

The Roles of Endorsement and Stigma in Suicidal Ideation and Behavior among Chinese College Students

Abstract
1. Introduction
2. Method and Materials
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analyses
3. Results
3.1. Suicide Risk
3.2. Correlations among Variables
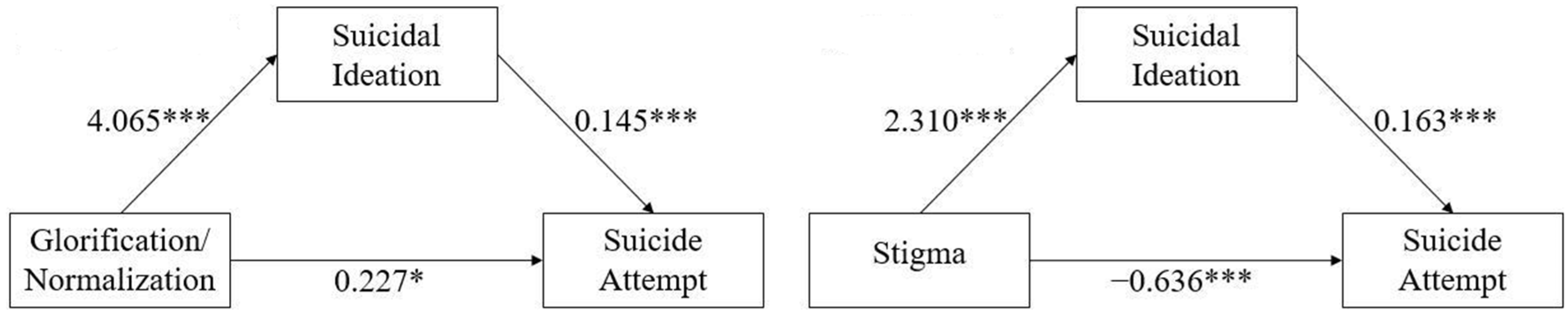
3.3. Mediating Effect of Suicidal Ideation
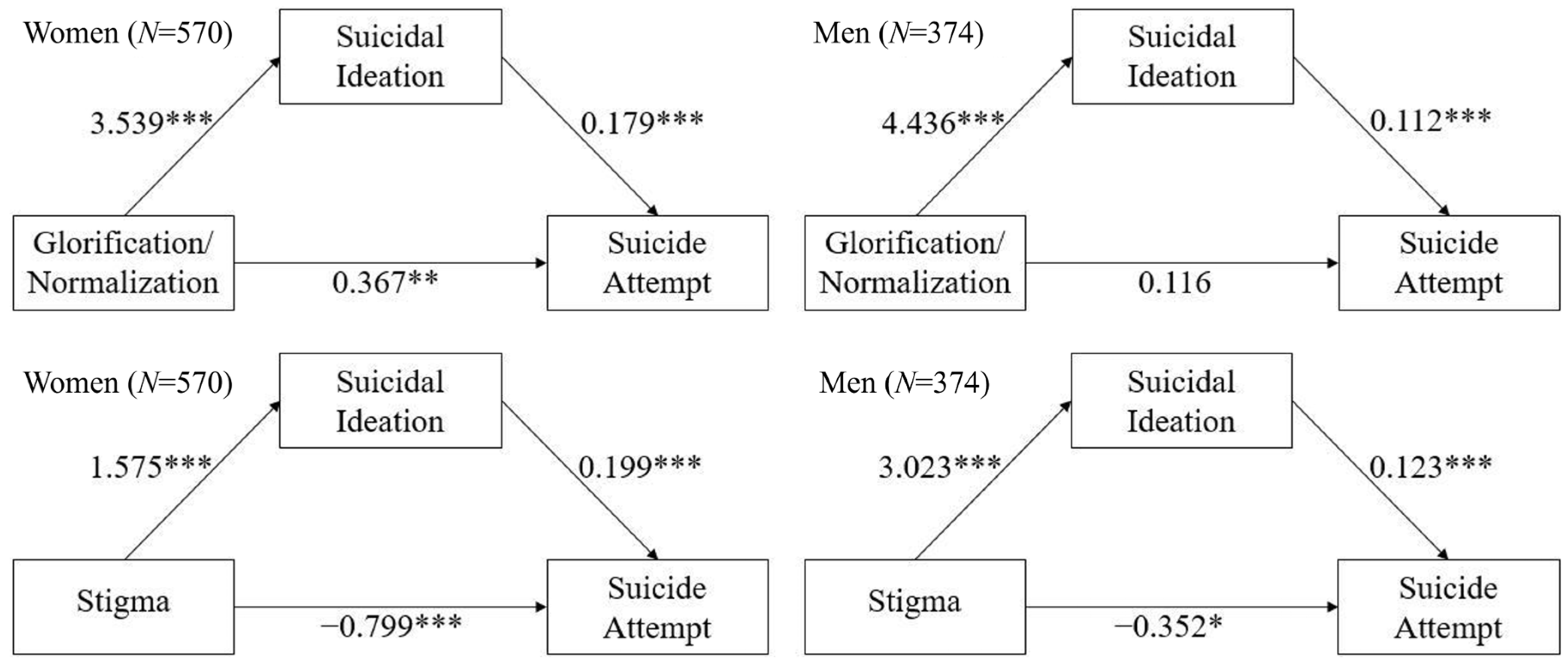
3.4. Gender Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 6 November 2022).
- American Psychiatric Press. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Press: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- National Health Commission of China. China Health Statistics Yearbook 2021; China Union Medical University Press: Beijing, China, 2022; pp. 277–307.
- National Health Commission of China. China Health Statistics Yearbook 2020; China Union Medical University Press: Beijing, China, 2021; pp. 277–307.
- National Health and Family Planning Commission of China. China Health Statistics Yearbook 2011; China Union Medical University Press: Beijing, China, 2012; pp. 287–341.
- Jiang, H.; Niu, L.; Hahne, J.; Hu, M.; Fang, J.; Shen, M.; Xiao, S. Changing of suicide rates in China, 2002–2015. J. Affect. Disord. 2018, 240, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, Y.; Lei, X.; Zhang, D.; Liu, L.; Tang, S.; Chen, L. Prevalence of suicidal ideation in Chinese college students: A meta-analysis. PLoS ONE 2014, 9, e104368. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Saito, E. Risk factors of suicide among Chinese college students: A literature review. China J. Soc. Work. 2022, 15, 22–47. [Google Scholar] [CrossRef]
- Beck, A.T.; Beck, R.; Kovacs, M. Classification of suicidal behaviors: I. Quantifying intent and medical lethality. Am. J. Psychiatry 1975, 132, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Nock, K.K.; Borges, G.; Bromet, E.J.; Alonso, J.; Amgermeyer, N.; Beautrai, A.; Bruffaerts, R.; Chiu, W.T.; De Girolamo, G.; Gluzman, S. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br. J. Psychiatry 2008, 192, 98–105. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M. Differentiating suicide attempters from suicide ideators: A critical frontier for suicidology research. Suicide Life-Threat. Behav. 2014, 44, 1–5. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M. The three-step theory (3ST): A new theory of suicide rooted in the “ideation-to-action” framework. Int. J. Cogn. Ther. 2015, 8, 114–129. [Google Scholar] [CrossRef]
- Tsai, M.; Lari, H.; Saffy, S.; Klonsky, E.D. Examining the Three-Step Theory (3ST) of Suicide in a Prospective Study of Adult Psychiatric Inpatients. Behav. Ther. 2021, 52, 673–685. [Google Scholar] [CrossRef]
- Kim, H.H.; Chun, J. Bullying victimization, school environment, and suicide ideation and plan: Focusing on youth in low-and middle-income countries. J. Adolesc. Health 2020, 66, 115–122. [Google Scholar] [CrossRef]
