
Effects of Physical Activity on Physical and Mental Health of Older Adults Living in Care Settings: A Systematic Review of Meta-Analyses

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
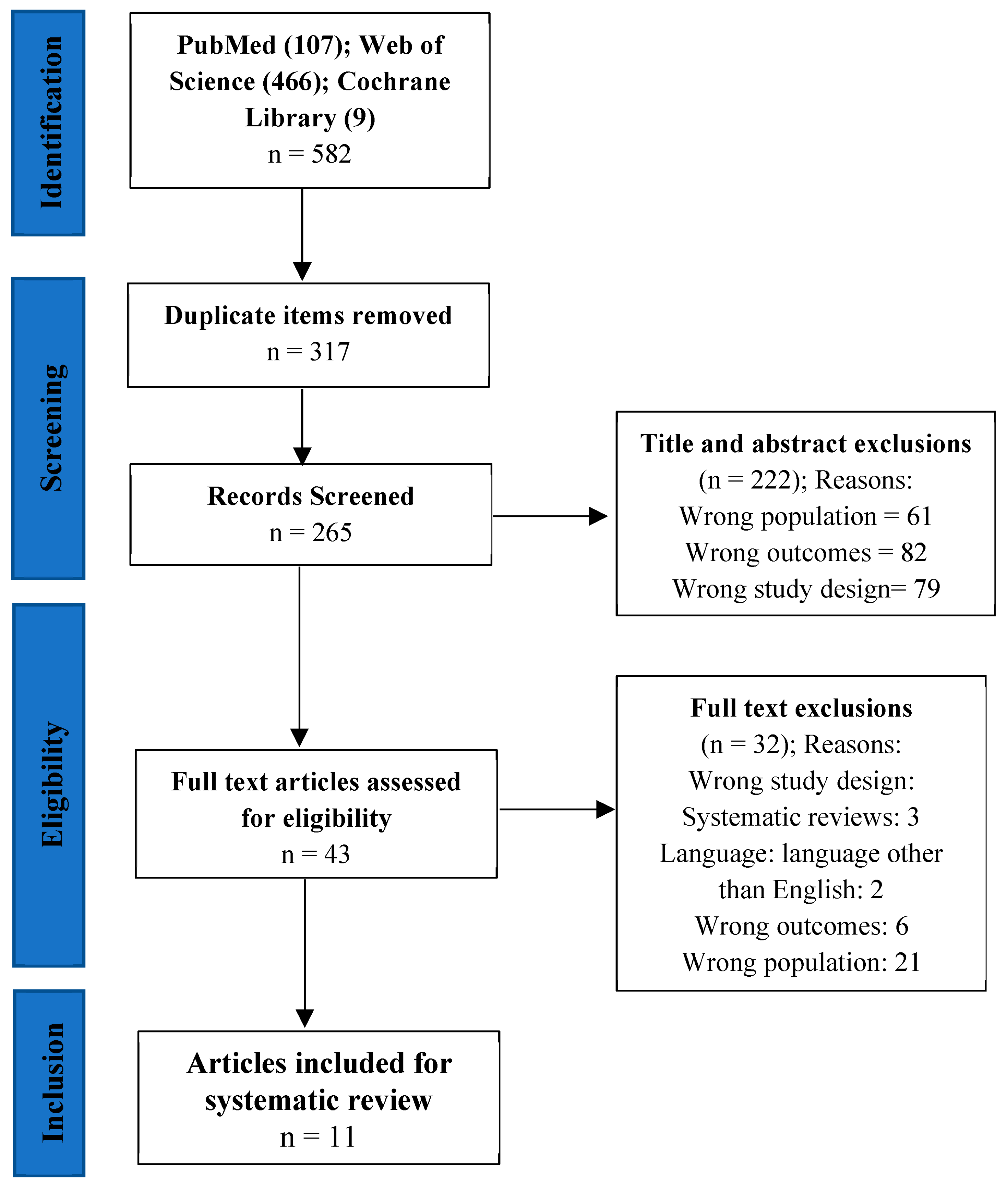
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
3. Results
3.1. Characteristics of the Meta-Analyses
3.2. Quality of Meta-Analyses
3.2.1. Data Sources
3.2.2. Analysis of Individual Studies by the Meta-Analyst and General Meta-Analysis
3.3. Effects of Interventions on Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowe, J.W.; Kahn, R.L. Successful Aging. Gerontologist 1997, 37, 433–440. [Google Scholar] [CrossRef]
- Urtamo, A.; Jyväkorpi, S.K.; Strandberg, T.E. Definitions of successful ageing: A brief review of a multidimensional concept. Acta Biomed. 2019, 90, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.; Schmitt, E.; Kaltenbach, G.; Lang, P.-O. La fragilité: Un concept robuste mais une méthode d’évaluation encore fragile. NPG Neurologie—Psychiatrie—Gériatrie 2014, 14, 43–49. [Google Scholar] [CrossRef]
- National Institute on Aging. Residential Facilities, Assisted Living, and Nursing Homes. Available online: https://www.nia.nih.gov/health/residential-facilities-assisted-living-and-nursing-homes (accessed on 9 May 2023).
