
Results of the MOVE MS Program: A Feasibility Study on Group Exercise for Individuals with Multiple Sclerosis



Abstract
1. Introduction
2. Materials and Methods
2.1. Program Design
Program Description
2.2. Research Design
2.2.1. Recruitment
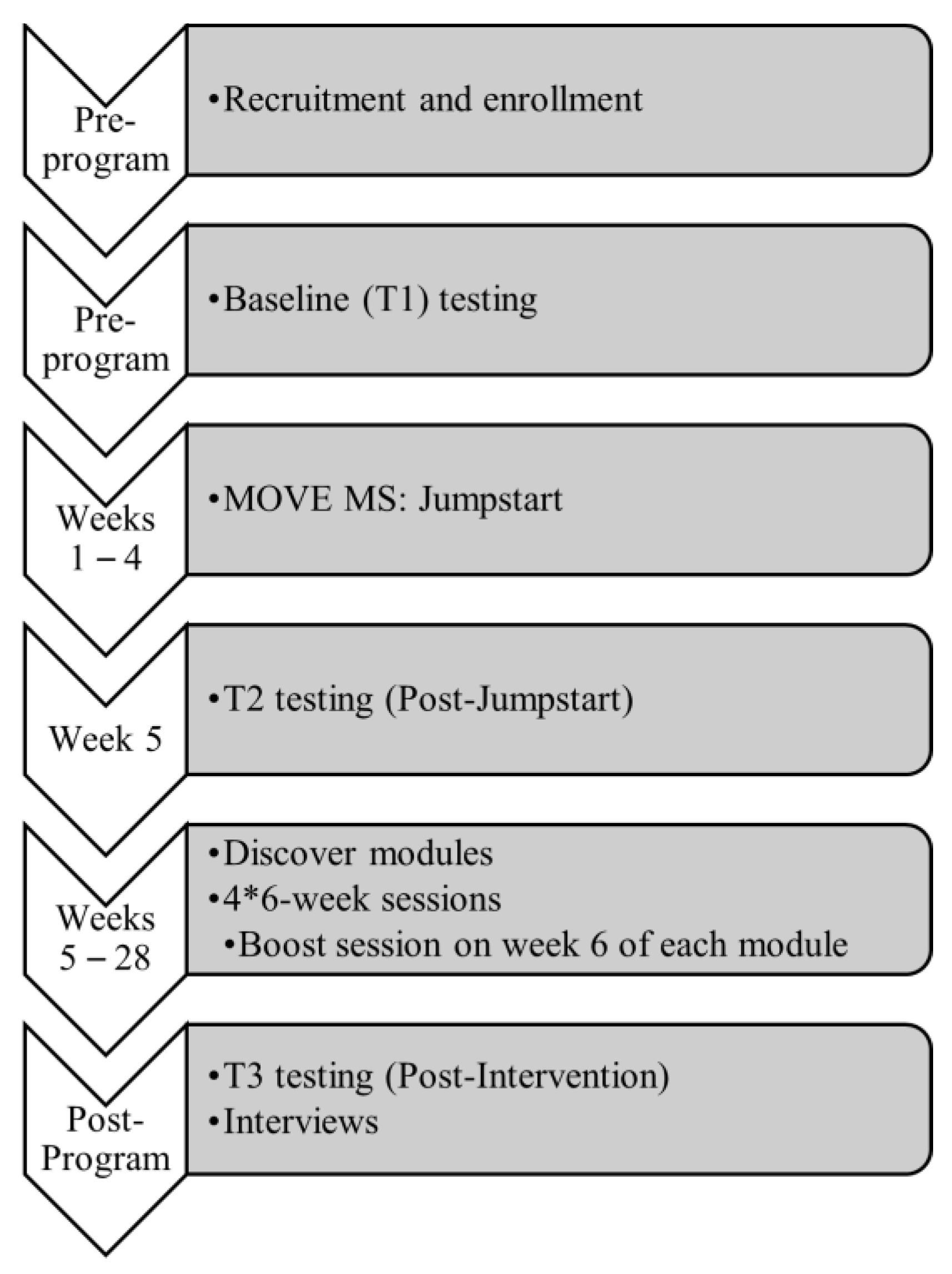
2.2.2. Research Procedures
2.2.3. Feasibility Outcome Measures
2.2.4. Qualitative Data Collection
2.2.5. Scientific Outcome Measures
2.3. Statistical Analysis
2.4. Qualitative Analysis
Quality
3. Results
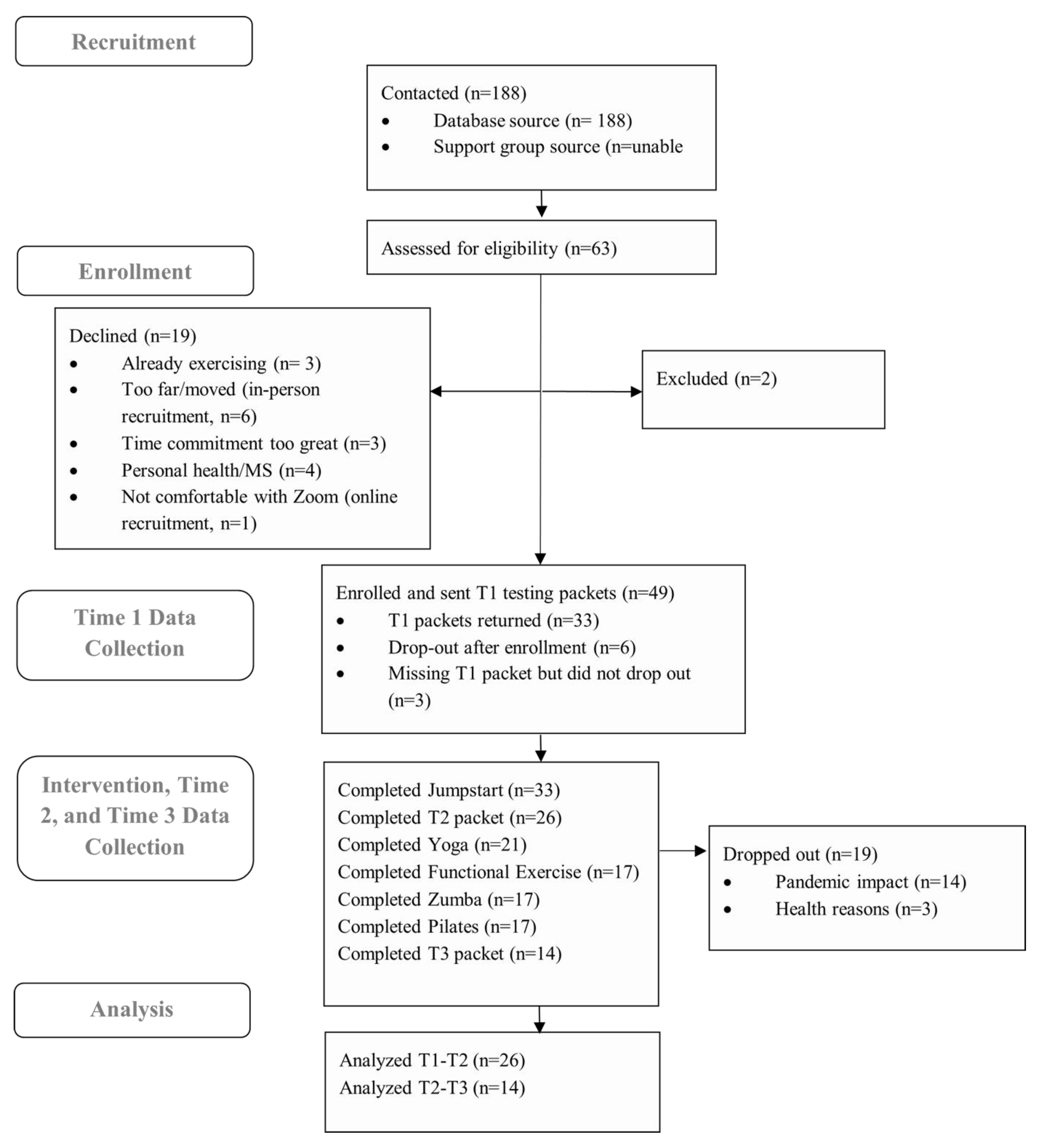
3.1. Recruitment and Enrollment
3.2. Baseline Participant Demographics
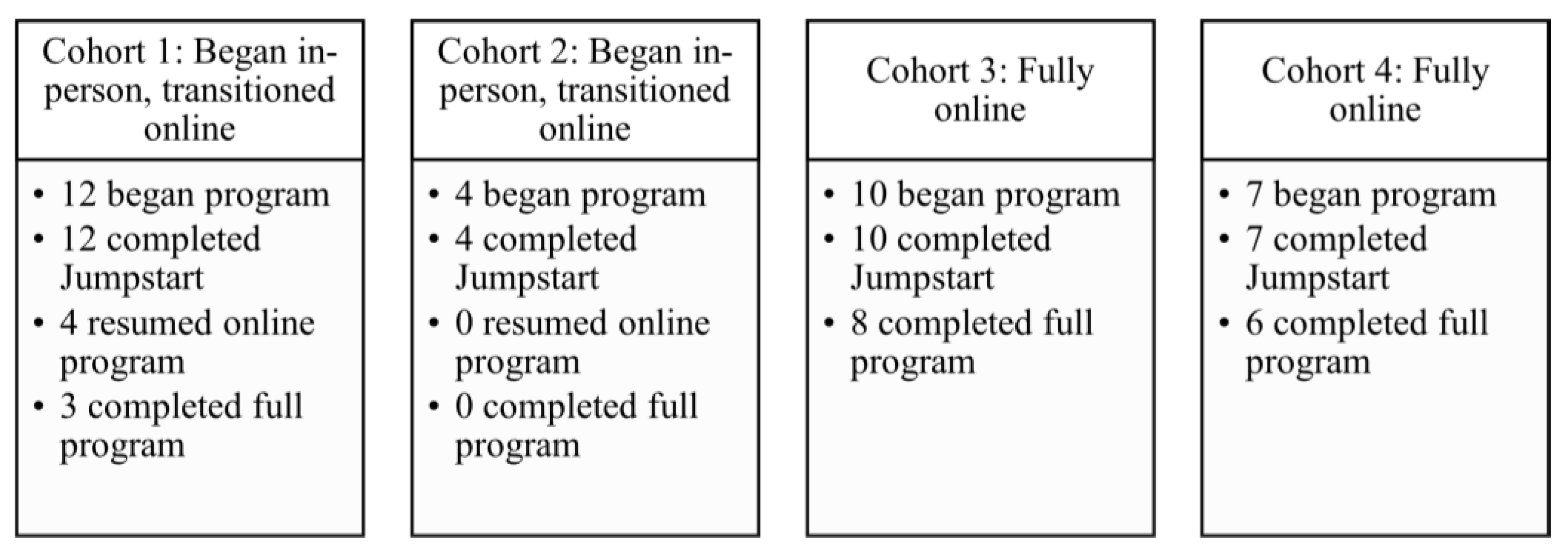
3.3. Intervention Delivery
3.4. Feasibility Metrics
3.5. Scientific Feasibility
3.6. Program Feedback
3.7. Qualitative Results from Interviews
3.7.1. Facilitators and Barriers to MOVE MS Participation
I would say the biggest difficulty was just my own technical difficulty, but honestly, having the Zoom class that was so convenient because for me, like fatigue is one of my big issues, and it takes a lot of energy for me to get up and get ready, get dressed, get out of the house to the health center. And then that’s a pretty good walk. And then, exercise for an hour and then go home. With the zoom, you can just go to the chair so you can save all that energy for the class itself. Honestly, the Zoom classes were kind of a godsend.