- Bilsen, J. Suicide and youth: Risk factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.H. Parental overprotection and youth suicide behavior in low-and middle-income countries: A multilevel analysis of cross-national data. Int. J. Public Health 2019, 64, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Ren, Y.; Li, X.; Jiang, Y.; Liu, S.; You, J. Self-compassion and family cohesion moderate the association between suicide ideation and suicide attempts in Chinese adolescents. J. Adolesc. 2020, 79, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Kite, M.E.; Whitley, B.E. Psychology of Prejudice and Discrimination, 3rd ed.; Routledge: London, UK, 2016. [Google Scholar] [CrossRef]
- Stangor, C. The Study of Stereotyping, Prejudice, and Discrimination within Social Psychology: A Quick History of Theory and Research; Psychology Press: New York, NY, USA, 2016; pp. 3–27. [Google Scholar]
- Choi, D.; Noh, G. The influence of social media use on attitude toward suicide through psychological well-being, social isolation, and social support. Inf. Commun. Soc. 2020, 23, 1427–1443. [Google Scholar] [CrossRef]
- Downs, M.F.; Eisenberg, D. Help Seeking and Treatment Use Among Suicidal College Students. J. Am. Coll. Health 2012, 60, 104–114. [Google Scholar] [CrossRef]
- Foo, X.Y.; Alwi, M.; Najib, M.; Ismail, S.I.F.; Ibrahim, N.; Jamil Osman, Z. Religious commitment, attitudes toward suicide, and suicidal behaviors among college students of different ethnic and religious groups in Malaysia. J. Relig. Health 2014, 53, 731–746. [Google Scholar] [CrossRef]
- Gunnell, D.; Harbord, R.; Singleton, N.; Jenkins, R.; Lewis, G. Factors influencing the development and amelioration of suicidal thoughts in the general population: Cohort study. Br. J. Psychiatry 2004, 185, 385–393. [Google Scholar] [CrossRef]
- Joe, S.; Romer, D.; Jamieson, P.E. Suicide Acceptability is Related to Suicide Planning in U.S. Adolescents and Young Adults. Suicide Life-Threat. Behav. 2007, 37, 165–178. [Google Scholar] [CrossRef]
- Zemaitiene, N.; Zaborskis, A. Suicidal tendencies and attitude towards freedom to choose suicide among Lithuanian schoolchildren: Results from three cross-sectional studies in 1994, 1998, and 2002. BMC Public Health 2005, 5, 83. [Google Scholar] [CrossRef][Green Version]
- Bunney, W.E.; Kleinman, A.M.; Pellmar, T.C.; Goldsmith, S.K. Reducing Suicide: A National Imperative; National Academies Press: Washington, DC, USA, 2002. [Google Scholar]
- Zhang, E.Y. Confucian Moral Views on Life and Death: Female Suicide in the Lienüzhuan. Int. J. Chin. Comp. Philos. Med. 2009, 7, 67–86. [Google Scholar] [CrossRef]
