
Comparison of Pre-Diagnosis Physical Activity and Its Correlates between Lung and Other Cancer Patients: Accelerometer Data from the UK Biobank Prospective Cohort

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Methods
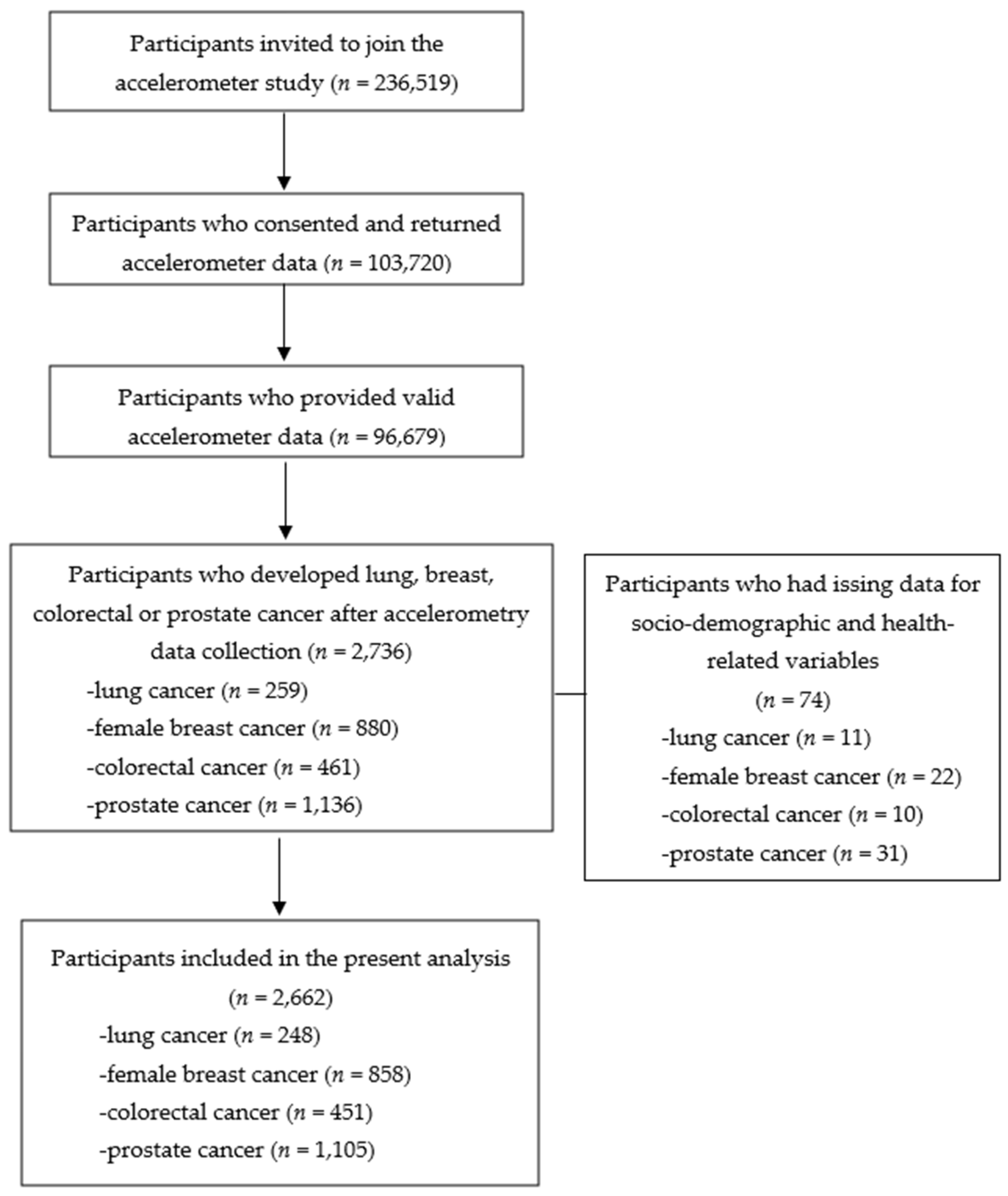
2.1. Data Source and Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Characteristics of Participants
3.2. Comparison of Pre-Diagnosis PA
3.3. Comparison of Correlates of Pre-Diagnosis PA
3.4. Survival Analysis
4. Discussion
4.1. Pre-Diagnosis MVPA
4.2. Correlates of PA
4.3. Pre-Diagnosis PA and All-Cause Mortality
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Fuller, J.T.; Hartland, M.C.; Maloney, L.; Davison, K. Therapeutic effects of aerobic and resistance exercises for cancer survivors: A systematic review of meta-analyses of clinical trials. Br. J. Sports Med. 2018, 52, 1311. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr 2020, 4, pkz080. [Google Scholar] [CrossRef]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sport. Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyl, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V. Nutrition and Physical Activity Guidelines for Cancer Survivors. CA Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef]
- Troeschel, A.N.; Leach, C.R.; Shuval, K.; Stein, K.D.; Patel, A.V. Physical Activity in Cancer Survivors During “Re-Entry” Following Cancer Treatment. Prev. Chronic Dis. 2018, 15, E65. [Google Scholar] [CrossRef] [PubMed]
- Forbes, C.C.; Blanchard, C.M.; Mummery, W.K.; Courneya, K.S. A comparison of physical activity correlates across breast, prostate and colorectal cancer survivors in Nova Scotia, Canada. Support. Care Cancer 2014, 22, 891–903. [Google Scholar] [CrossRef]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Thraen-Borowski, K.M.; Gennuso, K.P.; Cadmus-Bertram, L. Accelerometer-derived physical activity and sedentary time by cancer type in the United States. PLoS ONE 2017, 12, e0182554. [Google Scholar] [CrossRef]
- Courneya, K.S.; Friedenreich, C.M. Physical activity and cancer control. Semin. Oncol. Nurs. 2007, 23, 242–252. [Google Scholar] [CrossRef]
