
Perioperative Nutritional Management in Enhanced Recovery after Bariatric Surgery

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
- A minimum of 6 h fasting for solids and 2 h for clear fluids before anaesthesia induction is advised under standard circumstances;
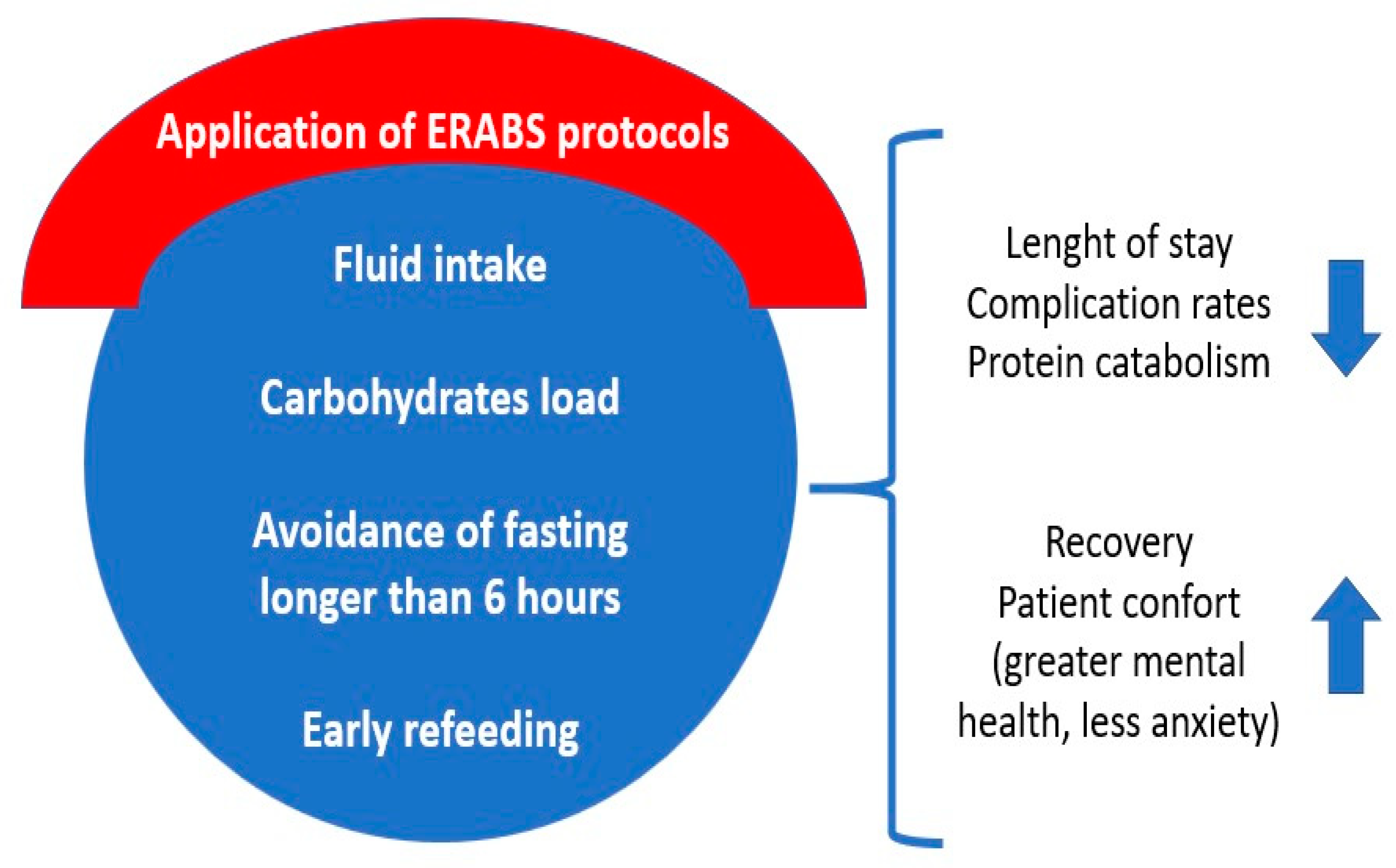
- For postoperative nutrition, clear liquid intake can start two hours after surgery, followed by more nourishing fluids. Dietary consultations will offer texture-specific guidance based on the type of surgery. Patients should eat slowly, chew thoroughly, and avoid beverages during meals. Carbonated drinks and alcohol are not allowed (Figure 1).
