
Parents of Adolescents Who Experience Suicidal Phenomena—A Scoping Review of Their Experience

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search Strategy
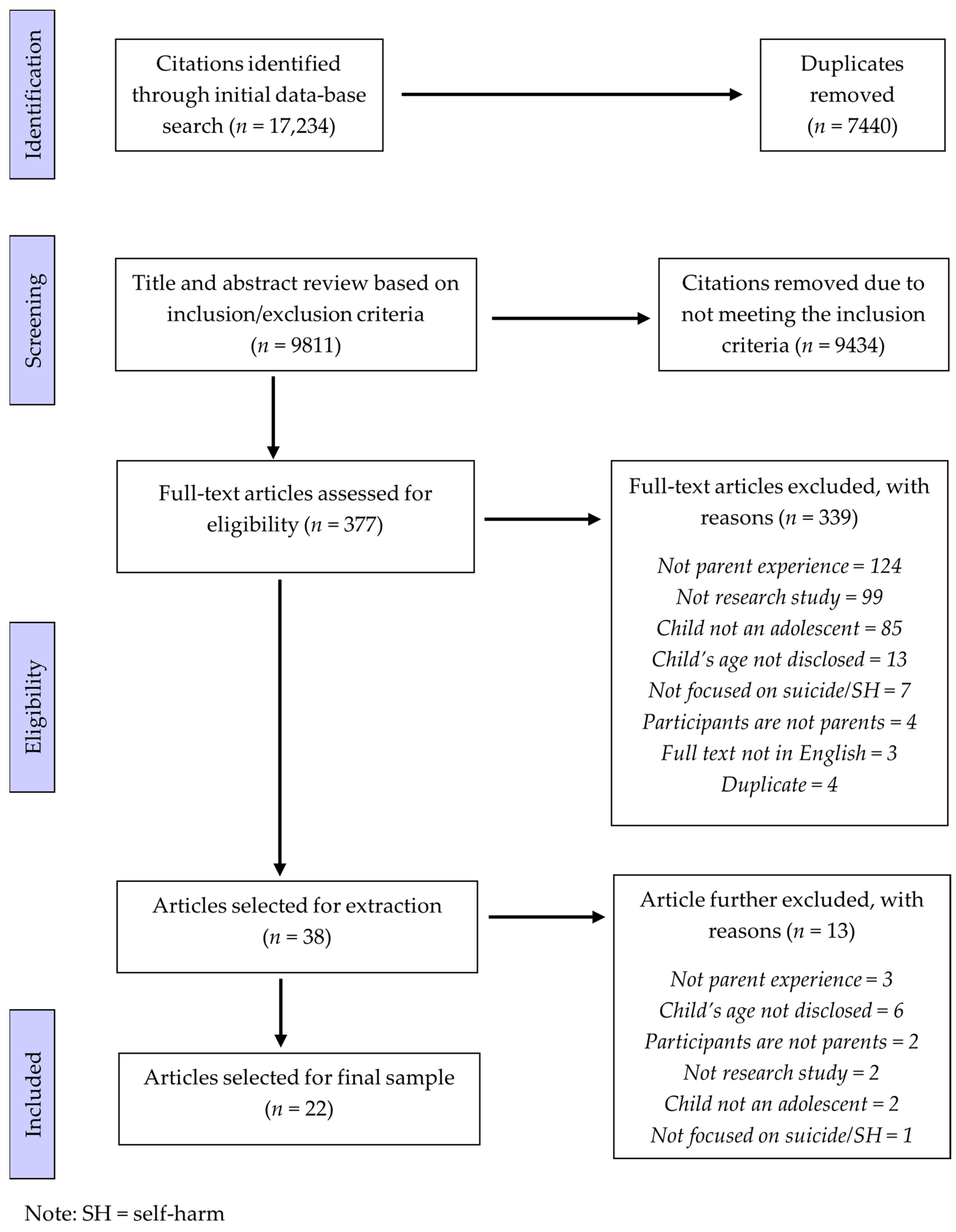
2.3. Screening
2.4. Data Charting
- Descriptive information about the study: authors, title of publication, year of publication, country of origin, if the study was qualitative/quantitative/mixed methods, study aim, study design, focusing on suicide or self-harm (intent not disclosed) or NSSI, recruitment setting, age of child, child gender characteristics, participant population, sample size, gender proportions, and data source.