- Schmitz, K.H. Exercise Oncology: Prescribing Physical Activity before and after a Cancer Diagnosis; Springer Nature: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef]
- Schmid, D.; Leitzmann, M. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: A systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1293–1311. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Guo, F.; Ye, J.; Li, Y.; Shi, D.; Fang, D.; Guo, J.; Li, L. Pre-and post-diagnosis physical activity is associated with survival benefits of colorectal cancer patients: A systematic review and meta-analysis. Oncotarget 2016, 7, 52095. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sport. Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Depenbusch, J.; Haussmann, A.; Tsiouris, A.; Schmidt, L.; Hermann, S.; Sieverding, M.; Wiskemann, J.; Ungar, N. Change patterns and determinants of physical activity differ between breast, prostate, and colorectal cancer patients. Support. Care Cancer 2020, 28, 3207–3218. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Wiskemann, J.; Ulrich, C.M.; Schneeweiss, A.; Steindorf, K. Self-reported physical activity behavior of breast cancer survivors during and after adjuvant therapy: 12 months follow-up of two randomized exercise intervention trials. Acta Oncol. 2017, 56, 618–627. [Google Scholar] [CrossRef]
- Boyle, T.; Vallance, J.K.; Ransom, E.K.; Lynch, B.M. How sedentary and physically active are breast cancer survivors, and which population subgroups have higher or lower levels of these behaviors? Support. Care Cancer 2016, 24, 2181–2190. [Google Scholar] [CrossRef]
- Puleo, G.E.; Borger, T.; Bowling, W.R.; Burris, J.L. The State of the Science on Cancer Diagnosis as a “Teachable Moment” for Smoking Cessation: A Scoping Review. Nicotine Tob. Res. 2021, 24, 160–168. [Google Scholar] [CrossRef]
- Bluethmann, S.M.; Basen-Engquist, K.; Vernon, S.W.; Cox, M.; Gabriel, K.P.; Stansberry, S.A.; Carmack, C.L.; Blalock, J.A.; Demark-Wahnefried, W. Grasping the ‘teachable moment’: Time since diagnosis, symptom burden and health behaviors in breast, colorectal and prostate cancer survivors. Psychooncology 2015, 24, 1250–1257. [Google Scholar] [CrossRef]
- World Health Organization. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 18 November 2021).
