
Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i

 and
and
Abstract
1. Introduction
1.1. Health Literacy and Health Disparities among People with Serious Mental Illness
1.2. Individual and Social Factors Associated with Health Literacy
1.3. Clubhouses: Socially-Oriented Community Mental Health Centers
1.4. The Present Study
2. Materials and Methods
2.1. Overview
2.2. Sample and Procedures
2.3. Measures
2.3.1. Demographics
2.3.2. Self-Efficacy
2.3.3. Stigma
2.3.4. Health Literacy
2.3.5. Social Networks/Health Discussion Partners
2.3.6. Mental and Physical Health
2.4. Data Analysis
3. Results
3.1. Participant Demographic Characteristics and Average Health Literacy
3.2. Social Network Characteristics and Average Health Literacy
3.3. Health Literacy Associations with Individual and Social Factors
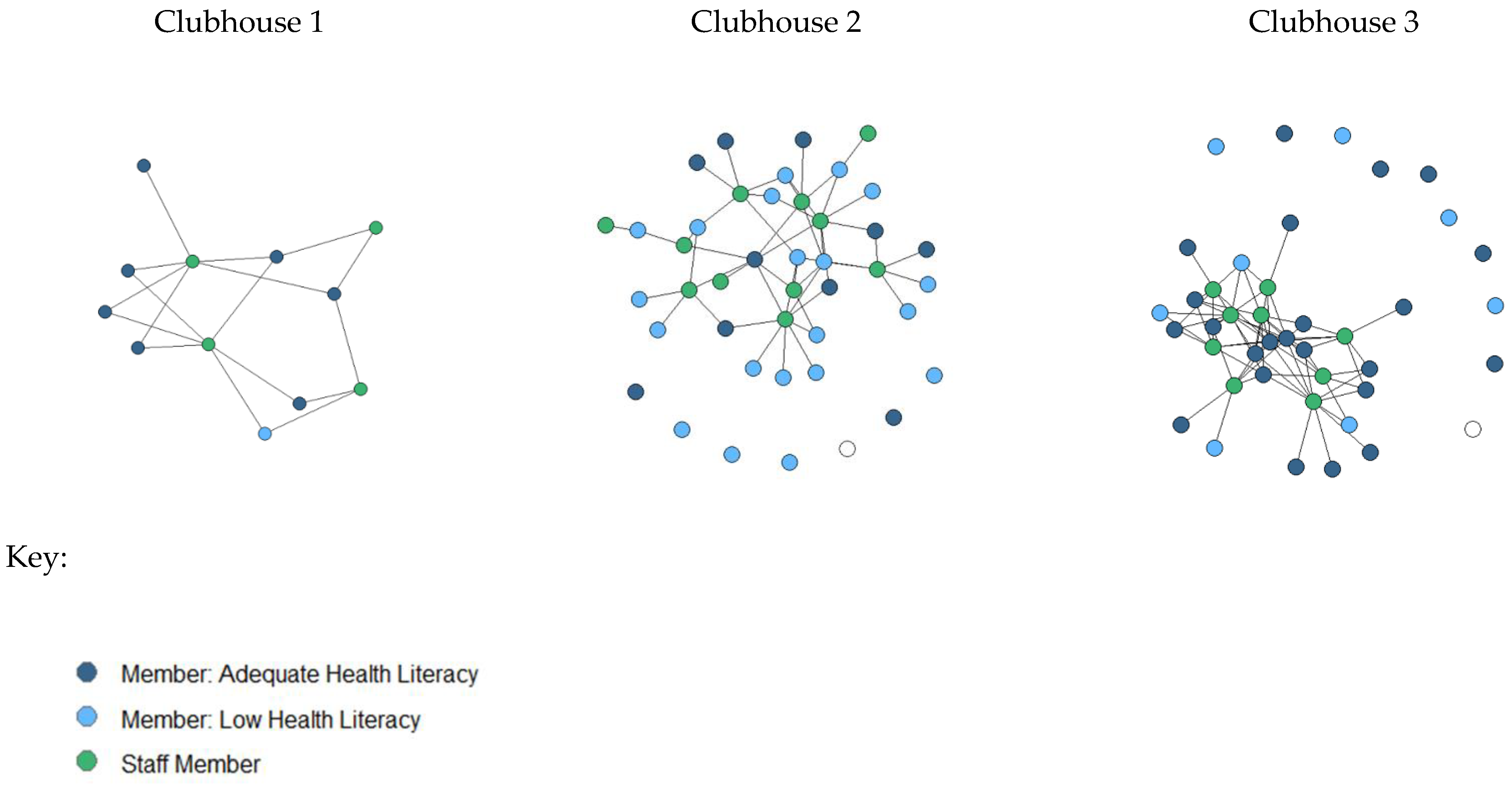
Health Literacy and Staff Health Discussion Partner Social Network Visualizations
4. Discussion
4.1. Associations with Health Literacy Defined by Confidence Filling out Medical Forms
4.2. Associations with Health Literacy Defined by Needing Assistance Reading Pamphlets or Other Written Materials
4.3. Limitations and Opportunities for Future Research
4.4. Potential Utility of This Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, N.H.; Daumit, G.L.; Dua, T.; Aquila, R.; Charlson, F.; Cuijpers, P.; Druss, B.; Dudek, K.; Freeman, M.; Fujii, C.; et al. Excess Mortality in Persons with Severe Mental Disorders: A Multilevel Intervention Framework and Priorities for Clinical Practice, Policy and Research Agendas. World Psychiatry 2017, 16, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Substance Abuse and Mental Health Services Administration Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021; 156p.
