

Interventions to Facilitate Return to Work after Stroke: A Systematic Review

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Study Selection
2.4. Data Extraction and Analysis
3. Results
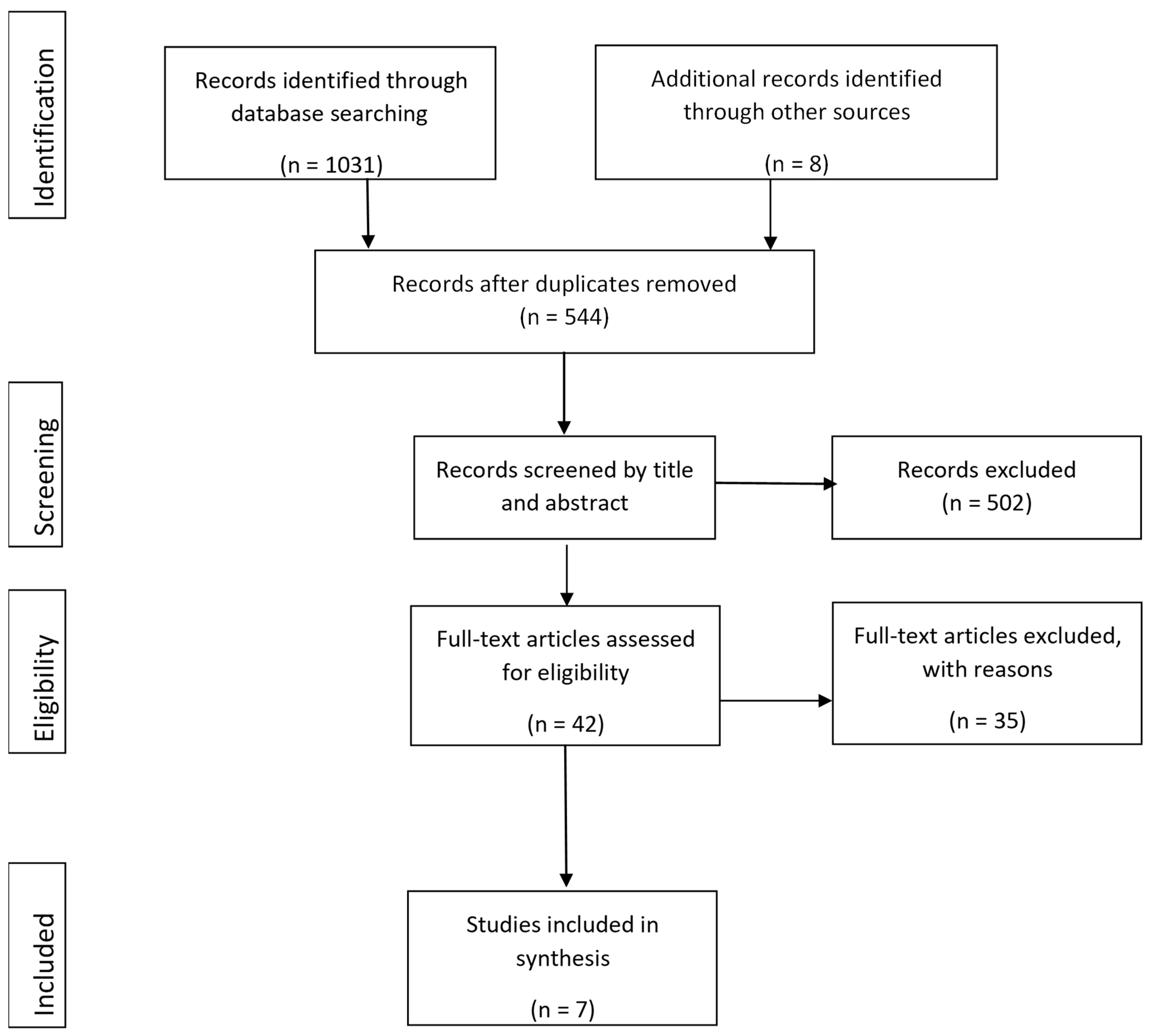
3.1. Study Selection
3.2. Study Characteristics

3.3. Methodological Quality Assessment
3.4. Study Population
3.5. Follow-up
3.6. Interventions
3.7. Outcomes
4. Discussion
4.1. Limitations
4.2. Conclusions and Directions for Future Research
- Implications for Rehabilitation:
- The incidence of stroke in people under the age of 65 is rising, so returning to work is an important outcome of rehabilitation.
