
The Epidemiological Surveillance of Mesothelioma Mortality in Italy as a Tool for the Prevention of Asbestos Exposure

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
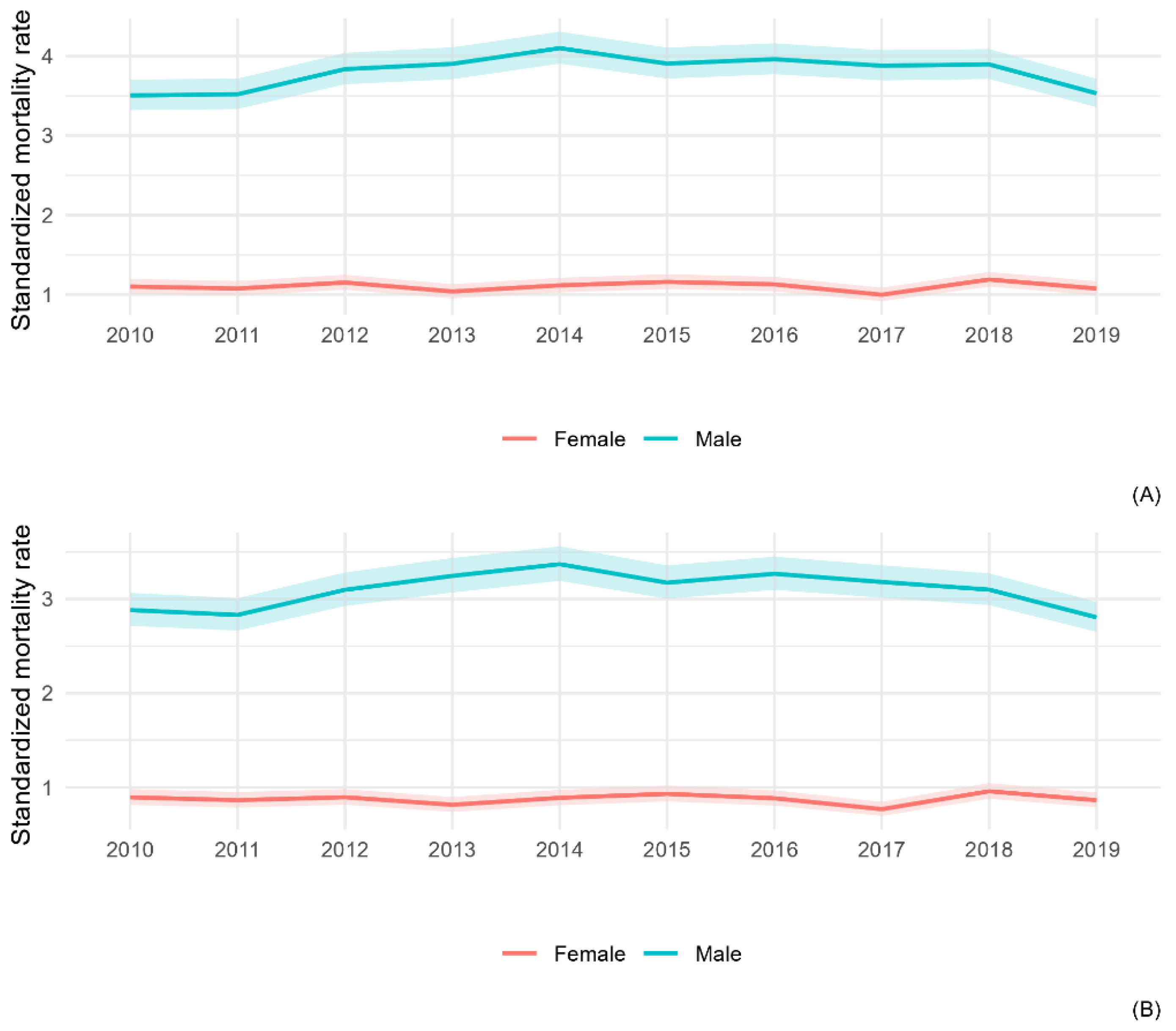
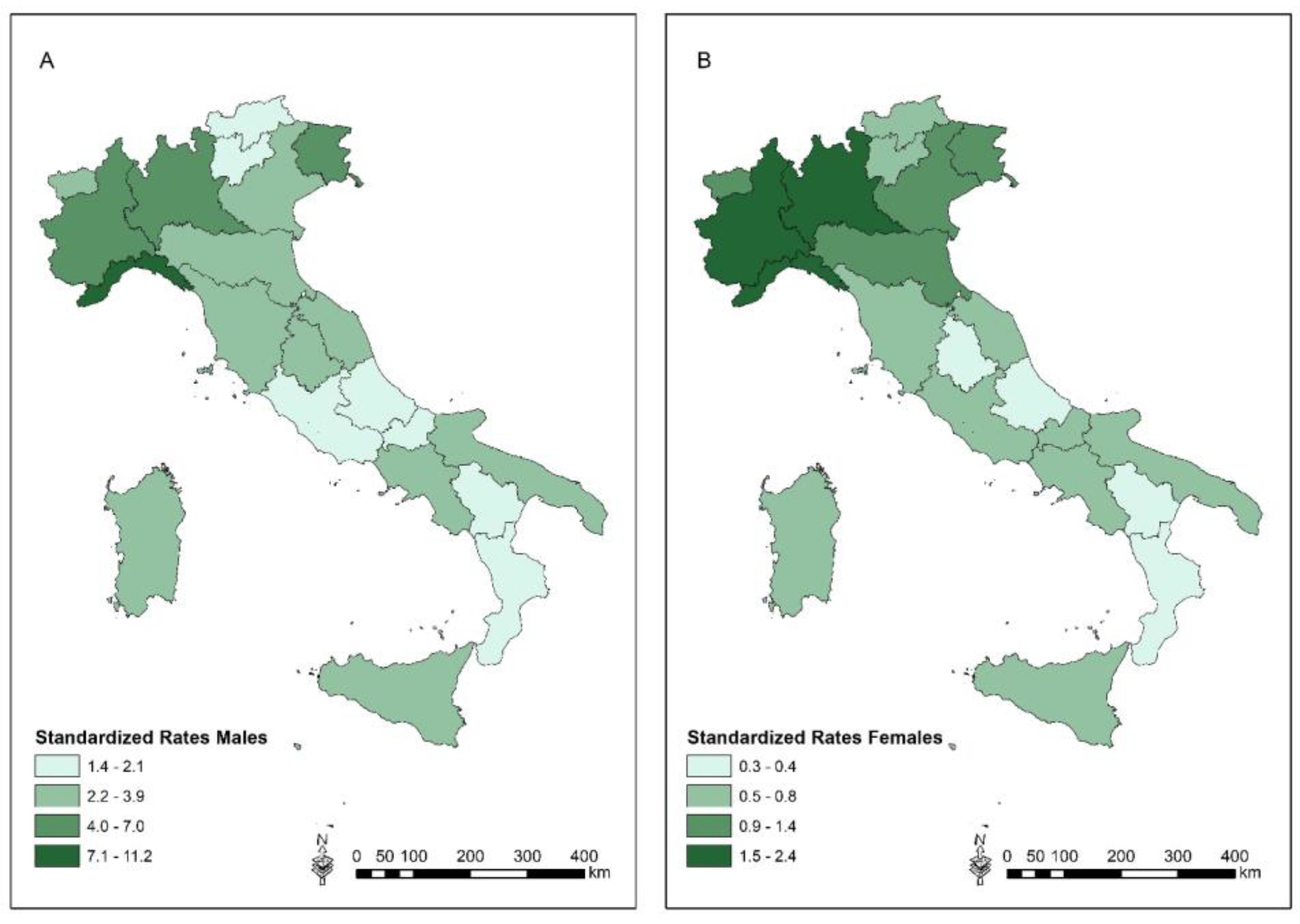