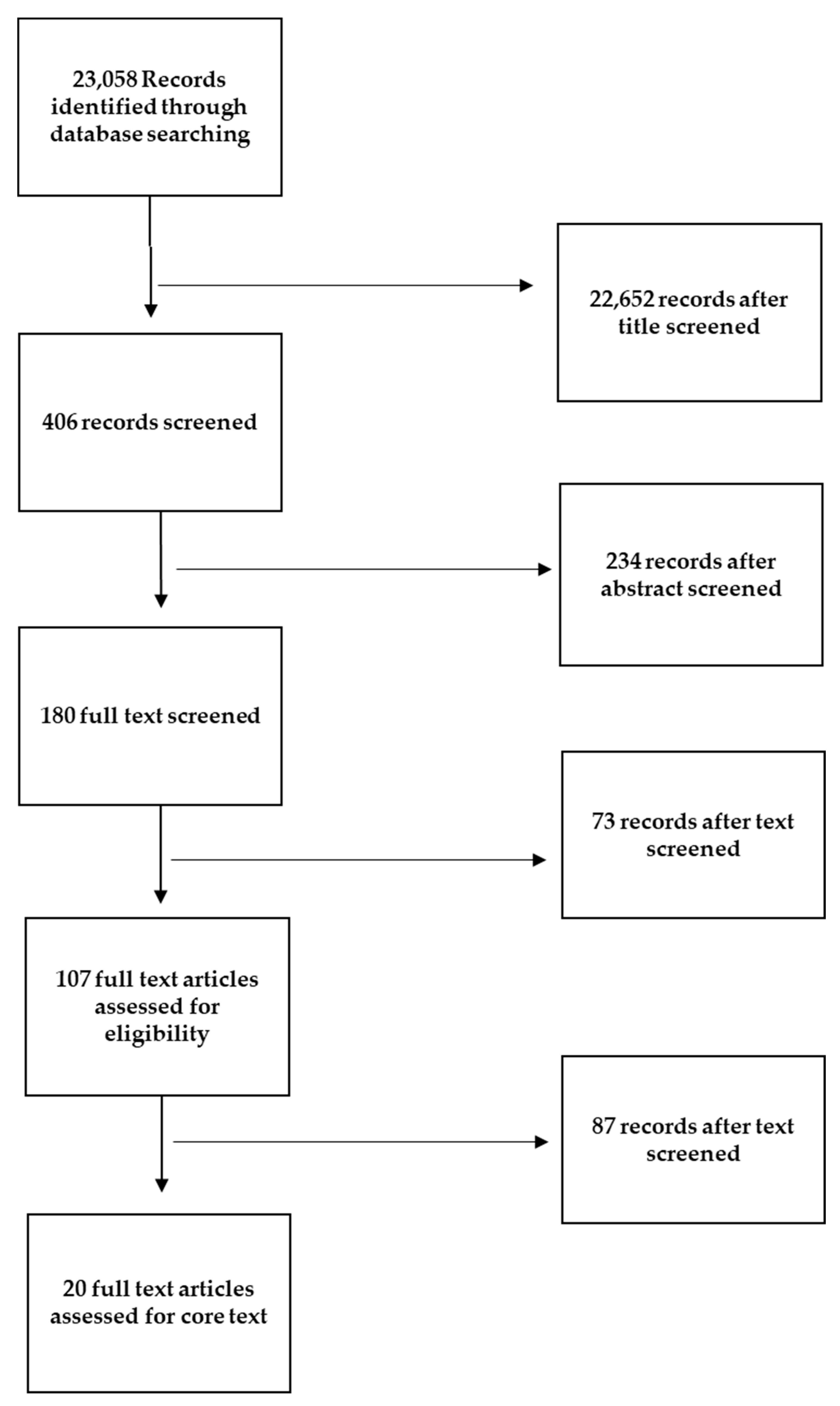
2. Methods
3. Preoperative Fasting (PF)
4. Preoperative Carbohydrates Load (PreCL)
5. Postoperative Fasting/Early Oral Feeding (POF/EOF)
6. Discussion
Gaps in the Research
7. Strengths and Limitations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Apovian, C.M. Obesity: Definition, Comorbidities, Causes, and Burden. Am. J. Manag. Care 2016, 22, s176–s185. [Google Scholar]
- Kelishadi, R. Health Impacts of Obesity. Pak. J. Med. Sci. 2014, 31, 239–242. [Google Scholar] [CrossRef]
- Dhawan, D.; Sharma, S. Abdominal Obesity, Adipokines and Non-Communicable Diseases. J. Steroid Biochem. Mol. Biol. 2020, 203, 105737. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef] [PubMed]
- Pinna, F.; Sardu, C.; Orrù, W.; Velluzzi, F.; Loviselli, A.; Contu, P.; Carpiniello, B. Psychopathology, Psychosocial Factors and Obesity. Riv. Psichiatr. 2016, 51, 30–36. [Google Scholar] [PubMed]
- Carpiniello, B.; Pinna, F.; Velluzzi, F.; Loviselli, A. Mental Disorders in Patients with Metabolic Syndrome. The Key Role of Central Obesity. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2012, 17, e259–e266. [Google Scholar] [CrossRef]
- Tiwari, A.; Balasundaram, P. Public Health Considerations Regarding Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572122/ (accessed on 13 February 2023).