- Granger, C.L.; Connolly, B.; Denehy, L.; Hart, N.; Antippa, P.; Lin, K.Y.; Parry, S.M. Understanding factors influencing physical activity and exercise in lung cancer: A systematic review. Support. Care Cancer 2017, 25, 983–999. [Google Scholar] [CrossRef]
- Shephard, R.J. Limits to the measurement of habitual physical activity by questionnaires. Br. J. Sport. Med. 2003, 37, 197–206. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Perez-Bravo, F.; Ibanez, L.; Salas, C.; Bailey, M.E.; Gill, J.M. Objective vs. self-reported physical activity and sedentary time: Effects of measurement method on relationships with risk biomarkers. PLoS ONE 2012, 7, e36345. [Google Scholar] [CrossRef]
- Douma, J.A.J.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Jansen, F.; Langendijk, J.A.; Baatenburg de Jong, R.J.; Terhaard, C.H.J.; Takes, R.P.; Chinapaw, M.J.; Altenburg, T.M.; et al. Demographic, clinical and lifestyle-related correlates of accelerometer assessed physical activity and fitness in newly diagnosed patients with head and neck cancer. Acta Oncol. 2020, 59, 342–350. [Google Scholar] [CrossRef]
- Buffart, L.M.; Thong, M.S.; Schep, G.; Chinapaw, M.J.; Brug, J.; van de Poll-Franse, L.V. Self-reported physical activity: Its correlates and relationship with health-related quality of life in a large cohort of colorectal cancer survivors. PLoS ONE 2012, 7, e36164. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B.M.; Boyle, T.; Winkler, E.; Occleston, J.; Courneya, K.S.; Vallance, J.K. Patterns and correlates of accelerometer-assessed physical activity and sedentary time among colon cancer survivors. Cancer Causes Control 2016, 27, 59–68. [Google Scholar] [CrossRef]
- Kampshoff, C.S.; Stacey, F.; Short, C.E.; van Mechelen, W.; Chinapaw, M.J.; Brug, J.; Plotnikoff, R.; James, E.L.; Buffart, L.M. Demographic, clinical, psychosocial, and environmental correlates of objectively assessed physical activity among breast cancer survivors. Support. Care Cancer 2016, 24, 3333–3342. [Google Scholar] [CrossRef] [PubMed]
- Doherty, A.; Jackson, D.; Hammerla, N.; Plotz, T.; Olivier, P.; Granat, M.H.; White, T.; van Hees, V.T.; Trenell, M.I.; Owen, C.G.; et al. Large Scale Population Assessment of Physical Activity Using Wrist Worn Accelerometers: The UK Biobank Study. PLoS ONE 2017, 12, e0169649. [Google Scholar] [CrossRef]
- Hildebrand, M.; van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sport. Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef]
- O’Donnell, J.; Smith-Byrne, K.; Velardo, C.; Conrad, N.; Salimi-Khorshidi, G.; Doherty, A.; Dwyer, T.; Tarassenko, L.; Rahimi, K. Self-reported and objectively measured physical activity in people with and without chronic heart failure: UK Biobank analysis. Open Heart 2020, 7, e001099. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.; Oguz, M.; Carroll, R.; Thakkar, P.; Yang, F. Comparison of accelerometer-derived physical activity levels between individuals with and without cancer: A UK Biobank study. Future Oncol. 2019, 15, 3763–3774. [Google Scholar] [CrossRef]
- Barker, J.; Smith Byrne, K.; Doherty, A.; Foster, C.; Rahimi, K.; Ramakrishnan, R.; Woodward, M.; Dwyer, T. Physical activity of UK adults with chronic disease: Cross-sectional analysis of accelerometer-measured physical activity in 96 706 UK Biobank participants. Int. J. Epidemiol. 2019, 48, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- UK Biobank. Grip Strength. Available online: https://biobank.ndph.ox.ac.uk/ukb/ukb/docs/Gripstrength.pdf (accessed on 30 March 2021).