- Stack, S. Contributing factors to suicide: Political, social, cultural and economic. Prev. Med. 2021, 152, 106498. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Pirkis, J.; Blood, R.W.; Beautrais, A.; Burgess, P.; Skehan, J. Media guidelines on the reporting of suicide. Crisis 2006, 27, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.T.A.; Hawton, K.; Chen, T.H.H.; Yen, A.M.F.; Chang, J.; Chong, M.; Liu, C.; Lee, Y.; Teng, P.; Chen, L. The influence of media reporting of a celebrity suicide on suicidal behavior in patients with a history of depressive disorder. J. Affect. Disord. 2007, 103, 69–75. [Google Scholar] [CrossRef]
- Phillips, D.P. The influence of suggestion on suicide: Substantive and theoretical implications of the Werther effect. Am. Sociol. Rev. 1974, 39, 340–354. [Google Scholar] [CrossRef]
- Scherr, S.; Reinemann, C. Belief in a Werther Effect: Third-Person Effects in the Perceptions of Suicide Risk for Others and the Moderating Role of Depression. Suicide Life-Threat. Behav. 2011, 41, 624–634. [Google Scholar] [CrossRef]
- Ha, J.; Yang, H. The Werther effect of celebrity suicides: Evidence from South Korea. PLoS ONE 2021, 16, e0249896. [Google Scholar] [CrossRef]
- Amitai, M.; Apter, A. Social aspects of suicidal behavior and prevention in early life: A review. Int. J. Environ. Res. Public Health 2012, 9, 985–994. [Google Scholar] [CrossRef]
- Belfort, E.L.; Mezzacappa, E.; Ginnis, K. Similarities and differences among adolescents who communicate suicidality to others via electronic versus other means: A pilot study. Adolesc. Psychiatry 2012, 2, 258–262. [Google Scholar] [CrossRef]
- Luxton, D.D.; June, J.D.; Fairall, J.M. Social media and suicide: A public health perspective. Am. J. Public Health 2012, 102, S195–S200. [Google Scholar] [CrossRef]
- Liu, X.; Huang, J.; Yu, N.X.; Li, Q.; Zhu, T. Mediation effect of suicide-related social media use behaviors on the association between suicidal ideation and suicide attempt: Cross-sectional questionnaire study. J. Med. Internet Res. 2020, 22, e14940. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, R.; Epstein, S.; Dutta, R.; Ougrin, D. Social media, internet use and suicide attempts in adolescents. Curr. Opin. Psychiatry 2019, 32, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Prentice-Hall, Inc.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Gearing, R.E.; Brewer, K.B.; Cheung, M.; Leung, P.; Chen, W.; He, X. Suicide in China: Community attitudes and stigma. OMEGA-J. Death Dying 2023, 86, 809–832. [Google Scholar] [CrossRef]
- Corrigan, P. How stigma interferes with mental health care. Am. Psychol. 2004, 59, 614. [Google Scholar] [CrossRef] [PubMed]
- Vogel, D.L.; Wade, N.G.; Haake, S. Measuring the self-stigma associated with seeking psychological help. J. Couns. Psychol. 2006, 53, 325–337. [Google Scholar] [CrossRef]
- Vogel, D.L.; Bitman, R.L.; Hammer, J.H.; Wade, N.G. Is stigma internalized? The longitudinal impact of public stigma on self-stigma. J. Couns. Psychol. 2013, 60, 311. [Google Scholar] [CrossRef]
