
Influence of Psychological Factors on Participation and Life Satisfaction in the Context of Travel and Tourism after Spinal Cord Injury


Abstract
1. Introduction
2. Literature Review
2.1. Travel and Tourism Participation of PwSCI
2.2. Self-Determination Theory Applications in Travel Participation of PwSCI
2.3. Life Satisfaction of PwSCI after Travel Participation
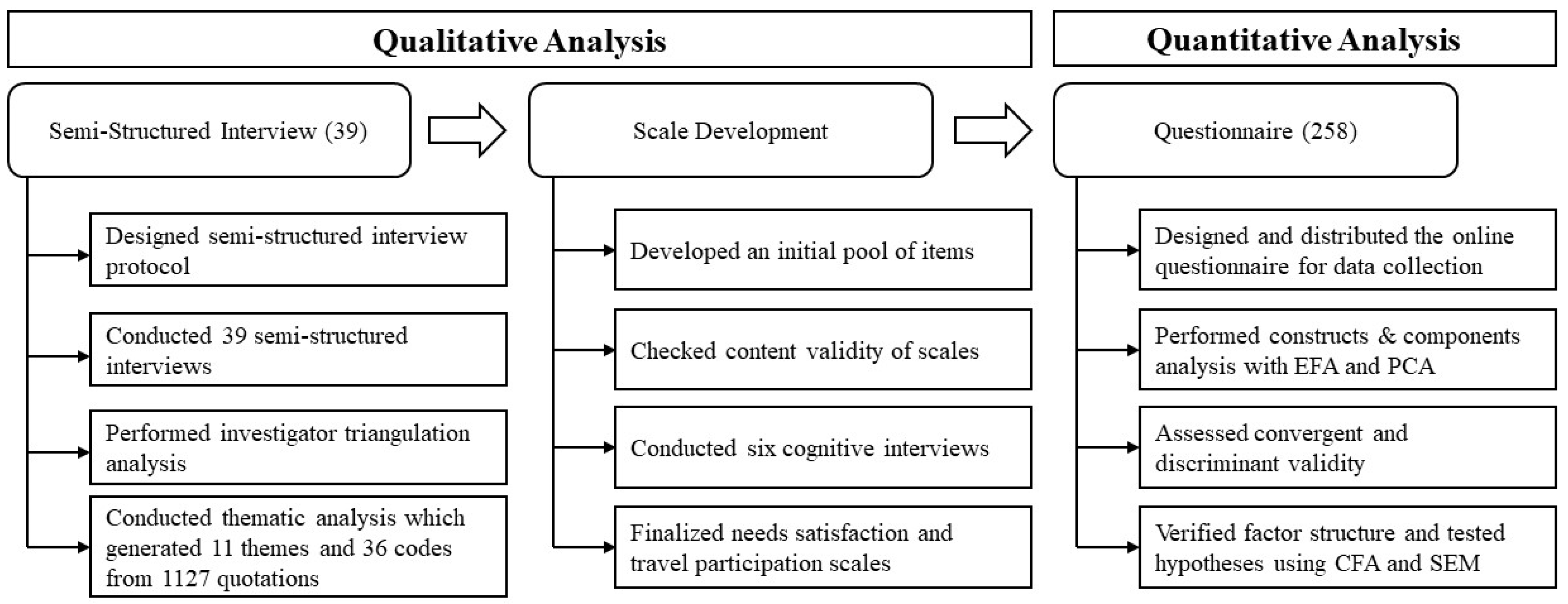
3. Methodology
3.1. Qualitative Analysis
3.2. Quantitative Analysis
4. Results
4.1. Qualitative Analyses
4.2. Quantitative Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jörgensen, S.; Iwarsson, S.; Lexell, J. Secondary health conditions, activity limitations, and life satisfaction in older adults with long-term spinal cord injury. PM&R 2017, 9, 356–366. [Google Scholar]
- Barclay, L.; Lentin, P.; Bourke-Taylor, H.; McDonald, R. The experiences of social and community participation of people with non-traumatic spinal cord injury. Aust. Occup. Ther. J. 2019, 66, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C.; Forwell, S.J.; Jongbloed, L.E.; Backman, C.L. Community participation after spinal cord injury. Arch. Phys. Med. Rehabil. 2007, 88, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Moura, A.; Eusébio, C.; Devile, E. The ‘why’and ‘what for’of participation in tourism activities: Travel motivations of people with disabilities. Curr. Issues Tour. 2022, 3, 1–17. [Google Scholar] [CrossRef]
- Cole, S.; Zhang, Y.; Wang, W.; Hu, C.M. The influence of accessibility and motivation on leisure travel participation of people with disabilities. J. Travel Tour. Mark. 2019, 36, 119–130. [Google Scholar] [CrossRef]
- Chen, C.C.; Petrick, J.F. Health and wellness benefits of travel experiences: A literature review. J. Travel Res. 2013, 52, 709–719. [Google Scholar] [CrossRef]
- Gassaway, J.; Sweatman, M.; Rider, C.; Edens, K.; Weber, M. Therapeutic recreation outcomes during inpatient SCI rehabilitation: Propensity score analysis of SCI rehab data. Ther. Recreat. J. 2019, 53, 99–116. [Google Scholar] [CrossRef]
- Zhang, Y.; Cole, S.; Hirt, E.; Bilgihan, A. Self-determined travel facilitation with mental construal priming. Tour. Manag. 2017, 61, 472–483. [Google Scholar] [CrossRef]
- Glossary of Tourism Terms. Available online: https://www.unwto.org/glossary-tourism-terms (accessed on 18 October 2022).
