

Theoretical Derivation of a Telephone-Based Health Coaching Intervention for Promoting Physical Activity and Healthy Nutrition

Abstract
1. Introduction
2. Theoretical and Empirical Basis
2.1. Style of Interaction between Coaches and Patients
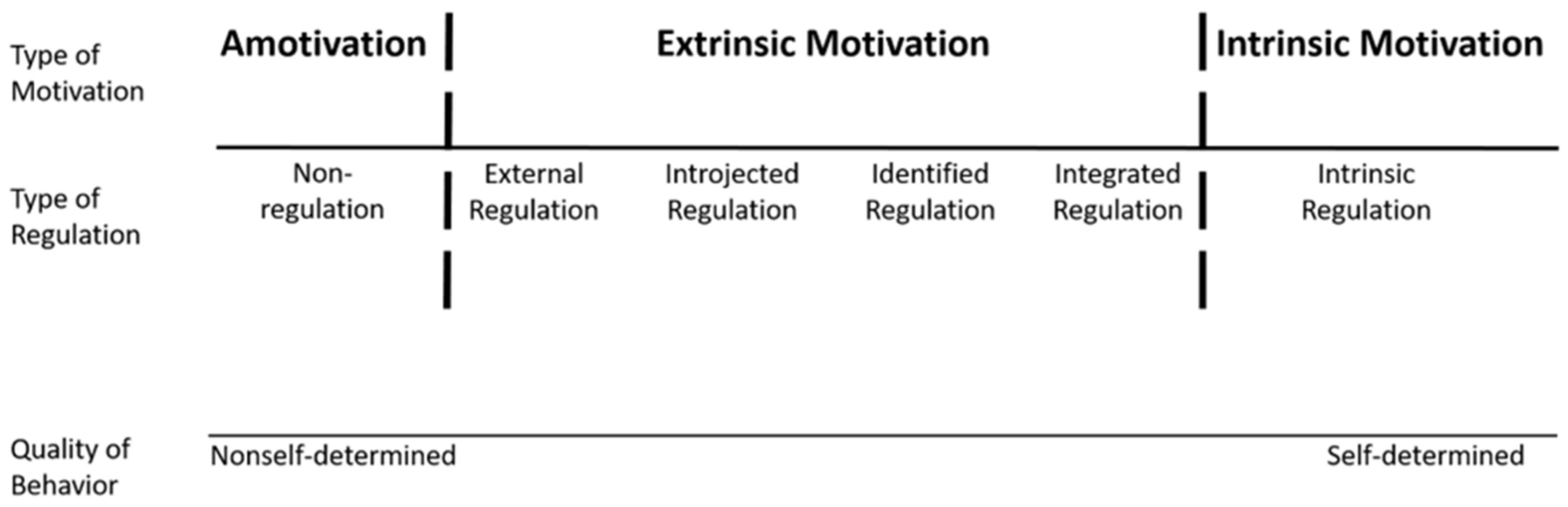
2.1.1. SDT
2.1.2. MI
2.2. The Contents of the Interaction
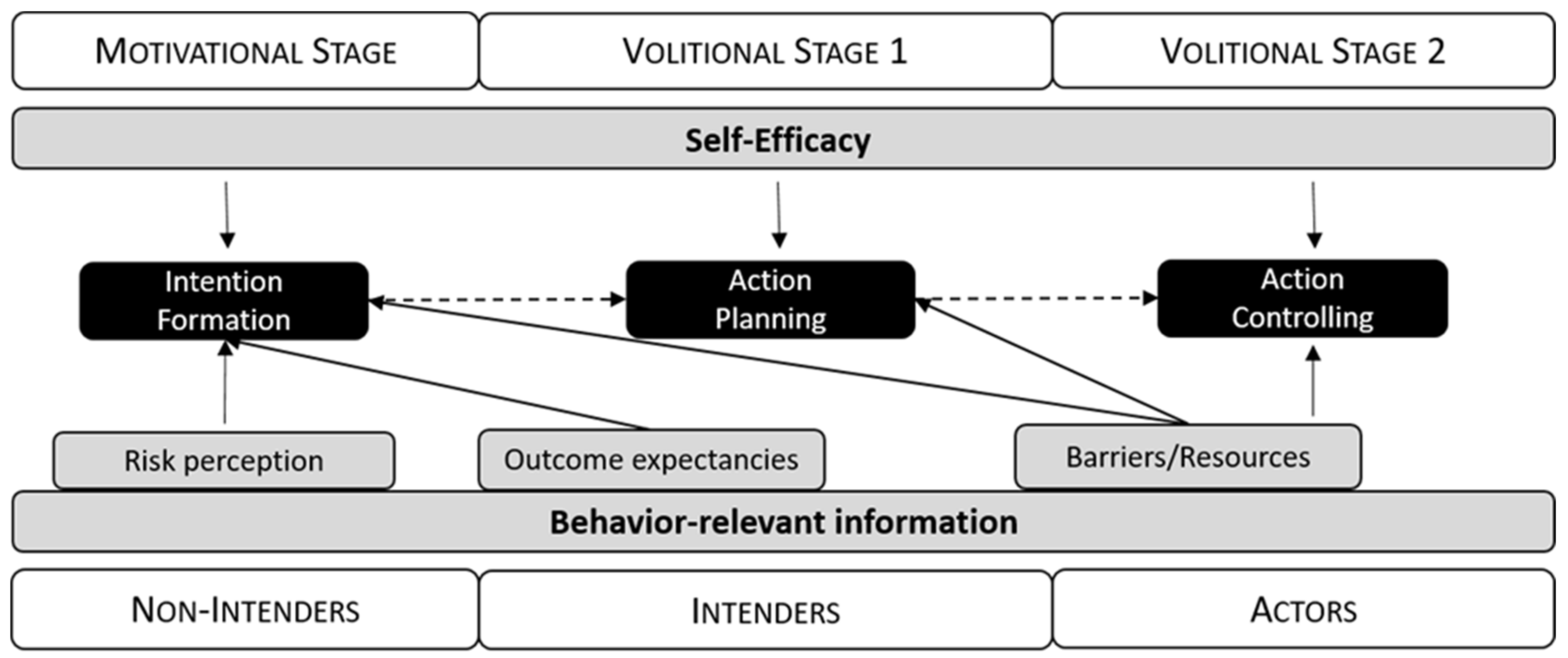
2.2.1. HAPA
- Non-intenders are especially affected by information about their health risks and about the risk-related outcomes of their current and any possible alternative behavior. They balance the positive and negative consequences of both kinds of behavior. The more the balance is in favor of the alternative behavior, the more likely non-intenders are to form an intention to perform that alternative behavior.
- Intenders concretize this intention into an internalized goal and try to develop concrete plans as to how and when to perform the intended behavior. The more they internalize their goal and succeed in developing plans of action, the more likely they are to initiate the behavior.
- Actors are especially susceptible to information regarding barriers that might impede and resources that might facilitate the behavior (e.g., daily routines). The fewer barriers and the more resources they see, the more likely they are to actually maintain the behavior or resume it after a relapse.