- Cavanagh, J.T.; Carson, A.J.; Sharpe, M.; Lawrie, S.M. Psychological autopsy studies of suicide: A systematic review. Psychol. Med. 2003, 33, 395–405. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Larson, J.E.; Rüsch, N. Self-stigma and the “why try” effect: Impact on life goals and evidence-based practices. World Psychiatry 2009, 8, 75–81. [Google Scholar] [CrossRef]
- Menon, S.; Bhagat, V. The Review Study on Suicidal Risk among Youth/Adolescents, its Prevention and Interventions. Res. J. Pharm. Technol. 2022, 15, 1405–1415. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E., Jr. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Witte, T.K.; Gordon, K.H.; Bender, T.W.; Joiner Jr, T.E. Suicidal desire and the capability for suicide: Tests of the interpersonal-psychological theory of suicidal behavior among adults. J. Consult. Clin. Psychol. 2008, 76, 72. [Google Scholar] [CrossRef]
- Hawton, K. Sex and suicide: Gender differences in suicidal behaviour. Br. J. Psychiatry 2000, 177, 484–485. [Google Scholar] [CrossRef] [PubMed]
- Alothman, D.; Fogarty, A. Global differences in geography, religion and other societal factors are associated with sex differences in mortality from suicide: An ecological study of 182 countries. J. Affect. Disord. 2020, 260, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, Z.; Sun, L.; Sun, Y.; Ye, D. Prevalence of suicide attempts among college students in China: A meta-analysis. PLoS ONE 2015, 10, e0116303. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, C.S.; Heath, P.J.; Vogel, D.L.; Chekay, R. Age differences in public stigma, self-stigma, and attitudes toward seeking help: A moderated mediation model. J. Clin. Psychol. 2019, 75, 2259–2272. [Google Scholar] [CrossRef] [PubMed]
- Oliffe, J.L.; Ogrodniczuk, J.S.; Gordon, S.J.; Creighton, G.; Kelly, M.T.; Black, N.; Mackenzie, C. Stigma in Male Depression and Suicide: A Canadian Sex Comparison Study. Community Ment. Health J. 2016, 52, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Batterham, P.J.; Calear, A.L.; Christensen, H. Correlates of suicide stigma and suicide literacy in the community. Suicide Life-Threat. Behav. 2013, 43, 406–417. [Google Scholar] [CrossRef]
- Batterham, P.J.; Calear, A.L.; Christensen, H. The Stigma of Suicide Scale: Psychometric properties and correlates of the stigma of suicide. Crisis 2013, 34, 13–21. [Google Scholar] [CrossRef]
- Han, J.; Batterham, P.J.; Calear, A.L.; Wu, Y.; Shou, Y.; Van Spijker, B.A. Translation and validation of the Chinese versions of the suicidal ideation attributes scale, stigma of suicide scale, and literacy of suicide scale. Death Stud. 2017, 41, 173–179. [Google Scholar] [CrossRef]