- Lowe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brahler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Routledge: London, UK, 1988. [Google Scholar]
- Sweegers, M.; Boyle, T.; Vallance, J.; Chinapaw, M.; Brug, J.; Aaronson, N.; D’Silva, A.; Kampshoff, C.; Lynch, B.; Nollet, F. Which cancer survivors are at risk for a physically inactive and sedentary lifestyle? Results from pooled accelerometer data of 1447 cancer survivors. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 66. [Google Scholar] [CrossRef]
- D’Silva, A.; Bebb, G.; Boyle, T.; Johnson, S.T.; Vallance, J.K. Demographic and clinical correlates of accelerometer assessed physical activity and sedentary time in lung cancer survivors. Psychooncology 2018, 27, 1042–1049. [Google Scholar] [CrossRef]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Gray, S.; Petermann, F.; Iliodromiti, S.; Welsh, P.; Lyall, D.M.; Anderson, J.; Pellicori, P.; Mackay, D.F.; Pell, J.P.; et al. Walking Pace Is Associated with Lower Risk of All-Cause and Cause-Specific Mortality. Med. Sci. Sport. Exerc. 2019, 51, 472–480. [Google Scholar] [CrossRef]
- Middleton, A.; Fulk, G.D.; Beets, M.W.; Herter, T.M.; Fritz, S.L. Self-Selected Walking Speed is Predictive of Daily Ambulatory Activity in Older Adults. J. Aging Phys. Act. 2016, 24, 214–222. [Google Scholar] [CrossRef]
- Montoye, A.H.K.; Clevenger, K.A.; Pfeiffer, K.A.; Nelson, M.B.; Bock, J.M.; Imboden, M.T.; Kaminsky, L.A. Development of cut-points for determining activity intensity from a wrist-worn ActiGraph accelerometer in free-living adults. J. Sport. Sci. 2020, 38, 2569–2578. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Shaw, E.; Neilson, H.K.; Brenner, D.R. Epidemiology and biology of physical activity and cancer recurrence. J. Mol. Med. 2017, 95, 1029–1041. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Female | Male | ||||||
|---|---|---|---|---|---|---|---|---|
| Lung (n = 129) | Breast (n = 858) | Colorectal (n = 194) | p Value a | Lung (n = 119) | Prostate (n = 1105) | Colorectal (n = 257) | p Value b | |
| Socio-demographics | ||||||||
| Age at accelerometer study, mean (SD) | 66.09 (5.81) | 62.82 (7.50) | 65.74 (6.59) | <0.001 | 68.44 (5.89) | 67.95 (5.66) | 66.94 (6.50) | <0.05 |
| Age at cancer diagnosis, mean (SD) | 68.81 (5.96) | 65.33 (7.64) | 68.25 (6.77) | <0.001 | 71.32 (5.97) | 69.72 (5.64) | 69.52 (6.82) | <0.05 |
| White race, % | 97.67 | 97.44 | 96.91 | 0.894 | 97.48 | 97.92 | 98.83 | 0.571 |
| Townsend Index of deprivation, mean (SD) | −0.96 (3.12) | −1.71 (2.73) | −1.41 (3.02) | <0.05 | −1.31 (3.13) | −2.05 (2.60) | −1.78 (2.78) | <0.01 |
| BMI, % Underweight | 0.78 | 0.93 | 1.03 | 0.226 | 0.00 | 0.09 | 0.00 | <0.05 |
| Normal | 35.66 | 40.79 | 39.18 | 23.53 | 27.15 | 24.51 | ||
| Overweight | 35.66 | 40.09 | 36.60 | 42.86 | 53.57 | 52.53 | ||
| Obese | 27.91 | 18.18 | 23.20 | 33.61 | 19.19 | 22.96 | ||
| Smoking status, % | <0.001 | <0.001 | ||||||
| Never | 27.13 | 57.46 | 45.88 | 15.97 | 48.05 | 45.91 | ||
| Previous | 60.39 | 36.25 | 51.03 | 58.82 | 46.06 | 44.36 | ||
| Current | 22.48 | 6.29 | 3.09 | 25.21 | 5.88 | 9.73 | ||
| Alcohol drinking frequency, % | 0.143 | <0.01 | ||||||