2.2.2. BCTs
3. Derivation of the Intervention
3.1. Core of the Intervention
3.1.1. Coaching Tools
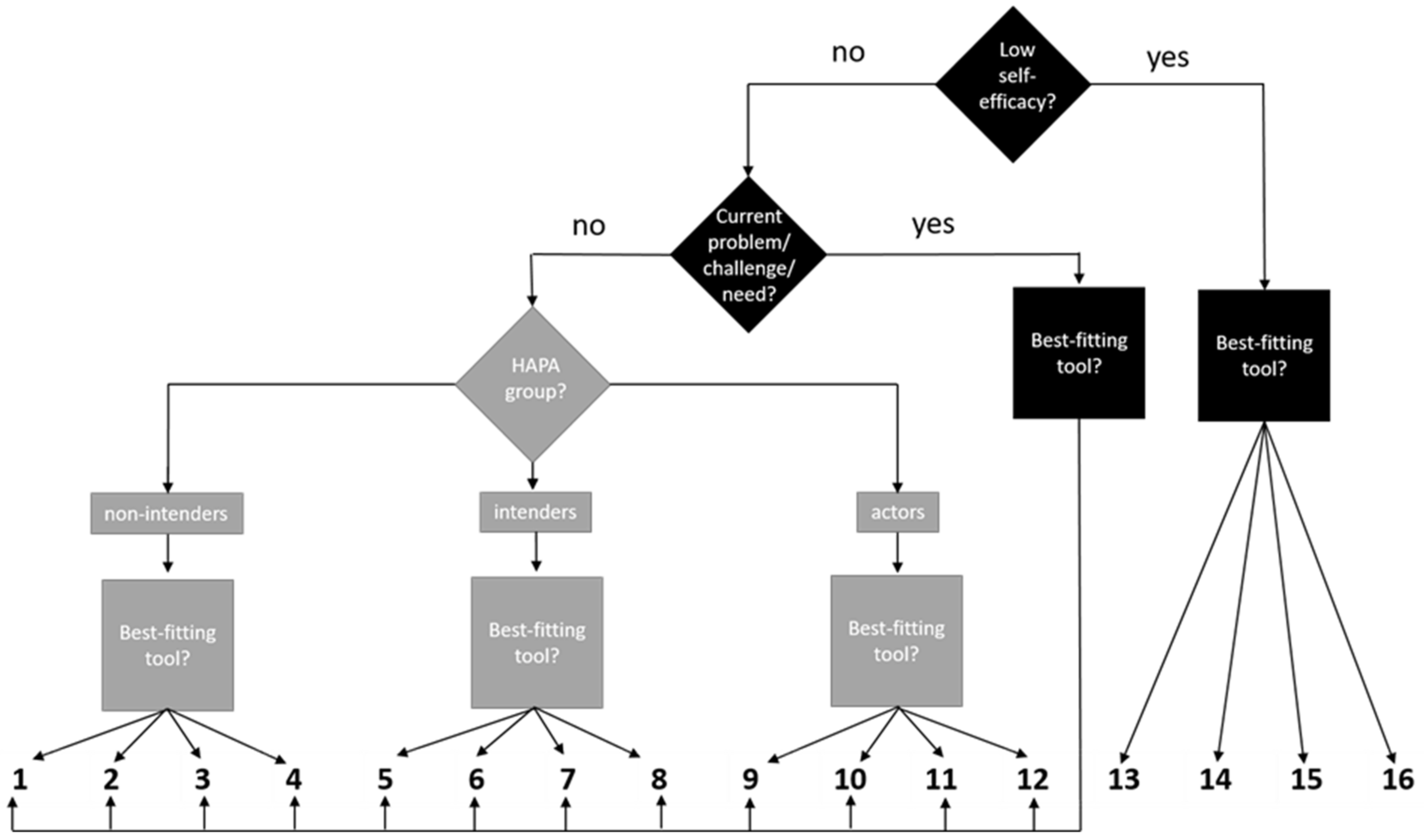
3.1.2. Selection of the Coaching Tools for the Individual Sessions
3.2. Measures to Ensure Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Study Preregistration Information
References
- Uusitupa, M.; Khan, T.A.; Viguiliouk, E.; Kahleova, H.; Rivellese, A.A.; Hermansen, K.; Pfeiffer, A.; Thanopoulou, A.; Salas-Salvadó, J.; Schwab, U.; et al. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2611. [Google Scholar] [CrossRef]
- Wang, D.D.; Hu, F.B. Precision nutrition for prevention and management of type 2 diabetes. Lancet Diabetes Endocrinol. 2018, 6, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Gronek, P.; Wielinski, D.; Cyganski, P.; Rynkiewicz, A.; Zając, A.; Maszczyk, A.; Gronek, J.; Podstawski, R.; Czarny, W.; Balko, S.; et al. A Review of Exercise as Medicine in Cardiovascular Disease: Pathology and Mechanism. Aging Dis. 2020, 11, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Brubaker, P.H.; Harber, M.P.; Lavie, C.J.; Myers, J.; Kaminsky, L.A. The Journal of Cardiopulmonary Rehabilitation and Prevention at 40 Years and Its Role in Promoting Lifestyle Medicine for Prevention of Cardiovascular Diseases: PART 1. J. Cardiopulm. Rehabil. Prev. 2020, 40, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.H.M.; van Berckel, B.N.M.; Scheltens, P.; Scherder, E.J.A.; van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef]
- Da Silva, H.R.; Nascimento, F.R.d.S.; Santos, S.L.d.; Lustosa, M.J.L.; Filho, J.C.L.C.d.M.; Portela, C.L.; Costa, R.H.F.; Junior, C.A.A.d.M.; Da Fernandes, L.K.S.; Neto, J.C.P. The importance of physical activity and healthy eating in cancer prophylaxis. Res. Soc. Dev. 2020, 9, e68942868. [Google Scholar] [CrossRef]
- Wang, L.; Ai, D.; Zhang, N. Exercise benefits coronary heart disease. In Exercise for Cardiovascular Disease Prevention and Treatment: From Molecular to Clinical, Part 2; Xiao, J., Ed.; Springer: Singapore, 2017; pp. 3–7. ISBN 978-981-10-4304-8. [Google Scholar]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Merellano-Navarro, E.; Gusi, N. Physical Exercise Improves Heart Rate Variability in Patients with Type 2 Diabetes: A Systematic Review. Curr. Diab Rep. 2017, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Thomas, C.J.; Tierney, A.C.; Kucianski, T.; George, E.S.; Ruiz-Canela, M.; Hebert, J.R.; Shivappa, N.; Itsiopoulos, C. Randomization to 6-month Mediterranean diet compared with a low-fat diet leads to improvement in Dietary Inflammatory Index scores in patients with coronary heart disease: The AUSMED Heart Trial. Nutr. Res. 2018, 55, 94–107. [Google Scholar] [CrossRef] [PubMed]