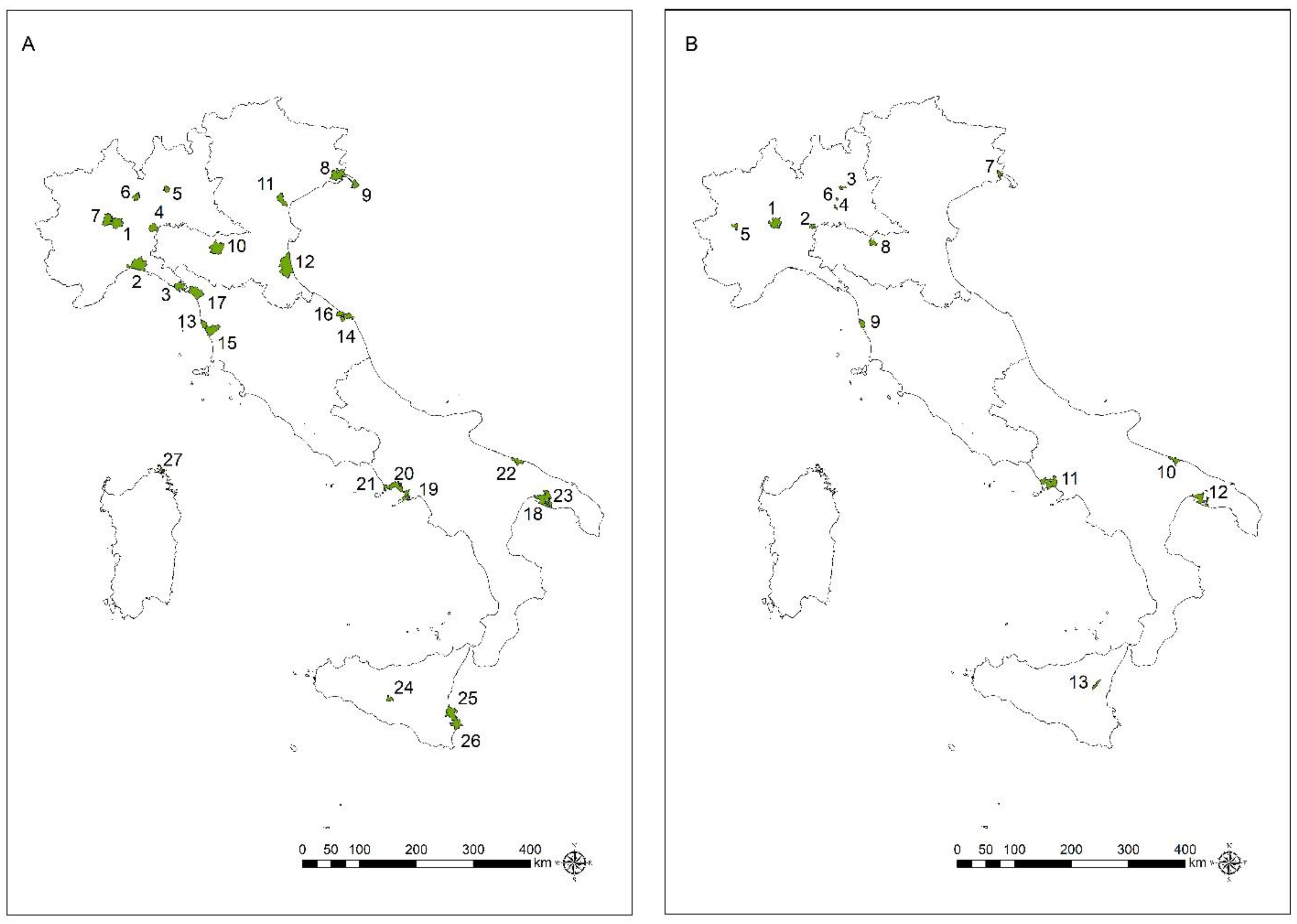
3.1. All-Ages Population
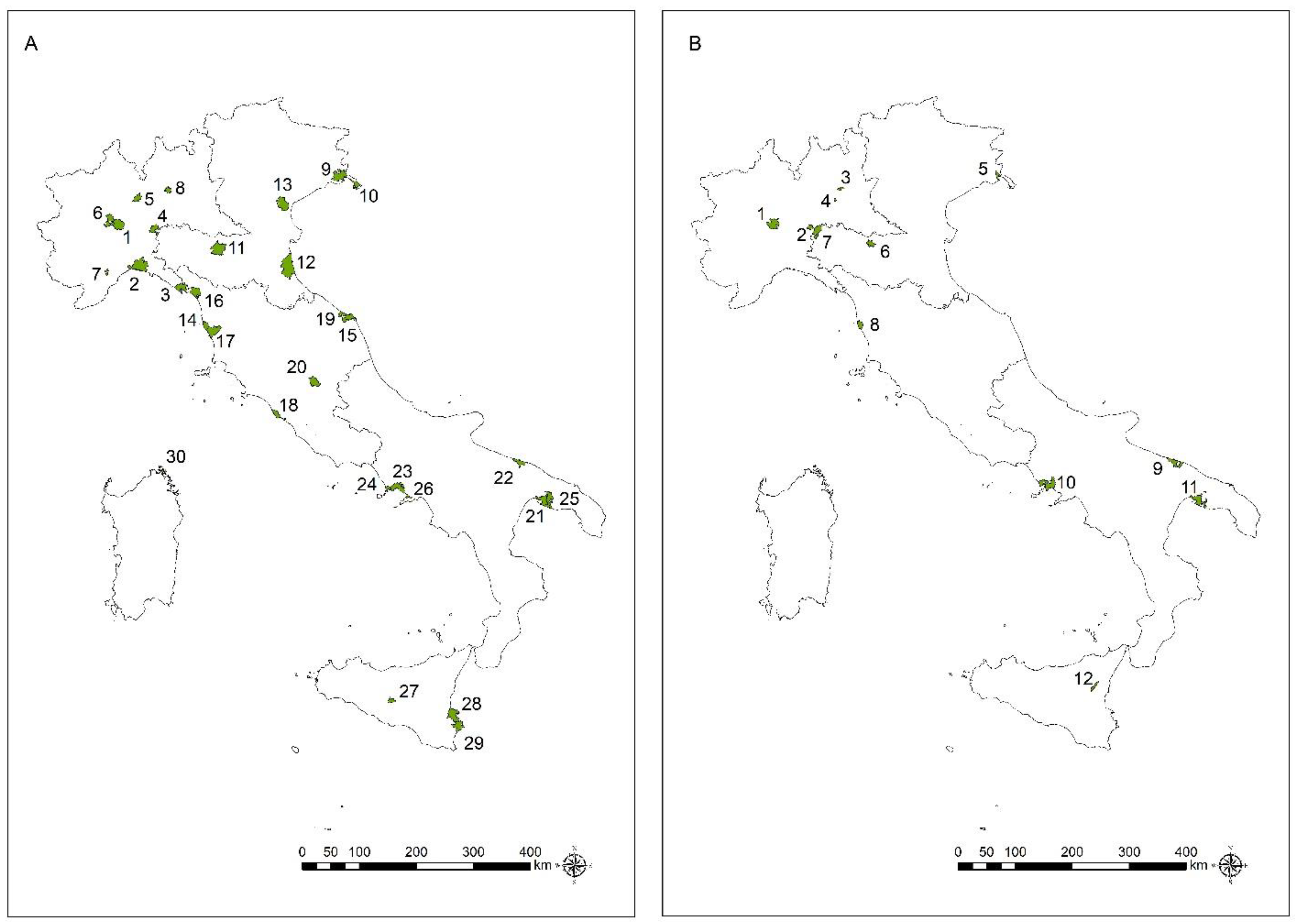
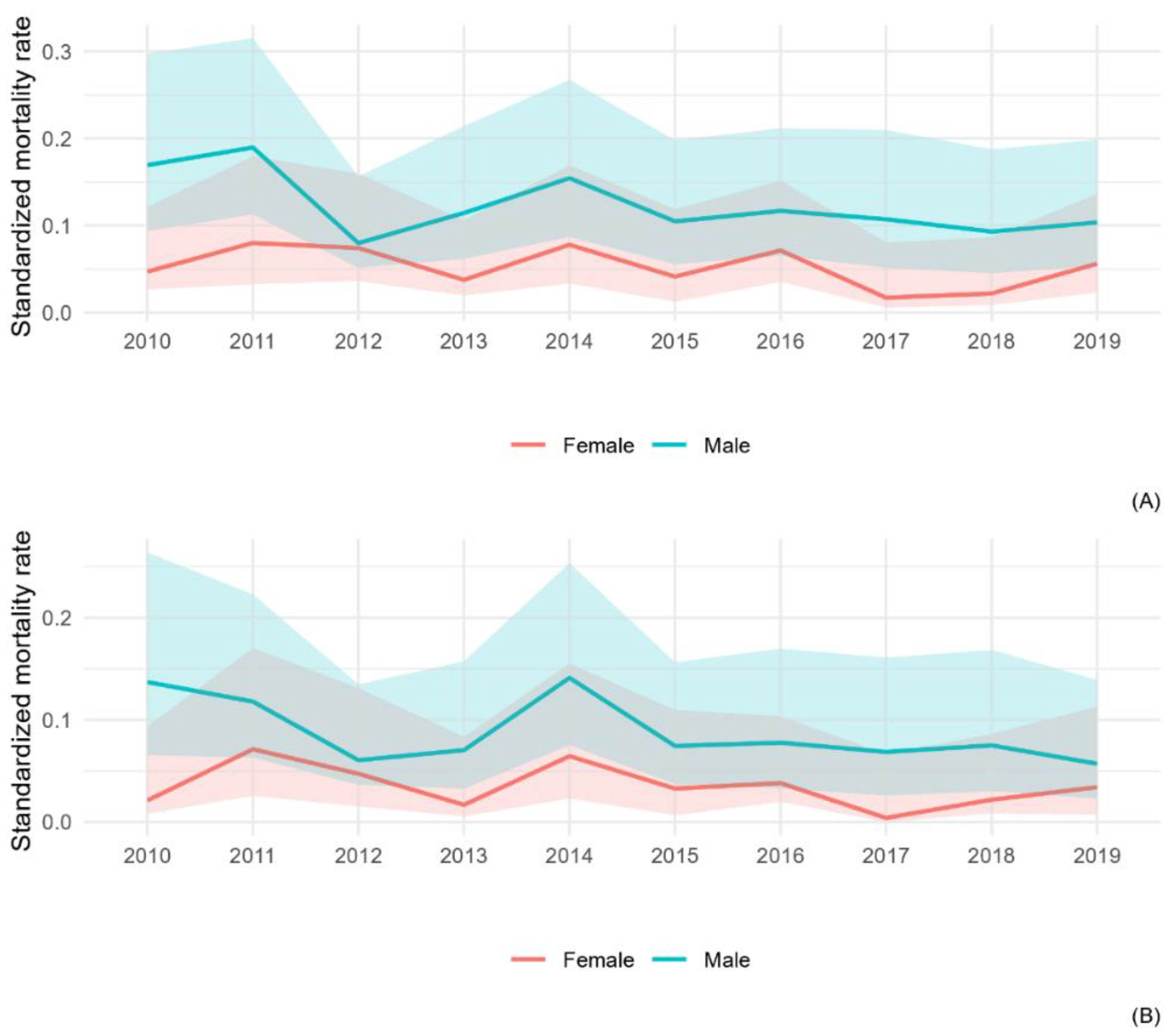
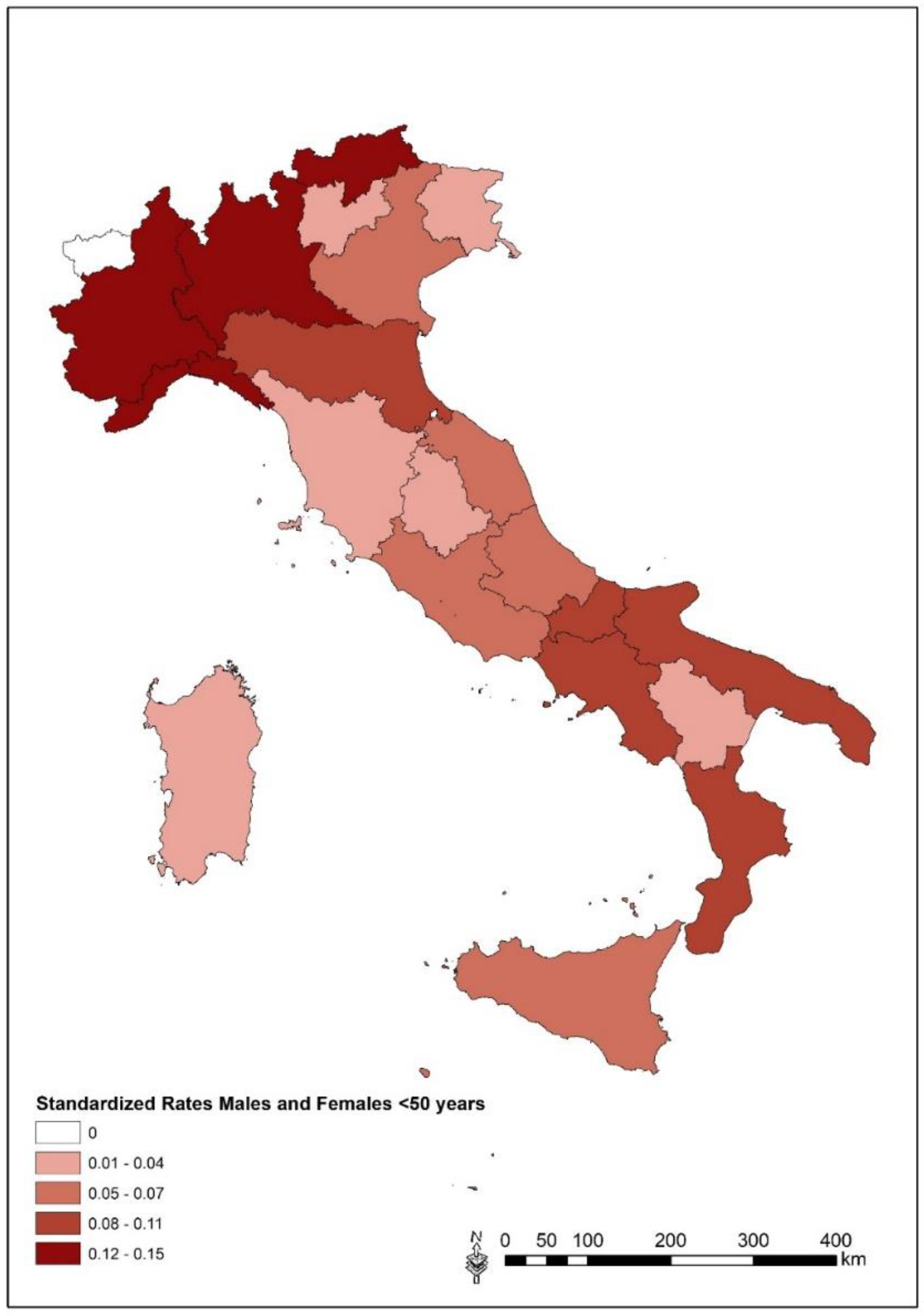
3.2. Focus in ≤50 Years Age-Class
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Asbestos. In Arsenic, Metals, Fibres and Dust. A Review on Human Carcinogens. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2012; Volume 100C, pp. 219–309. [Google Scholar]
- International Labour Office and World Health Organization. Outline for the Development of National Programs for Elimination of Asbestos Related Diseases. 2007. Available online: https://www.ilo.org/safework/info/publications/WCMS_108555/lang--en/index.htm (accessed on 20 March 2023).