- National Institute on Aging. What Is Long-Term Care? Available online: https://www.nia.nih.gov/health/what-long-term-care (accessed on 9 May 2023).
- Rapp, K.; Becker, C.; Cameron, I.D.; König, H.-H.; Büchele, G. Epidemiology of Falls in Residential Aged Care: Analysis of More Than 70,000 Falls From Residents of Bavarian Nursing Homes. J. Am. Med. Dir. Assoc. 2012, 13, 187.e1–187.e6. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Dubost, V.; Revel-Delhom, C.; Berrut, G.; Belmin, J. French Society of Geriatrics and Gerontology. How to manage recurrent falls in clinical practice: Guidelines of the French society of geriatrics and gerontology. J. Nutr. Health Aging 2011, 15, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Hartholt, K.A.; van Beeck, E.F.; Polinder, S.; van der Velde, N.; van Lieshout, E.M.M.; Panneman, M.J.M.; van der Cammen, T.J.M.; Patka, P. Societal Consequences of Falls in the Older Population: Injuries, Healthcare Costs, and Long-Term Reduced Quality of Life. J. Trauma Inj. Infect. Crit. Care 2011, 71, 748–753. [Google Scholar] [CrossRef]
- Cameron, I.D.; Gillespie, L.D.; Robertson, M.C.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst. Rev. 2012, 12, CD005465. [Google Scholar] [CrossRef]
- Cameron, I.D.; Dyer, S.M.; Panagoda, C.E.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst. Rev. 2018, 9, CD005465. [Google Scholar] [CrossRef]
- Rapp, K.; Becker, C.; E Lamb, S.; Icks, A.; Klenk, J. Hip Fractures in Institutionalized Elderly People: Incidence Rates and Excess Mortality. J. Bone Miner. Res. 2008, 23, 1825–1831. [Google Scholar] [CrossRef]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35 (Suppl. S2), ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Kok, R.; Reynolds, C.F. Management of Depression in Older Adults. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Da Silva, J.L.; Agbangla, N.F.; Le Page, C.; Ghernout, W.; Andrieu, B. Effects of Chronic Physical Exercise or Multicomponent Exercise Programs on the Mental Health and Cognition of Older Adults Living in a Nursing Home: A Systematic Review of Studies From the Past 10 Years. Front. Psychol. 2022, 13, 888851. [Google Scholar] [CrossRef]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodríguez-Mañas, L.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. AGE 2014, 36, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Jahanpeyma, P.; Koçak, F.K.; Yıldırım, Y.; Şahin, S.; Şenuzun Aykar, F. Effects of the Otago exercise program on falls, balance, and physical performance in older nursing home residents with high fall risk: A randomized controlled trial. Eur. Geriatr. Med. 2020, 12, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Crombie, I.; Davies, H.T. What Is Meta-Analysis? 2nd ed.; Evidence Based Medicine; Hayward Medical Publishing: Little Bookham, UK, 2009; pp. 1–8. [Google Scholar]
- Riley, R.D.; Lambert, P.; Abo-Zaid, G. Meta-analysis of individual participant data: Rationale, conduct, and reporting. BMJ 2010, 340, c221. [Google Scholar] [CrossRef]
- de Souto Barreto, P.D.S.; Rolland, Y.; Vellas, B.; Maltais, M. Association of Long-term Exercise Training with Risk of Falls, Fractures, Hospitalizations, and Mortality in Older Adults: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2019, 179, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Saragih, I.D.; Yang, Y.; Saragih, I.S.; Batubara, S.O.; Lin, C. Effects of resistance bands exercise for frail older adults: A systematic review and meta-analysis of randomised controlled studies. J. Clin. Nurs. 2022, 31, 43–61. [Google Scholar] [CrossRef]
- Lam, F.M.; Huang, M.-Z.; Liao, L.-R.; Chung, R.C.; Kwok, T.C.; Pang, M.Y. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: A systematic review. J. Physiother. 2018, 64, 4–15. [Google Scholar] [CrossRef]