| ≤1–3 times/month | 37.21 | 29.37 | 36.08 | 27.73 | 16.20 | 14.01 | ||
| 1–4 times/week | 41.09 | 49.18 | 41.75 | 41.18 | 52.94 | 48.64 | ||
| Daily or almost daily | 21.71 | 21.45 | 22.16 | 31.09 | 30.86 | 37.35 | ||
| Health-related characteristics | ||||||||
| Overall health rating, % | <0.05 | <0.001 | ||||||
| Excellent | 10.85 | 19.93 | 20.10 | 10.08 | 21.54 | 16.73 | ||
| Good | 63.57 | 64.69 | 64.43 | 50.42 | 60.54 | 61.09 | ||
| Fair | 18.60 | 12.94 | 13.40 | 32.77 | 16.65 | 19.46 | ||
| Poor | 6.98 | 2.45 | 2.06 | 6.72 | 1.27 | 2.72 | ||
| No. of comorbidities, % | 0.149 | <0.001 | ||||||
| 0 | 56.59 | 64.57 | 59.28 | 40.34 | 57.74 | 54.09 | ||
| 1 | 31.78 | 28.90 | 31.96 | 35.29 | 33.57 | 32.30 | ||
| 2+ | 11.63 | 6.53 | 8.76 | 24.37 | 8.69 | 13.62 | ||
| Self-reported walking pace, % | <0.001 | <0.001 | ||||||
| Slow | 15.50 | 478. | 8.76 | 11.76 | 3.35 | 6.61 | ||
| Steady or average | 54.26 | 51.86 | 47.94 | 53.78 | 48.69 | 52.14 | ||
| Brisk | 30.23 | 43.36 | 43.30 | 34.45 | 47.71 | 41.25 | ||
| Grip strength in kg, mean (SD) | 24.32 (6.64) | 25.08 (6.29) | 24.62 (5.81) | 0.339 | 38.93 (8.32) | 41.09 (8.33) | 39.87 (8.08) | <0.01 |
| Anxiety and depression, mean (SD) | 5.48 (2.12) | 5.26 (1.94) | 5.24 (1.72) | 0.456 | 5.03 (1.58) | 5.02 (1.55) | 4.99 (1.64) | 0.930 |
| Accelerometer measured PA | ||||||||
| Total acceleration, mean (SD) | 25.31 (7.79) | 27.50 (7.32) | 26.57 (7.11) | <0.01 | 22.87 (6.83) | 26.91 (8.74) | 24.82 (7.47) | <0.001 |
| MVPA (min/day), mean (SD) | 91.05 (44.16) | 106.74 (43.37) | 101.98(45.02) | <0.001 | 77.95 (36.04) | 101.49 (45.72) | 91.41 (44.11) | <0.001 |
| Moderate PA (min/day), mean (SD) | 88.72 (41.90) | 103.53 (40.99) | 99.65 (43.50) | <0.001 | 75.78 (34.49) | 97.40 (43.06) | 88.27 (42.11) | <0.001 |
| Vigorous PA (min/day), mean (SD) | 2.33 (4.37) | 3.20 (4.86) | 2.33 (3.20) | <0.05 | 2.18 (4.04) | 4.09 (5.89) | 3.14 (4.28) | <0.001 |
| Female (n = 1181) | Male (n = 1481) | |||
|---|---|---|---|---|
| Unadjusted Coefficient b (95% CI) | Adjusted Coefficient a b (95% CI) | Unadjusted Coefficient b (95% CI) | Adjusted Coefficient a b (95% CI) | |
| Type of cancer | ||||
| Lung cancer | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Female breast cancer | 15.68 (7.58, 23.78) *** | 5.62 (–2.26, 13.50) | − | − |
| Colorectal cancer | 10.93 (1.18, 20.67) * | 6.37 (−2.90, 15.64) | 13.46 (3.72, 23.19) ** | 6.33 (−2.97, 15.64) |
| Prostate cancer | − | − | 23.54 (15.07, 32.01) *** | 15.32 (7.11, 23.53) *** |
| Age at accelerometer study | −1.61 (−1.94, −1.27) *** | −2.41 (−2.78, −2.04) | ||
| White race (reference: non-white) | −0.49 (−15.38, 14.39) | −7.72 (−23.36, 7.91) | ||
| Townsend Index of deprivation | −0.31 (−1.15, 0.53) | −0.32 (−1.14, 0.49) | ||
| BMI | ||||
| Underweight | 8.65 (−15.84, 33.15) | 64.43 (−17.77, 146.613) | ||
| Normal | 0.00 (reference) | 0.00 (reference) | ||
| Overweight | −9.44 (−14.75, −4.14) *** | −11.35 (−16.49, −6.20) *** | ||
| Obese | −21.74 (−28.27, −15.21) *** | −24.20 (−30.54, −17.85) *** | ||
| Smoking status | ||||
| Never | 0.00 (reference) | 0.00 (reference) | ||