- Reimers, C.D.; Knapp, G.; Reimers, A.K. Does physical activity increase life expectancy? A review of the literature. J. Aging Res. 2012, 2012, 243958. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, P.; Ghimire, L. A review about the effect of life style modification on diabetes and quality of life. Glob. J. Health Sci. 2012, 4, 185–190. [Google Scholar] [CrossRef]
- United Nations. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases, New York. 2011. Available online: https://digitallibrary.un.org/record/710899/ (accessed on 20 October 2022).
- Konerding, U.; Szel, C. Promoting physical activity in persons with type 2 diabetes mellitus: A systematic review of systematic reviews. Patient Educ. Couns. 2021, 104, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Wolever, R.Q.; Simmons, L.A.; Sforzo, G.A.; Dill, D.; Kaye, M.; Bechard, E.M.; Southard, M.E.; Kennedy, M.; Vosloo, J.; Yang, N. A systematic review of the literature on health and wellness coaching: Defining a key behavioral intervention in healthcare. Glob. Adv. Health Med. 2013, 2, 38–57. [Google Scholar] [CrossRef]
- De Greef, K.; Deforche, B.; Tudor-Locke, C.; De Bourdeaudhuij, I. A cognitive-behavioural pedometer-based group intervention on physical activity and sedentary behaviour in individuals with type 2 diabetes. Health Educ. Res. 2010, 25, 724–736. [Google Scholar] [CrossRef] [PubMed]
- Kirk, A.; Mutrie, N.; MacIntyre, P.; Fisher, M. Effects of a 12-month physical activity counselling intervention on glycaemic control and on the status of cardiovascular risk factors in people with Type 2 diabetes. Diabetologia 2004, 47, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.R.; Buis, L.R.; Janney, A.W.; Goodrich, D.E.; Sen, A.; Hess, M.L.; Mehari, K.S.; Fortlage, L.A.; Resnick, P.J.; Zikmund-Fisher, B.J.; et al. An online community improves adherence in an internet-mediated walking program. Part 1: Results of a randomized controlled trial. J. Med. Internet Res. 2010, 12, e71. [Google Scholar] [CrossRef]
- Richardson, C.R.; Mehari, K.S.; McIntyre, L.G.; Janney, A.W.; Fortlage, L.A.; Sen, A.; Strecher, V.J.; Piette, J.D. A randomized trial comparing structured and lifestyle goals in an internet-mediated walking program for people with type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 59. [Google Scholar] [CrossRef] [PubMed]
- Kooiman, T.J.M.; de Groot, M.; Hoogenberg, K.; Krijnen, W.P.; van der Schans, C.P.; Kooy, A. Self-tracking of Physical Activity in People with Type 2 Diabetes: A Randomized Controlled Trial. Comput. Inform. Nurs. 2018, 36, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Poppe, L.; de Bourdeaudhuij, I.; Verloigne, M.; Shadid, S.; van Cauwenberg, J.; Compernolle, S.; Crombez, G. Efficacy of a Self-Regulation-Based Electronic and Mobile Health Intervention Targeting an Active Lifestyle in Adults Having Type 2 Diabetes and in Adults Aged 50 Years or Older: Two Randomized Controlled Trials. J. Med. Internet Res. 2019, 21, e13363. [Google Scholar] [CrossRef]