- Study details: Key findings, data collection method, sample details, analysis approach, findings in relation to parent’s experience, parent mental health, relationship with suicidal child, relationship with other immediate family, experiences of the child’s mental health, perceived reasons for adolescents’ suicide crisis/NSSI, managing suicidal crisis/NSSI behaviour, logistics of child’s care, and changes to lifestyle.
2.5. Data Summary and Synthesis
3. Results
3.1. Discovery of Suicidal Phenomena
3.1.1. Unsure How to Respond
3.1.2. Emotional Response
3.2. During the Management of Suicidal Phenomena
3.2.1. Parent Wellbeing
3.2.2. Help-Seeking for Child
3.2.3. Parent and Child (Dis)connection
3.2.4. Poor Access to Support for Parents
3.2.5. Changes in Parent Behaviour and Impact on Family
3.2.6. Making Sense of the Suicidal Phenomena
3.3. After the Suicidal Phenomena Ceased
3.3.1. Changes in Parent–Child Relationship
3.3.2. Support for Parents
4. Discussion
4.1. Limitations of the Papers Reviewed
4.2. Limitations of This Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy EMBASE

{kind=link}
| Search | Search Content |
|---|---|
| 1 | exp suicidal behavior/ |
| 2 | (Suicid * adj4 (crisis or attempt * or behavio * or ideation or experience * or distress or death *)).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
| 3 | automutilation/ |
| 4 | (self harm or non-suicidal self injury or self-inflicted injury).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
| 5 | 1 or 2 or 3 or 4 |
| 6 | exp child parent relation/ |
| 7 | exp parent/ |
| 8 | parental behavior/ |
| 9 | (parent * or mother * or father * or caregiver * or guardian * or legal guardian *).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
| 10 | legal guardian/ |
| 11 | 6 or 7 or 8 or 9 or 10 |
| 12 | adolescent/ |
| 13 | (Youth * or Adolescent * or Teenager * or Young adult * or child * or young people * or young person * or emerging adult *).mp. [mp = title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] |
| 14 | 12 or 13 |
| 15 | 5 and 11 and 14 |
| 16 | limit 15 to English |
References
- Australian Institute of Health and Welfare. Deaths in Australia; AIHW: Canberra, Australia, 2022. Available online: https://www.aihw.gov.au/reports/life-expectancy-death/deaths-in-australia (accessed on 6 April 2023).
- Australian Institute of Health and Welfare. Suicide & Self-Harm Monitoring; AIHW: Canberra, Australia, 2022. Available online: https://www.aihw.gov.au/suicide-self-harm-monitoring/data/suicide-self-harm-monitoring-data (accessed on 6 April 2023).
- Martínez-Alés, G.; Pamplin, J.R.; Rutherford, C.; Gimbrone, C.; Kandula, S.; Olfson, M.; Gould, M.S.; Shaman, J.; Keyes, K.M. Age, period, and cohort effects on suicide death in the United States from 1999 to 2018: Moderation by sex, race, and firearm involvement. Mol. Psychiatry 2021, 26, 3374–3382. [Google Scholar] [CrossRef]
- Plener, P.L.; Schumacher, T.S.; Munz, L.M.; Groschwitz, R.C. The longitudinal course of non-suicidal self-injury and deliberate self-harm: A systematic review of the literature. Bord. Personal. Disord. Emot. Dysregul. 2015, 2, 2. [Google Scholar] [CrossRef]
- Zubrick, S.R.; Hafekost, J.; Johnson, S.E.; Lawrence, D.; Saw, S.; Sawyer, M.; Ainley, J.; Buckingham, W.J. Self-harm: Prevalence estimates from the second Australian child and adolescent survey of mental health and wellbeing. Aust. N. Z. J. Psychiatry 2016, 50, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Zubrick, S.R.; Hafekost, J.; Johnson, S.E.; Lawrence, D.; Saw, S.; Sawyer, M.; Ainley, J.; Buckingham, W.J. Suicidal behaviours: Prevalence estimates from the second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Aust. N. Z. J. Psychiatry 2016, 50, 899–910. [Google Scholar] [CrossRef]