- Kivimäki, M.; Strandberg, T.; Pentti, J.; Nyberg, S.T.; Frank, P.; Jokela, M.; Ervasti, J.; Suominen, S.B.; Vahtera, J.; Sipilä, P.N.; et al. Body-Mass Index and Risk of Obesity-Related Complex Multimorbidity: An Observational Multicohort Study. Lancet Diabetes Endocrinol. 2022, 10, 253–263. [Google Scholar] [CrossRef]
- Mohammed, M.S.; Sendra, S.; Lloret, J.; Bosch, I. Systems and WBANs for Controlling Obesity. J. Healthc. Eng. 2018, 2018, 1564748. [Google Scholar] [CrossRef] [PubMed]
- Durrer Schutz, D.; Busetto, L.; Dicker, D.; Farpour-Lambert, N.; Pryke, R.; Toplak, H.; Widmer, D.; Yumuk, V.; Schutz, Y. European Practical and Patient-Centred Guidelines for Adult Obesity Management in Primary Care. Obes. Facts 2019, 12, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Flore, G.; Preti, A.; Carta, M.G.; Deledda, A.; Fosci, M.; Nardi, A.E.; Loviselli, A.; Velluzzi, F. Weight Maintenance after Dietary Weight Loss: Systematic Review and Meta-Analysis on the Effectiveness of Behavioural Intensive Intervention. Nutrients 2022, 14, 1259. [Google Scholar] [CrossRef]
- Busetto, L.; Bettini, S.; Makaronidis, J.; Roberts, C.A.; Halford, J.C.G.; Batterham, R.L. Mechanisms of Weight Regain. Eur. J. Intern. Med. 2021, 93, 3–7. [Google Scholar] [CrossRef]
- Pisanu, S.; Deledda, A.; Loviselli, A.; Huybrechts, I.; Velluzzi, F. Validity of Accelerometers for the Evaluation of Energy Expenditure in Obese and Overweight Individuals: A Systematic Review. J. Nutr. Metab. 2020, 2020, 2327017. [Google Scholar] [CrossRef] [PubMed]
- Deledda, A.; Pintus, S.; Loviselli, A.; Fosci, M.; Fantola, G.; Velluzzi, F. Nutritional Management in Bariatric Surgery Patients. Int. J. Environ. Res. Public Health 2021, 18, 12049. [Google Scholar] [CrossRef]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; De Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for Metabolic and Bariatric Surgery. Surg. Obes. Relat. Dis. 2022, 18, 1345–1356. [Google Scholar] [CrossRef]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines For The Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored By American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society For Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Endocr. Pract. 2019, 25, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Franchi, A.; Biolcati Rinaldi, R.; Rizzo, G.; D’Adamo, M.; Guglielmi, V.; Bellia, A.; Padua, E.; Caprio, M.; Sbraccia, P. Long-Term Iron and Vitamin B12 Deficiency Are Present after Bariatric Surgery, despite the Widespread Use of Supplements. Int. J. Environ. Res. Public Health 2021, 18, 4541. [Google Scholar] [CrossRef] [PubMed]
- Hanipah, Z.N.; Schauer, P.R. Bariatric Surgery as a Long-Term Treatment for Type 2 Diabetes/Metabolic Syndrome. Annu. Rev. Med. 2020, 71, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Carter, S.; Purkayastha, S.; Hakky, S.; Moorthy, K.; Cousins, J.; Ahmed, A.R. Enhanced Recovery After Bariatric Surgery (ERABS): Clinical Outcomes from a Tertiary Referral Bariatric Centre. Obes. Surg. 2014, 24, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, E.; Dos Reis Falcão, L.F.; O’Kane, M.; Liem, R.; Pournaras, D.J.; Salminen, P.; Urman, R.D.; Wadhwa, A.; Gustafsson, U.O.; Thorell, A. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations: A 2021 Update. World J. Surg. 2022, 46, 729–751. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.H.; Ljungqvist, O.; Von Meyenfeldt, M.; Revhaug, A.; Dejong, C.H.C.; Lassen, K.; Nygren, J.; Hausel, J.; Soop, M.; Andersen, J.; et al. Enhanced Recovery after Surgery: A Consensus Review of Clinical Care for Patients Undergoing Colonic Resection. Clin. Nutr. 2005, 24, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef]
- Kehlet, H. Multimodal Approach to Control Postoperative Pathophysiology and Rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef]
- Aktimur, R. Enhanced Recovery after Surgery in Bariatric and Metabolic Surgery. Ann. Laparosc. Endosc. Surg. 2021, 6, 48. [Google Scholar] [CrossRef]
- Thorell, A.; MacCormick, A.D.; Awad, S.; Reynolds, N.; Roulin, D.; Demartines, N.; Vignaud, M.; Alvarez, A.; Singh, P.M.; Lobo, D.N. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2065–2083. [Google Scholar] [CrossRef]
- Marinari, G.; Foletto, M.; Nagliati, C.; Navarra, G.; Borrelli, V.; Bruni, V.; Fantola, G.; Moroni, R.; Tritapepe, L.; Monzani, R.; et al. Enhanced Recovery after Bariatric Surgery: An Italian Consensus Statement. Surg. Endosc. 2022, 36, 7171–7186. [Google Scholar] [CrossRef]
- Brethauer, S.A.; Grieco, A.; Fraker, T.; Evans-Labok, K.; Smith, A.; McEvoy, M.D.; Saber, A.A.; Morton, J.M.; Petrick, A. Employing Enhanced Recovery Goals in Bariatric Surgery (ENERGY): A National Quality Improvement Project Using the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program. Surg. Obes. Relat. Dis. 2019, 15, 1977–1989. [Google Scholar] [CrossRef]
- ISS. La Terapia Chirurgica dell’Obesità e Delle Complicanze Associate. Available online: https://www.iss.it/web/guest/-/terapia-chirurgica-obesita-e-complicanze (accessed on 20 December 2022).