- Liu, C.-J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2009, CD002759. [Google Scholar] [CrossRef]
- Miller, K.J.; Gonçalves-Bradley, D.C.; Areerob, P.; Hennessy, D.; Mesagno, C.; Grace, F. Comparative effectiveness of three exercise types to treat clinical depression in older adults: A systematic review and network meta-analysis of randomised controlled trials. Ageing Res. Rev. 2020, 58, 100999. [Google Scholar] [CrossRef] [PubMed]
- Rogan, S.; de Bruin, E.D.; Radlinger, L.; Joehr, C.; Wyss, C.; Stuck, N.-J.; Bruelhart, Y.; de Bie, R.A.; Hilfiker, R. Effects of whole-body vibration on proxies of muscle strength in old adults: A systematic review and meta-analysis on the role of physical capacity level. Eur. Rev. Aging Phys. Act. 2015, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Lane, P.W.; Anagnostelis, B.; Anzures-Cabrera, J.; Baker, N.F.; Cappelleri, J.C.; Haughie, S.; Hollis, S.; Lewis, S.C.; Moneuse, P.; et al. A tool to assess the quality of a meta-analysis. Res. Synth. Methods 2013, 4, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Gulka, H.J.; Patel, V.; Arora, T.; McArthur, C.; Iaboni, A. Efficacy and Generalizability of Falls Prevention Interventions in Nursing Homes: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1024–1035.e4. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Luo, J.; Reangsing, C.; Schneider, J.K. Effects of exercise on depressive symptoms among nursing home residents: A meta-analysis. Aging Ment. Health 2021, 26, 1514–1523. [Google Scholar] [CrossRef]
- Crocker, T.; Young, J.; Forster, A.; Brown, L.; Ozer, S.; Greenwood, D.C. The effect of physical rehabilitation on activities of daily living in older residents of long-term care facilities: Systematic review with meta-analysis. Age Ageing 2013, 42, 682–688. [Google Scholar] [CrossRef]
- Crocker, T.; Forster, A.; Young, J.; Brown, L.; Ozer, S.; Smith, J.; Green, J.; Hardy, J.; Burns, E.; Glidewell, E.; et al. Physical rehabilitation for older people in long-term care. Cochrane Database Syst. Rev. 2013, 2, CD004294. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, H.S. Exercise Interventions for Preventing Falls Among Older People in Care Facilities: A Meta-Analysis. Worldviews Evid.-Based Nurs. 2016, 14, 74–80. [Google Scholar] [CrossRef]
- Schoberer, D.; Breimaier, H.E. Meta-analysis and GRADE profiles of exercise interventions for falls prevention in long-term care facilities. J. Adv. Nurs. 2020, 76, 121–134. [Google Scholar] [CrossRef]
- Silva, R.B.; Eslick, G.D.; Duque, G. Exercise for Falls and Fracture Prevention in Long Term Care Facilities: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2013, 14, 685–689.e2. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Barbosa, F.; del Pozo-Cruz, J.; del Pozo-Cruz, B.; García-Hermoso, A.; Alfonso-Rosa, R.M. Effects of Whole-Body Vibration on Functional Mobility, Balance, Gait Strength, and Quality of Life in Institutionalized Older People: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Aging Phys. Act. 2020, 28, 219–230. [Google Scholar] [CrossRef]
- Cao, P.-Y.; Zhao, Q.-H.; Xiao, M.-Z.; Kong, L.-N.; Xiao, L. The effectiveness of exercise for fall prevention in nursing home residents: A systematic review meta-analysis. J. Adv. Nurs. 2018, 74, 2511–2522. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Zhang, X.B.; Zhu, X.; Meng, L.; Zhang, Q. Effects of Otago Exercise Program on postural control ability in elders living in the nursing home: A systematic review and meta-analysis. Medicine 2023, 102, e33300. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Tian, B. The effectiveness of physical exercise type and length to prevent falls in nursing homes: A systematic review and meta-analysis. J. Clin. Nurs. 2021, 31, 32–42. [Google Scholar] [CrossRef]