3.7.2. Module and Instructor Feedback
I think definitely having an instructor with MS, was super helpful. Just because it gives you like that extra confidence of like, well she can do it I can do it. It was all made it easier to kind of see how her body would react and be like, oh okay so that is normal… So for her to offer those suggestions based on the way her own body was responding was very helpful to me.(Participant 203)
3.7.3. Group Dynamic
Before class, I [wasn’t sure] if I could keep up with these people. But, obviously, it doesn’t matter. We’re all going through different things… After probably the first month, we kind of formed that team. And we’re all there for each other, which was good, and actually very supportive.(Participant 307)
Knowing the people that I’ve been online with get excited when I logged in and they’re all on and they’re all talking and stuff like that. So, I think that’s what got me motivated to—to stay on with the program.(Participant 304)
3.7.4. Suggestions for Improvement
I wish there was a bank of videos to watch on the days we didn’t have class because I was definitely not as good about [exercising] when we didn’t have a scheduled class, but I felt like if I could put in my calendar, I’d watch the video and do it. That’s just how I am. If it’s not an actual obligation and I can put a video on or like have someone show me how to do it, then it’s hard for me to find that time.(Participant 203)
3.7.5. MOVE MS is a Reminder That MS Affects Everyone Differently
I don’t know that [MOVE MS] changed [my understanding of disability], but I’ve been reminded that people with MS come in all shapes and sizes and colors and levels of impairment. It’s interesting that there are some symptoms that almost everyone identifies with and others that are particular to that individual.(Participant 108)
In the general sense of disability, I would say no, however, you know you have a piece of pie that represents disability, right? So, what MOVE MS did was, okay, I have my pie disability but now I have a little bit more information to add to the picture, so I might add a little whipped cream and a little whatever on top of the pie because it’s just an additional information to complete the picture that much more. Just interacting with people that are in the same boat, you know, just hearing what they might be met with or working through that day, or, you know, what their life is like. Yeah, I just think it made the picture a bit more complete.(Participant 204)
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Semi-Structured Interview Questions
Establishing the Perceived Benefits or Any Adverse Consequences from Taking Part in the Exercise Program
- (1)
- Can you tell me about any expectations you had before participating in this program?
- What did you think about exercise for people with MS before beginning the program? Has this changed?
- (2)
- Can you give me an overall evaluation of the MOVE MS program? What did you like? What did you dislike?
- If you’ve experienced any benefits from doing the MOVE MS program, will you tell me about them please?
- When did you become aware of these benefits?
- Did experiencing these benefits change anything for you? How did they impact your life?
- (3)
- Did you experience any problems or have any non-beneficial experiences from participating in the program?
- Did experiencing these things change anything for you?
Evaluative questions on the program
- (4)
- Remind me how you first found out about the MOVE MS program (program guides, television, newspaper, support group, email, phone call, doctor’s office, center, other).
- How else could we have let you know about the opportunity to take part?
- (5)
- What made you contact us after you found out about the program?
- What motivated you to say “Yes” to participating?
Now we will discuss your participation in the program
- (6)
- Can you tell me about any problems you overcame to participate in the program?
- What could we have done to help lessen those problems?
- (7)
- What did you think about exercising in a group and in the center/online via Zoom?
- What would have made it easier?
- (8)
- Which modules did you complete? What did you think of the exercises that you did? (i.e., Zumba, pilates, yoga, aquatics, functional exercise)
- In what way(s) were they appropriate or not appropriate for you? Why? (fitness, MS, busy life, home environment?)
- (9)
- What did you think about the instructors throughout the program?
- Tell me about your experiences with the various instructors
- (10)
- What are your perceptions of having a peer with MS teaching some of the modules?
- (11)
- What made it possible for you to stick with this program?
- (12)
- Overall, thinking about the entire program, what aspect of the program do you think was the most important for your overall health? Why?
- (13)
- Overall, thinking about the entire program, what aspect of the program did you enjoy the most? Why?
- (14)
- How do you think we could improve the program?
- (15)
- In what ways have your views about disability changed as a result of being involved in MOVE MS if at all?