- Rehabilitation efforts have not been designed to meet the needs of younger stroke survivors wishing to return to work, and there is limited available evidence for the efficacy of interventions to promote return to work in this population.
- Further research needs to be conducted and appropriate interventions implemented to ensure that stroke survivors receive the necessary assistance to transition back to work.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Search Terms and Search Strategies Searches Performed 28 September 2019
Appendix A.1.1. MEDLINE
- stroke.mp. or Stroke/(241,492)
- cerebrovascular accident.mp. (3776)
- CVA.mp. (2324)
- Cerebral Hemorrhage/or Subarachnoid Hemorrhage/or Brain Ischemia/or Cerebral Infarction/or ischaemic infarct.mp. (112,705)
- brain hemorrhage.mp. or Intracranial Hemorrhages/(7231)
- brain haemorrhage.mp. (154)
- intracerebral hemorrhage.mp. (9410)
- intracerebral haemorrhage.mp. (1705)
- subdural hemorrhage.mp. (548)
- subdural haemorrhage.mp. (161)
- brain infarction.mp. or Brain Infarction/(6008)
- cerebral ischemia.mp. (21,851)
- treatment.mp. or Therapeutics/(4,104,398)
- intervention.mp. (481,370)
- Rehabilitation/or Stroke Rehabilitation/or rehabilitation.mp. (281,828)
- occupational therapy.mp. or Occupational Therapy/(14,995)
- OT.mp. (21,768)
- return to work.mp. or Return to Work/(8242)
- re-employment.mp. (163)
- reemployment.mp. (120)
- job re-entry.mp. or Return to Work/(2159)
- job reentry.mp. (2)
- work resumption.mp. (139)
- employment resumption.mp. (0)
- job resumption.mp. (2)
- RTW.mp. (818)
- return-to-work.mp. (8242)
- returning to work.mp. (1120)
- RTW.mp. (818)
- back to work.mp. (635)
- unemployment.mp. or Unemployment/(12,161)
- work incapacity.mp. or Absenteeism/or Sick Leave/(13,565)
- work absence.mp. (323)
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 (333,845)
- 13 or 14 or 15 or 16 or 17 (4,591,868)
- 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 (33,416)
- 34 and 35 and 36 (240)
- limit 37 to (english language and humans and yr = “2000-Current”) (187)
Appendix A.1.2. Web of Science
Appendix A.1.3. PsycINFO
- exp Cerebral Ischemia/or exp Cerebrovascular Accidents/or stroke.mp. (36,920)
- CVA.mp. (428)
- ischemic infarct.mp. (59)
- exp Cerebral Hemorrhage/or brain hemorrhage.mp. (1990)
- exp Cerebral Hemorrhage/or intracerebral hemorrhage.mp. (2449)
- exp Subarachnoid Hemorrhage/or subarachnoid hemorrhage.mp. (1463)
- subdural hemorrhage.mp. (61)
- intracranial hemorrhage.mp. (494)
- exp Cerebral Ischemia/or brain ischemia.mp. (7179)
- brain infarction.mp. (1011)
- treatment.mp. or exp Treatment/(1,235,779)
- intervention.mp. or exp Intervention/(260,955)
- exp Rehabilitation/or rehabilitation.mp. (76,132)
- occupational therapy.mp. or exp Occupational Therapy/(10,223)
- OT.mp. (2276)
- return to work.mp. or exp Reemployment/(2988)
- re-employment.mp. (181)
- exp Vocational Rehabilitation/(7197)
- job re-entry.mp. (3)
- job reentry.mp. (6)
- work resumption.mp. (50)
- return to employment.mp. (60)
- return to job.mp. (8)
- work re-entry.mp. (21)
- employment resumption.mp. (1)
- job resumption.mp. (1)
- RTW.mp. (452)
- return-to-work.mp. (2574)
- returning to work.mp. (588)
- back to work.mp. (243)
- back-to-work.mp. (243)
- exp Unemployment/(4102)
- work incapacity.mp. (36)
- work absence.mp. (171)
- absenteeism.mp. (5525)
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 (40,485)
- 11 or 12 or 13 or 14 or 15 (1,329,444)
- 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 (19,369)
- 36 and 37 and 38 (116)
- limit 39 to (english language and yr = “2000–Current”) (105)
Appendix A.1.4. Scopus
- Cinahl:
| # | Query | Limiters/Expanders | Last Run Via |