- Binazzi, A.; Marinaccio, A. (Eds.) Il Registro Nazionale dei Mesoteliomi (ReNaM). Settimo Rapporto; INAIL: Rome, Italy, 2021; Available online: https://www.inail.it/cs/internet/comunicazione/pubblicazioni/catalogo-generale/pubbl-il-registro-nazionale-mesoteliomi-settimo-rapporto.html (accessed on 20 March 2023).
- Furuya, S.; Odgerel, C.O.; Takahashi, K.; David, A.; Takala, J. Global Asbestos Disaster. Int. J. Environ. Public Health 2018, 15, 1000. [Google Scholar] [CrossRef] [PubMed]
- Thives, L.P.; Ghisi, E.; Thives-Junior, J.J.; Vieira, A.S. Is asbestos still a problem in the world? A current review. J. Environ. Manag. 2022, 319, 115716. [Google Scholar] [CrossRef] [PubMed]
- Arachi, D.; Furuya, S.; David, A.; Mangwiro, A.; Odgerel, C.O.; Lee, K.; Tighe, P.; Takala., J.; Driscoll, T.; Takahashi, K. Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. Int. J. Environ. Res. Public Health 2021, 18, 1804. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Declaration of the Sixth Ministerial Conference on Environment and Health: Annex 1. Compendium of Possible Actions to Advance the Implementation of the Ostrava Declaration; World Health Regional Office for Europe: Geneva, Switzerland, 2017; Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/341944/OstravaDeclaration_SIGNED.pdf (accessed on 20 March 2023).
- Mott, F.E. Mesothelioma: A review. Ochsner. J. 2012, 12, 70–79. [Google Scholar]
- Odgerel, C.O.; Arachi, D.; Driscoll, T.; Lin, R.T.; Takala, J.; Takahashi, K. Burden of mesothelioma deaths by National Income Category: Current status and future implications. Int. J. Environ. Res. Public Health 2020, 17, 6900. [Google Scholar] [CrossRef]
- Odgerel, C.O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko, O.M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 74, 851–858. [Google Scholar] [CrossRef]
- Harikrishnan, S.; Jeemon, P.; Mini, G.K.; Thankappan, K.R.; Sylaja, P.; GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar]
- World Health Organization. Mesothelioma. 2018. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/18-Mesothelioma-fact-sheet.pdf (accessed on 23 March 2023).
- GBD 2019 Cancer Collaboration. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019. A systematic analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef]
- Noonan, C.W. Environmental asbestos exposure and risk of mesothelioma. Ann. Transl. Med. 2017, 5, 234. [Google Scholar] [CrossRef]
- Catelan, D.; Consonni, D.; Biggeri, A.; Dallari, B.; Pesatori, A.C.; Riboldi, L.; Mensi, C. Estimate of environmental and occupational components in the spatial distribution of malignant mesothelioma incidence in Lombardy (Italy). Environ. Res. 2020, 188, 109691. [Google Scholar] [CrossRef]
- Xu, R.; Barg, F.; Emmett, E.A.; Wiebe, D.J.; Hwang, W.-T. Association between mesothelioma and non-occupational asbestos exposure: Systematic review and meta-analysis. Environ. Health 2018, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Rake, C.; Gilham, C.; Hatch, J.; Damton, A.; Hodgson, J.; Peto, J. Occupational, domestic and environmental mesothelioma risks in British population: A case-control study. Br. J. Cancer 2009, 100, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Berry, G.; de Klerk, N.; Hansen, J.; Heyworth, J.; Ambrosini, G. Age and sex differences in malignant mesothelioma after residential exposure to blue asbestos (crocidolite). Chest 2017, 131, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Luce, D.; Bugel, I.; Goldberg, P.; Goldberg, M.; Salomon, C.; Billon-Galland, M.A. Environmental exposure to tremolite and respiratory cancer in New Caledonia: A case-control study. Am. J. Epidemiol. 2000, 151, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Magnani, C.; Dalmasso, P.; Biggeri, A.; Ivaldi, C.; Mirabelli, D.; Terracini, B. Increased risk of malignant mesothelioma of the pleura after residential or domestic exposure to asbestos: A case-control study in Casale Monferrato, Italy. Environ. Health Perspect. 2001, 109, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Franklin, P.; Olsen, N.; Sleith, J.; Samuel, L.; Aboagye-Sarfo, P.; de Klerk, N.; Musk, A.W. All-cause mortality and cancer incidence among adults exposed to blue asbestos during childhood. Am. J. Ind. Med. 2013, 56, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Franklin, P.; Berry, G.; Peters, S.; Sodhi-Berry, N.; Brims, F.; Musk, A.W.; de Klerk, N.H. Are children more vulnerable to mesothelioma than adults? A comparison of mesothelioma risk among children and adults exposed non-occupationally to blue asbestos at Wittenoom. Occup. Environ. Med. 2018, 75, 898–903. [Google Scholar] [CrossRef]