- Social component? (interacting with others with MS)
- Educational component? (learning about different ways to perceive exercise)
- Physical component? (just exercising in my body)
Appendix B. Primary and Secondary Scientific Feasibility Outcomes

{kind=link}
{kind=link}
{kind=link}
| Baseline (T1) n = 33 | Post-Jumpstart (T2) n = 26 | Follow-Up (T3) n = 15 | T1-T2 n = 25 | T1-T2 n = 25 | T1-T2-T3 n = 14 | T1-T2-T3 n = 14 | |
|---|---|---|---|---|---|---|---|
| Outcome | Mean (SD) | Mean (SD) | Mean (SD) | F-value | Partial Eta 2 | F-value | Partial Eta 2 |
| GLTEQ | 14.2 (11.8) | 16.2 (11.7) | 16.6 (11.2) | 0.34 | 0.01 | 0.53 | 0.08 |
| PDDS | 2.5 (2.3) | 2.5 (2.1) | 2.7 (2.2) | 2.00 | 0.08 | 0.18 | 0.03 |
| MSIS-Psych | 35.6 (19.4) | 30.4 (18.7) | 32.4 (17.5) | 2.12 | 0.09 | 1.07 | 0.16 |
| MSIS-Phys | 33.0 (23.3) | 32.9 (19.4) | 34.4 (23.8) | 3.76 | 0.14 | 0.48 | 0.09 |
| MSWS-12 | 44.1 (32.4) | 42.1 (30.2) | 37.4 (34.1) | 2.09 | 0.08 | 1.68 | 0.23 |
| LMSQOL | 12.2 (4.3) | 10.6 (3.7) | 10.53 (3.9) | 2.90 | 0.11 | 2.63 | 0.32 |
| HADS-Anx | 6.0 (3.7) | 5.8 (3.2) | 6.64 (2.7) | 0.06 | 0.003 | 0.23 | 0.04 |
| HADS-Dep | 7.2 (2.6) | 7.2 (2.9) | 7.46 (2.9) | 0.05 | 0.002 | 0.48 | 0.09 |
| UCLALS | 17.2 (13.6) | 18.9 (14.3) | 18.33 (13.4) | 0.16 | 0.007 | 0.44 | 0.07 |
| LOT-R | 17.7 (4.3) | 17.0 (4.3) | 18.60 (4.9) | 0.14 | 0.006 | 0.57 | 0.10 |
| UWSES | 47.7 (6.7) | 48.0 (9.1) | 47.76 (6.7) | 0.04 | 0.002 | 0.43 | 0.11 |
| ESES | 74.9 (29.5) | 48.6 (22.6) | 48.48 (20.7) | 63.34 | 0.73 | 49.78 | 0.90 * |
| IRAS-SI | 29.1 (7.5) | 30.1 (7.2) | 28.33 (7.4) | 1.92 | 0.07 | 1.80 | 0.23 |
| IRAS-RI | 12.6 (6.1) | 12.7 (6.8) | 12.14 (5.9) | 0.57 | 0.03 | 1.76 | 0.24 |
| IRAS-II | 28.2 (3.4) | 28.1 (3.1) | 29.93 (2.8) | 0.53 | 0.02 | 1.08 | 0.15 |
Appendix C. Feedback Results
| Jumpstart Mean (n = 20) | Yoga Mean (n = 18) | Functional Mean (n = 12) | Zumba Mean (n = 11) | Pilates Mean (n = 10) | |
|---|---|---|---|---|---|
| Overall Satisfaction | 5.0 | 4.5 | 4.5 | 4.3 | 4.5 |
| Instructor Satisfaction | 4.8 | 4.7 | 4.7 | 5.0 | 4.6 |
| Progression Satisfaction | n/a | 4.3 | 4.6 | 4.6 | 4.7 |
| Appropriate based on MS | 5.0 | 4.3 | 4.7 | 4.4 | 4.4 |
| Appropriate based on fitness | 4.6 | 4.3 | 4.7 | 4.3 | 4.1 |
| Sufficient team support | 5.0 | 4.9 | 4.8 | 4.9 | 4.8 |
| I will use what I learned to keep exercising | 4.8 | 4.6 | 4.6 | 4.4 | 4.0 |
| Exemplary Open-Ended Comments on Feedback Surveys | My physical level made some of the exercises not as challenging, but I was glad to be in an atmosphere of accessibility for others. (Participant 106) | Yoga made me feel really good doing it with others who understand MS. (Participant 202) Many of the moves are harder to do in the chair compared to the floor (Participant 206) | I would present this info at the beginning of the study and integrate it into all classes. (Participant 303) All way appropriate and helpful for my MS. (Participant 306) | It was something new, I did notice increased stamina by the end of class. (Participant 210) Love how she teaches the steps for seated and standing. (Participant 212) | [The peer instructor] is GREAT. She is clear, adaptive, and encouraging to her students. I have proprioception issues, so Pilates was especially helpful. (Participant 108) |
References
- Ensari, I.; Motl, R.W.; Pilutti, L.A. Exercise training improves depressive symptoms in people with multiple sclerosis: Results of a meta-analysis. J. Psychosom. Res. 2014, 76, 465–471. [Google Scholar] [CrossRef]
- Pilutti, L.A.; Greenlee, T.A.; Motl, R.W.; Nickrent, M.S.; Petruzzello, S.J. Effects of exercise training on fatigue in multiple sclerosis: A meta-analysis. Psychosom. Med. 2013, 75, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Pilutti, L.A. The benefits of exercise training in multiple sclerosis. Nat. Rev. Neurol. 2012, 8, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Pilutti, L.A. Is physical exercise a multiple sclerosis disease modifying treatment? Expert Rev. Neurother. 2016, 16, 951–960. [Google Scholar] [CrossRef]
- Latimer-Cheung, A.E.; Ginis, K.A.M.; Hicks, A.L.; Motl, R.W.; Pilutti, L.A.; Duggan, M.; Wheeler, G.; Persad, R.; Smith, K.M. Development of evidence-informed physical activity guidelines for adults with multiple sclerosis. Arch. Phys. Med. Rehabil. 2013, 94, 1829–1836. [Google Scholar] [CrossRef]
- Tarakci, E.; Yeldan, I.; Huseyinsinoglu, B.E.; Zenginler, Y.; Eraksoy, M. Group exercise training for balance, functional status, spasticity, fatigue and quality of life in multiple sclerosis: A randomized controlled trial. Clin. Rehabil. 2013, 27, 813–822. [Google Scholar] [CrossRef]