- Amanollahi, A.; Moradi-Lakeh, M.; Shokraneh, F.; Bashiri, Y.; Mahmudi, L. Assessing the quality of meta-analyses in systematic reviews in pharmaceutical research in Iran by 2016: A systematic review. Med. J. Islam. Repub. Iran 2020, 34, 209–216. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Tufanaru, C.; Munn, Z.; Stephenson, M.; Aromataris, E. Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int. J. Evid.-Based Health 2015, 13, 196–207. [Google Scholar] [CrossRef]
- Shakeel, S.; Newhouse, I.; Malik, A.; Heckman, G. Identifying Feasible Physical Activity Programs for Long-Term Care Homes in the Ontario Context. Can. Geriatr. J. 2015, 18, 73–104. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Stubbs, B.; Denkinger, M.D.; Brefka, S.; Dallmeier, D. What works to prevent falls in older adults dwelling in long term care facilities and hospitals? An umbrella review of meta-analyses of randomised controlled trials. Maturitas 2015, 81, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Aizenstein, H.; Reynolds, C.F., III; Butters, M.A.; Erickson, K.I. Exercise effects on depression: Possible neural mechanisms. Gen. Hosp. Psychiatry 2017, 49, 2–10. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef]
- Dishman, R.K.; Berthoud, H.-R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H.; et al. Neurobiology of Exercise. Obesity 2006, 14, 345–356. [Google Scholar] [CrossRef]
- De Matos, M.G.; Calmeiro, L.; Da Fonseca, D. Effet de l’activité physique sur l’anxiété et la dépression [Effect of physical activity on anxiety and depression]. Presse Med. 2009, 38, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Penseyres, I.; Martin, J.-L. Mieux comprendre les mécanismes physiologiques de l’activité physique pour mieux traiter la dépression [Improving understanding of the physiological mechanisms of exercise to better treat depression]. Rev. Med. Suisse 2018, 14, 950–952. [Google Scholar] [CrossRef]
- Ofosu, E.F.; de Nys, L.; Connelly, J.; Ryde, G.C.; Whittaker, A.C. Dimensions of Physical Activity Are Important in Managing Anxiety in Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2023, 24, 1–14. [Google Scholar] [CrossRef]
- André, N.; Agbangla, N.F. Are Barriers the Same Whether I Want to Start or Maintain Exercise? A Narrative Review on Healthy Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 6247. [Google Scholar] [CrossRef]
- Buckinx, F.; Bruyère, O.; Lengelé, L.; Reginster, J.-Y.; Marchal, Q.; Hurtrez, P.; Mouton, A. The effects of GAMotion (a giant exercising board game) on physical capacity, motivation and quality of life among nursing home residents: A pilot interventional study. Exp. Gerontol. 2020, 138, 110983. [Google Scholar] [CrossRef] [PubMed]
- Mouton, A.; Gillet, N.; Mouton, F.; Van Kann, D.; Bruyere, O.; Cloes, M.; Buckinx, F. Effects of a giant exercising board game intervention on ambulatory physical activity among nursing home residents: A preliminary study. Clin. Interv. Aging 2017, 12, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Kolappa, K.; Henderson, D.C.; Kishore, S.P. No physical health without mental health: Lessons unlearned? Bull. World Health Organ. 2013, 91, 3–3A. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criteria | Frequency (%) | |
|---|---|---|
| Yes (%) | No (%) | |
| Eligibility criteria were stated and suitably specific for | ||
| Participants | 11 (100) | - |
| Experimental intervention (s) | 11 (100) | - |
| Comparator intervention (s) | 10 (90.9) | 1 (9.09) |
| Outcomes | 10 (90.9) | 1 (9.09) |
| Study designs | 11 (100) | - |
| Further restrictions on eligibility on studies or reports | ||
| Specific restriction | - | - |
| Publication status restriction | 4 (36.36) | 7 (63.63) |