- Van Spijker, B.A.; Batterham, P.J.; Calear, A.L.; Farrer, L.; Christensen, H.; Reynolds, J.; Kerkhof, A.J. The Suicidal Ideation Attributes Scale (SIDAS): Community-based validation study of a new scale for the measurement of suicidal ideation. Suicide Life-Threat. Behav. 2014, 44, 408–419. [Google Scholar] [CrossRef]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The Suicidal Behaviors Questionnaire-Revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Huen, J.M.Y.; Yip, P.S.F.; Osman, A.; Leung, A.N.M. The Suicidal Behaviors Questionnaire-Revised (SBQ-R) and its Chinese version (C-SBQ-R): Further validity testing using the culture, comprehension, and translation bias procedure. Psychol. Assess. 2022, 34, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Reynders, A.; Kerkhof, A.J.; Molenberghs, G.; Van Audenhove, C. Attitudes and stigma in relation to help-seeking intentions for psychological problems in low and high suicide rate regions. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, L.; Dubke, R.; Corrigan, P.W. The specificity of public stigma: A comparison of suicide and depression-related stigma. Psychiatry Res. 2017, 256, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Batterham, P.J.; Calear, A.L.; Ma, J. Seeking professional help for suicidal ideation: A comparison between Chinese and Australian university students. Psychiatry Res. 2018, 270, 807–814. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, Z.; Batterham, P.J.; Han, J. Perceived Suicide Stigma and Associated Factors in Chinese College Students: Trans-lation and Validation of the Stigma of Suicide Attempt Scale and the Stigma of Suicide and Suicide Survivors Scale. Int. J. Environ. Res. Public Health 2021, 18, 3400. [Google Scholar] [CrossRef]
- Vogel, D.L.; Shechtman, Z.; Wade, N.G. The role of public and self-stigma in predicting attitudes toward group counseling. Couns. Psychol. 2010, 38, 904–922. [Google Scholar] [CrossRef]
- Gould, M.S. Suicide and the media. Ann. N. Y. Acad. Sci. 2001, 932, 200–224. [Google Scholar] [CrossRef]
- Guarneri, J.A.; Oberleitner, D.E.; Connolly, S. Perceived Stigma and Self-Stigma in College Students: A Literature Review and Implications for Practice and Research. Basic Appl. Soc. Psychol. 2019, 41, 48–62. [Google Scholar] [CrossRef]
- Robinson, J.; Cox, G.; Bailey, E.; Hetrick, S.; Rodrigues, M.; Fisher, S.; Herrman, H. Social media and suicide prevention: A systematic review. Early Interv. Psychiatry 2016, 10, 103–121. [Google Scholar] [CrossRef]
- Wu, R.; Zhu, H.; Wang, Z.; Jiang, C. A Large Sample Survey of Suicide Risk among University Students in China. BMC Psychiatry 2021, 21, 474. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Su, S.; Jiang, Z.; Guo, S.; Lu, Q.; Liu, L.; Zhao, Y.; Wu, P.; Que, J.; Shi, L.; et al. Prevalence and Risk Factors of Mental Health Symptoms and Suicidal Behavior Among University Students in Wuhan, China During the COVID-19 Pandemic. Front. Psychiatry 2021, 12, 695017. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, K.d.O.M.; de Lisboa, J.L.; Dias, B.M.F.; Ferreira, R.C.; de Araujo Zarzar, P.M.P.; Sampaio, A.A. Suicidal ideation among university students during the COVID-19 pandemic: A rapid systematic review with meta-analysis. Res. Soc. Dev. 2022, 11, e2211426426. [Google Scholar] [CrossRef]