- Bevilacqua, L.A.; Obeid, N.R.; Spaniolas, K.; Bates, A.; Docimo, S.; Pryor, A. Early Postoperative Diet after Bariatric Surgery: Impact on Length of Stay and 30-Day Events. Surg. Endosc. 2019, 33, 2475–2478. [Google Scholar] [CrossRef]
- Tong, E.; Chen, Y.; Ren, Y.; Zhou, Y.; Di, C.; Zhou, Y.; Shao, S.; Qiu, S.; Hong, Y.; Yang, L.; et al. Effects of Preoperative Carbohydrate Loading on Recovery after Elective Surgery: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials. Front. Nutr. 2022, 9, 951676. [Google Scholar] [CrossRef]
- Ban, K.; Berian, J.; Ko, C. Does Implementation of Enhanced Recovery after Surgery (ERAS) Protocols in Colorectal Surgery Improve Patient Outcomes? Clin. Colon Rectal Surg. 2019, 32, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Heber, D.; Greenway, F.L.; Kaplan, L.M.; Livingston, E.; Salvador, J.; Still, C. Endocrine and Nutritional Management of the Post-Bariatric Surgery Patient: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2010, 95, 4823–4843. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN Practical Guideline: Clinical Nutrition in Surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Joshi, G.P.; Abdelmalak, B.B.; Weigel, W.A.; Harbell, M.W.; Kuo, C.I.; Soriano, S.G.; Stricker, P.A.; Tipton, T.; Grant, M.D.; Marbella, A.M.; et al. 2023 American Society of Anesthesiologists Practice Guidelines for Preoperative Fasting: Carbohydrate-Containing Clear Liquids with or without Protein, Chewing Gum, and Pediatric Fasting Duration—A Modular Update of the 2017 American Society of Anesthesiologists Practice Guidelines for Preoperative Fasting. Anesthesiology 2023, 138, 132–151. [Google Scholar] [CrossRef] [PubMed]
- Kratzing, C. Pre-Operative Nutrition and Carbohydrate Loading. Proc. Nutr. Soc. 2011, 70, 311–315. [Google Scholar] [CrossRef]
- Pimenta, G.P.; De Aguilar-Nascimento, J.E. Prolonged Preoperative Fasting in Elective Surgical Patients: Why Should We Reduce It? Nutr. Clin. Pract. 2014, 29, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, J.T. Preoperative Fasting: Will the Evidence Ever Be Put into Practice? AJN Am. J. Nurs. 2011, 111, 38–43. [Google Scholar] [CrossRef]
- Merchant, R.N.; Chima, N.; Ljungqvist, O.; Kok, J.N.J. Preoperative Fasting Practices Across Three Anesthesia Societies: Survey of Practitioners. JMIR Perioper. Med. 2020, 3, e15905. [Google Scholar] [CrossRef]
- Cuomo, R.; Giardino, F.R.; Nisi, G.; Brandi, C.; Zerini, I.; Voglino, C.; Gaggelli, I.; Grimaldi, L. Aspiration Pneumonia: A Shadow in Post-Bariatric Patient: Correlation between Aspiration and Minigrastric Bypass. Obes. Surg. 2019, 29, 3937–3940. [Google Scholar] [CrossRef]
- Andersson, H.; Zarén, B.; Frykholm, P. Low Incidence of Pulmonary Aspiration in Children Allowed Intake of Clear Fluids until Called to the Operating Suite. Paediatr. Anaesth. 2015, 25, 770–777. [Google Scholar] [CrossRef]
- Beach, M.L.; Cohen, D.M.; Gallagher, S.M.; Cravero, J.P. Major Adverse Events and Relationship to Nil per Os Status in Pediatric Sedation/Anesthesia Outside the Operating Room. Anesthesiology 2016, 124, 80–88. [Google Scholar] [CrossRef]
- Xiao, M.Z.X.; Englesakis, M.; Perlas, A. Gastric Content and Perioperative Pulmonary Aspiration in Patients with Diabetes Mellitus: A Scoping Review. Br. J. Anaesth. 2021, 127, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Zhu, F.; An, Y.; Qin, L.; Lv, J.; Zhao, X.; Shen, J. Prolonged Preoperative Fasting and Prognosis in Critically Ill Gastrointestinal Surgery Patients. Asia Pac. J. Clin. Nutr. 2020, 29, 41–47. [Google Scholar] [CrossRef]
- Lirosi, M.C.; Tirelli, F.; Biondi, A.; Mele, M.C.; Larotonda, C.; Lorenzon, L.; D’Ugo, D.; Gasbarrini, A.; Persiani, R. Enhanced Recovery Program for Colorectal Surgery: A Focus on Elderly Patients Over 75 Years Old. J. Gastrointest. Surg. 2019, 23, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Black, M.K.; Lupa, M.C.; Lemley, L.W.; Dreesen, E.B.; Deaton, A.M.; Iii, R.M.W. Things We Do for No ReasonTM: NPO after Midnight. J. Hosp. Med. 2021, 16, 368–370. [Google Scholar] [CrossRef]
- Sarin, A.; Chen, L.; Wick, E.C. Enhanced Recovery after Surgery-Preoperative Fasting and Glucose Loading-A Review. J. Surg. Oncol. 2017, 116, 578–582. [Google Scholar] [CrossRef]
- Lambert, E.; Carey, S. Practice Guideline Recommendations on Perioperative Fasting: A Systematic Review. JPEN J. Parenter. Enter. Nutr. 2016, 40, 1158–1165. [Google Scholar] [CrossRef]