| Language restriction | 6 (54.54) | 5 (45.45) |
| Other restriction | 9 (81.81) | 2 (18.18) |
| Data for meta-analysis were sought from | ||
| Published literature | 11 (100) | - |
| Online repositories | 10 (90.9) | 1 (9.09) |
| Correspondence with trialists | 1 (9.09) | 10 (90.9) |
| In-house IPD a | - | 11 (100) |
| Other IPD | - | 11 (100) |
| The search for trials included | ||
| Bibliographic databases | 11 (100) | - |
| Grey literature | 2 (18.18) | 9 (81.81) |
| The web | 2 (18.18) | 9 (81.81) |
| In-houses collections | - | 11 (100) |
| Reference lists | 9 (81.81) | 2 (18.18) |
| Hand searching | 8 (72.72) | 3 (27.27) |
| Correspondence with industry | - | 11 (100) |
| Other correspondence | - | 11 (100) |
| Other sources | 1 (9.09) | 10 (90.9) |
| Which bibliographic databases are mentioned | ||
| PubMed/MEDLINE | 11 (100) | - |
| EMBASE | 9 (81.81) | 2 (18.18) |
| CENTRAL/Cochrane Library | 10 (90.9) | 1 (9.09) |
| Science Citation Database | 3 (27.27) | 8 (72.72) |
| Other | 11 (100) | - |
| Criteria | Frequency (%) | |
|---|---|---|
| Yes (%) | No (%) | |
| Risk of bias (quality assessment) or eligibility criteria include | ||
| Generation of allocation sequence | 10 (90.9) | 1 (9.09) |
| Concealment of allocation sequence | 11 (100) | - |
| Blinding | 10 (90.9) | 1 (9.09) |
| Attrition/dropout/ITT b | 9 (81.81) | 2 (18.18) |
| Other | 7 (63.63) | 4 (36.36) |
| The synthesis methods used in the paper | ||
| Pooling (no stratification by study) | - | - |
| Fixed-effect meta-analysis | 3 (27.27) | 8 (72.72) |
| Random-effect meta-analysis | 11 (100) | - |
| Fixed-effect meta regression | - | - |
| Random-effect meta regression | 1 (9.09) | 10 (90.9) |
| Tools was used for assessed reporting bias | ||
| Funnel plots | 8 (72.72) | 3 (27.27) |
| Egger test | 5 (45.45) | 6 (54.54) |
| Begg-mazumdar rank correlation test | 1 (9.09) | 10 (90.9) |
| Other Funnel plots asymmetry test | - | - |
| Trim and Fill | 1 (9.09) | 10 (90.9) |
| Other | 5 (45.45) | 6 (54.54) |
| Criteria | Yes (%) | Unclear (%) | No (%) | Not Applicable (%) |
|---|---|---|---|---|
| Issues for continuous data | ||||
| Was the choice of effect size appropriate? | 11 (100%) | - | - | - |
| Was skew of data a potential problem that was not appropriately addressed? | - | 1 (9.09%) | 2 (18.18%) | 8 (72.72%) |
| Issues for binary data | ||||
| Were methods appropriate to rare events/sparse data? | 2 (18.18%) | - | - | 9 (81.81%) |
| Were cut points to dichotomize continuous/ordinal outcomes justified? | 3 (27.27%) | 1 (9.09%) | - | 7 (63.63%) |
| Issues for time-to-event data | ||||
| Were time-to-event data appropriately dealt with? | 2 (18.18%) | - | - | 9 (81.81%) |
| Issues for ordinal data | ||||
| Were ordinal data appropriately dealt with? | - | - | - | 11 (100%) |
| Indirect comparisons? | ||||
| Were indirect comparisons performed appropriately? | 2 (18.18%) | 1 (9.09%) | - | 8 (72.72%) |
| Summary Judgment | Yes | Probably Yes | Unclear | Probably No | No | Not Applicable |
|---|---|---|---|---|---|---|
| Were the review methods adequate such that biases in location and assessment of studies were minimized or able to be identified? | 11 (100%) | - | - | - | - | - |
| Were the individual studies analyzed appropriately and without avoidable bias? | 7 (63.63%) | 4 (36.36%) | - | - | - | - |
| Were the basic meta-analysis methods appropriate? | 11 (100%) | - | - | - | - | - |
| Are the conclusions justified and the interpretation sound? | 11/11 (100%) | - | - | - | - | - |
| References | Major Results |
|---|---|
| Gulka et al. [28] | PA reduced the number of falls (RR c = 0.73, 95% CI d [0.60, 0.88]), fallers (RR = 0.80, 95% CI [0.72, 0.89]), and recurrent fallers (RR = 0.70, 95% CI [0.60, 0.81]). |