- Van Vuuren, C.L.; Van Der Wal, M.F.; Cuijpers, P.; Chinapaw, M.J.M. Are suicidal thoughts and behaviors a temporary phenomenon in early adolescence? Crisis 2020, 42, 78–81. [Google Scholar] [CrossRef]
- Olfson, M.; Wall, M.; Wang, S.; Crystal, S.; Bridge, J.A.; Liu, S.-M.; Blanco, C. Suicide after deliberate self-harm in adolescents and young adults. Pediatrics 2018, 141, e20173517. [Google Scholar] [CrossRef] [PubMed]
- Boyd, D.T.; Quinn, C.R.; Jones, K.V.; Beer, O.W. Suicidal ideations and attempts within the family context: The role of parent support, bonding, and peer experiences with suicidal behaviors. J. Racial Ethn. Health Disparities 2022, 9, 1740–1749. [Google Scholar] [CrossRef] [PubMed]
- Clarke, S.; Allerhand, L.A.; Berk, M.S. Recent advances in understanding and managing self-harm in adolescents. F1000Research 2019, 8, 1794. [Google Scholar] [CrossRef] [PubMed]
- Duarte, E.; Gouveia-Pereira, M.; Gomes, H.S.; Sampaio, D. How do families represent the functions of deliberate self-harm? A comparison between the social representations from adolescents and their parents. Arch. Suicide Res. 2020, 24 (Suppl. S1), 173–189. [Google Scholar] [CrossRef] [PubMed]
- Demuthova, S.; Vaclavikova, I.; Selecka, L.; Blatny, M. The Problem of Self-Disclosure of Self-Harming Behaviour in Adolescence. Postmod. Open. 2020, 11, 1–19. [Google Scholar] [CrossRef]
- Pan, C.-H.; Lee, M.-B.; Wu, C.-Y.; Liao, S.-C.; Chan, C.-T.; Chen, C.-Y. Suicidal ideation, psychopathology, and help-seeking in 15 to 19-year-old adolescents in Taiwan: A population-based study 2015–2019. J. Affect. Disord. 2021, 282, 846–851. [Google Scholar] [CrossRef]
- Arbuthnott, A.E.; Lewis, S.P. Parents of youth who self-injure: A review of the literature and implications for mental health professionals. Child Adolesc. Psychiatry Ment. Health 2015, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Simes, D.; Shochet, I.; Murray, K.; Sands, I.G. A systematic review of qualitative research of the experiences of young people and their caregivers affected by suicidality and self-harm: Implications for family-based treatment. Adolesc. Res. Rev. 2022, 7, 211–233. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Evans, E.; Hawton, K.; Rodham, K.; Deeks, J. The prevalence of suicidal phenomena in adolescents: A systematic review of population-based studies. Suicide Life-Threat. Behav. 2005, 35, 239–250. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Baetens, I.; Claes, L.; Onghena, P.; Grietens, H.; Van Leeuwen, K.; Pieters, C.; Wiersema, J.R.; Griffith, J.W. The effects of nonsuicidal self-injury on parenting behaviors: A longitudinal analyses of the perspective of the parent. Child Adolesc. Psychiatry Ment. Health 2015, 9, 24. [Google Scholar] [CrossRef]
- Berk, M.S.; Rathus, J.; Kessler, M.; Clarke, S.; Chick, C.; Shen, H.; Llewellyn, T. Pilot test of a DBT-based parenting intervention for parents of youth with recent self-harm. Cogn. Behav. Pract. 2022, 29, 348–366. [Google Scholar] [CrossRef]
- Czyz, E.K.; Horwitz, A.G.; Yeguez, C.E.; Ewell Foster, C.J.; King, C.A. Parental self-efficacy to support teens during a suicidal crisis and future adolescent emergency department visits and suicide attempts. J. Clin. Child Adolesc. Psychol. 2018, 47 (Suppl. S1), S384–S396. [Google Scholar] [CrossRef] [PubMed]
- Daly, P. Mothers living with suicidal adolescents: A phenomenological study of their experiences. J. Psychosoc. Nurs. Ment. Health Serv. 2005, 43, 22–28. [Google Scholar]
- de Miranda Trinco, M.E.; Santos, J.C.; Barbosa, A. Experiences and needs of parents of adolescentes with self-harm behaviors during hospitalization. Rev. Enferm. Ref. 2017, 4, 115–124. [Google Scholar] [CrossRef]