| S16 | S12 AND S13 | Limiters-English Language; Published Date: 20000101–20191231 Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S15 | S12 AND S13 | Limiters-Published Date: 20000101–20191231 Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S14 | S12 AND S13 | Expanders-Apply equivalent subjects Search modes- Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S13 | S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S12 | S1 OR S2 OR S3 OR S4 | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S11 | “work resumption” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S10 | “job retraining” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S9 | “job reentry” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S8 | (MH “Rehabilitation, Vocational+”) OR “vocational rehabilitation” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S7 | “reemployment” | Expanders-Apply equivalent subjects Search modes- Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S6 | “re-employment” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S5 | (MH “Job Re-Entry”) OR “return to work” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S4 | “CVA” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S3 | “cerebrovascular accident” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S2 | “stroke rehabilitation” | Expanders-Apply equivalent subjects Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
| S1 | (MH “Stroke+”) OR “stroke” OR (MH “Stroke Patients”) | Expanders-Apply equivalent subjects Search modes- Boolean/Phrase | Interface-EBSCOhost Research Databases Search Screen-Advanced Search Database-CINAHL |
References
- George, M.G.; Tong, X.; Bowman, B.A. Prevalence of Cardiovascular Risk Factors and Strokes in Younger Adults. JAMA Neurol. 2017, 74, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Deloitte Access Economics. The Economic Impact of Stroke in Australia. 2013. Available online: https://www.deloitte.com/au/en/services/economics/perspectives/economic-impact-stroke-australia.html (accessed on 2 March 2023).
- Gottesman, R.F.; Hillis, A.E. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol. 2010, 9, 895–905. [Google Scholar] [CrossRef]
- Lawrence, E.S.; Coshall, C.; Dundas, R.; Stewart, J.; Rudd, A.G.; Howard, R.; Wolfe, C.D. Estimates of the prevalence of acute stroke impairments and disability in a multi-ethnic population. Stroke J. Am. Heart Assoc. 2001, 32, 1279–1284. [Google Scholar]
- Cumming, T.; Packer, M.; Kramer, S.F.; English, C. Review of the prevalence of fatigue after stroke: A systematic review and me-ta-analysis. Int. J. Stroke 2016, 11, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Australasian Faculty of Occupational & Environmental Medicine. Realising the Health Benefits of Work. 2011. Available online: https://www.racp.edu.au/docs/default-source/advocacy-library/realising-the-health-benefits-of-work.pdf (accessed on 2 March 2023).
- Ghatnekar, O.; Persson, U.; Glader, E.L.; Terent, A. Cost of stroke in Sweden: An incidence estimate. Int. J. Technol. Assess. Health 2004, 20, 375–380. [Google Scholar] [CrossRef]
- Lock, S.; Jordan, L.; Bryan, K.; Maxim, J. Work after stroke: Focusing on barriers and enablers. Disabil. Soc. 2005, 20, 33–47. [Google Scholar] [CrossRef]
- Medin, J.; Barajas, J.; Ekberg, K. Stroke patients’ experiences of return to work. Disabil. Rehabil. 2006, 28, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Röding, J.; Lindström, B.; Malm, J.A.N.; Öhman, A. Frustrated and invisible--younger stroke patients’ experiences of the rehabilitation process. Disabil. Rehabil. 2003, 25, 867–874. [Google Scholar] [CrossRef]
- Donker-Cools, B.H.P.M.; Daams, J.G.; Wind, H.; Frings-Dresen, M.H.W. Effective return-to-work interventions after acquired brain injury: A systematic review. Brain Inj. 2016, 30, 113–131. [Google Scholar] [CrossRef]
- Brouns, R.; Espinoza, A.V.; Goudman, L.; Moens, M.; Verlooy, J. Interventions to promote work participation after ischaemic stroke: A systematic review. Clin. Neurol. Neurosurg. 2019, 185, 105458. [Google Scholar] [CrossRef]