- World Health Organization. International Classification of Functioning, Disability, and Health. Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 18 October 2022).
- Magasi, S.R.; Heinemann, A.W.; Whiteneck, G.G. Participation following traumatic spinal cord injury: An evidence-based review for research: Report on the national institute on disability and rehabilitation research spinal cord injury measures meeting. J. Spinal Cord Med. 2008, 31, 145–156. [Google Scholar] [CrossRef]
- Scelza, W.M.; Kirshblum, S.C.; Wuermser, L.A.; Ho, C.H.; Priebe, M.M.; Chiodo, A.E. Spinal cord injury medicine. 4. Community reintegration after spinal cord injury. Arch. Phys. Med. Rehabil. 2007, 88, S71–S75. [Google Scholar] [CrossRef]
- Keogh-Hoss, M.; McCormick, B. Survey to identify quality indicators for recreational therapy practice. Annu. Ther. Creat. 2007, 15, 35–44. [Google Scholar]
- Brown, M.; Gordon, W.; Spielman, L.; Haddad, L. Participation by individuals with spinal cord injury in social and recreational activity outside the home. Top. Spinal Cord Inj. Rehabil. 2002, 7, 83–100. [Google Scholar] [CrossRef]
- Wang, P.P.; Badley, E.M.; Gignac, M. Exploring the role of contextual factors in disability models. Disabil. Rehabil. 2006, 28, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Keeves, J.; Gabbe, B.; Arnup, S.; Ekegren, C.; Beck, B. Serious injury in metropolitan and regional Victoria: Exploring travel to treatment and utilization of post-discharge health services by injury type. Int. J. Environ. Res. Public Health 2022, 19, 14063. [Google Scholar] [CrossRef] [PubMed]
- Zawadzka, D.; Ratajczak-Szponik, N.; Ostrowska, B. Interdisciplinary cooperation in technical, medical, and social sciences: A focus on creating accessibility. Int. J. Environ. Res. Public Health 2022, 19, 16669. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.W.; Godbey, G. Reconceptualizing barriers to family leisure. Leis. Sci. 1987, 9, 119–127. [Google Scholar] [CrossRef]
- Moghimehfar, F.; Halpenny, E.A. How do people negotiate through their constraints to engage in pro-environmental behavior? A study of front-country campers in Alberta, Canada. Tour. Manag. 2016, 57, 362–372. [Google Scholar] [CrossRef]
- Michalovic, E.; Rocchi, M.; Sweet, S.N. Motivation and participation in daily and social activities among adults with spinal cord injury: Applying self-determination theory. Disabil. Health J. 2019, 12, 489–494. [Google Scholar] [CrossRef]
- Ahn, J. Role of harmonious and obsessive passions for autonomy, competence, and relatedness support with integrated resort experiences. Curr. Issues Tour. 2020, 23, 756–769. [Google Scholar] [CrossRef]
- Buzinde, C.N. Theoretical linkages between well-being and tourism: The case of self-determination theory and spiritual tourism. Ann. Tour. Res. 2020, 83, 102920. [Google Scholar] [CrossRef]
- Ying, T.; Tan, X.; Ye, S.; Ka, X.; Zhou, Y. Examining tourist mindfulness in museums: The roles of familiarity and motivation. Asia Pac. J. Tour. Res. 2020, 25, 981–996. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Shi, L.; Cole, S.; Chancellor, H.C. Understanding leisure travel motivations of travelers with acquired mobility impairments. Tour. Manag. 2012, 33, 228–231. [Google Scholar] [CrossRef]
- Beard, J.G.; Ragheb, M.G. Measuring leisure motivation. J. Leis. Res. 1983, 15, 219–228. [Google Scholar] [CrossRef]