| Previous | 1.08 (−3.97, 6.13) | 5.68 (1.04, 10.32) * | ||
| Current | −14.26 (−23.61, −4.90) ** | −11.73 (−20.18, −3.28) ** | ||
| Alcohol drinking frequency | ||||
| ≤1–3 times/month | 0.00 (reference) | 0.00 (reference) | ||
| 1–4 times/week | 9.43 (3.94, 14.92) ** | 6.60 (0.55, 12.65) * | ||
| Daily or almost daily | 12.66 (5.94, 19.38) *** | 7.63 (1.11, 14.16) * | ||
| Lung Cancer (n = 248) | Breast Cancer (n = 858; Only Females) | |||
| Unadjusted Coefficient b (95% CI) | Adjusted Coefficient b (95% CI) | Unadjusted Coefficient b (95% CI) | Adjusted Coefficient b (95% CI) | |
| Male (reference: female) | −13.10 (−23.23, −2.97) * | 1.36 (−12.66,15.39) | − | − |
| Age at accelerometer study | −2.29 (−3.10, −1.48) *** | −2.35 (−3.22, −1.48) *** | −1.57 (−1.94, −1.19) *** | −1.50 (−1.90, −1.11) *** |
| White (reference: non−white) | −8.80 (−42.16, 24.55) | −3.04 (−32.88,26.80) | −5.86 (−24.25, 12.53) | −3.31 (−20.64, 14.01) |
| Townsend Index of Deprivation | −2.14 (−3.76, −0.51) * | −1.23 (−2.80, 0.36) | 0.28 (−0.79, 1.34) | 0.65 (−0.36, 1.65) |
| BMI | ||||
| Underweight | −54.23 (−134.20, 25.73) | −47.59 (−120.05, 24.87) | 27.86 (−1.76, 57.48) | 19.05 (−9.05, 47.15) |
| Normal | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Overweight | −8.96 (−21.21, 3.30) | −3.86 (−15.02, 7.30) | −14.31 (−20.60, −8.02) *** | −8.48 (−14.60, −2.35) ** |
| Obese | −19.79 (−32.76, −6.82) ** | −8.36 (−21.19, 4.47) | −25.54 (−33.51, −17.56) *** | −14.99 (−22.94, −7.04) *** |
| Smoking status | ||||
| Never | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Previous | −18.09 (−30.57, −5.62) ** | −7.06 (−18.83, 4.70) | 1.09 (−5.07, 7.26) | 3.71 (−2.08, 9.50) |
| Current | −34.96 (−49.55, −20.37) *** | −26.43 (−40.30, −12.56) *** | −8.62 (−20.82, 3.58) | −8.88 (−20.24, 2.47) |
| Alcohol drinking frequency | ||||
| ≤1–3 times/month | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| 1–4 times/week | 16.51 (4.70, 28.33) ** | 1.90 (−9.12, 12.92) | 11.43 (4.70, 18.17) ** | 7.71 (1.37, 14.06) * |
| Daily or almost daily | 17.45 (4.23, 30.67) * | 8.97 (−3.16, 21.11) | 11.78 (3.58, 19.99) ** | 9.55 (1.71, 17.39) * |
| Overall health rating | ||||
| Excellent | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Good | −3.87 (−20.54, 12.81) | 0.93 (−14.05, 15.91) | −5.21 (−12.58, 2.15) | −0.55 (−7.71, 6.61) |
| Fair | −21.98 (−40.20, −3.75) * | −1.36 (−19.16, 16.43) | −18.80 (−29.06, 8.54) *** | −6.91 (−17.48, 3.65) |
| Poor | −36.90 (−61.28, −12.52) ** | −15.35 (−43.42, 12.71) | −33.90 (−53.36, −14.43) ** | −20.77 (−41.01, −0.53) * |
| No. of comorbidities | −12.87 (−18.11, −7.64) *** | −3.10 (−9.02, 2.81) | −8.36 (−12.84, −3.88) *** | −2.40 (−6.80, 2.02) |
| Self-reported walking pace | ||||
| Slow | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Steady or average | 25.64 (1−.99, 40.29) ** | 11.36 (−3.54, 26.26) | 26.85 (13.41, 40.28) *** | 16.36 (2.53, 30.18) * |
| Brisk | 43.24 (27.62, 58.86) *** | 23.06 (6.52, 39.60) *** | 44.12 (30.57, 57.67) *** | 29.08 (14.84, 43.33) *** |
| Grip strength (kg) | −0.08 (−0.57, 0.41) | −0.60 (−1.28, 0.08) | 0.50 (0.04, 0.96) * | −3.36 (−0.82, 0.10) |