- Ewell Foster, C.; Magness, C.; Czyz, E.; Kahsay, E.; Martindale, J.; Hong, V.; Baker, E.; Cavataio, I.; Colombini, G.; Kettley, J. Predictors of parent behavioral engagement in youth suicide discharge recommendations: Implications for family-centered crisis interventions. Child Psychiatry Hum. Dev. 2022, 53, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.; Yang, J.; Liao, X.; Lin, J.; Peng, Y.; Shen, Y.; Ou, J.; Li, Y.; Chen, R. Parents’ attitudes toward and experience of non-suicidal self-injury in adolescents: A qualitative study. Front. Psychiatry 2020, 11, 651. [Google Scholar] [CrossRef]
- Fu, X.; Yang, J.; Liao, X.; Shen, Y.; Ou, J.; Li, Y.; Chen, R. Parents’ and medical staff’s experience of adolescents with suicide-related behaviors admitted to a general hospital in China: Qualitative study. BMC Psychiatry 2021, 21, 62. [Google Scholar] [CrossRef]
- Gillespie, C.; Joyce, M.; Flynn, D.; Corcoran, P. Dialectical behaviour therapy for adolescents: A comparison of 16-week and 24-week programmes delivered in a public community setting. Child Adolesc. Ment. Health 2019, 24, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.A.; Puzia, M.E.; Godfrey, D.A.; Crowell, S.E. Physiological and behavioral effects of interpersonal validation: A multilevel approach to examining a core intervention strategy among self-injuring adolescents and their mothers. J. Clin. Psychol. 2020, 76, 559–580. [Google Scholar] [CrossRef]
- Kawabe, K.; Horiuchi, F.; Ochi, M.; Oka, Y.; Ueno, S.-I. Suicidal ideation in adolescents and their caregivers: A cross sectional survey in Japan. BMC Psychiatry 2016, 16, 231. [Google Scholar] [CrossRef]
- Kelada, L.; Whitlock, J.; Hasking, P.; Melvin, G. Parents’ experiences of nonsuicidal self-injury among adolescents and young adults. J. Child Fam. Stud. 2016, 25, 3403–3416. [Google Scholar] [CrossRef]
- Kelada, L.; Hasking, P.; Melvin, G.A. School response to self-injury: Concerns of mental health staff and parents. Sch. Psychol. Q. 2017, 32, 173–187. [Google Scholar] [CrossRef]
- McKay, K.; Shand, F. Child-Sized Gaps in the System: Case Studies of Child Suicidality and Support within the Australian Healthcare System. Educ. Dev. Psychol. 2016, 33, 139–148. [Google Scholar] [CrossRef]
- Miers, D.; Abbott, D.; Springer, P.R. A phenomenological study of family needs following the suicide of a teenager. Death Stud. 2012, 36, 118–133. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.H.M.; Wyman Battalen, A.; Sellers, C.M.; Spirito, A.; Yen, S.; Maneta, E.; Ryan, C.A.; Braciszewski, J.M. An mHealth approach to extend a brief intervention for adolescent alcohol use and suicidal behavior: Qualitative analyses of adolescent and parent feedback. J. Technol. Hum. Serv. 2019, 37, 255–285. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, J.L.; Gulbas, L.E.; Suarez Bonilla, G.; Manzo, G.; Piña-Watson, B.; Zayas, L.H. Father-daughter relationships among latina adolescents who attempted suicide: An exploratory dyadic analysis. Fam. Process 2022, 61, 890–905. [Google Scholar] [CrossRef]
- Oldershaw, A.; Richards, C.; Simic, M.; Schmidt, U. Parents’ perspectives on adolescent self-harm: Qualitative study. Br. J. Psychiatry 2008, 193, 140–144. [Google Scholar] [CrossRef]
- Townsend, M.L.; Miller, C.E.; Matthews, E.L.; Grenyer, B.F. Parental response style to adolescent self-harm: Psychological, social and functional impacts. Int. J. Environ. Res. Public Health 2021, 18, 13407. [Google Scholar] [CrossRef] [PubMed]
- Wagner, B.M.; Aiken, C.; Mullaley, P.M.; Tobin, J.J. Parents’ reactions to adolescents’ suicide attempts. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Huang, X.; Huang, X.; Zhao, W. Parents’ lived experience of adolescents’ repeated non-suicidal self-injury in China: A qualitative study. BMC Psychiatry 2022, 22, 70. [Google Scholar] [CrossRef] [PubMed]