- Carling, A.; Forsberg, A.; Gunnarsson, M.; Nilsagård, Y. CoDuSe group exercise programme improves balance and reduces falls in people with multiple sclerosis: A multi-centre, randomized, controlled pilot study. Mult. Scler. J. 2016, 23, 1394–1404. [Google Scholar] [CrossRef]
- Ayán Pérez, C.L.; De Paz Fernández, J.A.; Sánchez, V.M.; de Souza Teixeira, F. Individuals with multiple sclerosis who participate in a 6-week group exercise programme “show an improvement in their quality of life and fatigue”. Sport Sci. Health 2011, 6, 85–88. [Google Scholar] [CrossRef]
- Learmonth, Y.C.; Marshall-McKenna, R.; Paul, L.; Mattison, P.; Miller, L. A qualitative exploration of the impact of a 12-week group exercise class for those moderately affected with multiple sclerosis. Disabil. Rehabil. 2013, 35, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Paul, L.; McFadyen, A.K.; Marshall-McKenna, R.; Mattison, P.; Miller, L.; McFarlane, N.G. Short-term effect of aerobic exercise on symptoms in multiple sclerosis and chronic fatigue syndrome. Int. J. MS Care 2014, 16, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Wynne, D.; Rickhart, E.; Cooper, K. Investigating adherence and quality of life in relation to group based exercise among individuals with multiple sclerosis: A systematic review. Physiotherapy 2017, 103, e97. [Google Scholar] [CrossRef]
- Aubrey, G.; Demain, S. Perceptions of group exercise in the management of multiple sclerosis. Int. J. Ther. Rehabil. 2012, 19, 557–565. [Google Scholar] [CrossRef]
- Kinnett-Hopkins, D.; Adamson, B.; Rougeau, K.; Motl, R.W. People with MS are less physically active than healthy controls but as active as those with other chronic diseases: An updated meta-analysis. Mult. Scler. Relat. Disord. 2017, 13, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Motl, R.W. Physical activity and exercise training in multiple sclerosis: A review and content analysis of qualitative research identifying perceived determinants and consequences. Disabil. Rehabil. 2016, 38, 1227–1242. [Google Scholar] [CrossRef] [PubMed]
- Riemann-Lorenz, K.; Wienert, J.; Streber, R.; Motl, R.W.; Coote, S.; Heesen, C. Long-term physical activity in people with multiple sclerosis: Exploring expert views on facilitators and barriers. Disabil. Rehabil. 2020, 42, 3059–3071. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Mowry, E.M.; Ehde, D.M.; LaRocca, N.G.; Smith, K.E.; Costello, K.; Shinto, L.; Ng, A.V.; Sullivan, A.B.; Giesser, B.; et al. Wellness and multiple sclerosis: The National MS Society establishes a Wellness Research Working Group and research priorities. Mult. Scler. J. 2018, 24, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Danoudis, M.; Iansek, R. A long-term community gym program for people with Parkinson’s disease: A feasibility study of the Monash Health “Health and Fitness” model. Disabil. Rehabil. 2022, 44, 7330–7338. [Google Scholar] [CrossRef]
- Collett, J.; Franssen, M.; Meaney, A.; Wade, D.; Izadi, H.; Tims, M.; Winward, C.; Bogdanovic, M.; Farme, A.; Dawes, H. Phase II randomised controlled trial of a 6-month self-managed community exercise programme for people with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 204–211. [Google Scholar] [CrossRef]
- Rafferty, M.R.; Prodoehl, J.; Robichaud, J.A.; David, F.J.; Poon, C.; Goelz, L.C.; Vaillancourt, D.E.; Kohrt, W.M.; Comella, C.L.; Corcos, D.M. Effects of 2 years of exercise on gait impairment in people with Parkinson Disease: The PRET-PD randomized trial. J. Neurol. Phys. Ther. 2017, 41, 21–30. [Google Scholar] [CrossRef]
- The LIFE group. Supporting community-based exercise in long-term neurological conditions: Experience from the Long-term Individual Fitness Enablement (LIFE) project. Clin. Rehabil. 2011, 25, 579–587. [Google Scholar] [CrossRef]
- Pérez-Rodríguez, M.; Gutiérrez-Suárez, A.; Arias, J.Á.R.; Andreu-Caravaca, L.; Pérez-Tejero, J. Effects of Exercise Programs on Functional Capacity and Quality of Life in People With Acquired Brain Injury: A Systematic Review and Meta-Analysis. Phys. Ther. 2023, 103, pzac153. [Google Scholar] [CrossRef] [PubMed]
- Bynon, B.; White, J.; Marquez, J.; Pollack, M. Master Stroke: A mixed methods study exploring the experience of community dwelling stroke survivors in a pilot, group stroke prevention program. Int. J. Stroke 2012, 7, 931–938. [Google Scholar]
- Duncan, P.W.; Studenski, S.; Richards, L.; Gollub, S.; Lai, S.M.; Reker, D.; Perera, S.; Yates, J.; Koch, V.; Rigler, S.; et al. Randomized clinical trial of therapeutic exercise in subacute stroke. Stroke 2003, 34, 2173–2180. [Google Scholar] [CrossRef] [PubMed]
