takacs, Anna Szilagyi, Reka Szekeres, Zita Wachal, Csaba Hegedus, Gyula Buchholcz, Balazs Varga, Daniel Priksz, and et al. 2023. "Examination of Preferences for COVID-19 Vaccines in Hungary Based on Their Properties—Examining the Impact of Pandemic Awareness with a Hybrid Choice Approach" International Journal of Environmental Research and Public Health 20, no. 2: 1270. https://doi.org/10.3390/ijerph20021270
APA StyleBlaga, Z., Czine, P., Takacs, B., Szilagyi, A., Szekeres, R., Wachal, Z., Hegedus, C., Buchholcz, G., Varga, B., Priksz, D., Bombicz, M., Szabo, A. M., Kiss, R., Gesztelyi, R., Romanescu, D. D., Szabo, Z., Szucs, M., Balogh, P., Szilvassy, Z., & Juhasz, B. (2023). Examination of Preferences for COVID-19 Vaccines in Hungary Based on Their Properties—Examining the Impact of Pandemic Awareness with a Hybrid Choice Approach. International Journal of Environmental Research and Public Health, 20(2), 1270. https://doi.org/10.3390/ijerph20021270