- Konerding, U.; Redaèlli, M.; Ackermann, K.; Altin, S.; Appelbaum, S.; Biallas, B.; Bödecker, A.-W.; Botzenhardt, S.; Chermette, C.; Cichocki, M.; et al. A pragmatic randomised controlled trial referring to a Personalised Self-management SUPport Programme (P-SUP) for persons enrolled in a disease management programme for type 2 diabetes mellitus and/or for coronary heart disease. Trials 2021, 22, 659. [Google Scholar] [CrossRef]
- Sand-Jecklin, K.; Coyle, S. Efficiently assessing patient health literacy: The BHLS instrument. Clin. Nurs. Res. 2014, 23, 581–600. [Google Scholar] [CrossRef] [PubMed]
- Brenk-Franz, K.; Hibbard, J.H.; Herrmann, W.J.; Freund, T.; Szecsenyi, J.; Djalali, S.; Steurer-Stey, C.; Sönnichsen, A.; Tiesler, F.; Storch, M.; et al. Validation of the German version of the patient activation measure 13 (PAM13-D) in an international multicentre study of primary care patients. PLoS ONE 2013, 8, e74786. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. (Eds.) Overview of Self-Determination Theory: An organismic dialectical perspective. In Handbook of Self-Determination Research; Rochester Press: Rochester, NY, USA, 2002; pp. 3–33. [Google Scholar]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change, 3rd ed.; The Guilford Press: New York, NY, USA; London, UK, 2013; ISBN 9781462507566. [Google Scholar]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational Interviewing and Self–Determination Theory. J. Soc. Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. (Eds.) Handbook of Self-Determination Research; Rochester Press: Rochester, NY, USA, 2002. [Google Scholar]
- Williams, G.C.; Rodin, G.C.; Ryan, R.M.; Grolnick, W.S.; Deci, E.L. Autonomous regulation and long-term medication adherence in adult outpatients. Health Psychol. 1998, 17, 269–276. [Google Scholar] [CrossRef]
- Williams, G.C.; Freedman, Z.R.; Deci, E.L. Supporting autonomy to motivate patients with diabetes for glucose control. Diabetes Care 1998, 21, 1644–1651. [Google Scholar] [CrossRef]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: Effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef]
- Sheeran, P.; Wright, C.E.; Avishai, A.; Villegas, M.E.; Lindemans, J.W.; Klein, W.M.P.; Rothman, A.J.; Miles, E.; Ntoumanis, N. Self-determination theory interventions for health behavior change: Meta-analysis and meta-analytic structural equation modeling of randomized controlled trials. J. Consult. Clin. Psychol. 2020, 88, 726–737. [Google Scholar] [CrossRef]
- Rogers, C.R. Client-Centered Therapy, Its Current Practice, Implications and Theory; Constable: London, UK, 1951; ISBN 1-84119-840-4. [Google Scholar]
- Ekong, G.; Kavookjian, J. Motivational interviewing and outcomes in adults with type 2 diabetes: A systematic review. Patient Educ. Couns. 2016, 99, 944–952. [Google Scholar] [CrossRef]