- Wei, X.; Liu, X.-F.; Fong, K. Outcomes of return-to-work after stroke rehabilitation: A systematic review. Br. J. Occup. Ther. 2016, 79, 299–308. [Google Scholar] [CrossRef]
- Ashley, K.D.; Lee, L.T.; Heaton, K. Return to Work Among Stroke Survivors. Work. Health Saf. 2019, 67, 87–94. [Google Scholar] [CrossRef]
- O’keefe, S.; Stanley, M.; Adam, K.; Lannin, N.A. A Systematic Scoping Review of Work Interventions for Hospitalised Adults with an Acquired Neurological Impairment. J. Occup. Rehabil. 2019, 29, 569–584. [Google Scholar] [CrossRef]
- Green, T.L.; McGovern, H.; Hinkle, J.L. Understanding Return to Work After Stroke Internationally: A Scoping Review. J. Neurosci. Nurs. 2021, 53, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Proffitt, R.; Boone, A.; Hunter, E.G.; Schaffer, O.; Strickland, M.; Wood, L.; Wolf, T.J. Interventions to Improve Social Participation, Work, and Leisure Among Adults Poststroke: A Systematic Review. Am. J. Occup. Ther. 2022, 76, 7605205120. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Lia, L.; Francavilla, F.; Chiappetta, M.; De Sio, S. Factors that facilitate and hinder the return to work after stroke: An overview of systematic reviews. Med. Lav. 2022, 113, e2022029. [Google Scholar] [CrossRef]
- Duong, P.; Sauvé-Schenk, K.; Egan, M.Y.; Meyer, M.J.; Morrison, T. Operational Definitions and Estimates of Return to Work Poststroke: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 100, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRIS-MA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of random-ised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.L. Description of a return-to-work occupational therapy programme for stroke rehabilitation in Singapore. Occupa-Tional Ther. Int. 2008, 15, 87–99. [Google Scholar] [CrossRef]
- Doucet, T.; Muller, F.; Verdun-Esquer, C.; Debelleix, X.; Brochard, P. Returning to work after a stroke: A retrospective study at the Physical and Re-habilitation Medicine Center La Tour de Gassies. Ann. Phys. Rehabil. Med. 2012, 55, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Mennemeyer, S.T.; Taub, E.; Uswatte, G.; Pearson, S. Employment in households with stroke after Constraint-Induced Movement therapy. Neurorehabilitation 2006, 21, 157–165. [Google Scholar] [CrossRef]
- Bin Zainal, M.N.; Wen, P.K.P.; Sien, N.Y.; Kee, K.M.; Chieh, K.J.; Asano, M. Supporting People with Stroke to Return to Work in Singapore: Findings from a Pilot Vocational Rehabilitation Program. Am. J. Occup. Ther. 2020, 74, 7406205040p1–7406205040p9. [Google Scholar] [CrossRef] [PubMed]
- Cain, S.; Churilov, L.; Collier, J.M.; Carvalho, L.B.; Borschmann, K.; Moodie, M.; Thijs, V.; Bernhardt, J. Factors associated with paid employment 12 months after stroke in A Very Early Rehabilitation Trial (AVERT). Ann. Phys. Rehabil. Med. 2022, 65, 101565. [Google Scholar] [CrossRef]
- Langhorne, P.; Wu, O.; Rodgers, H.; Ashburn, A.; Bernhardt, J. A Very Early Rehabilitation Trial after stroke (AVERT): A Phase III, multicentre, randomised controlled trial. Health Technol. Assess. 2017, 21, 1–120. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.; Radford, K.; Sinclair, E.; Walker, M. Return to Work after Stroke: Recording, Measuring, and Describing Occupational Therapy Intervention. Br. J. Occup. Ther. 2014, 77, 457–465. [Google Scholar] [CrossRef]
- Radford, K.; Grant, M.; Sinclair, E.; Kettlewell, J.; Watkin, C. Describing return to work after stroke: A feasibility trial of 12-month outcomes. J. Rehabil. Med. 2020, 52, jrm00048. [Google Scholar]
- Ntsiea, M.V.; van Aswegen, H.; Lord, S.; Olorunju S, S. The effect of a workplace intervention programme on return to work after stroke: A randomised controlled trial. Clin. Rehabil. 2014, 29, 663–673. [Google Scholar] [CrossRef]