- Holt, R.I.G. Cardiovascular disease and severe mental illness. In Key Issues in Mental Health; Sartorius, N., Holt, R.I.G., Maj, M., Eds.; S. Karger AG: Berlin, Germany, 2014; Volume 179, pp. 54–65. ISBN 978-3-318-02603-0. [Google Scholar]
- Newcomer, J.W.; Hennekens, C.H. Severe Mental Illness and Risk of Cardiovascular Disease. JAMA 2007, 298, 1794. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.R.; Macias, C.; Barreira, P.J.; Fisher, W.H.; Hargreaves, W.A.; Harding, C.M. Prevalence, Severity, and Co-Occurrence of Chronic Physical Health Problems of Persons with Serious Mental Illness. Psychiatr. Serv. 2004, 55, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Galon, P.; Graor, C.H. Engagement in Primary Care Treatment by Persons with Severe and Persistent Mental Illness. Arch. Psychiatr. Nurs. 2012, 26, 272–284. [Google Scholar] [CrossRef]
- Ratzan, S.; Parker, R.; Selden, C.; Zorn, M. National Library of Medicine Current Bibliographies in Medicine: Health Literacy; National Institutes of Health: Bethesda, MD, USA, 2000. [Google Scholar]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Clausen, W.; Watanabe-Galloway, S.; Bill Baerentzen, M.; Britigan, D.H. Health Literacy Among People with Serious Mental Illness. Community Ment. Health J. 2016, 52, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Krishan, S.; von Esenwein, S.A.; Druss, B.G. The Health Literacy of Adults with Severe Mental Illness. Psychiatr. Serv. 2012, 63, 397. [Google Scholar] [CrossRef]
- Sentell, T.; Shumway, M. Low Literacy and Mental Illness in a Nationally Representative Sample. J. Nerv. Ment. Dis. 2003, 191, 549–552. [Google Scholar] [CrossRef]
- Kutner, M.; Greenburg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy. NCES 2006-483; U.S. Department of Education: Washington, DC, USA, 2006.
- Clouston, S.A.P.; Manganello, J.A.; Richards, M. A Life Course Approach to Health Literacy: The Role of Gender, Educational Attainment and Lifetime Cognitive Capability. Age Ageing 2017, 46, 493–499. [Google Scholar] [CrossRef]
- Crowe, A.; Mullen, P.R.; Littlewood, K. Self-Stigma, Mental Health Literacy, and Health Outcomes in Integrated Care. J. Couns. Dev. 2018, 96, 267–277. [Google Scholar] [CrossRef]
- Von Wagner, C.; Knight, K.; Steptoe, A.; Wardle, J. Functional Health Literacy and Health-Promoting Behaviour in a National Sample of British Adults. J. Epidemiol. Community Health 2007, 61, 1086–1090. [Google Scholar] [CrossRef] [PubMed]
- Downey, L.V.A.; Zun, L.S. Assessing Adult Health Literacy in Urban Healthcare Settings. J. Natl. Med. Assoc. 2008, 100, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Rompa, D. Functional Health Literacy Is Associated with Health Status and Health-Related Knowledge in People Living with HIV-AIDS. J. Acquir. Immune Defic. Syndr. 2000, 25, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.R. The Prevalence of Limited Health Literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Weekes, C.V. African Americans and Health Literacy: A Systematic Review. ABNF J 2012, 23, 76–80. [Google Scholar]
- Zhou, A.Q.; Lee, H.Y.; Lee, R.M. Who Has Low Health Literacy and Does It Matter for Depression? Findings from Aggregated and Disaggregated Racial/Ethnic Groups. Cult. Divers. Ethn. Minor. Psychol. 2019, 25, 73–81. [Google Scholar] [CrossRef]
- Sentell, T.; Baker, K.K.; Onaka, A.; Braun, K. Low Health Literacy and Poor Health Status in Asian Americans and Pacific Islanders in Hawai’i. J. Health Commun. 2011, 16 (Suppl S3), 279–294. [Google Scholar] [CrossRef]