- Dalsgaard, S.B.; Würtz, E.T.; Hansen, J.; Røe, O.D.; Omland, Ø. Environmental asbestos exposure in childhood and risk of mesothelioma later in life: A long term follow-up register based cohort study. Occup. Environ. Med. 2019, 76, 407–413. [Google Scholar] [CrossRef]
- Dalsgaard, S.B.; Würtz, E.T.; Hansen, J.; Røe, O.D.; Omland, Ø. Cancer incidence and risk of multiple cancers after environmental exposure in childhood. A long-term Register-based cohort study. Int. J. Environ. Res. Public Health 2021, 19, 268. [Google Scholar] [CrossRef]
- Dalsgaard, S.B.; Würtz, E.T.; Hansen, J.; Røe, O.D.; Omland, Ø. A cohort study on cancer incidence among women exposed to environmental asbestos in childhood with a focus on female cancers, including breast. Int. J. Environ. Res. Public Health 2022, 19, 2086. [Google Scholar] [CrossRef]
- Fazzo, L.; Binazzi, A.; Ferrante, D.; Minelli, G.; Consonni, D.; Bauleo, L.; Bruno, C.; Bugani, M.; De Santis, M.; Iavarone, I.; et al. Burden of mortality from asbestos-related diseases in Italy. Int. J. Environ. Res. Public Health 2021, 18, 10012. [Google Scholar] [CrossRef]
- Fazzo, L.; Minelli, G.; Bruno, C.; Comba, P.; Conti, S.; De Santis, M.; Zona, A.; Binazzi, A.; Magnani, C.; Martinaccio, A.; et al. Early mortality from malignant mesothelioma in Italy as proxy of environmental exposure to asbestos in children. Ann. Ist. Super. Sanità 2020, 56, 478–486. [Google Scholar] [CrossRef]
- Fazzo, L.; Minelli, G.; De Santis, M.; Bruno, C.; Zona, A.; Conti, S.; Comba, P. Epidemiological surveillance of mesothelioma mortality in Italy. Cancer Epidemiol. 2018, 55, 184–191. [Google Scholar] [CrossRef]
- Mensi, C.; Bonzini, M.; Macchione, M.; Sieno, C.; Riboldi, L.; Pesatori, A.C. Differences among peritoneal and pleural mesothelioma: Data from the Lombardy Region Mesothelioma Register (Italy). Med. Lav. 2011, 102, 409–416. [Google Scholar]
- Zona, A.; Fazzo, L.; Minelli, G.; De Santis, M.; Bruno, C.; Conti, S.; Comba, P. Peritoneal mesothelioma mortality in Italy: Spatial analysis and search for asbestos exposure sources. Cancer Epidemiol. 2019, 60, 162–167. [Google Scholar] [CrossRef]
- Oddone, E.; Boolon, J.; Nava, C.R.; Consonni, D.; Marinacio, A.; Magnani, C.; Gasparrini, A.; Barone Adesi, F. Effect of asbestos consumption on malignant pleural mesothelioma in Italy: Forecasts of mortality up to 2040. Cancers 2021, 13, 338. [Google Scholar] [CrossRef]
- Han, Y.; Zhang, T.; Chen, H.; Yang, X. Global magnitude and temporal trend of mesothelioma burden along with the contribution of occupational asbestos exposure in 204 countries and territories from 1990 to 2019: Results from the Global Burden of Diseases study 2019. Crit. Rev. Oncol. Hematol. 2022, 179, 103821. [Google Scholar] [CrossRef]
- Airoldi, C.; Magnani, C.; Lazzarato, F.; Mirabelli, D.; Tunesi, S.; Ferrante, D. Environmental asbestos exposure and clustering of malignant mesothelioma in community: A spatial analysis in a population-based case-control study. Environ. Health 2021, 20, 103. [Google Scholar] [CrossRef]
- Consonni, D.; De Matteis, S.; Dallari, B.; Pesatori, A.C.; Riboldi, L.; Mensi, C. Impact of an asbestos cement factory on mesothelioma incidence in a community in Italy. Environ. Res. 2020, 183, 108968. [Google Scholar] [CrossRef]
- Mirabelli, D.; Calisti, R.; Barone-Adesi, F.; Fornero, E.; Merletti, F.; Magnani, C. Excess of mesotheliomas after exposure to chrysotile in Balangero, Italy. Occup. Environ. Med. 2008, 65, 815–819. [Google Scholar] [CrossRef]
- Mensi, C.; Dallari, B.; Polonioli, M.; Riboldi, L.; Consonni, D.; Pesatori, A.C. Mesothelioma in agriculture in Lombardy, Italy: An unrecognized risk. Int. J. Environ. Res. Public Health 2021, 18, 358. [Google Scholar] [CrossRef] [PubMed]
- Pasetto, R.; Fazzo, L.; Zona, A.; Bruno, C.; Pirastu, R.; Binazzi, A.; Corfiati, M.; Silvestri, S.; Comba, P.; Marinaccio, A. SENTIERI-ReNaM: Valutazione globale del carico di mesothelioma. Epidemiol. Prev. 2016, 40 (Suppl. 1), 99–104. [Google Scholar] [PubMed]
- Gualtieri, A.F.; Pollastri, S.; Bursi Gandolfi, N.; Ronchetti, F.; Albonico, C.; Cavallo, A.; Zanetti, G.; Marini, P.; Sala, O. Determination of the concentration of asbestos minerals in highly contaminated mine tailings: An example from abandoned mine waste of Crétaz and Emarese (Valle d’Aosta, Italy). Am. Mineral. 2014, 99, 1233–1247. [Google Scholar] [CrossRef]
- Zona, A.; Fazzo, L.; Benedetti, M.; Bruno, C.; Vecchi, S.; Pasetto, R.; Minichilli, F.; De Santis, M.; Nannavecchia, A.M.; Di Fonzo, D.; et al. SENTIERI: Studio epidemiologico nazionale dei territory e degli insediamenti esposti a rischio da inquinamento. Sesto Rapport. Epidemiol. Prev. 2023, 47 (Suppl. 1), 1–286. [Google Scholar] [CrossRef]