- Hofgren, C.; Björkdahl, A.; Esbjörnsson, E.; Stibrant-Sunnerhagen, K. Recovery after stroke: Cognition, ADL- function and return to work. J. Neurol. Sci. 2009, 283, 316. [Google Scholar] [CrossRef]
- Langhammer, B.; Sunnerhagen, K.S.; Sällström, S.; Becker, F.; Stanghelle, J.K. Return to work after specialized rehabilitation-An explorative longitu-dinal study in a cohort of severely disabled persons with stroke in seven countries: The Sunnaas International Network stroke study. Brain Behav. 2018, 8, e01055. [Google Scholar] [CrossRef]
- Adams, R.A.; Sherer, M.; Struchen, M.A.; Nick, T.G. Post-acute brain injury rehabilitation for patients with stroke. Brain Inj. 2004, 18, 811–823. [Google Scholar] [CrossRef] [PubMed]
- Johansson, U.; Hellman, T.; Nilsson, A.; Eriksson, G. The ReWork-Stroke rehabilitation programme described by use of the TIDieR checklist. Scand. J. Occup. Ther. 2020, 28, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Johansson, U.; Ekbladh, E.; Bernspång, B.; Hellman, T.; Eriksson, G. Work Potential and Work Performance during the First Try-Out of the Person-Centred Return to Work Rehabilitation Programme ReWork-Stroke: A Case Study. Healthcare 2020, 8, 454. [Google Scholar] [CrossRef] [PubMed]
- Schow, T.; Harris, P.; Teasdale, T.W.; Rasmussen, M.A. Evaluation of a four month rehabilitation program for stroke patients with balance problems and binocular visual dysfunction. Neurorehabilitation 2016, 38, 331–341. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Country | Study Design | Sample Size | Sample Gender | Sample Age (Years) | Sample Education | n | Time Since Stroke Onset/Follow-Up Period Post-Stroke |
|---|---|---|---|---|---|---|---|---|
| Adams et al. [33] | USA | Pre-post-treatment observation study | 127 | 77 male, 50 female | Median: 48 25th percentile: 38 (IQR 38–54) 75th percentile: 54 | <High school diploma High school diploma or equivalent Some college College degree | 9 35 29 54 | 12 months |
| Bin Zainal et al. [25] | Singapore | Retrospective study | 50 | 37 male, 23 female | Median 44 (IQR 38–48) | Not reported | Not reported | |
| Chan [22] | Singapore | Retrospective study | 29 | Not reported | Not reported | Not reported | Not reported | |
| Doucet et al. [23] | France | Retrospective study | 56 | 35 male, 21 female | Mean 48.3 ± 10.1 | Junior high Vocational High school | 13 22 21 | ≥3 years |
| Grant et al. [28] Radford et al. [29] | UK | Feasibility RCT | 46 | 36 male, 10 female | Mean 58.3 ± 12.7 (intervention) Mean 53.8 ± 12.6 (control) | Not reported | 3, 6 and 12 months | |
| Hofgren et al. [31] | Sweden | Cohort study | 58 | 44 male, 14 female | Mean 52 ± 7.9 | Not reported | 1 year and 3 years | |
| Johansson et al. [34] Öst Nilsson [35] | Sweden | Pilot study | 10 | 6 male, 4 female | Mean 43.9 | Not reported | 3 months and 9 months | |
| Langhammer et al. [32] | Norway, China, USA, Russia, Palestine, Israel, Sweden | Exploratory longitudinal study | 230 | 154 male, 76 female | Mean 58.5 | 0–6 years of education 7–12 years of education 13+ years of education | 32 93 105 | 6 months and 12 months |
| Mennemeyer et al. [24] | USA | Retrospective study | 121 | 69 male, 52 female | Mean 65.75 | High school College or higher | 49 51 | 24 ± 16 months |
| Ntsiea et al. [30] | South Africa | RCT | 80 | 41 male, 39 female | Mean 45 ± 8.7 | Degree >Grade 12 Grade 12 Grade 11 <Grade 7 | 6 16 24 27 7 | 4.6 ± 1.8 weeks |
| Schow et al. [36] | Denmark | Pilot study | 29 | 16 male, 13 female | Mean 56.86 ± 7.5 | Not reported | Time since stroke 3–36 months. 6 month follow-up. |
| Internal Validity (13) | ||||||
|---|---|---|---|---|---|---|
| Study | Reporting (11) | External Validity (3) | Bias (7) | Confounding (6) | Power (5) | Total Score (32) |
| Adams et al. [33] | 7 | 3 | 4 | 4 | 0 | 18 |
| Bin Zainal, et al. [25] | 6 | 2 | 3 | 2 | 0 | 13 |