- Page, S.J.; O’Connor, E.; Peterson, K. Leaving the disability ghetto: A qualitative study of factors underlying achievement motivation among athletes with disabilities. J. Sport Soc. Issues 2001, 25, 40–55. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, M.G.; Kim, J.H.; Min, Y.S.; Kim, C.-H.; Kim, K.T.; Hwang, J.M. Factor analysis affecting degree of depression in family caregivers of patients with spinal cord injury: A cross-sectional pilot study. Int. J. Environ. Res. Public Health 2022, 19, 10878. [Google Scholar] [CrossRef]
- Yau, M.S.; McKercher, B.; Packer, T.L. Traveling with a disability: More than an access issue. Ann. Tour. Res. 2004, 31, 946–960. [Google Scholar] [CrossRef]
- Unger, L.S.; Kernan, J.B. On the meaning of leisure: An investigation of some determinants of the subjective experience. J. Consum. Res. 1983, 9, 381–392. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276. [Google Scholar] [CrossRef]
- Grzeskowiak, S.; Sirgy, M.J.; Lee, D.-J.; Claiborne, C. Housing well-being: Developing and validating a measure. Soc. Indic. Res. 2006, 79, 503–541. [Google Scholar] [CrossRef]
- Lättman, K.; Olsson, L.E.; Friman, M.; Fujii, S. Perceived accessibility, satisfaction with daily travel, and life satisfaction among the elderly. Int. J. Environ. Res. Public Health 2019, 16, 4498. [Google Scholar] [CrossRef] [PubMed]
- Sirgy, M.J.; Lee, D.J. Macro measures of consumer well-being: A critical analysis and a research agenda. J. Macromark. 2006, 26, 27–44. [Google Scholar] [CrossRef]
- Petrick, J.F.; Huether, D. Is travel better than chocolate and wine? The benefits of travel: A special series. J. Travel Res. 2013, 52, 705–708. [Google Scholar] [CrossRef]
- McCabe, S.; Joldersma, T.; Li, C. Understanding the benefits of social tourism: Linking participation to subjective well-being and quality of life. Int. J. Tour. Res. 2010, 12, 761–773. [Google Scholar] [CrossRef]
- Gilbert, D.; Abdullah, J. Holidaytaking and the sense of well-being. Ann. Tour. Res. 2004, 31, 103–121. [Google Scholar] [CrossRef]
- Strauss-Blasche, G.; Muhry, F.; Lehofer, M.; Moser, M.; Marktl, W. Time course of well-being after a three-week resort-based respite from occupational and domestic demands: Carry-over, contrast and situation effects. J. Leis. Res. 2004, 36, 293–309. [Google Scholar] [CrossRef]
- Smith, R.W. Leisure of disable tourists: Barriers to participation. Ann. Tour. Res. 1987, 14, 376–389. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, Y.; Wang, W.; Cole, S. Contribution of travel participation to social integration and life satisfaction after spinal cord injury. Disabil. Health J. 2021, 14, 101167. [Google Scholar] [CrossRef]
- Friese, S. Qualitative Data Analysis with ATLAS. Ti; Sage Publications: Newbury Park, CA, USA, 2019. [Google Scholar]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: Newbury Park, CA, USA, 2021. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Handbook of Self-Determination Research; University Rochester Press: Rochester, NY, USA, 2004. [Google Scholar]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate data analysis 6th Edition. Pearson Prentice Hall. New Jersey. humans: Critique and reformulation. J. Abnorm. Psychol. 2006, 87, 49–74. [Google Scholar]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics; Sage Publications: Newbury Park, CA, USA, 1981; pp. 39–50. [Google Scholar]
- National Spinal Cord Injury Statistical Center. Traumatic Spinal Cord Injury Facts and Figures at a Glance. Available online: https://www.nscisc.uab.edu/public/Facts%20and%20Figures%202022%20-%20English%20Final.pdf (accessed on 23 October 2022).