- Parikh, N.S.; Parker, R.M.; Nurss, J.R.; Baker, D.W.; Williams, M.V. Shame and Health Literacy: The Unspoken Connection. Patient Educ. Couns. 1996, 27, 33–39. [Google Scholar] [CrossRef]
- Levin, S.; Van Laar, C.; Crocker, J. Stigma and Group Inequality: Social Psychological Perspectives; Taylor & Francis Group: Mahwah, NJ, USA, 2005; ISBN 978-1-4106-1705-7. [Google Scholar]
- Bandura, A.; Schunk, D.H. Cultivating Competence, Self-Efficacy, and Intrinsic Interest through Proximal Self-Motivation. J. Personal. Soc. Psychol. 1981, 41, 586–598. [Google Scholar] [CrossRef]
- Drapalski, A.L.; Lucksted, A.; Perrin, P.B.; Aakre, J.M.; Brown, C.H.; DeForge, B.R.; Boyd, J.E. A Model of Internalized Stigma and Its Effects on People with Mental Illness. Psychiatr. Serv. 2013, 64, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Kleim, B.; Vauth, R.; Adam, G.; Stieglitz, R.-D.; Hayward, P.; Corrigan, P. Perceived Stigma Predicts Low Self-Efficacy and Poor Coping in Schizophrenia. J. Ment. Health 2008, 17, 482–491. [Google Scholar] [CrossRef]
- Pasmatzi, E.; Koulierakis, G.; Giaglis, G. Self-Stigma, Self-Esteem and Self-Efficacy of Mentally Ill. Psychiatriki 2016, 27, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L.M.C.; Moore, C.D.; Hensing, G.; Krantz, G.; Staland-Nyman, C. General Self-Efficacy and Its Relationship to Self-Reported Mental Illness and Barriers to Care: A General Population Study. Community Ment. Health J. 2014, 50, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.D.; Arozullah, A.M.; Cho, Y.I. Health Literacy, Social Support, and Health: A Research Agenda. Soc. Sci. Med. 2004, 58, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Sentell, T.; Pitt, R.; Buchthal, O.V. Health Literacy in a Social Context: Review of Quantitative Evidence. HLRP: Health Lit. Res. Pract. 2017, 1, e41–e70. [Google Scholar] [CrossRef] [PubMed]
- Pitt, R.; Davis, T.; Manganello, J.; Massey, P.; Okan, O.; McFarlane, E.; Buchthal, O.; Davis, J.; Arnold, C.; Sentell, T. Health literacy in a social context: A meta-narrative review. In International Handbook of Health Literacy; Policy Press Bristol: Bristol, UK, 2019; pp. 665–688. ISBN 978-1-4473-4452-0. [Google Scholar]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. ‘Distributed Health Literacy’: Longitudinal Qualitative Analysis of the Roles of Health Literacy Mediators and Social Networks of People Living with a Long-Term Health Condition. Health Expect. 2015, 18, 1180–1193. [Google Scholar] [CrossRef]
- Nimmon, L.; Regehr, G. The Complexity of Patients’ Health Communication Social Networks: A Broadening of Physician Communication. Teach. Learn. Med. 2018, 30, 352–366. [Google Scholar] [CrossRef]
- Sentell, T.; Agner, J.; Pitt, R.; Davis, J.; Guo, M.; McFarlane, E. Considering Health Literacy, Health Decision Making, and Health Communication in the Social Networks of Vulnerable New Mothers in Hawai‘i: A Pilot Feasibility Study. Int. J. Environ. Res. Public Health 2020, 17, 2356. [Google Scholar] [CrossRef]
- Sentell, T.L.; Agner, J.L.; Davis, J.; Mannem, S.; Seto, T.B.; Valente, T.W.; Vawer, M.; Taira, D.A. Social Networks in Patients Hospitalized with Preventable Conditions for Heart Disease and Diabetes in Hawai‘i by Health Literacy. Chronic Illn. 2022, 18, 517–531. [Google Scholar] [CrossRef]
- Perry, B.L.; Pescosolido, B.A. Social Network Activation: The Role of Health Discussion Partners in Recovery from Mental Illness. Soc. Sci. Med. 2015, 125, 116–128. [Google Scholar] [CrossRef]
- Davis, L.; Brekke, J. Social Support and Functional Outcome in Severe Mental Illness: The Mediating Role of Proactive Coping. Psychiatry Res. 2014, 215, 39–45. [Google Scholar] [CrossRef]