| Cain et al. [26] Langhorne et al. [27] | 5 | 3 | 5 | 4 | 0 | 17 |
| Chan [22] | 5 | 2 | 3 | 0 | 0 | 10 |
| Doucet et al. [23] | 7 | 1 | 4 | 4 | 0 | 16 |
| Grant et al. [28] Radford et al. [29] | 5 | 3 | 5 | 3 | 0 | 16 |
| Hofgren et al. [31] | 8 | 1 | 4 | 5 | 0 | 18 |
| Johansson et al. [34] Öst Nilsson [35] | 6 | 0 | 4 | 3 | 0 | 13 |
| Langhammer et al. [32] | 6 | 0 | 4 | 2 | 0 | 12 |
| Mennemeyer et al. [24] | 8 | 1 | 3 | 1 | 0 | 13 |
| Ntsiea et al. [30] | 0 | 2 | 3 | 4 | 0 | 19 |
| Schow et al. [36] | 4 | 2 | 2 | 1 | 0 | 9 |
| Study | Intervention Summary | Treatment Duration | Vocational Status, n (%) | |||
|---|---|---|---|---|---|---|
| Pre-Stroke | Admission | Discharge | Follow-Up | |||
| Adams et al. [33] | Mixture of group and individual therapy activities teaching compensatory strategies, arranging environmental supports, providing counselling and education. | Median: 113 days 25th percentile: 78 days 75th percentile: 163 days | 90 (100%) employed | Productive: 4 (4.4%) i. Competitive employment: 0 (0%) ii. Modified employment: 2 (2.2%) iii. Educational programme: 1(1.1%) iv. Homemaker: 0 (0%) v. Supported employment: 1 (1.1%) vi. Volunteer: 0 (0%) Non-productive: 86 (95.6%) | Productive: 73 (81.1%) i. Competitive employment: 33 (36.7%) ii. Modified employment: 15 (16.7%) iii. Educational programme: 2 (2.2%) iv. Homemaker: (2.2%) v. Supported employment: 2 (2.2%) vi. Volunteer: 19 (21.1%) Non-productive: 17 (18.9%) | Productive: 68 (75.6%) i. Competitive employment: 35 (38.9%) ii. Modified employment: 9 (10%) iii. Educational programme: 3 (3.3%) iv. Homemaker: 9 (10%) v. Supported employment: 0 (0%) vi. Volunteer: 12 (13.3%) Non-productive: 22 (24.4%) |
| Bin Zainal et al. [25] | Transition to employment (TTE) vocational rehabilitation programme. Individualised services including physical rehabilitation, psychosocial, employment, and caregiver support. Assessment of the home and work environments, assistive technology, work task simulation, job accommodations and modifications. | Median of 10 months. | Not reported | Not reported | 44 returned to work. 6 did not return to work | Not reported |
| Cain et al. [26] Langhorne et al. [27] | Very early mobilisation (AVERT) as an in-patient within 24 h assistance with functional tasks, sitting on edge of the bed, standing up, sitting out of bed and walking. | Not reported | 64% <65 years old were working before stroke. | Not reported | Not reported | 42% had returned to work at 3 months. Of those working at 3 months, 149 (90%) were still employed at 12 months. At 12 months, 221 (59%) had returned to work. |
| Chan [22] | Client interviewed by a work placement officer and assessed by OT, psychologist and social worker. Participation in job trials and job placements, upgrading skills course if necessary. | Not reported | Not reported | Not reported | Not reported | Employed: 16 (55%) i. Open employed: 10 (34%) ii. Sheltered workshop: 6 (21%) |
| Doucet et al. [23] | Patients attended a French Centre for Physical and Rehabilitation Medicine (CPRM) after a first stroke. Intervention not described. | 195.7 ± 162.5 days (median: 145.5 days) | 56 (100%) | Not reported | Not reported | 18 (32.1%) Of those who returned to work, 9 (50%) returned to the same work position, and 9 (50%) changed jobs. |
| Grant et al. [28] Radford et al. [29] | Individually tailored early vocational rehabilitation with an occupational therapist, involving work preparation, discussing work options, timing of the return to work and the hours they felt able to manage. Teaching pacing and fatigue management. Applying for voluntary work, visits to Job Centre Plus, and looking for education and retraining opportunities. Use of routines and timekeeping, patient contact with workplace, detailed job analysis, and identifying potential problems and solutions. Return to work process including planning, monitoring