- O’Halloran, P.D.; Blackstock, F.; Shields, N.; Holland, A.; Iles, R.; Kingsley, M.; Bernhardt, J.; Lannin, N.; Morris, M.E.; Taylor, N.F. Motivational interviewing to increase physical activity in people with chronic health conditions: A systematic review and meta-analysis. Clin. Rehabil. 2014, 28, 1159–1171. [Google Scholar] [CrossRef]
- Söderlund, L.L.; Madson, M.B.; Rubak, S.; Nilsen, P. A systematic review of motivational interviewing training for general health care practitioners. Patient Educ. Couns. 2011, 84, 16–26. [Google Scholar] [CrossRef]
- Thompson, D.R.; Chair, S.Y.; Chan, S.W.; Astin, F.; Davidson, P.M.; Ski, C.F. Motivational interviewing: A useful approach to improving cardiovascular health? J. Clin. Nurs. 2011, 20, 1236–1244. [Google Scholar] [CrossRef]
- Thepwongsa, I.; Muthukumar, R.; Kessomboon, P. Motivational interviewing by general practitioners for Type 2 diabetes patients: A systematic review. Family Pract. 2017, 34, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R. Psychologie des Gesundheitsverhaltens: Einführung in Die Gesundheitspsychologie, 3rd ed.; Hogrefe: Göttingen, Germany, 2004; ISBN 3-8017-1816-6. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Lippke, S.; Luszczynska, A. Mechanisms of health behavior change in persons with chronic illness or disability: The Health Action Process Approach (HAPA). Rehabil. Psychol. 2011, 56, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Carey, R.N.; Connell, L.E.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Michie, S. Behavior Change Techniques and Their Mechanisms of Action: A Synthesis of Links Described in Published Intervention Literature. Ann. Behav. Med. 2019, 53, 693–707. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Bandura, A. Self-Efficacy: The Exercise of Control, 2nd ed.; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Zhang, C.-Q.; Zhang, R.; Schwarzer, R.; Hagger, M.S. A meta-analysis of the health action process approach. Health Psychol. 2019, 38, 623–637. [Google Scholar] [CrossRef]
- Lippke, S.; Schwarzer, R.; Ziegelmann, J.P.; Scholz, U.; Schüz, B. Testing stage-specific effects of a stage-matched intervention: A randomized controlled trial targeting physical exercise and its predictors. Health Educ. Behav. 2010, 37, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the intention–behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef]
- Steca, P.; Pancani, L.; Greco, A.; D’Addario, M.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Cesana, F.; et al. Changes in dietary behavior among coronary and hypertensive patients: A longitudinal investigation using the health action process approach. Appl. Psychol. Health Well-Being 2015, 7, 316–339. [Google Scholar] [CrossRef] [PubMed]