- Lemen, R.A.; Landrigan, P.J. Sailors and the risk of asbestos-related cancer. Int. J. Environ. Public Health 2021, 18, 8417. [Google Scholar] [CrossRef]
- Ferrante, D.; Bertolotti, M.; Todesco, A.; Mirabelli, D.; Terracini, B.; Magnani, C. Cancer mortality and incidence of mesothelioma in a cohort of wives of asbestos workers in Casale Monferrato, Italy. Environ. Health Perspect. 2007, 115, 1401–1405. [Google Scholar] [CrossRef]
- Vimercati, L.; Cavone, D.; Delfino, M.C.; Caputi, A.; De Maria, L.; Sponselli, S.; Corrado, V.; Ferri, G.M.; Serio, G. Asbestos air pollution: Description of a mesothelioma cluster due to residential exposure from an asbestos cement factory. Int. J. Environ. Res. Public Health 2020, 17, 2636. [Google Scholar] [CrossRef]
- Menegozzo, S.; Comba, P.; Ferrante, D.; De Santis, M.; Gorini, G.; Izzo, F.; Magnani, C.; Pirastu, R.; Simonetti, A.; Tunesi, S.; et al. Mortality study in an asbestos cement factory in Naples, Italy. Ann. Ist. Super. Sanità 2011, 47, 296–304. [Google Scholar] [CrossRef]
- Fazzo, L.; Menegozzo, S.; Soggiu, M.E.; De Santis, M.; Santoro, M.; Cozza, V.; Brangi, A.; Menegozzo, M.; Comba, P. Mesothelioma incidence in the neighbourhood of an asbestos-cement plant located in a national priority contaminated site. Ann. Ist. Super. Sanità 2014, 50, 322–327. [Google Scholar] [CrossRef]
- Ascoli, V.; Carnevale-Scalzo, C.; Nardi, F.; Efrati, C.; Menegozo, M. A one-generation cluster of malignant mesothelioma within a family reveals exposure to asbestos-contaminated jute bags in Naples, Italy. Eur. J. Epidemiol. 2003, 18, 171–174. [Google Scholar] [CrossRef]
- Silvestri, S. Managing asbestos in Italy: Twenty years after the ban. New Solut 2012, 22, 486–496. [Google Scholar] [CrossRef]
- Hemminki, K.; Xinjun, L.I. Mesothelioma id a killer of urban men in Sweden. Int. J. Cancer 2003, 105, 144–146. [Google Scholar] [CrossRef]
- Ascoli, V.; Comba, P.; Pastto, R. Urban mesothelioma: Is there an emerging risk of asbestos in place? Int. J. Cancer 2004, 111, 975–976. [Google Scholar] [CrossRef]
- Capella, S.; Bellis, D.; Fioretti, E.; Marinelli, R.; Belluso, E. Respirable inorganic fibres dispersed in air and settled in human lung samples: Assessment of their nature, source, and concentration in a NW Italy large city. Environ. Pollut. 2020, 263 Pt B, 114384. [Google Scholar] [CrossRef]
- Marinaccio, A.; Corfiati, M.; Binazzi, A.; Di Marzio, D.; Scarselli, A.; Ferrante, D.; Bonafede, M.; Verardo, M.; Mirabelli, D.; Gennario, V.; et al. The epidemiology of malignant mesothelioma in women: Gender differences and modalities of asbestos exposure. Occup. Environ. Med. 2018, 75, 254–262. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Fluoro-edenite. In Some Nanomaterials and Some Fibres. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 2017; Volume 111, pp. 215–242. [Google Scholar]
- Comba, P.; Gainfagna, A.; Paoletti, L. Pleural mesothelioma cases in Biancavilla are related to a new fluoro-edentie fibrous amphibole. Arch. Environ. Health 2003, 58, 229–232. [Google Scholar] [CrossRef]
- Biggeri, A.; Pasetto, R.; Belli, S.; Bruno, C.; DI Maria, G.; Mastrantonio, M.; Trinca, S.; Ucceli, R.; Comba, P. Mortality from chronic obstructive pulmonary disease and pleural mesothelioma in an area contaminated by natural fiber (fluoro-edenite). Scand. J. Work Environ. Health 2004, 30, 249–252. [Google Scholar] [CrossRef]
- Bruno, C.; Comba, P.; Zona, A. Adverse health effects of fluoro-edenitic fibers: Epidemiological evidence and public health priorities. Ann. N. Y. Acad. Sci. 2006, 1076, 778–783. [Google Scholar] [CrossRef]
- Ballan, G.; Del Brocco, A.; Loizzo, S.; Fabbri, A.; Maroccia, Z.; Fiorentini, C.; Travaglione, S. Mode of action of fibous amphiboles: The case of Biancavilla (Sicily, Italy). Ann. Ist. Super. Sanità 2014, 50, 133–138. [Google Scholar] [CrossRef]
- Magnani, C.; Ferrante, D.; Barone-Adesi, F.; Bertolotti, M.; Todesco, A.; Mirabelli, D.; Terracini, B. Cancer risk after cessation of asbestos exposure: A cohort study of Italian asbestos cement workers. Occup. Environ. Med. 2008, 65, 164–170. [Google Scholar] [CrossRef]
- Bellagamba, S.; Paglietti, F.; Malinconico, S.; Conestabile Della Staffa, B.; De Simone, P.; Lonigro, I. Remediation activities in an Italian Superfund: Case study of an industrial plant in Broni. In Proceedings of the 4th World Congress on New Technologies (NewTech’18), Madrid, Spain, 19–21 August 2018. [Google Scholar] [CrossRef]
- Ministero dell’Ambiente e della Sicurezza Energetica. Iter Delle Bonifiche. 2018. Available online: www.mase.gov.it/sites/default/files/bonifiche/Iter_bonifiche/presentazione_dicembre_2018.pdf (accessed on 21 March 2023).