- Jose, P.E. The Merits of Using Longitudinal Mediation. Educ. Psychol. 2016, 51, 331–341. [Google Scholar] [CrossRef]
- John, A.; Pirkis, J.; Gunnell, D.; Appleby, L.; Morrissey, J. Trends in suicide during the COVID-19 pandemic. BMJ 2020, 371, m4352. [Google Scholar] [CrossRef]
- Sher, L.; Peters, J.J. The impact of the COVID-19 pandemic on suicide rates. QJM Int. J. Med. 2020, 113, 707. [Google Scholar] [CrossRef]
- Ryu, S.; Nam, H.J.; Jhon, M.; Lee, J.; Kim, J.; Kim, S. Trends in suicide deaths before and after the COVID-19 outbreak in Korea. PLoS ONE 2022, 17, e0273637. [Google Scholar] [CrossRef]
- Stene-Larsen, K.; Raknes, G.; Engdahl, B.; Qin, P.; Mehlum, L.; Strøm, M.S.; Reneflot, A. Suicide trends in Norway during the first year of the COVID-19 pandemic: A register-based cohort study. Eur. Psychiatry 2022, 65, E26. [Google Scholar] [CrossRef]
- Shi, L.; Que, J.; Lu, Z.; Gong, Y.; Liu, L.; Wang, Y.; Ran, M.; Ravindran, N.; Ravindran, A.V.; Fazel, S.; et al. Prevalence and correlates of suicidal ideation among the general population in China during the COVID-19 pandemic. Eur. Psychiatry 2021, 64, e18. [Google Scholar] [CrossRef]
- Efstathiou, V.; Stefanou, M.; Siafakas, N.; Makris, M.; Tsivgoulis, G.; Zoumpourlis, V.; Spandidos, D.A.; Smyrnis, N.; Rizos, E. Suicidality and COVID-19: Suicidal ideation, suicidal behaviors and completed suicides amidst the COVID-19 pandemic (Review). Exp. Ther. Med. 2022, 23, 107. [Google Scholar] [CrossRef]
- Walther, A.; Eggenberger, L.; Grub, J.; Ogrodniczuk, J.S.; Seidler, Z.E.; Rice, S.M.; Kealy, D.; Oliffe, J.L.; Ehlert, U. Examining the Role of Traditional Masculinity and Depression in Men’s Risk for Contracting COVID-19. Behav. Sci. 2022, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Appleby, L.; et al. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Education Level | Men | Women |
|---|---|---|
| Year 1 | 5.51% (52) | 11.02% (104) |
| Year 2 | 10.91% (103) | 13.88% (131) |
| Year 3 | 16.53% (156) | 18.64% (176) |
| Year 4 | 4.77% (45) | 12.29% (116) |
| Graduate school | 1.91% (18) | 4.34% (41) |
| Total | 39.62% (374) | 60.38% (570) |
| Variables | Mean (±SD) | Percentiles | ||
|---|---|---|---|---|
| 25% | 50% | 75% | ||
| SOSS-Stig | 2.59 (±0.93) | 2.00 | 2.60 | 3.20 |
| SOSS-I/D | 3.84 (±0.87) | 3.67 | 4.00 | 4.33 |
| SOSS-G/N | 2.64 (±0.98) | 2.00 | 2.50 | 3.25 |
| SIDAS | 7.60 (±11.31) | 0.00 | 0.00 | 12.00 |
| SBQ-R | 6.57 (±3.25) | 4.00 | 6.00 | 9.00 |
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. SOSS-Stigma | — | ||||
| 2. SOSS-I/D | 0.34 *** [0.28, 0.39] | — | |||
| 3. SOSS-G/N | −0.13 *** [−0.21, −0.05] | −0.33 *** [−0.40, −0.26] | — | ||