- Avery, L.; Flynn, D.; Dombrowski, S.U.; van Wersch, A.; Sniehotta, F.F.; Trenell, M.I. Successful behavioural strategies to increase physical activity and improve glucose control in adults with Type 2 diabetes. Diabet. Med. 2015, 32, 1058–1062. [Google Scholar] [CrossRef] [PubMed]
- Van Rhoon, L.; Byrne, M.; Morrissey, E.; Murphy, J.; McSharry, J. A systematic review of the behaviour change techniques and digital features in technology-driven type 2 diabetes prevention interventions. Digit. Health 2020, 6, 2055207620914427. [Google Scholar] [CrossRef]
- Cradock, K.A.; ÓLaighin, G.; Finucane, F.M.; McKay, R.; Quinlan, L.R.; Martin Ginis, K.A.; Gainforth, H.L. Diet behavior change techniques in type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2017, 40, 1800–1810. [Google Scholar] [CrossRef]
- Obino, K.F.M.; Pereira, C.A.; Caron-Lienert, R.S. Coaching and barriers to weight loss: An integrative review. Diabetes Metab. Syndr. Obes. 2017, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Neuhausen, A.; Gawlik, A.; Nacak, Y.; Hamm, I.; Funke, C.; Giesen, L.; Vitinius, F. Evaluation of a Telephone Coaching Training Using a Mixed Method Approach; Department of Psychosomatics and Psychotherapy, Faculty of Medicine, University Hospital Cologne, University of Cologne: Cologne, Germany, 2023; to be submitted. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Coaching Tool Name and Goal | Behavior Change Technique (BCT) | |
|---|---|---|---|
| Coaching Tools for Non-intender | 1 | Activity check Patients increase their awareness of their current level of physical activity, in terms of risk perception. Patients form an intention to become more active and, thus, undertake more for their own health. | Feedback on behavior |
| 2 | My activity type Patients create an activity profile in order to typify, summarize, and, subsequently, reflect on their own ideas about physical activity. | Instruction on how to perform the behavior | |
| 3 | Decision balance Patients identify and increase their awareness of both the positive consequences of health behavior change and the negative consequences of continuing with their current behavior. | Pros and cons | |
| 4 | My health motivation Patients identify their own level of self-determination in terms of physical activity/healthy nutrition and develop ways in which they can strive for a more autonomous form of regulation. | Feedback on behavior | |
| Coaching Tools for Intender | 5 | My health plan Patients translate their goals into precise action plans by independently concretizing the “what, when, where, and, possibly, with whom?” of their health plan. | Action planning |
| 6 | My health diary Patients document their physical activity/healthy nutrition and the positive consequences and feelings during and after; they are, thus, made aware of the connection between greater physical activity/healthier nutrition and their mood. | Self-monitoring of behavior | |