- Ritsner, M.S.; Arbitman, M.; Lisker, A.; Ponizovsky, A.M. Ten-Year Quality of Life Outcomes among Patients with Schizophrenia and Schizoaffective Disorder II. Predictive Value of Psychosocial Factors. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2012, 21, 1075–1084. [Google Scholar] [CrossRef]
- Meyer, M.S.; Agner, J.; Botero, A.; Cha, T. Mapping Community: A Scoping Review of Clubhouse Members’ Social Networks and Their Impact on Recovery in Mental Illness. Psychiatr. Rehabil. J. 2022. [Google Scholar] [CrossRef]
- Albert, M.; Becker, T.; Mccrone, P.; Thornicroft, G. Social Networks and Mental Health Service Utilisation—A Literature Review. Int. J. Soc. Psychiatry 1998, 44, 248–266. [Google Scholar] [CrossRef]
- McKay, C.; Nugent, K.L.; Johnsen, M.; Eaton, W.W.; Lidz, C.W. A Systematic Review of Evidence for the Clubhouse Model of Psychosocial Rehabilitation. Adm. Policy Ment. Health 2018, 45, 28–47. [Google Scholar] [CrossRef]
- Coniglio, F.D.; Hancock, N.; Ellis, L.A. Peer Support Within Clubhouse: A Grounded Theory Study. Community Ment. Health J. 2012, 48, 153–160. [Google Scholar] [CrossRef]
- Carolan, M.; Onaga, E.; Pernice-Duca, F.; Jimenez, T. A Place to Be: The Role of Clubhouses in Facilitating Social Support. Psychiatr. Rehabil. J. 2011, 35, 125–132. [Google Scholar] [CrossRef]
- Quality Standards | Clubhouse International. Available online: https://clubhouse-intl.org/resources/quality-standards/ (accessed on 29 May 2022).
- Agner, J.; Barile, J.P.; Botero, A.; Cha, T.; Herrera, N.; Kaukau, T.M.; Nakamura, L.; Inada, M. Hawaii Clubhouse Coalition Understanding the Role of Mental Health Clubhouses in Promoting Wellness and Health Equity Using Pilinahā—An Indigenous Framework for Health. Am. J. Community Psychol. 2020, 66, 290–301. [Google Scholar] [CrossRef]
- Agner, J. Understanding the Role of Participation, Mattering, and Reciprocal Social Support in Improving Health-Related Quality of Life among Hawai’i’s Mental Health Clubhouse Members. Ph.D. Thesis, University of Hawai’i at Manoa, Honolulu, HI, USA, 2020. [Google Scholar]
- Herman, S.E.; Onaga, E.; Pernice-Duca, F.; Oh, S.; Ferguson, C. Sense of Community in Clubhouse Programs: Member and Staff Concepts. Am. J. Community Psychol. 2005, 36, 343–356. [Google Scholar] [CrossRef]
- Tanaka, K.; Craig, T.; Davidson, L. Clubhouse Community Support for Life: Staff–Member Relationships and Recovery. J. Psychosoc. Rehabil. Ment. Health 2015, 2, 131–141. [Google Scholar] [CrossRef]
- Kinn, L.G.; Tanaka, K.; Bellamy, C.; Davidson, L. “Pushing the Boat Out”: A Meta-Synthesis of How Members, Staff and Family Experience the Clubhouse Model. Community Ment. Health J. 2018, 54, 1199–1211. [Google Scholar] [CrossRef]
- Wu, Y.; Braun, K.; Onaka, A.T.; Horiuchi, B.Y.; Tottori, C.J.; Wilkens, L. Life Expectancies in Hawai‘i: A Multi-Ethnic Analysis of 2010 Life Tables. Hawaii J. Med. Public Health 2017, 76, 9–14. [Google Scholar]
- Does, S.; Leslie, G.J.; Bell, A.N.; Yamaguchi-Pedroza, K.; Shalbi, K.M.; Shih, M. The Harms of Racial Miscategorization: Comparing Multiracial Individuals’ Well-Being in the Continental U.S. versus Hawai‘i. Cult. Divers. Ethn. Minor. Psychol. 2021. [Google Scholar] [CrossRef]
- Herman, M. Forced to Choose: Some Determinants of Racial Identification in Multiracial Adolescents. Child Dev. 2004, 75, 730–748. [Google Scholar] [CrossRef]
- Townsend, S.S.M.; Markus, H.R.; Bergsieker, H.B. My Choice, Your Categories: The Denial of Multiracial Identities. J. Soc. Issues 2009, 65, 185–204. [Google Scholar] [CrossRef]