- Noba, L.; Wakefield, A. Are Carbohydrate Drinks More Effective than Preoperative Fasting: A Systematic Review of Randomised Controlled Trials. J. Clin. Nurs. 2019, 28, 3096–3116. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, S.; Wu, G. ESPEN Practical Guideline: Clinical Nutrition in Surgery. Clin. Nutr. 2021, 40, 5071. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.; Wendel, K.; Polits, S.; Gislason, H.; Hedenbro, J.L. Preoperative Nutrition and Postoperative Discomfort in an ERAS Setting: A Randomized Study in Gastric Bypass Surgery. Obes. Surg. 2016, 26, 743–748. [Google Scholar] [CrossRef]
- Desborough, J.P. The Stress Response to Trauma and Surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef]
- Nygren, J. The Metabolic Effects of Fasting and Surgery. Best Pract. Res. Clin. Anaesthesiol. 2006, 20, 429–438. [Google Scholar] [CrossRef]
- Smith, M.D.; McCall, J.; Plank, L.; Herbison, G.P.; Soop, M.; Nygren, J. Preoperative Carbohydrate Treatment for Enhancing Recovery after Elective Surgery. Cochrane Database Syst. Rev. 2014, 8, 9161. [Google Scholar] [CrossRef]
- Suh, S.; Hetzel, E.; Alter-Troilo, K.; Lak, K.; Gould, J.C.; Kindel, T.L.; Higgins, R.M. The Influence of Preoperative Carbohydrate Loading on Postoperative Outcomes in Bariatric Surgery Patients: A Randomized, Controlled Trial. Surg. Obes. Relat. Dis. 2021, 17, 1480–1488. [Google Scholar] [CrossRef]
- Awad, S.; Varadhan, K.K.; Ljungqvist, O.; Lobo, D.N. A Meta-Analysis of Randomised Controlled Trials on Preoperative Oral Carbohydrate Treatment in Elective Surgery. Clin. Nutr. 2013, 32, 34–44. [Google Scholar] [CrossRef]
- Wendler, E.; Nassif, P.A.N.; Malafaia, O.; Brites Neto, J.L.; Ribeiro, J.G.A.; Proença, L.B.D.; Mattos, M.E.; Ariede, B.L. Shorten Preoperative Fasting and Introducing Early Eating Assistance in Recovery after Gastrojejunal Bypass? ABCD Arq. Bras. Cir. Dig. 2021, 34, e1606. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.D.S.; Grigoletti, S.S.; Marcadenti, A. Fasting Abbreviation among Patients Submitted to Oncologic Surgery: Systematic Review. ABCD Arq. Bras. Cir. Dig. 2015, 28, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Jang, A.; Jeong, O. Intolerability to Postoperative Early Oral Nutrition in Older Patients (≥70 Years) Undergoing Gastrectomy for Gastric Cancer: A Case-Control Study. PLoS ONE 2021, 16, e0251844. [Google Scholar] [CrossRef]
- Ricci, C.; Ingaldi, C.; Alberici, L.; Serbassi, F.; Pagano, N.; De Raffele, E.; Minni, F.; Pironi, L.; Sasdelli, A.S.; Casadei, R. Preoperative Carbohydrate Loading before Elective Abdominal Surgery: A Systematic Review and Network Meta-Analysis of Phase II/III Randomized Controlled Trials. Clin. Nutr. 2022, 41, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro de Amorim, A.C. Estado Nutricional y Tiempo de Ayuno Perioperatorio Versus. Nutr. Hosp. 2015, 32, 878–887. [Google Scholar] [CrossRef]
- Silva de Assis, M.C. ¿Duracion del Ayuno Postoperatorio se Asocia con la Infeccion y La. Nutr. Hosp. 2014, 30, 919–926. [Google Scholar] [CrossRef]
- Hur, H.; Kim, S.G.; Shim, J.H.; Song, K.Y.; Kim, W.; Park, C.H.; Jeon, H.M. Effect of Early Oral Feeding after Gastric Cancer Surgery: A Result of Randomized Clinical Trial. Surgery 2011, 149, 561–568. [Google Scholar] [CrossRef]
- Major, P.; Wysocki, M.; Torbicz, G.; Gajewska, N.; Dudek, A.; Małczak, P.; Pędziwiatr, M.; Pisarska, M.; Radkowiak, D.; Budzyński, A. Risk Factors for Prolonged Length of Hospital Stay and Readmissions After Laparoscopic Sleeve Gastrectomy and Laparoscopic Roux-En-Y Gastric Bypass. Obes. Surg. 2018, 28, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, N.; Oki, E.; Tanizawa, Y.; Suzuki, Y.; Aikou, S.; Kunisaki, C.; Tsuchiya, T.; Fukushima, R.; Doki, Y.; Natsugoe, S.; et al. Effect of Early Oral Feeding on Length of Hospital Stay Following Gastrectomy for Gastric Cancer: A Japanese Multicenter, Randomized Controlled Trial. Surg. Today 2018, 48, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.P.; Menezes, T.M.; Toledo, D.O.; De-Oliveira, A.T.T.; Longatto-Filho, A.; Nascimento, J.E.D.A. Early Oral Feeding Post-Upper Gastrointestinal Tract Resection and Primary Anastomosis in Oncology. ABCD Arq. Bras. Cir. Dig. 2018, 31, e1359. [Google Scholar] [CrossRef] [PubMed]
- Sierzega, M.; Choruz, R.; Pietruszka, S.; Kulig, P.; Kolodziejczyk, P.; Kulig, J. Feasibility and Outcomes of Early Oral Feeding after Total Gastrectomy for Cancer. J. Gastrointest. Surg. 2015, 19, 473–479. [Google Scholar] [CrossRef]
- Małczak, P.; Wysocki, M.; Twardowska, H.; Dudek, A.; Tabiś, J.; Major, P.; Pisarska, M.; Pędziwiatr, M. Impact of Adherence to the ERAS® Protocol on Short-Term Outcomes after Bariatric Surgery. Obes. Surg. 2020, 30, 1498–1505. [Google Scholar] [CrossRef]
- Goretti, G.; Marinari, G.M.; Vanni, E.; Ferrari, C. Value-Based Healthcare and Enhanced Recovery after Surgery Implementation in a High-Volume Bariatric Center in Italy. Obes. Surg. 2020, 30, 2519–2527. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery after Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef]