| Anxiety and depression | −4.08 (−6.75, −1.40) ** | −1.54 (−4.38, 1.30) | −1.30 (−2.80, 0.20) | −0.67 (−2.18, 0.85) |
| Adjusted R2 | − | 28.56% | − | 16.28% |
| VIF | − | 1.12−3.20 | − | 1.03−7.05 |
| Colorectal Cancer (n = 451) | Prostate Cancer (n = 1105; Only Males) | |||
| Unadjusted Coefficient b (95% CI) | Adjusted Coefficient b (95% CI) | Unadjusted Coefficient b (95% CI) | Adjusted Coefficient b (95% CI) | |
| Male (reference: female) | −10.57 (−18.89, −2.25) * | −3.02 (−14.92, 8.89) | − | − |
| Age at accelerometer study | −2.16 (−2.76, −1.56) *** | −2.02 (−2.66, −1.38) *** | −2.31 (−2.76, −1.85) *** | −2.37 (−2.84, −1.90) *** |
| White (reference: non-white) | −10.49 (−40.13, 19.14) | −18.66 (−47.62, 10.30) | −9.91 (−28.81, 8.99) | −8.08 (−25.98, 9.82) |
| Townsend Index of Deprivation | −0.72 (−2.15, 0.72) | −0.52 (−1.87, 0.83) | 0.27 (−0.77, 1.31) | 0.18 (−0.81, 1.17) |
| BMI | ||||
| Underweight | −11.89 (−73.42, 49.63) | −25.84 (−85.79, 34.12) | 48.89 (−39.50, 137.29) | 62.0 (−21.24, 145.29) |
| Normal | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Overweight | −11.19 (−20.67, −1.70) * | −5.85 (−15.07, 3.37) | −11.52 (−17.78, −5.27) *** | −7.95 (−13.97, −1.92) * |
| Obese | −25.21 (−36.41, −14.01) *** | −17.04 (−28.26, −5.82) ** | −24.85 (−32.77, −16.94) *** | −17.97 (−25.92, −10.03) *** |
| Smoking status | ||||
| Never | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Previous | 3.88 (−4.70, 12.46) | 10.80 (2.49, 19.12) * | −1.56 (−7.13, 4.00) | 7.23 (1.87, 12.59) ** |
| Current | −8.49 (−25.43, 8.44) | −3.02 (−18.96, 12.91) | −7.36 (−19.15, 4.43) | −5.90 (−17.06, 5.25) |
| Alcohol drinking frequency | ||||
| ≤1–3 times/month | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| 1–4 times/week | 10.11 (−0.39, 20.61) | 5.14 (−5.06, 15.34) | 5.79 (−1.87, 13.45) | 4.25 (−2.94, 11.45) |
| Daily or almost daily | 7.25 (−4.07, 18.58) | 6.07 (−5.19, 17.34) | 4.55 (−3.76, 12.83) | 2.44 (−5.45, 10.32) |
| Overall health rating | ||||
| Excellent | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Good | −15.96 (−26.83, −5.08) ** | −10.21 (−20.75, 0.32) | −8.23 (−14.89, −1.57) * | −4.22 (−10.72, 2.28) |
| Fair | −23.17 (−36.98, −9.37) ** | −11.27 (−25.66, 3.12) | −23.22 (−31.88, −14.55) *** | −12.53 (−21.70, −3.35) ** |
| Poor | −42.00 (−69.84, −14.17) ** | −24.24 (−53.20, 4.71) | −49.46 (−73.73, −25.18) *** | −41.36 (−66.04, −16.67) ** |
| No. of comorbidities | −9.69 (−15.12, −4.27) *** | −2.39 (−7.82, 3.05) | −11.34 (−15.00, −7.68) *** | −4.22 (−8.02, −0.42) * |
| Self-reported walking pace | ||||
| Slow | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) | 0.00 (reference) |
| Steady or average | 22.72 (7.14, 38.31) ** | 20.41 (3.93, 36.89) * | 30.15 (15.16, 45.13) *** | 14.57 (−0.09, 29.22) |
| Brisk | 41.78 (26.00, 57.56) *** | 31.01 (13.82, 48.20) *** | 41.84 (26.85, 56.83) *** | 21.34 (6.37, 36.31) ** |
| Grip strength (kg) | −0.05 (−0.45, 0.34) | −0.27 (−0.85, 0.30) | 0.18 (−0.15, 0.50) | −0.27 (−0.69, −0.05) * |
| Anxiety and depression | 0.29 (−2.26, 2.84) | 0.09 (−2.43, 2.60) | −0.28 (−1.93, 1.36) | 0.56 (−1.05, 2.17) |
| Adjusted R2 | − | 18.44% | − | 14.98% |
| VIF | − | 1.09−5.15 | − | 1.01−9.03 |