- Magnani, C.; Mensi, C.; Binazzi, A.; Marsili, D.; Grosso, F.; Ramos-Bonilla, J.P.; Ferrante, D.; Migliore, E.; Mirabelli, D.; Terracini, B.; et al. The Italian experience on the development of mesothelioma registries: A pathway for the other countries to address the negative legacy of asbestos. Int. J. Environ. Res. Public Health 2023, 20, 936. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Chellini, E.; Merler, E.; Pavone, V.; Silvestri, S.; Miligi, L.; Gorini, G.; Bressan, V.; Girardi, P.; Ancona, L.; et al. Italian pool of asbestos workers cohorts: Mortality trends of asbestos-related neoplasms after long time since the first exposure. Occup. Environ. Med. 2017, 74, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Kanarek, M.S. Mesothelioma from chrysotile asbestos: Update. Ann. Epidemiol. 2011, 21, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, P.G.; Calisti, R.; Calabresi, C. Mesoteliomi maligni della pleura da esposizione ambientale ad amianto in Italia. Epidemiol. Prev. 2021, 45, 289–295. [Google Scholar] [CrossRef]
- Caputo, A.; De Santis, M.; Manno, V.; Cauzillo, G.; Bruni, B.M.; Palumbo, L.; Conti, S.; Comba, P. Health impact of asbestos fibres naturally occurring in Mount Pollino area (Basilicata Region, Southern Italy. Epidemiol. Prev. 2018, 42, 142–150. [Google Scholar] [CrossRef]
- Mirabelli, D.; Cadum, E. Mortality among patients with pleural and peritoneal tumors in Alta Valle di Susa. Epidemiol. Prev. 2002, 26, 284–286. [Google Scholar]
- Scarselli, A.; Marinaccio, A.; Iavicoli, S. Ophiolitic outcrops, naturally occurring asbestos exposure and mortality risk from malignant mesothelioma in Calabria (Souther Italy). Public Health 2021, 195, 57–60. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cause of Death | ICD | Males | Females | ||
|---|---|---|---|---|---|
| Cases | SR (90% CI) | Cases | SR (90% CI) | ||
| All MM | C45 | 11,161 | 3.82 (3.76–3.88) | 4285 | 1.10 (1.07–1.13) |
| Pleural MM | C450 | 9084 | 3.10 (3.05–3.16) | 3412 | 0.87 (0.85–0.90) |
| Peritoneal MM | C451 | 409 | 0.14 (0.13–0.15) | 252 | 0.07 (0.06–0.08) |
| MM pericardium | C452 | 6 | 0.0020 (0.0009–0.0048) | 3 | 0.00091 (0.00025–0.0026) |
| MM of other sites | C457 | 282 | 0.097 (0.088–0.11) | 108 | 0.027 (0.023–0.033) |
| MM, unspecified | C459 | 1380 | 0.48 (0.45–0.50) | 510 | 0.13 (0.12–0.14) |
| Age-Class (Years) | Males | Females | ||
|---|---|---|---|---|
| Cases (Percentage of All Cases) | SR (90% CI) | Cases (Percentage of All Cases) | SR (90% CI) | |
| ≤50 | 176 (1.6%) | 0.12 (0.10–1.15) | 90 (2.1%) | 0.05 (0.04–0.07) |
| 51–79 | 7800 (69.9%) | 7.90 (7.75–8.05) | 2607 (60.8%) | 2.26 (2.19–2.34) |
| 80+ | 3185 (28.5%) | 21.80 (21.16–22.47) | 1588 (37.1%) | 6.27 (6.01–6.54) |
| All | 11,161 (100%) | 3.82 (3.76–3.88) | 4285 (100%) | 1.10 (1.07–1.13) |
| Cause of Death | ICD | Males | Females | ||
|---|---|---|---|---|---|
| Cause of Death | ICD | Cases | SR (90% CI) | Cases | SR (90% CI) |
| All MM | C45 | 176 | 0.12 (0.10–0.15) | 90 | 0.05 (0.04–0.07) |
| Pleural MM | C450 | 123 | 0.088 (0.071–0.11) | 54 | 0.03 (0.025–0.049) |
| Peritoneal MM | C451 | 29 | 0.017 (0.011–0.028) | 18 | 0.0080 (0.0000–0.0051) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fazzo, L.; Minelli, G.; De Santis, M.; Ceccarelli, E.; Iavarone, I.; Zona, A. The Epidemiological Surveillance of Mesothelioma Mortality in Italy as a Tool for the Prevention of Asbestos Exposure. Int. J. Environ. Res. Public Health 2023, 20, 5957. https://doi.org/10.3390/ijerph20115957
Fazzo L, Minelli G, De Santis M, Ceccarelli E, Iavarone I, Zona A. The Epidemiological Surveillance of Mesothelioma Mortality in Italy as a Tool for the Prevention of Asbestos Exposure. International Journal of Environmental Research and Public Health. 2023; 20(11):5957. https://doi.org/10.3390/ijerph20115957
Chicago/Turabian StyleFazzo, Lucia, Giada Minelli, Marco De Santis, Emiliano Ceccarelli, Ivano Iavarone, and Amerigo Zona. 2023. "The Epidemiological Surveillance of Mesothelioma Mortality in Italy as a Tool for the Prevention of Asbestos Exposure" International Journal of Environmental Research and Public Health 20, no. 11: 5957. https://doi.org/10.3390/ijerph20115957
APA StyleFazzo, L., Minelli, G., De Santis, M., Ceccarelli, E., Iavarone, I., & Zona, A. (2023). The Epidemiological Surveillance of Mesothelioma Mortality in Italy as a Tool for the Prevention of Asbestos Exposure. International Journal of Environmental Research and Public Health, 20(11), 5957. https://doi.org/10.3390/ijerph20115957