| 4. SIDAS | 0.22 *** [0.15, 0.29] | −0.06 [−0.12, 0.01] | 0.38 *** [0.31, 0.44] | — | |
| 5. SBQ-R | −0.09 ** [−0.16, −0.02] | 0.12 *** [0.06, 0.18] | 0.23 *** [0.17, 0.30] | 0.49 *** [0.43, 0.54] | — |
| Effect | Estimate | p | 95% Confidence Interval | |
|---|---|---|---|---|
| G/N | Direct effect | 0.227 | 0.022 | [−0.032, 0.423] |
| Mediating effect | 0.590 | <0.001 | [0.473, 0.705] | |
| Total effect | 0.818 | <0.001 | [0.610, 1.025] | |
| Stigma | Direct effect | −0.636 | <0.001 | [−0.827, −0.445] |
| Mediating effect | 0.376 | <0.001 | [0.225, 0.520] | |
| Total effect | −0.260 | 0.023 | [−0.484, −0.037] |
| Measures | Women | Men | t | p | Cohen’s d | ||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| SOSS-G/N | 2.59 | 0.91 | 2.71 | 1.08 | 1.73 | 0.084 | 0.120 |
| SOSS-I/D | 3.93 | 0.77 | 3.69 | 0.99 | 4.29 | <0.001 | 0.271 |
| SOSS-Stig | 2.76 | 0.98 | 2.49 | 0.89 | 4.33 | <0.001 | 0.288 |
| SIDAS | 6.58 | 10.35 | 9.16 | 12.49 | 3.46 | <0.001 | 0.225 |
| SBQ-R | 6.88 | 3.32 | 6.10 | 3.07 | 3.61 | <0.001 | 0.244 |
| Effect | Estimate | p | 95% Confidence Interval | |
|---|---|---|---|---|
| G/N Women | Direct effect | 0.367 | 0.006 | [0.107, 0.628] |
| Mediating effect | 0.634 | <0.001 | [0.462, 0.797] | |
| Total effect | 1.002 | <0.001 | [0.708, 1.295] | |
| G/N Men | Direct effect | 0.116 | 0.433 | [−0.174, 0.406] |
| Mediating effect | 0.497 | <0.001 | [0.342, 0.669] | |
| Total effect | 0.612 | <0.001 | [0.321, 0.904] | |
| Stigma Women | Direct effect | −0.799 | <0.001 | [−1.045, −0.552] |
| Mediating effect | 0.313 | <0.001 | [0.080, 0.526] | |
| Total effect | −0.485 | 0.002 | [−0.792, −0.178] | |
| Stigma Men | Direct effect | −0.352 | 0.020 | [−0.648, −0.055] |
| Mediating effect | 0.372 | <0.001 | [0.193, 0.567] | |
| Total effect | 0.021 | 0.901 | [−0.303, 0.344] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyu, S.; Li, Y. The Roles of Endorsement and Stigma in Suicidal Ideation and Behavior among Chinese College Students. Int. J. Environ. Res. Public Health 2023, 20, 877. https://doi.org/10.3390/ijerph20010877
Lyu S, Li Y. The Roles of Endorsement and Stigma in Suicidal Ideation and Behavior among Chinese College Students. International Journal of Environmental Research and Public Health. 2023; 20(1):877. https://doi.org/10.3390/ijerph20010877
Chicago/Turabian StyleLyu, Shunyan, and Yu Li. 2023. "The Roles of Endorsement and Stigma in Suicidal Ideation and Behavior among Chinese College Students" International Journal of Environmental Research and Public Health 20, no. 1: 877. https://doi.org/10.3390/ijerph20010877
APA StyleLyu, S., & Li, Y. (2023). The Roles of Endorsement and Stigma in Suicidal Ideation and Behavior among Chinese College Students. International Journal of Environmental Research and Public Health, 20(1), 877. https://doi.org/10.3390/ijerph20010877