- Perreira, K.M.; Telles, E.E. The Color of Health: Skin Color, Ethnoracial Classification, and Discrimination in the Health of Latin Americans. Soc. Sci. Med. 2014, 116, 241–250. [Google Scholar] [CrossRef]
- Kozlowski, A.J.; Cella, D.; Nitsch, K.P.; Heinemann, A.W. Evaluating Individual Change with the Quality of Life in Neurological Disorders (Neuro-QoL) Short Forms. Arch. Phys. Med. Rehabil. 2016, 97, 650–654.e8. [Google Scholar] [CrossRef]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief Questions to Identify Patients with Inadequate Health Literacy. Fam. Med. 2004, 36, 588–594. [Google Scholar]
- Duong, T.V.; Chang, P.W.; Yang, S.-H.; Chen, M.-C.; Chao, W.-T.; Chen, T.; Chiao, P.; Huang, H.-L. A New Comprehensive Short-form Health Literacy Survey Tool for Patients in General. Asian Nurs. Res. 2017, 11, 30–35. [Google Scholar] [CrossRef]
- Mock, M.S.; Sethares, K.A. Concurrent validity and acceptability of health literacy measures of adults hospitalized with heart failure. Appl. Nurs. Res. 2019, 46, 50–56. [Google Scholar] [CrossRef]
- Zotti, P.; Cocchi, S.; Polesel, J.; Cipolat Mis, C.; Bragatto, D.; Cavuto, S.; Conficconi, A.; Costanzo, C.; De Giorgi, M.; Drace, C.A.; et al. Cross-cultural validation of health literacy measurement tools in Italian oncology patients. BMC Health Serv. Res. 2017, 17, 410. [Google Scholar] [CrossRef]
- CDC |Healthy Days Core Module: HRQOL-14 Measure | HRQOL. Available online: https://www.cdc.gov/hrqol/hrqol14_measure.htm (accessed on 5 November 2018).
- Brown, D.S.; Thompson, W.W.; Zack, M.M.; Arnold, S.E.; Barile, J.P. Associations Between Health-Related Quality of Life and Mortality in Older Adults. Prev. Sci. 2015, 16, 21–30. [Google Scholar] [CrossRef]
- Moriarty, D.G.; Zack, M.M.; Kobau, R. The Centers for Disease Control and Prevention’s Healthy Days Measures—Population Tracking of Perceived Physical and Mental Health over Time. Health Qual. Life Outcomes 2003, 1, 37. [Google Scholar] [CrossRef]
- Valente, T.W. Social Networks and Health: Models, Methods, and Applications; Oxford University Press: Oxford, UK, 2010; ISBN 978-0-19-971972-3. [Google Scholar]
- Burt, R.; Meltzer, D.; Seid, M.; Borgert, A.; Chung, J.; Colletti, R.; Dellal, G.; Kahn, S.; Kaplan, H.; Peterson, L.; et al. What’s in a Name Generator? Choosing the Right Name Generators for Social Network Surveys in Healthcare Quality and Safety Research. BMJ Qual. Saf. 2012, 21, 992–1000. [Google Scholar] [CrossRef]
- Blakemore, A.; Hann, M.; Howells, K.; Panagioti, M.; Sidaway, M.; Reeves, D.; Bower, P. Patient Activation in Older People with Long-Term Conditions and Multimorbidity: Correlates and Change in a Cohort Study in the United Kingdom. BMC Health Serv. Res. 2016, 16, 582. [Google Scholar] [CrossRef]
- Dahl, A.M.; Hosler, A.S. Health Literacy and Emergency Department Utilization Among Community Adults with Mental and Chronic Health Conditions. Adv. Emerg. Nurs. J. 2020, 42, 293–303. [Google Scholar] [CrossRef]
- Panagioti, M.; Skevington, S.M.; Hann, M.; Howells, K.; Blakemore, A.; Reeves, D.; Bower, P. Effect of Health Literacy on the Quality of Life of Older Patients with Long-Term Conditions: A Large Cohort Study in UK General Practice. Qual. Life Res. 2018, 27, 1257–1268. [Google Scholar] [CrossRef]
- Angner, E.; Miller, M.J.; Ray, M.N.; Saag, K.G.; Allison, J.J. Health Literacy and Happiness: A Community-Based Study. Soc. Indic. Res. 2009, 95, 325. [Google Scholar] [CrossRef]
- Tokuda, Y.; Doba, N.; Butler, J.P.; Paasche-Orlow, M.K. Health Literacy and Physical and Psychological Wellbeing in Japanese Adults. Patient Educ. Couns. 2009, 75, 411–417. [Google Scholar] [CrossRef]