| Unadjusted Hazard Ratio (95% CI) (n = 2661, No. of Events = 426) | Adjusted Hazard Ratio a (95% CI) (n = 2661, No. of Events = 426) | |
|---|---|---|
| Time in MVPA (h/day) | ||
| <1 h (reference) | 1.0 (Reference) | 1.0 (Reference) |
| 1–1.5 h | 0.63 (0.50, 0.81) *** | 0.90 (0.69, 1.16) |
| 1.5–2 h | 0.49 (0.38, 0.64) *** | 0.68 (0.52, 0.91) ** |
| ≥2 h | 0.32 (0.24, 0.43) *** | 0.57 (0.42, 0.78) *** |
| Cancer type | ||
| Lung cancer (reference) | 1.0 (Reference) | |
| Female breast cancer | 0.08 (0.05, 0.11) *** | |
| Colorectal cancer | 0.31 (0.24, 0.41) *** | |
| Prostate cancer | 0.08 (0.06, 0.10) *** | |
| Male (reference: female) | 1.25 (0.97, 1.62) | |
| Age at cancer diagnosis | ||
| <65 years | 1.0 (Reference) | |
| 65–70 years | 0.94 (0.68, 1.28) | |
| 70–75 years | 1.25 (0.94, 1.66) | |
| ≥75 years | 1.49 (1.08, 2.04) * | |
| White race (reference: non-white) | 1.58 (0.68, 3.65) | |
| Townsend Index of deprivation | 1.00 (0.96, 1.03) | |
| BMI | ||
| Underweight | 3.24 (0.98, 10.66) | |
| Normal | 1.0 (Reference) | |
| Overweight | 1.04 (0.82, 1.32) | |
| Obese | 1.04 (0.79, 1.39) | |
| Smoking status | ||
| Never | 1.0 (Reference) | |
| Previous | 1.18 (0.95, 1.47) | |
| Current | 1.47 (1.07, 2.02) * | |
| Alcohol drinking frequency | ||
| ≤1–3 times/month | 1.0 (Reference) | |
| 1–4 times/week | 1.40 (1.08, 1.82) * | |
| Daily or almost daily | 1.25 (0.94, 1.67) | |
| Diabetes | 1.42 (0.97, 2.08) | |
| Heart attack | 0.77 (0.45, 1.32) | |
| Angina | 0.72 (0.42, 1.24) | |
| Stroke | 1.54 (0.87, 2.74) | |
| Hypertension | 0.94 (0.75, 1.17) | |
| COPD | 1.37 (0.85, 2.20) | |
| Asthma | 0.86 (0.63, 1.18) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.; Veliz, P.T.; Smith, E.M.L.; Chen, W.; Reddy, R.M.; Larson, J.L. Comparison of Pre-Diagnosis Physical Activity and Its Correlates between Lung and Other Cancer Patients: Accelerometer Data from the UK Biobank Prospective Cohort. Int. J. Environ. Res. Public Health 2023, 20, 1001. https://doi.org/10.3390/ijerph20021001
Zhou W, Veliz PT, Smith EML, Chen W, Reddy RM, Larson JL. Comparison of Pre-Diagnosis Physical Activity and Its Correlates between Lung and Other Cancer Patients: Accelerometer Data from the UK Biobank Prospective Cohort. International Journal of Environmental Research and Public Health. 2023; 20(2):1001. https://doi.org/10.3390/ijerph20021001
Chicago/Turabian StyleZhou, Weijiao, Philip T. Veliz, Ellen M. Lavoie Smith, Weiyun Chen, Rishindra M. Reddy, and Janet L. Larson. 2023. "Comparison of Pre-Diagnosis Physical Activity and Its Correlates between Lung and Other Cancer Patients: Accelerometer Data from the UK Biobank Prospective Cohort" International Journal of Environmental Research and Public Health 20, no. 2: 1001. https://doi.org/10.3390/ijerph20021001
APA StyleZhou, W., Veliz, P. T., Smith, E. M. L., Chen, W., Reddy, R. M., & Larson, J. L. (2023). Comparison of Pre-Diagnosis Physical Activity and Its Correlates between Lung and Other Cancer Patients: Accelerometer Data from the UK Biobank Prospective Cohort. International Journal of Environmental Research and Public Health, 20(2), 1001. https://doi.org/10.3390/ijerph20021001