- Bakkum, A.J.T.; De Groot, S.; Stolwijk-Swüste, J.M.; Van Kuppevelt, D.J.; Van Der Woude, L.H.V.; Janssen, T.W.J. Effects of hybrid cycling versus handcycling on wheelchair-specific fitness and physical activity in people with long-term spinal cord injury: A 16-week randomized controlled trial. Spinal Cord 2015, 53, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Elsworth, C.; Winward, C.; Sackley, C.; Meek, C.; Freebody, J.; Esser, P.; Izadi, H.; Soundy, A.; Barker, K.; Hilton-Jones, D.; et al. Supported community exercise in people with long-term neurological conditions: A phase II randomized controlled trial. Clin. Rehabil. 2011, 25, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.V.; Smith, B.; Papathomas, A. Disability and the gym: Experiences, barriers and facilitators of gym use for individuals with physical disabilities. Disabil. Rehabil. 2016, 39, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.V.; Adamson, B.C. A syndemics approach to exercise is medicine. Health 2023, 27, 323–344. [Google Scholar] [CrossRef]
- Adamson, B.C.; Adamson, M.D.; Littlefield, M.M.; Motl, R.W. Move it or lose it: Perceptions of the impact of physical activity on multiple sclerosis symptoms, relapse, and disability identity. Qual. Res. Sport Exerc. Health 2018, 10, 457–475. [Google Scholar] [CrossRef]
- Vick, A. The embodied experience of episodic disability among women with multiple sclerosis. Disabil. Soc. 2013, 28, 176–189. [Google Scholar] [CrossRef]
- Adamson, B.; Adamson, M.; Clarke, C.; Richardson, E.V.; Sydnor, S. Social Justice Through Sport and Exercise Studies: A Manifesto. J. Sport Soc. Issues 2022, 46, 407–444. [Google Scholar] [CrossRef]
- Adamson, B.; Adamson, M.; Kinnett-Hopkins, D.; Motl, R. Medicalization of Exercise through Vigilance, Productivity, and Self-Care: A Secondary Data Analysis of Qualitative Interviews among Those with Multiple Sclerosis. Adapt. Phys. Act. Q. 2022, 39, 399–423. [Google Scholar] [CrossRef]
- Bogart, K.R. Disability identity predicts lower anxiety and depression in multiple sclerosis. Rehabil. Psychol. 2015, 60, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Bogart, K.R. The role of disability self-concept in adaptation to congenital or acquired disability. Rehabil. Psychol. 2014, 59, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Bogart, K.R.; Rottenstein, A.; Lund, E.M.; Bouchard, L. Who Self-Identifies as Disabled? An Examination of Impairment and Contextual Predictors. Rehabil. Psychol. 2017, 62, 553–562. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Pekmezi, D.; Wingo, B.C. Promotion of physical activity and exercise in multiple sclerosis: Importance of behavioral science and theory. Mult. Scler. J. Exp. Transl. Clin. 2018, 4, 2055217318786745. [Google Scholar] [CrossRef]
- Crow, L. Lying down anyhow: An autoethnography. Qual. Inq. 2013, 20, 359–361. [Google Scholar] [CrossRef]
- Mingus, M. Moving Toward the Ugly: A Politic Beyond Desirability. Leaving Evidence. 2011. Available online: https://leavingevidence.wordpress.com/2011/08/22/moving-toward-the-ugly-a-politic-beyond-desirability/ (accessed on 15 May 2023).
- Mingus, M. Access Intimacy: The Missing Link. Leaving Evidence. 2011. Available online: https://leavingevidence.wordpress.com/2011/05/05/access-intimacy-the-missing-link/ (accessed on 15 May 2023).
- Peers, D.; Spencer-Cavaliere, N.; Eales, L. Say what you mean: Rethinking disability language in Adapted Physical Activity Quarterly. Adapt. Phys. Act. Q. 2014, 31, 265–282. [Google Scholar] [CrossRef]
- Smith, B.; Papathomas, A. Disability, Sport and Exercising Bodies. In Disabling Barriers—Enabling Environments, 3rd ed.; Swain, J., Thomas, C., French, S., Barnes, C., Eds.; Sage Publications: London, UK, 2014; pp. 1–354. [Google Scholar]
- Williams, T.L.; Hunt, E.R.; Papathomas, A.; Smith, B. Exercise is medicine? Most of the time for most; but not always for all. Qual. Res. Sport Exerc. Health 2018, 10, 441–456. [Google Scholar] [CrossRef]
- Richardson, E.V.; Smith, B.; Papathomas, A. Crossing boundaries: The perceived impact of disabled fitness instructors in the gym. Psychol. Sport Exerc. 2017, 29, 84–92. [Google Scholar] [CrossRef]
- Ginis, K.A.M.; Nigg, C.R.; Smith, A.L. Peer-delivered physical activity interventions: An overlooked opportunity for physical activity promotion. Transl. Behav. Med. 2013, 3, 434. [Google Scholar] [CrossRef]
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Methodol. 2010, 10, 67. [Google Scholar] [CrossRef]
- Tariq, S.; Woodman, J. Using mixed methods in health research. JRSM Short Rep. 2013, 4, 204253331347919. [Google Scholar] [CrossRef]
- O’Cathain, A.; Hoddinott, P.; Lewin, S.; Thomas, K.J.; Young, B.; Adamson, J.; Jansen, Y.J.F.M.; Mills, N.; Moore, G.; Donovan, J.L. Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: Guidance for researchers. Pilot Feasibility Stud. 2015, 1, 32. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of Patient Determined Disease Steps (PDDS) Scale Scores in Persons with Multiple Sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Godin, G. The Godin-Shephard leisure-time physical activity questionnaire. HAJC 2011, 4, 18–22. [Google Scholar]