- Wallace, L.S.; Rogers, E.S.; Roskos, S.E.; Holiday, D.B.; Weiss, B.D. Brief Report: Screening Items to Identify Patients with Limited Health Literacy Skills. J. Gen. Intern. Med. 2006, 21, 874–877. [Google Scholar] [CrossRef]
- Bautista, R.E.D.; Glen, E.T.; Shetty, N.K.; Wludyka, P. The Association between Health Literacy and Outcomes of Care among Epilepsy Patients. Seizure 2009, 18, 400–404. [Google Scholar] [CrossRef]
- Wynia, M.K.; Osborn, C.Y. Health Literacy and Communication Quality in Health Care Organizations. J. Health Commun. 2010, 15, 102–115. [Google Scholar] [CrossRef]
- Amoah, P.A.; Phillips, D.R. Socio-Demographic and Behavioral Correlates of Health Literacy: A Gender Perspective in Ghana. Women Health 2020, 60, 123–139. [Google Scholar] [CrossRef]
- Heizomi, H.; Iraji, Z.; Vaezi, R.; Bhalla, D.; Morisky, D.E.; Nadrian, H. Gender Differences in the Associations Between Health Literacy and Medication Adherence in Hypertension: A Population-Based Survey in Heris County, Iran. Vasc. Health Risk Manag. 2020, 16, 157–166. [Google Scholar] [CrossRef]
- Hayes, R.D.; Chang, C.-K.; Fernandes, A.C.; Begum, A.; To, D.; Broadbent, M.; Hotopf, M.; Stewart, R. Functional Status and All-Cause Mortality in Serious Mental Illness. PLoS ONE 2012, 7, e44613. [Google Scholar] [CrossRef]
- De Mooij, L.D.; Kikkert, M.; Theunissen, J.; Beekman, A.T.F.; de Haan, L.; Duurkoop, P.W.R.A.; Van, H.L.; Dekker, J.J.M. Dying Too Soon: Excess Mortality in Severe Mental Illness. Front. Psychiatry 2019, 10, 855. [Google Scholar] [CrossRef]
- Thornicroft, G. Physical Health Disparities and Mental Illness: The Scandal of Premature Mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef]
- Miller, B.J.; Paschall, C.B.; Svendsen, D.P. Mortality and Medical Comorbidity Among Patients with Serious Mental Illness. Psychiatr. Serv. 2006, 57, 1482–1487. [Google Scholar] [CrossRef]
- Lassetter, J.H.; Clark, L.; Morgan, S.E.; Brown, L.B.; VanServellen, G.; Duncan, K.; Hopkins, E.S. Health Literacy and Obesity Among Native Hawaiian and Pacific Islanders in the United States. Public Health Nurs. 2015, 32, 15–23. [Google Scholar] [CrossRef]
- Sentell, T.; Kennedy, F.; Seto, T.; Vawer, M.; Chiriboga, G.; Valdez, C.; Garrett, L.M.; Paloma, D.; Taira, D. Sharing the Patient Experience: A “Talk Story” Intervention for Heart Failure Management in Native Hawaiians. J. Patient Exp. 2020, 7, 399–407. [Google Scholar] [CrossRef]
- Ellis, J.; Mullan, J.; Worsley, A.; Pai, N. The Role of Health Literacy and Social Networks in Arthritis Patients’ Health Information-Seeking Behavior: A Qualitative Study. Int. J. Fam. Med. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Winch, S.; Ahmed, N.; Rissel, C.; Maxwell, M.; Coutts, J.; Lucas, K. The Reach and Flow of Health Information in Two Aboriginal Communities: A Social Network Analysis. Aust. J. Prim. Health 2017, 23, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Brach, C.; Keller, D.; Hernandez, L.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D. Ten Attributes of Health Literate Health Care Organizations; NAM Perspectives; Discussion Paper; National Academy of Medicine: Washington, DC, USA, 2012. [Google Scholar] [CrossRef]
- Farmanova, E.; Bonneville, L.; Bouchard, L. Organizational Health Literacy: Review of Theories, Frameworks, Guides, and Implementation Issues. INQUIRY 2018, 55, 004695801875784. [Google Scholar] [CrossRef] [PubMed]
- Bohanny, W.; Wu, S.-F.V.; Liu, C.-Y.; Yeh, S.-H.; Tsay, S.-L.; Wang, T.-J. Health Literacy, Self-Efficacy, and Self-Care Behaviors in Patients with Type 2 Diabetes Mellitus. J. Am. Assoc. Nurse Pract. 2013, 25, 495–502. [Google Scholar] [CrossRef]