- Virgens, I.P.A.D.; Carvalho, A.L.M.D.; Nagashima, Y.G.; Silva, F.M.; Fayh, A.P.T. Is Perioperative Fasting Associated with Complications, Length of Hospital Stay and Mortality among Gastric and Colorectal Cancer Patients? A Cohort Study. Sao Paulo Med. J. 2020, 138, 407–413. [Google Scholar] [CrossRef]
- Tsang, E.; Lambert, E.; Carey, S. Fasting Leads to Fasting: Examining the Relationships between Perioperative Fasting Times and Fasting for Symptoms in Patients Undergoing Elective Abdominal Surgery. Asia Pac. J. Clin. Nutr. 2018, 27, 968–974. [Google Scholar] [CrossRef]
- Rossoni, C.; Oliveira Magro, D.; Santos, Z.C.; Cambi, M.P.C.; Patias, L.; Bragança, R.; Pellizzaro, D.; Parmar, C.; Ribeiro, R. Enhanced Recovery After Surgery (ERAS) Protocol in Bariatric and Metabolic Surgery (BMS)—Analysis of Practices in Nutritional Aspects from Five Continents. Obes. Surg. 2020, 30, 4510–4518. [Google Scholar] [CrossRef] [PubMed]
- Van Noort, H.H.J.; Eskes, A.M.; Vermeulen, H.; Besselink, M.G.; Moeling, M.; Ubbink, D.T.; Huisman–de Waal, G.; Witteman, B.J.M. Fasting Habits over a 10-Year Period: An Observational Study on Adherence to Preoperative Fasting and Postoperative Restoration of Oral Intake in 2 Dutch Hospitals. Surgery 2021, 170, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Smith, I.; Kranke, P.; Murat, I.; Smith, A.; O’Sullivan, G.; Sreide, E.; Spies, C.; in’T Veld, B. Perioperative Fasting in Adults and Children: Guidelines from the European Society of Anaesthesiology. Eur. J. Anaesthesiol. 2011, 28, 556–569. [Google Scholar] [CrossRef]
- De-Marchi, J.J.; De-Souza, M.M.; Salomão, A.B.; Nascimento, J.E.D.A.; Selleti, A.A.; de-Albuquerque, E.; Mendes, K.B.V. Cuidados Perioperatórios Em Cirurgia Bariátrica No Contexto Do Projeto ACERTO: Realidade e o Imaginário de Cirurgiões em um Hospital de Cuiabá. Rev. Col. Bras. Cir. 2017, 44, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Rattray, M.; Marshall, A.P.; Desbrow, B.; Roberts, S. A Qualitative Exploration of Patients’ Experiences with and Perceptions of Recommencing Feeding after Colorectal Surgery. J. Hum. Nutr. Diet. 2019, 32, 63–71. [Google Scholar] [CrossRef]
- Sun, Z.; Sun, X.; Huo, Y.; Mi, M.; Peng, G.; Zhang, C.; Jiang, Y.; Zhou, Y.; Zhao, X.; Li, T.; et al. Abbreviated Perioperative Fasting Management for Elective Fresh Fracture Surgery: Guideline Adherence Analysis. BMC Musculoskelet. Disord. 2022, 23, 688. [Google Scholar] [CrossRef]
- Dang, J.T.; Szeto, V.G.; Elnahas, A.; Ellsmere, J.; Okrainec, A.; Neville, A.; Malik, S.; Yorke, E.; Hong, D.; Biertho, L.; et al. Canadian Consensus Statement: Enhanced Recovery after Surgery in Bariatric Surgery. Surg. Endosc. 2020, 34, 1366–1375. [Google Scholar] [CrossRef] [PubMed]
- Alazawi, W.; Pirmadjid, N.; Lahiri, R.; Bhattacharya, S. Inflammatory and Immune Responses to Surgery and Their Clinical Impact. Ann. Surg. 2016, 264, 73–80. [Google Scholar] [CrossRef]
- Cata, J.P.; Velasquez, J.F.; Ramirez, M.F.; Vauthey, J.-N.; Gottumukkala, V.; Conrad, C.; Kim, B.J.; Aloia, T. Inflammation and Pro-Resolution Inflammation after Hepatobiliary Surgery. World J. Surg. Oncol. 2017, 15, 152. [Google Scholar] [CrossRef]
- Schulte, F.; Asbeutah, A.A.; Benotti, P.N.; Wood, G.C.; Still, C.; Bistrian, B.R.; Hardt, M.; Welty, F.K. The Relationship between Specialized Pro-Resolving Lipid Mediators, Morbid Obesity and Weight Loss after Bariatric Surgery. Sci. Rep. 2020, 10, 20128. [Google Scholar] [CrossRef] [PubMed]
- López-Vicario, C.; Titos, E.; Walker, M.E.; Alcaraz-Quiles, J.; Casulleras, M.; Durán-Güell, M.; Flores-Costa, R.; Pérez-Romero, N.; Forné, M.; Dalli, J.; et al. Leukocytes from Obese Individuals Exhibit an Impaired SPM Signature. FASEB J. 2019, 33, 7072–7083. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Wang, C.-F.; Serhan, C.N.; Strichartz, G. Enduring Prevention and Transient Reduction of Postoperative Pain by Intrathecal Resolvin D1. Pain 2011, 152, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Fattori, V.; Zaninelli, T.H.; Rasquel-Oliveira, F.S.; Casagrande, R.; Verri, W.A. Specialized Pro-Resolving Lipid Mediators: A New Class of Non-Immunosuppressive and Non-Opioid Analgesic Drugs. Pharmacol. Res. 2020, 151, 104549. [Google Scholar] [CrossRef]
- Chiang, N.; Fredman, G.; Bäckhed, F.; Oh, S.F.; Vickery, T.; Schmidt, B.A.; Serhan, C.N. Infection Regulates Pro-Resolving Mediators that Lower Antibiotic Requirements. Nature 2012, 484, 524–528. [Google Scholar] [CrossRef]