- Motl, R.W.; Bollaert, R.E.; Sandroff, B.M. Validation of the Godin Leisure-Time Exercise Questionnaire Classification Coding System Using Accelerometry in Multiple Sclerosis. Rehabil. Psychol. 2017, 63, 77–82. [Google Scholar] [CrossRef]
- Hobart, J.; Lamping, D.; Fitzpatrick, R.; Riazi, A.; Thompson, A. The Multiple Sclerosis Impact Scale (MSIS-29): A new patient-based outcome measure. Brain 2001, 124, 962–973. [Google Scholar] [CrossRef]
- McGuigan, C.; Hutchinson, M. Confirming the validity and responsiveness of the Multiple Sclerosis Walking Scale-12 (MSWS-12). Neurology 2004, 62, 2103–2105. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Herzberg, P.Y.; Glaesmer, H.; Hoyer, J. Separating optimism and pessimism: A robust psychometric analysis of the revised Life Orientation Test (LOT-R). Psychol. Assess. 2006, 18, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Akbiyik, D.I.; Sumbuloglu, V.; Guney, Z.; Armutlu, K.; Korkmaz, N.; Keser, I.; Yuksel, M.M.; Karabudak, R. The validity and test-retest reliability of the Leeds Multiple Sclerosis Quality of Life scale in Turkish patients. Int. J. Rehabil. Res. 2009, 32, 162–166. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E. Self-efficacy and the maintenance of exercise participation in older adults. J. Behav. Med. 1993, 16, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Ingledew, D.K. The measurement of exercise motives: Factorial validity and invariance across gender of a revised Exercise Motivations Inventory. Br. J. Health Psychol. 1997, 2, 361–376. [Google Scholar] [CrossRef]
- Stepleman, L.M.; Floyd, R.M.; Valvano-Kelley, A.; Penwell-Waines, L.; Wonn, S.; Crethers, D.; Rahn, R.; Smith, S. Developing a measure to assess identity reconstruction in patients with multiple sclerosis. Rehabil. Psychol. 2017, 62, 165–177. [Google Scholar] [CrossRef]
- Connelly, L.M.; Peltzer, J.N. Underdeveloped Themes in Qualitative Research. Clin. Nurse Spec. 2016, 30, 52–57. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. IJQHC 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Giorgi, A.P.; Giorgi, B.M. The descriptive phenomenological method in Qualitative Research in Psychology: Expanding perspectives in methodology and design. In Qualitative Research in Psychology: Expanding Perspectives in Methodology and Design, 1st ed.; Camic, P.M., Rhodes, J.E., Yardley, L., Eds.; American Psychological Association: Washington, DC, USA, 2003; pp. 243–274. [Google Scholar]
- Smith, J.; Osborn, M. Interpretative phenomenological analysis. In Qualitative Psychology: A Practical Guide; Smith, J., Ed.; Sage: London, UK, 2003; pp. 229–254. [Google Scholar]
- Smith, J.; Flowers, P.; Larkin, M. Interpretative Phenomenological Analysis: Theory, Method and Research, 1st ed.; Sage: Los Angeles, CA, USA, 2009. [Google Scholar]
- Smith, B.; McGannon, K.R. Developing rigor in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport Exerc. Psychol. 2017, 11, 101–121. [Google Scholar] [CrossRef]
- Sebastião, E.; McAuley, E.; Shigematsu, R.; Adamson, B.C.; Bollaert, R.E.; Motl, R.W. Home-based, square-stepping exercise program among older adults with multiple sclerosis: Results of a feasibility randomized controlled study. Contemp. Clin. Trials 2018, 73, 136–144. [Google Scholar] [CrossRef]
- Learmonth, Y.C.; Adamson, B.C.; Kinnett-Hopkins, D.; Bohri, M.; Motl, R.W. Results of a feasibility randomised controlled study of the guidelines for exercise in multiple sclerosis project. Contemp. Clin. Trials 2017, 54, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.; Edginton-Bigelow, K.; Bowsheir, C.; Weston, M.; Grant, E. Feasibility and effects of a group kickboxing program for individuals with multiple sclerosis: A pilot report. J. Bodyw. Mov. Ther. 2012, 16, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.M.; Daley, A.J.; Kesterton, S.W.; Woodroofe, N.M.; Saxton, J.M.; Sharrack, B. Pragmatic exercise intervention in people with mild to moderate multiple sclerosis: A randomised controlled feasibility study. Contemp. Clin. Trials 2013, 35, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Baez, M.; Far, I.K.; Ibarra, F.; Ferron, M.; Didino, D.; Casati, F. Effects of online group exercises for older adults on physical, psychological and social wellbeing: A randomized pilot trial. PeerJ 2017, 2017, 1–27. [Google Scholar] [CrossRef]
- Cutrona, C.E.; Russell, D. The provisions of social relationships and adaptation to stress. Adv. Pers. Relatsh. 1987, 1, 37–67. [Google Scholar]