and grading, and maintenance. Work site visits. Confidence building, behavioural problems, dealing with others, and teaching relaxation techniques. Mobility training, driving assessment, using public transport. Memory and executive functioning training. Referral and consultation with specialist services. | Mean of 10 (SD 7, range 1–25) intervention sessions (approx. one hour per session). | Not reported | 2 in full-time education 7 were volunteering 69.6% of intervention group (16/23) and 73.9% of control group (17/23) were working full-time, and 1 (1/23; 4.3%) and 3 (3/23; 13%), respectively, were working part-time. Ten of intervention group (21%) were self-employed and working full-time baseline, six (6/23;26.1%) of control group were self-employed. | Not reported | 31; 67.4% returned to work at some point following stroke; 9 (19.6%) did not RTW during up to 12-month follow-up (intervention = 4; control = 5). (8/24) 52% who were employed full-time at stroke onset resumed full-time work at 12 months post-stroke. |
| Hofgren et al. [31] | Patients received 9 h of individually tailored training (from an OT and PT) per week for 3 weeks either at home or at the clinic after discharge from a rehabilitation ward. Focus on activities in their natural context, content including personal care, shopping and leisure. | 3 weeks | 55 (95%) (included 4 people who were unemployed at the time of stroke but looking for work classified as ‘employed’ by study definition). | Not reported | Not reported | 1 year: 4 (7%) 3 years: 11 (20%) |
| Johansson et al. [34] Öst Nilsson [35] | Preparation phase: resources and hindrances for RTW are mapped and a plan for work trial is made. Work trial phase: training at the workplace. Occupational therapist co-ordinates stakeholders and work visits. | 4.5–19 months | Not reported | Not reported | Not reported | At 9 months: 3 still working. 7 returned to paid employment to some extent. |
| Langhammer et al. [32] | Specialised rehabilitation for people whose needs are beyond the scope of local rehabilitation services. Intervention not described. | Mean: 49 days | 123 (53.4%) | Not reported | Not reported | 6 months: 36 (18%) 12 months: 37 (20%) |
| Mennemeyer et al. [24] | Constraint induced movement therapy. | Not specified. | 56 (48%) | 25 (22%) | Not reported | 29 (25%) |
| Ntsiea et al. [30] | Workplace intervention programme. | Not reported | 80 (100%) | Not reported | Not reported | At 3 months: Intervention: 27% Control: 2% 6 months: Intervention: 60% Control: 20% |
| Schow et al. [36] | Intensive balance and visual therapy in groups of six or seven, by physiotherapist and optometrist, and home exercises. | Four months | 24% in some sort of employment, 3.3% working full time. | At 6 months 60% in some form of employment and 27.6% working full time. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearce, G.; O’Donnell, J.; Pimentel, R.; Blake, E.; Mackenzie, L. Interventions to Facilitate Return to Work after Stroke: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 6469. https://doi.org/10.3390/ijerph20156469
Pearce G, O’Donnell J, Pimentel R, Blake E, Mackenzie L. Interventions to Facilitate Return to Work after Stroke: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(15):6469. https://doi.org/10.3390/ijerph20156469
Chicago/Turabian StylePearce, Gemma, Joan O’Donnell, Rebecca Pimentel, Elizabeth Blake, and Lynette Mackenzie. 2023. "Interventions to Facilitate Return to Work after Stroke: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 15: 6469. https://doi.org/10.3390/ijerph20156469
APA StylePearce, G., O’Donnell, J., Pimentel, R., Blake, E., & Mackenzie, L. (2023). Interventions to Facilitate Return to Work after Stroke: A Systematic Review. International Journal of Environmental Research and Public Health, 20(15), 6469. https://doi.org/10.3390/ijerph20156469