| 7 | My health goal Patients use the SMART method tool to set a clear, unambiguous, and self-concordant goal. | Goal setting | |
| 8 | Visualization of my health goal Patients use visualization techniques to help themselves to further internalize their previously defined goal by “imagining” the achievement of their goal. | Goal setting | |
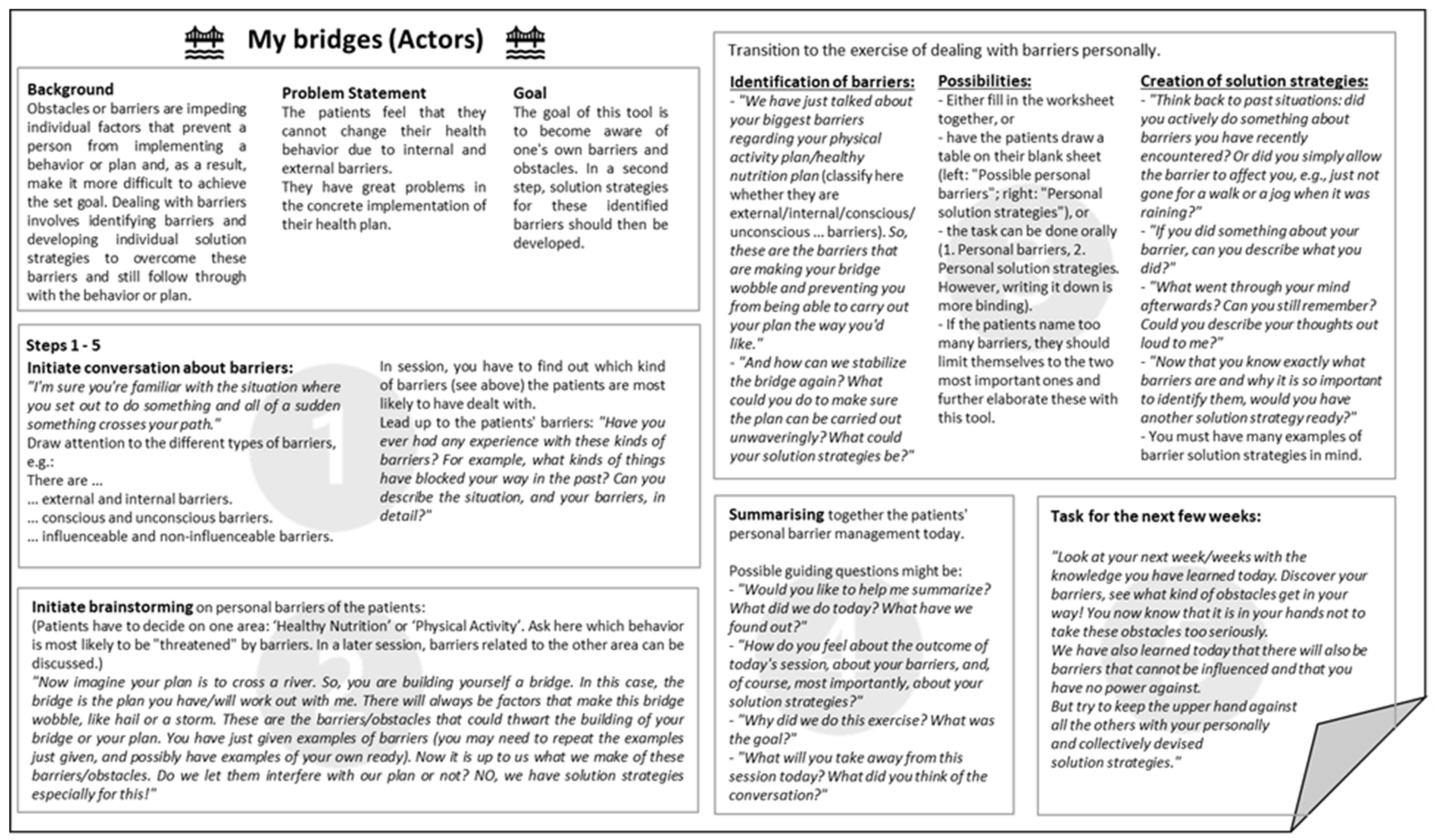
| Coaching Tools for Actors | 9 | My bridges Patients become aware of their own internal and external barriers and develop appropriate solution strategies for the barriers they identify. | Problem-solving |
| 10 | My health routine Patients develop a routine in their desired area (healthy nutrition/physical activity) that fits their wants/needs/everyday life and that they can integrate long-term into their daily routine. | Habit formation | |
| 11 | Self-reflection (scheduled for the 11th coaching session) Patients revisit and reflect on the greatest challenge to their behavior change that they have faced so far during the coaching process, to prepare for everyday life without the coach. | Focus on past success | |
| 12 | My future self-management (scheduled for the 12th coaching session) Patients review and consolidate the proven coaching tools and practical techniques they have learned and developed for their own health behavior change, to underline the importance of future planning in preparation for everyday life without the coach. | Action planning |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawlik, A.; Nacak, Y.; Kleinert, J.; Konerding, U.; Vitinius, F. Theoretical Derivation of a Telephone-Based Health Coaching Intervention for Promoting Physical Activity and Healthy Nutrition. Int. J. Environ. Res. Public Health 2023, 20, 6271. https://doi.org/10.3390/ijerph20136271
Gawlik A, Nacak Y, Kleinert J, Konerding U, Vitinius F. Theoretical Derivation of a Telephone-Based Health Coaching Intervention for Promoting Physical Activity and Healthy Nutrition. International Journal of Environmental Research and Public Health. 2023; 20(13):6271. https://doi.org/10.3390/ijerph20136271
Chicago/Turabian StyleGawlik, Angeli, Yeliz Nacak, Jens Kleinert, Uwe Konerding, and Frank Vitinius. 2023. "Theoretical Derivation of a Telephone-Based Health Coaching Intervention for Promoting Physical Activity and Healthy Nutrition" International Journal of Environmental Research and Public Health 20, no. 13: 6271. https://doi.org/10.3390/ijerph20136271
APA StyleGawlik, A., Nacak, Y., Kleinert, J., Konerding, U., & Vitinius, F. (2023). Theoretical Derivation of a Telephone-Based Health Coaching Intervention for Promoting Physical Activity and Healthy Nutrition. International Journal of Environmental Research and Public Health, 20(13), 6271. https://doi.org/10.3390/ijerph20136271