- Ye, M.; Hu, Y.; Xue, Q.; Liang, A.; Lu, Z. Understanding and change–Parents’ perspectives of their self-poisoning children: A phenomenological study. Int. Emerg. Nurs. 2021, 59, 101074. [Google Scholar] [CrossRef]
- Scott, A.J.; Webb, T.L.; Martyn-St James, M.; Rowse, G.; Weich, S. Improving sleep quality leads to better mental health: A meta-analysis of randomised controlled trials. Sleep Med. Rev. 2021, 60, 101556. [Google Scholar] [CrossRef]
- Corscadden, L.; Callander, E.J.; Topp, S.M. Who experiences unmet need for mental health services and what other barriers to accessing health care do they face? Findings from Australia and Canada. Int. J. Health Plan. Manag. 2019, 34, 761–772. [Google Scholar] [CrossRef]
- Tristiana, R.D.; Yusuf, A.; Fitryasari, R.; Wahyuni, S.D.; Nihayati, H.E. Perceived barriers on mental health services by the family of patients with mental illness. Int. J. Nurs. Sci. 2018, 5, 63–67. [Google Scholar] [CrossRef]
- Harandi, T.F.; Taghinasab, M.M.; Nayeri, T.D. The correlation of social support with mental health: A meta-analysis. Electron. Physician 2017, 9, 5212. [Google Scholar] [CrossRef]
- Weick, K.E. Making Sense of the Organization; Blackwell: Oxford, UK, 2001. [Google Scholar]
- Hughes, N.D.; Locock, L.; Simkin, S.; Stewart, A.; Ferrey, A.E.; Gunnell, D.; Kapur, N.; Hawton, K. Making sense of an unknown terrain: How parents understand self-harm in young people. Qual. Health Res. 2017, 27, 215–225. [Google Scholar] [CrossRef]
- Krysinska, K.; Curtis, S.; Lamblin, M.; Stefanac, N.; Gibson, K.; Byrne, S.; Thorn, P.; Rice, S.M.; McRoberts, A.; Ferrey, A. Parents’ experience and psychoeducation needs when supporting a young person who self-harms. Int. J. Environ. Res. Public Health 2020, 17, 3662. [Google Scholar] [CrossRef]
- Kirk, S.; Fallon, D.; Fraser, C.; Robinson, G.; Vassallo, G. Supporting parents following childhood traumatic brain injury: A qualitative study to examine information and emotional support needs across key care transitions. Child Care Health Dev. 2015, 41, 303–313. [Google Scholar] [CrossRef]
- Schlichthorst, M.; Ozols, I.; Reifels, L.; Morgan, A. Lived experience peer support programs for suicide prevention: A systematic scoping review. Int. J. Ment. Health Syst. 2020, 14, 65. [Google Scholar] [CrossRef]
- Wainwright, V.; Cordingley, L.; Chew-Graham, C.A.; Kapur, N.; Shaw, J.; Smith, S.; McGale, B.; McDonnell, S. Experiences of support from primary care and perceived needs of parents bereaved by suicide: A qualitative study. Br. J. Gen. Pract. 2020, 70, e102–e110. [Google Scholar] [CrossRef]
- Foggin, E.; McDonnell, S.; Cordingley, L.; Kapur, N.; Shaw, J.; Chew-Graham, C.A. GPs’ experiences of dealing with parents bereaved by suicide: A qualitative study. Br. J. Gen. Pract. 2016, 66, e737–e746. [Google Scholar] [CrossRef]
- Endo, K.; Yonemoto, N.; Yamada, M. Interventions for bereaved parents following a child’s death: A systematic review. Palliat. Med. 2015, 29, 590–604. [Google Scholar] [CrossRef]
- Stevenson, M.; Achille, M.; Liben, S.; Proulx, M.-C.; Humbert, N.; Petti, A.; Macdonald, M.E.; Cohen, S.R. Understanding how bereaved parents cope with their grief to inform the services provided to them. Qual. Health Res. 2017, 27, 649–664. [Google Scholar] [CrossRef]
- King, C.A.; Kerr, D.C.; Passarelli, M.N.; Foster, C.E.; Merchant, C.R. One-year follow-up of suicidal adolescents: Parental history of mental health problems and time to post-hospitalization attempt. J. Youth Adolesc. 2010, 39, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Geulayov, G.; Metcalfe, C.; Heron, J.; Kidger, J.; Gunnell, D. Parental suicide attempt and offspring self-harm and suicidal thoughts: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC) birth cohort. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 509–517.e2. [Google Scholar] [PubMed]