- Roberts, M.; Callahan, L.; O’Leary, C. Social Media: A Path to Health Literacy. Stud. Health Technol. Inform. 2017, 240, 464–475. [Google Scholar] [CrossRef]
- Narang, S.; Shukla, A.; Sen, B.K. Promoting Health Literacy in India Through Social Networks: Opportunities and Challenges. Lib. Her. 2015, 53, 389. [Google Scholar] [CrossRef]
- Quint, J.J.; Van Dyke, M.E.; Maeda, H.; Worthington, J.K.; Dela Cruz, M.R.; Kaholokula, J.K.; Matagi, C.E.; Pirkle, C.M.; Roberson, E.K.; Sentell, T.; et al. Disaggregating Data to Measure Racial Disparities in COVID-19 Outcomes and Guide Community Response—Hawaii, March 1, 2020–February 28, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1267–1273. [Google Scholar] [CrossRef]
- Rubin, V.; Ngo, D.; Ross, A.; Butler, D.; Nisha, B. Counting a Diverse Nation: Disaggregating Data on Race and Ethnicity to Advance a Culture of Health; PolicyLink: Oakland, CA, USA, 2018. [Google Scholar]
- McDermott, J.F.; Andrade, N.N. People and Cultures of Hawaii: The Evolution of Culture and Ethnicity; University of Hawai’i Press: Honolulu, HI, USA, 2011; ISBN 978-0-8248-6026-4. [Google Scholar]
- Pauker, K.; Meyers, C.; Sanchez, D.T.; Gaither, S.E.; Young, D.M. A Review of Multiracial Malleability: Identity, Categorization, and Shifting Racial Attitudes. Soc. Pers. Psychol. Compass 2018, 12, e12392. [Google Scholar] [CrossRef]
- Sørensen, K.; Karuranga, S.; Denysiuk, E.; McLernon, L. Health Literacy and Social Change: Exploring Networks and Interests Groups Shaping the Rising Global Health Literacy Movement. Glob. Health Promot. 2018, 25, 89–92. [Google Scholar] [CrossRef]


{kind=link}
| Needs Help Reading Instructions or Pamphlets | Confidence Filling Out Medical Forms Independently | ||||
|---|---|---|---|---|---|
| Total (n = 163) | Low Literacy (n = 67) | Adequate Literacy (n = 96) | Low Literacy (n = 91) | Adequate Literacy (n = 72) | |
| Avg (SD) | Avg (SD) | Avg (SD) | Avg (SD) | Avg (SD) | |
| Age | 51.52 (12.52) | 52.01 (13.85) | 51.18 (11.56) | 53.26 (12.26) | 49.32 (12.58) |
| Gender | n (%) | n (%) | n (%) | n (%) | n (%) |
| Male | 83 (50.92%) | 34 (50.75%) | 49 (51.04%) | 52 (57.14%) | 31 (43.06%) |
| Female | 76 (46.63%) | 31 (46.27%) | 45 (46.88%) | 36 (39.56%) | 40 (55.56%) |
| Non-Binary | 1 (0.61%) | 1 (1.49%) | 0 (0.00%) | 1 (1.10%) | 0 (0.00%) |
| Missing or Preferred not to Answer | 3 (1.84%) | 1 (1.49%) | 2 (2.08%) | 2 (2.20%) | 1 (1.39%) |
| Race/Ethnicity * | n (%) | n (%) | n (%) | n (%) | n (%) |
| Native Hawaiian or Pacific Islander | 54 (33.13%) | 20 (29.85%) | 34 (35.42%) | 31 (34.07%) | 23 (31.94%) |
| Filipino | 43 (26.38%) | 21 (31.34%) | 22 (22.92%) | 27 (29.67%) | 16 (22.22%) |
| Japanese | 34 (20.86%) | 14 (20.90%) | 20 (20.83%) | 18 (19.78%) | 16 (22.22%) |
| Chinese | 33 (20.25%) | 16 (23.88%) | 17 (17.71%) | 20 (21.98%) | 13 (18.06%) |
| White ** | 22 (13.50%) | 7 (10.45%) | 15 (15.63%) | 12 (13.19%) | 10 (13.89%) |
| Other | 24 (14.72%) | 9 (13.43%) | 15 (15.63%) | 13 (14.29%) | 11 (15.28%) |
| Missing or Preferred not to Answer | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| Education | n (%) | n (%) | n (%) | n (%) | n (%) |
| Did not complete high school or GED | 22 (13.50%) | 14 (20.90%) | 8 (8.33%) | 13 (14.29%) | 9 (12.50%) |
| Completed high school or obtained GED | 141 (86.50%) | 53 (79.10%) | 88 (91.67%) | 78 (85.71%) | 63 (87.50%) |
| Missing or Preferred not to Answer | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| Avg (SD) | Avg (SD) | Avg (SD) | Avg (SD) | Avg (SD) | |