- Martinou, E.; Stefanova, I.; Iosif, E.; Angelidi, A.M. Neurohormonal Changes in the Gut–Brain Axis and Underlying Neuroendocrine Mechanisms Following Bariatric Surgery. Int. J. Mol. Sci. 2022, 23, 3339. [Google Scholar] [CrossRef] [PubMed]
- Palmas, V.; Pisanu, S.; Madau, V.; Casula, E.; Deledda, A.; Cusano, R.; Uva, P.; Loviselli, A.; Velluzzi, F.; Manzin, A. Gut Microbiota Markers and Dietary Habits Associated with Extreme Longevity in Healthy Sardinian Centenarians. Nutrients 2022, 14, 2436. [Google Scholar] [CrossRef]
- Deledda, A.; Palmas, V.; Heidrich, V.; Fosci, M.; Lombardo, M.; Cambarau, G.; Lai, A.; Melis, M.; Loi, E.; Loviselli, A.; et al. Dynamics of Gut Microbiota and Clinical Variables after Ketogenic and Mediterranean Diets in Drug-Naïve Patients with Type 2 Diabetes Mellitus and Obesity. Metabolites 2022, 12, 1092. [Google Scholar] [CrossRef]
- Hajjar, R.; Gonzalez, E.; Fragoso, G.; Oliero, M.; Alaoui, A.A.; Calvé, A.; Vennin Rendos, H.; Djediai, S.; Cuisiniere, T.; Laplante, P.; et al. Gut Microbiota Influence Anastomotic Healing in Colorectal Cancer Surgery through Modulation of Mucosal Proinflammatory Cytokines. Gut 2023, 72, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, N.; Dang, Q.; Liu, L.; Wang, L.; Li, H.; Han, X. Exploring the Roles of Intestinal Flora in Enhanced Recovery after Surgery. iScience 2023, 26, 105959. [Google Scholar] [CrossRef]
- Ciobârcă, D.; Cătoi, A.F.; Copăescu, C.; Miere, D.; Crișan, G. Bariatric Surgery in Obesity: Effects on Gut Microbiota and Micronutrient Status. Nutrients 2020, 12, 235. [Google Scholar] [CrossRef] [PubMed]
- Furtado, M. Probiotics, Prebiotics, Gut Microbiota, and Obesity. Bariatr. Times 2009, 6, 27–30. Available online: https://bariatrictimes.com/probiotics-prebiotics-gut-microbiota-and-obesity/ (accessed on 10 January 2023).
- Fernández-Alonso, M.; Aguirre Camorlinga, A.; Messiah, S.E.; Marroquin, E. Effect of Adding Probiotics to an Antibiotic Intervention on the Human Gut Microbial Diversity and Composition: A Systematic Review. J. Med. Microbiol. 2022, 71, e01625. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, K.R.; Wolfe, R.R.; Ferrando, A.A. Pre- and Post-Surgical Nutrition for Preservation of Muscle Mass, Strength, and Functionality Following Orthopedic Surgery. Nutrients 2021, 13, 1675. [Google Scholar] [CrossRef] [PubMed]
- Baldissarro, E.; Aquilani, R.; Boschi, F.; Baiardi, P.; Iadarola, P.; Fumagalli, M.; Pasini, E.; Verri, M.; Dossena, M.; Gambino, A.; et al. The Hip Functional Retrieval after Elective Surgery May Be Enhanced by Supplemented Essential Amino Acids. BioMed Res. Int. 2016, 2016, 9318329. [Google Scholar] [CrossRef] [PubMed]
- Church, D.D.; Schutzler, S.E.; Wolfe, R.R.; Ferrando, A.A. Perioperative Amino Acid Infusion Reestablishes Muscle Net Balance during Total Hip Arthroplasty. Physiol. Rep. 2021, 9, e15055. [Google Scholar] [CrossRef]
- Hendrickson, N.R.; Davison, J.; Glass, N.A.; Wilson, E.S.; Miller, A.; Leary, S.; Lorentzen, W.; Karam, M.D.; Hogue, M.; Marsh, J.L.; et al. Conditionally Essential Amino Acid Supplementation Reduces Postoperative Complications and Muscle Wasting After Fracture Fixation: A Randomized Controlled Trial. J. Bone Jt. Surg. 2022, 104, 759–766. [Google Scholar] [CrossRef]
- Harris, R.M. Essential Amino Acid Supplementation: Feed the Injured Patient: Commentary on an Article by Nathan R. Hendrickson, MD; et al.: “Conditionally Essential Amino Acid Supplementation Reduces Postoperative Complications and Muscle Wasting After Fracture Fixation. A Randomized Controlled Trial”. J. Bone Jt. Surg. 2022, 104, e38. [Google Scholar] [CrossRef]
- Donatelli, F.; Schricker, T.; Mistraletti, G.; Asenjo, F.; Parrella, P.; Wykes, L.; Carli, F. Postoperative Infusion of Amino Acids Induces a Positive Protein Balance Independently of the Type of Analgesia Used. Anesthesiology 2006, 105, 253–259. [Google Scholar] [CrossRef]
- Cogo, E.; Elsayed, M.; Liang, V.; Cooley, K.; Guerin, C.; Psihogios, A.; Papadogianis, P. Are Supplemental Branched-Chain Amino Acids Beneficial during the Oncological Peri-Operative Period: A Systematic Review and Meta-Analysis. Integr. Cancer Ther. 2021, 20, 153473542199755. [Google Scholar] [CrossRef]
- Aoki, Y.; Aoshima, Y.; Atsumi, K.; Kaminaka, R.; Nakau, R.; Yanagida, K.; Kora, M.; Fujii, S.; Yokoyama, J. Perioperative Amino Acid Infusion for Preventing Hypothermia and Improving Clinical Outcomes during Surgery under General Anesthesia: A Systematic Review and Meta-Analysis. Anesth. Analg. 2017, 125, 793–802. [Google Scholar] [CrossRef]
- Mayman, D.J. Essential Amino Acid Supplementation Associated with Improved TKA Recovery. Available online: https://news.hss.edu/essential-amino-acid-supplementation-associated-with-improved-tka-recovery/ (accessed on 12 January 2023).