| Authors and Year | Country | S/NSSI/SH | Participants | Adolescent Demographics | Data Source | Recruitment Method | Temporal Theme/s |
|---|---|---|---|---|---|---|---|
| Baetens et al. (2015) [19] | Belgium | NSSI | 1438 parents (88.7% female) * | 12 years old, 54.7% female | Self-report surveys | Not reported | During management |
| Berk et al. (2022) [20] | USA | Suicide attempt and NSSI | 12 parents (75% female) Age 45–56 (mean age 49.4 years) | 13–17-year-olds (mean age 14.7 years), 70% female | Self-report surveys and structured interviews | Recruited through psychiatric clinic | Discovery, During management |
| Czyz et al. (2018) [21] | USA | Suicide | 162 parents (79.6% female) | 13–17 years (mean age = 15.41 years), 57% female | Self-report surveys | Recruited though psychiatric emergency department services | During management |
| Daly (2005) [22] | Canada | Suicide | 6 parents (100% female) Age range = 32–45 years | 12–16 years | Unstructured interviews | Outpatient family therapy provider | During management, After |
| de Miranda Trinco et al. (2017) [23] | Portugal | NSSI | 38 parents (89% female) | 13–18 years | Semi-structured interviews | Emergency department in a paediatric hospital | Discovery, During management |
| Ewell Foster et al. (2021) [24] | USA | Suicide | 118 parents (73.7% female) | 11–18 years, 57.3% female | Self-report surveys (baseline and follow-up) | Emergency department | Discovery, During management |
| Fu et al. (2020) [25] | China | NSSI | 20 parents (80% female) | 12–18 years (mean age = 14.5 years) 85% female | Semi-structured interviews | Child psychiatric ward | Discovery, During management, After |
| Fu et al. (2021) [26] | China | Suicide and self-harm | 15 parents (73% female) | 12–18 years (mean age = 14.2 years) | Semi-structured interviews | Psychiatric department in a general hospital | During management |
| Gillespie et al. (2019) [27] | Ireland | Self-harm | 167 parents (72.5% female) Age range = 25–65+ | 13–18 years | Self-report surveys | Community based child and adolescent mental health service | During management |
| Kaufman et al. (2020) [28] | USA | Self-harm | 60 parents (30 control and 30 of self-injuring adolescents) (100% female) Mean age clinical sample = 45.07 years Mean age control sample = 44.8 years | 13–17 years (mean age clinical sample = 15.47 years, mean age control sample = 14.77 years) 100% Female | Interview and self-report surveys | Online recruitment, paediatrician offices and local businesses, and outpatient and inpatient clinics | During management |
| Kawabe et al. (2016) [29] | Japan | Suicidal ideation | 179 parents and 6 caregivers (83% female) Median age 43 years | 12–15 years 51.4% female | Self-report surveys | 3 junior high schools in rural region of Japan | During management |
| Kelada et al. (2016) [30] | Australia | NSSI | 16 parents (94% female) 36–56 years (mean age = 45.44 years) | 14–17 years (mean age = 15.38 years) 62.5% female | Self-report surveys | 5 high schools | Discovery, During management, After |
| Kelada et al. (2017) [31] | Australia | NSSI | 10 parents (100% female) Mean age = 45.2 years | Mean age = 15.1 years 90% female | Survey with open ended questions | High schools | During management |
| McKay & Shand (2016) [32] | Australia | Suicide attempt | 3 parents (100% female) | 14–15 years 100% female | Semi-structured interviews | Online recruitment | During management, After |