| Stigma | 54.51 (8.99) | 56.38 (9.32) | 53.20 (8.55) | 54.68 (7.75) | 54.28 (10.39) |
| Self-Efficacy | 44.51 (12.37) | 42.51 (12.73) | 45.90 (11.99) | 41.54 (12.06) | 48.27 (11.81) |
| Number of Physically Unhealthy Days in Past Month | 7.29 (9.84) | 8.61 (10.53) | 6.38 (9.27) | 7.46 (9.84) | 7.08 (9.91) |
| Number of Mentally Unhealthy Days in Past Month | 8.06 (10.33) | 11.06 (11.02) | 5.96 (9.31) | 8.82 (10.23) | 7.08 (10.44) |
| Needs Help Reading Instructions or Pamphlets | Confidence Filling Out Medical Forms Independently | ||||
|---|---|---|---|---|---|
| Total (n = 163) | Low Literacy (n = 67) | Adequate Literacy (n = 96) | Low Literacy (n = 91) | Adequate Literacy (n = 72) | |
| Mean Count (Range) | Mean Count (Range) | Mean Count (Range) | Mean Count (Range) | Mean Count (Range) | |
| Staff Network Mean Size (Range) | 2.20 (0–9) | 1.78 (0–8) | 2.50 (0–9) | 2.16 (0–9) | 2.25 (0–9) |
| Member Network Mean Size (Range) | 0.94 (0–12) | 1.07 (0–12) | 0.85 (0–5) | 0.89 (0–12) | 1.01 (0–5) |
| Outside Network Mean Size (Range) | 1.47 (0–12) | 1.45 (0–12) | 1.49 (0–7) | 1.48 (0–12) | 1.46 (0–7) |
| Adequate Health Literacy | ||||
|---|---|---|---|---|
| Predictor Variables | Never or Rarely Needs Help Reading Instructions or Pamphlets | Quite a Bit or Extremely Confident Filling Out Medical Forms Independently | ||
| OR | 95% CI | OR | 95% CI | |
| Gender ** | ||||
| Non-male | 1.53 | 0.71–3.27 | 2.34 * | 1.10–4.97 |
| Male | ||||
| Age | 0.99 | 0.96–1.02 | 0.97 * | 0.94–1.00 |
| Race/Ethnicity | ||||
| Native Hawaiian or Pacific Islander | 1.49 | 0.57–3.89 | 0.33 * | 0.12–0.88 |
| Japanese | 1.13 | 0.46–2.76 | 1.17 | 0.48–2.80 |
| Filipino | 0.70 | 0.31–1.58 | 0.55 | 0.24–1.29 |
| Chinese | 0.62 | 0.25–1.59 | 0.88 | 0.35–2.23 |
| Other | 1.23 | 0.37–4.06 | 0.64 | 0.24–2.39 |
| White (non-multiracial) | ||||
| Education | ||||
| High School Diploma/GED | 3.74 * | 1.21–11.52 | 0.81 | 0.28–2.36 |
| Did not complete high school/GED | ||||
| Mental Health Not Good in Past 30 Days | 0.97 | 0.93–1.01 | 0.99 | 1.00–1.03 |
| Physical Health Not Good in Past 30 Days | 0.99 | 0.95–1.03 | 1.00 | 0.96–1.04 |
| Stigma | 0.97 | 0.93–1.02 | 1.01 | 0.96–1.05 |
| Self-Efficacy | 1.01 | 0.97–1.04 | 1.07 * | 1.03–1.10 |
| Size of Clubhouse Member Social Network | 0.78 | 0.61–1.02 | 1.00 | 0.78–1.28 |
| Size of Clubhouse Staff Social Network | 1.42 * | 1.13–1.79 | 1.11 | 0.91–1.37 |
| Size of Non-Clubhouse Social Network | 0.95 | 0.76–1.18 | 0.90 | 0.72–1.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agner, J.; Meyer, M.; Kaukau, T.M.; Liu, M.; Nakamura, L.; Botero, A.; Sentell, T. Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i. Int. J. Environ. Res. Public Health 2023, 20, 837. https://doi.org/10.3390/ijerph20010837
Agner J, Meyer M, Kaukau TM, Liu M, Nakamura L, Botero A, Sentell T. Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i. International Journal of Environmental Research and Public Health. 2023; 20(1):837. https://doi.org/10.3390/ijerph20010837
Chicago/Turabian StyleAgner, Joy, Monet Meyer, Tyra Mahealani Kaukau, Maileen Liu, Lisa Nakamura, Adriana Botero, and Tetine Sentell. 2023. "Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i" International Journal of Environmental Research and Public Health 20, no. 1: 837. https://doi.org/10.3390/ijerph20010837
APA StyleAgner, J., Meyer, M., Kaukau, T. M., Liu, M., Nakamura, L., Botero, A., & Sentell, T. (2023). Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i. International Journal of Environmental Research and Public Health, 20(1), 837. https://doi.org/10.3390/ijerph20010837