- Bearden, W.O.; Sharma, S.; Teel, J.E. Sample size effects on chi square and other statistics used in evaluating causal models. J. Mark. Res. 1982, 19, 425–430. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Forsyth, R.; Jarvis, S. Participation in Childhood; Wiley Online Library: New York, NY, USA, 2002; pp. 277–279. [Google Scholar]
- Zhang, Y.; Cole, S.; Ricci, P.; Gao, J. Context-based leisure travel facilitation among people with mobility challenges: A self-determination theory approach. J. Travel Res. 2019, 58, 42–62. [Google Scholar] [CrossRef]
- Pagan, R. How important are holiday trips in preventing loneliness? Evidence for people without and with self-reported moderate and severe disabilities. Curr. Issues Tour. 2020, 23, 1394–1406. [Google Scholar] [CrossRef]
- Blichfeldt, B.S.; Nicolaisen, J. Disabled travel: Not easy, but doable. Curr. Issues Tour. 2011, 14, 79–102. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. A self-determination theory perspective on social, institutional, cultural, and economic supports for autonomy and their importance for well-being. In Human Autonomy in Cross-Cultural Context; Springer: New York, NY, USA, 2011; pp. 45–64. [Google Scholar]
- Darcy, S.; Burke, P.F. On the road again: The barriers and benefits of automobility for people with disability. Transp. Res. Part A Policy Pract. 2018, 107, 229–245. [Google Scholar] [CrossRef]
- Jörgensen, S.; Svedevall, S.; Magnusson, L.; Martin Ginis, K.A.; Lexell, J. Associations between leisure time physical activity and cardiovascular risk factors among older adults with long-term spinal cord injury. Spinal Cord 2019, 57, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.; Deci, E.L.; Zhao, H.; Wang, W. How environmental and psychological factors interact with travel participation after spinal cord injury. Rehabil. Psychol. 2022, 67, 152–161. [Google Scholar] [CrossRef]
- McKercher, B.; Darcy, S. Re-conceptualizing barriers to travel by people with disabilities. Tour. Manag. Perspect. 2018, 26, 59–66. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The support of autonomy and the control of behavior. J. Personal. Soc. Psychol. 1987, 53, 1024. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Person | Gender 1 | Age | Years Since Injury | Work Status | Race | Annual Household Income | Assistive Device 2 |
|---|---|---|---|---|---|---|---|
| PSCI01 | M | 53 | 35 | NA | NA | $40,000–$59,999 | WC |
| PSCI02 | M | 64 | 24 | NA | Asian, Pacific Islander | <$20,000 | WC |
| PSCI03 | M | 50 | 50 | NA | White, Caucasian | $80,000–$99,999 | WC |
| PSCI04 | F | 73 | 5 | NA | White, Caucasian | >$100,000 | C/W |
| PSCI05 | F | 59 | 35 | Retired | Native American | <$20,000 | WC |
| PSCI06 | M | 57 | 40 | Part time employed | White, Caucasian | $40,000–$59,999 | PC/S |
| PSCI07 | F | 56 | 36 | NA | White, Caucasian | >$100,000 | WC |
| PSCI08 | M | 55 | 5 | NA | Multiracial | >$100,000 | WC |
| PSCI09 | M | 66 | 29 | NA | Multiracial | >$100,000 | WC |
| PSCI10 | M | 68 | 40 | NA | White, Caucasian | >$100,000 | WC |
| PSCI11 | M | 67 | 40 | Retired | White, Caucasian | $40,000–$59,999 | WC |
| PSCI12 | F | 41 | 15 | On disability | Black, African American | <$20,000 | WC |
| PSCI13 | F | 56 | 19 | Full time employed | White, Caucasian | >$100,000 | WC |
| PSCI14 | F | 70 | 70 | Retired | White, Caucasian | $20,000–$39,999 | PC/S |
| PSCI15 | F | 37 | 17.5 | Full time employed | White, Caucasian | $20,000–$39,999 | PC/S |
| PSCI16 | M | 50 | 33 | On disability | White, Caucasian | <$20,000 | WC |
| PSCI17 | F | 43 | 26 | Self-employed | White, Caucasian | $20,000–$39,999 | WC |
| PSCI18 | M | 67 | 15 | On disability | Hispanic | <$20,000 | PC/S |
| PSCI19 | M | 54 | 32 | On disability | White, Caucasian | <$20,000 | PC/S |