| Li et al. [29] | PA improved depressive symptoms among older adults compared with control groups (g e = 0.25; 95% CI [0.11, 0.38], p < 0.001). |
| Crocker et al. [30] | Physical rehabilitation improved independence in activities of daily living by 0.24 standard units (95% CI [0.11, 0.38], p = 0.0005) compared with control groups. |
| Crocker et al. [31] | Physical rehabilitation improved Barthel Index scores of six points (95% CI [2, 11], p = 0.008), Functional Independence Measure scores of five points (95% CI [−2, 12], p = 0.1), Rivermead Mobility Index scores by 0.7 points (95% CI [0.04, 1.3], p = 0.04), and Timed Up and Go test scores of five seconds (95% CI [−9 to 0], p = 0.05). |
| Lee and Kim [32] | PA had a preventive effect on the rate of falls (RR = 0.81, 95% CI [0.68, 0.97]). |
| Schoberer et al. [33] | Physical activity with a balance component (RR = 0.79, 95% CI [0.65, 0.98]) or with technical devices (RR = 0.55, 95% CI [0.30, 0.99]) reduced falls significantly. The evidence indicated that physical exercises conducted for longer than six months were beneficial (RR = 0.73, 95% CI [0.57, 0.94]). |
| Silva et al. [34] | PA had a preventive effect on falls (RR = 0.77, 95% CI [0.64, 0.92], p < 0.001). This effect was stronger when mixing several types of exercises (RR = 0.71, 95% CI [0.55, 0.90], p < 0.001) for at least 1–3 months (RR = 0.65, 95% CI [0.43, 0.98], p < 0.001) or for more than six months (RR = 0.70, 95% CI [0.56, 0.87], p < 0.001), with a frequency of at least 2–3 times per week (RR = 0.74, 95% CI [0.60, 0.91], p < 0.001). |
| Alvarez-Barbosa et al. [35] | Whole-body vibration improved functional mobility as assessed with the Time Up and Go test (MD = −2.49 s, 95% CI [−4.37, −0.61], p = 0.009). |
| Cao et al. [36] | PA groups showed no statistically significant differences in falls outcome (OR = 0.88, 95% CI [0.48, 1.59], p = 0.663) compared with control groups. |
| Kong et al. [37] | The Otago exercise program decreased fall risk (MD = −0.84; 95% CI [−1.17, −0.51]; p < 0.00001) and positively increased postural balance (MD = 5.55; 95% CI [3.60, 7.50], p < 0.00001), functional mobility in short distance (MD = −6.39; 95% CI [−8.07, −4.70], p < 0.00001), and lower-limb muscle strength (MD = 4.32; 95% CI [3.71, 4.93], p < 0.00001). |
| Wang and Tian [38] | PA significantly affected fall prevention (RR = 0.85, 95% CI [0.73, −0.98]). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbangla, N.F.; Séba, M.-P.; Bunlon, F.; Toulotte, C.; Fraser, S.A. Effects of Physical Activity on Physical and Mental Health of Older Adults Living in Care Settings: A Systematic Review of Meta-Analyses. Int. J. Environ. Res. Public Health 2023, 20, 6226. https://doi.org/10.3390/ijerph20136226
Agbangla NF, Séba M-P, Bunlon F, Toulotte C, Fraser SA. Effects of Physical Activity on Physical and Mental Health of Older Adults Living in Care Settings: A Systematic Review of Meta-Analyses. International Journal of Environmental Research and Public Health. 2023; 20(13):6226. https://doi.org/10.3390/ijerph20136226
Chicago/Turabian StyleAgbangla, Nounagnon Frutueux, Marie-Philippine Séba, Frédérique Bunlon, Claire Toulotte, and Sarah Anne Fraser. 2023. "Effects of Physical Activity on Physical and Mental Health of Older Adults Living in Care Settings: A Systematic Review of Meta-Analyses" International Journal of Environmental Research and Public Health 20, no. 13: 6226. https://doi.org/10.3390/ijerph20136226
APA StyleAgbangla, N. F., Séba, M.-P., Bunlon, F., Toulotte, C., & Fraser, S. A. (2023). Effects of Physical Activity on Physical and Mental Health of Older Adults Living in Care Settings: A Systematic Review of Meta-Analyses. International Journal of Environmental Research and Public Health, 20(13), 6226. https://doi.org/10.3390/ijerph20136226