| Miers et al. (2012) [33] | USA | Suicide death | 8 parents (75% female) Age range = 33–50 years | 13–18 years 33.3% female | Semi-structured interviews | Suicide bereavement groups | After |
| O’Brien et al. (2019) [34] | USA | Suicide | 8 parents (50% female) Mean age = 53.5 years | Mean age = 16.5 years 75% female | Semi-structured interviews | Inpatient psychiatric unit | During management |
| O’Gara et al. (2022) [35] | USA | Suicide | 10 fathers Mean age = 39.4 years | Age range = 11–19 years Mean age = 15.9 years 100% female | Semi-structured interviews | Mental health services associated with 3 hospitals and outpatient departments | Discovery, During management |
| Oldershaw et al. (2008) [36] | England | Self-harm | 12 parents (83% female) | Age range = 13–18 years 100% female | Semi-structured interviews | Community child and adolescent mental health services | Discovery, During management, After |
| Townsend et al. (2021) [37] | Australia | Self-harm | 37 parents (92% female) Mean age = 45.7 years | Age range = 12–18 years Mean age = 16.89 years 75.7% female | Self-report survey with open ended questions | Online recruitment and via community mental health services and parenting groups | During management |
| Wagner et al. (2000) [38] | USA | Suicide attempt | 34 parents (65% female) Mothers age range = 32–49 years (median = 39 years) Fathers age range = 38–55 years (median = 46 years) | Age range = 13–19 years Mean age = 15.5 years | Self-report survey | Private psychiatric hospital | Discovery, During management |
| Wang et al. (2022) [39] | China | NSSI | 24 parents (75% female) Mean age = 42.5 years | Age range = 12–18 years Mean age = 15 years 87.5% female | Semi-structured interviews | Psychiatric ward | Discovery, During management, After |
| Ye et al. (2021) [40] | China | Self-harm | 11 parents (73% female) Age range = 35–40 years Mean age = 37 years | Age range = 11–18 years | Semi-structured interviews | Emergency department | Discovery, During management |
| Temporal Themes | Sub-Themes | |
|---|---|---|
| 1. | Discovery of suicidal phenomena | 1.1 Unsure how to respond |
| 1.2 Emotional response | ||
| 2. | During the management of suicidal phenomena | 2.1 Parent wellbeing |
| 2.2 Help seeking for child | ||
| 2.3 Parent and child (dis)connection | ||
| 2.4 Poor access to support for parents | ||
| 2.5 Changes in parent behaviour and impact on family | ||
| 2.6 Making sense of the crisis | ||
| 3. | After the suicidal phenomena had ceased | 3.1 Changes in parent–child relationship |
| 3.2 Support for parents |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rheinberger, D.; Shand, F.; McGillivray, L.; McCallum, S.; Boydell, K. Parents of Adolescents Who Experience Suicidal Phenomena—A Scoping Review of Their Experience. Int. J. Environ. Res. Public Health 2023, 20, 6227. https://doi.org/10.3390/ijerph20136227
Rheinberger D, Shand F, McGillivray L, McCallum S, Boydell K. Parents of Adolescents Who Experience Suicidal Phenomena—A Scoping Review of Their Experience. International Journal of Environmental Research and Public Health. 2023; 20(13):6227. https://doi.org/10.3390/ijerph20136227
Chicago/Turabian StyleRheinberger, Demee, Fiona Shand, Lauren McGillivray, Sonia McCallum, and Katherine Boydell. 2023. "Parents of Adolescents Who Experience Suicidal Phenomena—A Scoping Review of Their Experience" International Journal of Environmental Research and Public Health 20, no. 13: 6227. https://doi.org/10.3390/ijerph20136227
APA StyleRheinberger, D., Shand, F., McGillivray, L., McCallum, S., & Boydell, K. (2023). Parents of Adolescents Who Experience Suicidal Phenomena—A Scoping Review of Their Experience. International Journal of Environmental Research and Public Health, 20(13), 6227. https://doi.org/10.3390/ijerph20136227