- Estabrooks, P.A.; Carron, A.V. The Physical Activity Group Environment Questionnaire: An instrument for the assessment of cohesion in exercise classes. Group Dyn. 2000, 4, 230–243. [Google Scholar] [CrossRef]



| Mean/N | SD/% | |
|---|---|---|
| Gender | ||
| Female | 25 | 75.8 |
| Male | 7 | 21.2 |
| Other | 1 | 3.0 |
| Age | 55.2 | 1.7 |
| Employment | ||
| Employed | 12 | 36.4 |
| Unemployed | 21 | 63.6 |
| Marital Status | ||
| Married | 20 | 60.6 |
| Never married | 6 | 18.2 |
| Divorced/separated | 4 | 12.1 |
| Widow/widower | 3 | 9.1 |
| Race | ||
| Black or African American | 3 | 9.1 |
| White | 29 | 87.9 |
| Latino/a | 1 | 3.0 |
| Education | ||
| High School Graduate | 8 | 24.2 |
| 1–3 Years of College | 8 | 24.2 |
| College/University Graduate | 11 | 33.3 |
| Master’s Degree | 3 | 9.1 |
| PhD or Equivalent | 3 | 9.1 |
| Income | ||
| <$25,000/year | 5 | 16.7 |
| $25,001–$45,000/year | 8 | 26.7 |
| $45,001–$65,000/year | 4 | 13.4 |
| >$65,001/year | 13 | 43.3 |
| Type of MS | ||
| RRMS | 25 | 78.1 |
| PPMS | 2 | 6.3 |
| SPMS | 4 | 12.5 |
| Benign MS | 1 | 3.1 |
| Number of years with MS | 15.8 | 9.7 |
| PDDS | ||
| 0–2 | 18 | 54.5 |
| 3–5 | 10 | 30.3 |
| 6–8 | 5 | 15.1 |
| Metric | Monitoring and Assessment Strategy | Results |
|---|---|---|
| Process: Critical program processes | a. Recruitment and eligibility rates. b. Adherence, retention, compliance (attendance), and attrition rates. | a. Recruitment rate: 36 enrolled in program/188 contacted = 19.1%. Eligibility rate: 61 eligible/63 screened = 96.8%. b. Adherence rate: 17 completed intervention/33 began intervention = 52.0%. Retention rate: 17 completed intervention/33 began intervention = 52.0%. Attendance: 67% cohort 1, 75% cohort 2, 86% cohort 3, 79% cohort 4. Attrition rate: 22 did not complete T3 or dropped out/33 began the intervention = 66.7%. |
| Resource: Time and monetary resource needs | c. Communication with participants. d. Staff training time. e. Monetary costs of the intervention. | c. Communication time: = 1661 min. d. Staff training time: Instructor and research assistant training time = 850 min, e. Monetary resources: In-person to online cohorts = 1760.36 USD. Online only cohorts = 3701.80 USD. |
| Management: Data management needs, intervention fidelity | f. Staff time requirements for data collection, data entry, and checking. g. Missing data items. h. Intervention fidelity. | f. Staff time needs for data collection: = 1674 min. Staff time needs for data entry and checking: 1861 min. g. Missing data items: 50 missing items/13,486 total items = 99.6% complete h. Jumpstart Fidelity: Cohorts 1 and 2 completed as planned, Cohorts 3 and 4 completed virtually with same content. Discover Fidelity: Cohorts 1–4 received all 4 Discover modules in the order proposed, virtual instead of in person. |
| Scientific: Participant burden, safety, and efficacy | i. AEs, SAEs and clinical emergencies. j. Participant burden and satisfaction. k. Treatment effect. | i. Adverse events: 1 adverse event in 1 participant (possibly unrelated to the study), muscle soreness. Serious adverse events: none reported. j. Participant burden: Mean time to complete questionnaires: T1: 37.44 min, T2: 35.12 min, T2.5: 29 min, T3: 33.92 min. Mean time to complete interview: 65.42 min. Participant Satisfaction: Feedback summaries provided in supplementary material. k. Primary scientific outcome: GLTEQ T1 mean = 14.2 (SD = 11.8), T2 mean = 16.2 (SD = 11.7), T3 mean = 16.6 (SD = 11.2), F-value = 0.53 (Partial Eta2 = 0.08). See all other patient reported outcome measures in supplementary material. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamson, B.; Wyatt, N.; Key, L.; Boone, C.; Motl, R.W. Results of the MOVE MS Program: A Feasibility Study on Group Exercise for Individuals with Multiple Sclerosis. Int. J. Environ. Res. Public Health 2023, 20, 6567. https://doi.org/10.3390/ijerph20166567
Adamson B, Wyatt N, Key L, Boone C, Motl RW. Results of the MOVE MS Program: A Feasibility Study on Group Exercise for Individuals with Multiple Sclerosis. International Journal of Environmental Research and Public Health. 2023; 20(16):6567. https://doi.org/10.3390/ijerph20166567
Chicago/Turabian StyleAdamson, Brynn, Nic Wyatt, Latashia Key, Carrena Boone, and Robert W. Motl. 2023. "Results of the MOVE MS Program: A Feasibility Study on Group Exercise for Individuals with Multiple Sclerosis" International Journal of Environmental Research and Public Health 20, no. 16: 6567. https://doi.org/10.3390/ijerph20166567
APA StyleAdamson, B., Wyatt, N., Key, L., Boone, C., & Motl, R. W. (2023). Results of the MOVE MS Program: A Feasibility Study on Group Exercise for Individuals with Multiple Sclerosis. International Journal of Environmental Research and Public Health, 20(16), 6567. https://doi.org/10.3390/ijerph20166567