- Yokoyama, T.; Yamaoka, I.; Hitosugi, T.; Selldén, E. Amino Acids during Perioperative Period. Open J. Anesthesiol. 2017, 7, 287–295. [Google Scholar] [CrossRef][Green Version]
- Bischoff, S.C.; Barazzoni, R.; Busetto, L.; Campmans-Kuijpers, M.; Cardinale, V.; Chermesh, I.; Eshraghian, A.; Kani, H.T.; Khannoussi, W.; Lacaze, L.; et al. European Guideline on Obesity Care in Patients with Gastrointestinal and Liver Diseases—Joint ESPEN/UEG Guideline. Clin. Nutr. 2022, 41, 2364–2405. [Google Scholar] [CrossRef] [PubMed]
- Brunani, A.; Perna, S.; Soranna, D.; Rondanelli, M.; Zambon, A.; Bertoli, S.; Vinci, C.; Capodaglio, P.; Lukaski, H.; Cancello, R. Body Composition Assessment Using Bioelectrical Impedance Analysis (BIA) in a Wide Cohort of Patients Affected with Mild to Severe Obesity. Clin. Nutr. 2021, 40, 3973–3981. [Google Scholar] [CrossRef] [PubMed]
- Johnson Stoklossa, C.A.; Forhan, M.; Padwal, R.S.; Gonzalez, M.C.; Prado, C.M. Practical Considerations for Body Composition Assessment of Adults with Class II/III Obesity Using Bioelectrical Impedance Analysis or Dual-Energy X-ray Absorptiometry. Curr. Obes. Rep. 2016, 5, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Coppini, L.Z.; Waitzberg, D.L.; Campos, A.C.L. Limitations and Validation of Bioelectrical Impedance Analysis in Morbidly Obese Patients. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 329–332. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ERABS Item | Publication | Type | Main Findings |
|---|---|---|---|
| [35] | Clinical guidelines | Avoiding PF is a part of ERAS | |
| [39] | article | Quit PF | |
| Preoperative fasting | [40] | Systematic review | Many anaesthetists follow outdated practices |
| [43] | Retrospective analysis | Need for aspiration is uncommon | |
| [45] | Retrospective study | Shorter PF favours recovery | |
| [51] | Comment | PF can be reasonable in some circumstances | |
| [65] | Observational study | Fluid intake reduces hospital stay | |
| [32] | Systematic review | Evidence about PreCL is low | |
| [37] | review | PreCL is beneficial | |
| [38] | review | PreCL reduces discomfort | |
| Preoperative carbohydrates load | [52] | RCT | PreCL does not reduce nausea |
| [54] | Review | PreCL reduce IR and improve SR | |
| [55] | Systematic review | PreCL reduces LOS | |
| [56] | RCT | PreCL does not rise risks | |
| [57] | Meta-analysis | PreCL can reduce LOS in major surgery | |
| [58] | RCT | PreCL accelerates recovery after RY | |
| Postoperative fasting/early refeeding | [31] | Retrospective study | Early feeding shortens LOS |
| [49] | Systematic review | Post-operative fasting has negative effects | |
| [69] | Retrospective study | Early feeding improves food tolerance | |
| [70] | Retrospective study | Early fluid intake reduces pain and complications |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flore, G.; Deledda, A.; Fosci, M.; Lombardo, M.; Moroni, E.; Pintus, S.; Velluzzi, F.; Fantola, G. Perioperative Nutritional Management in Enhanced Recovery after Bariatric Surgery. Int. J. Environ. Res. Public Health 2023, 20, 6899. https://doi.org/10.3390/ijerph20196899
Flore G, Deledda A, Fosci M, Lombardo M, Moroni E, Pintus S, Velluzzi F, Fantola G. Perioperative Nutritional Management in Enhanced Recovery after Bariatric Surgery. International Journal of Environmental Research and Public Health. 2023; 20(19):6899. https://doi.org/10.3390/ijerph20196899
Chicago/Turabian StyleFlore, Giovanna, Andrea Deledda, Michele Fosci, Mauro Lombardo, Enrico Moroni, Stefano Pintus, Fernanda Velluzzi, and Giovanni Fantola. 2023. "Perioperative Nutritional Management in Enhanced Recovery after Bariatric Surgery" International Journal of Environmental Research and Public Health 20, no. 19: 6899. https://doi.org/10.3390/ijerph20196899
APA StyleFlore, G., Deledda, A., Fosci, M., Lombardo, M., Moroni, E., Pintus, S., Velluzzi, F., & Fantola, G. (2023). Perioperative Nutritional Management in Enhanced Recovery after Bariatric Surgery. International Journal of Environmental Research and Public Health, 20(19), 6899. https://doi.org/10.3390/ijerph20196899