| PSCI20 | F | 58 | 15 | Self-employed | White, Caucasian | $20,000–$39,999 | WC |
| PSCI21 | M | 24 | 5 | Full time employed | White, Caucasian | $40,000–$59,999 | WC |
| PSCI22 | M | 63 | 4 | Full time employed | White, Caucasian | >$100,000 | NA |
| PSCI23 | M | 30 | 2 | On disability | White, Caucasian | <$20,000 | WC |
| PSCI24 | M | 24 | 3.3 | Part time employed | White, Caucasian | <$20,000 | WC |
| PSCI25 | F | 61 | 45 | Retired | White, Caucasian | $40,000–$59,999 | WC |
| PSCI26 | M | 48 | 20 | On disability | White, Caucasian | $20,000–$39,999 | NA |
| PSCI27 | F | 54 | 26 | On disability | White, Caucasian | $20,000–$39,999 | WC |
| PSCI28 | M | 52 | 30 | On disability | Black, African American | <$20,000 | PC/S |
| PSCI29 | M | 58 | 41 | Full time employed | White, Caucasian | >$100,000 | WC |
| PSCI30 | M | 49 | 10 | On disability | Hispanic | <$20,000 | WC/PC/S |
| PSCI31 | M | 64 | 46 | On disability | White, Caucasian | $20,000–$39,999 | WC |
| PSCI32 | M | 22 | 4 | Part time employed | White, Caucasian | $60,000–$79,999 | WC |
| PSCI33 | M | 60 | 11 | On disability/Retired | Multiracial | $40,000–$59,999 | PC/S |
| PSCI34 | M | 59 | 30 | Part time employed | White, Caucasian | $80,000–$99,999 | PC/S |
| PSCI35 | M | 65 | 12 | On disability | White, Caucasian | $80,000–$99,999 | WC |
| PSCI36 | M | 68 | 42 | Retired | White, Caucasian | >$100,000 | WC |
| PSCI37 | M | 72 | 36 | Retired | White, Caucasian | $40,000–$59,999 | PC/S |
| PSCI38 | F | 25 | 22 | Full time employed | White, Caucasian | $20,000–$39,999 | WC |
| PSCI39 | M | 51 | 25 | Full time employed | White, Caucasian | $60,000–$79,999 | WC |
| Measured Variables and Measurements | Covariance | Mean | Std. Deviation | CR | AVE | Cronbach’s α | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Competence | 0.879 | 0.479 | 0.721 | ||||||||
| Travel knowledge | When it comes to travel, I know what works and what does not work for me. | 0.638 | 4.28 | 0.799 | 0.752 | 0.479 | |||||
| I am aware of things/situations I do not have control over during travel. | 0.21 | 0.755 | 4.09 | 0.869 | |||||||
| I know the right questions to ask for travel service personnel to meet my needs. | 0.233 | 0.239 | 0.684 | 4.03 | 0.827 | ||||||
| I make sure I voice my concerns when travel services fail to meet my needs. | 0.092 | 0.216 | 0.134 | 0.821 | 4.06 | 0.906 | |||||
| Travel capacity | (Reversed) I sometimes do not know what to do when travel services fail to meet my needs | 1.356 | 3.16 | 1.160 | 0.813 | 0.522 | |||||
| I am quite experienced at traveling long distances. | 0.309 | 1.299 | 3.72 | 1.140 | |||||||
| I am good at problem solving during travel. | 0.424 | 0.286 | 0.577 | 4.15 | 0.760 | ||||||
| I know where to find helpful information for my trips. | 0.425 | 0.439 | 0.298 | 0.913 | 3.75 | 0.960 | |||||
| Autonomy | 0.903 | 0.540 | 0.776 | ||||||||
| Decision autonomy | I feel free to decide for myself when and to where I want to travel. | 1.245 | 3.88 | 1.116 | 0.854 | 0.544 | |||||
| I feel I am in complete control while traveling regardless of whether the service/place is accessible to me. | 0.428 | 1.216 | 2.90 | 1.103 | |||||||
| I feel free to choose what to do when I travel. | 0.665 | 0.631 | 1.123 | 3.65 | 1.060 | ||||||
| I generally feel I am in control of my own travel. | 0.508 | 0.43 | 0.388 | 0.865 | 3.86 | 0.930 | |||||
| I feel I can pretty much be myself when traveling. | 0.429 | 0.386 | 0.45 | 0.404 | 0.998 | 3.85 | 0.999 | ||||
| Having Control | (Reversed) I need to rely on others to make travel plans for me. | 1.309 | 3.83 | 1.14 | 0.774 | 0.533 | |||||
| Doing research and planning ahead of the trip makes me feel in control of my own travel. | 0.143 | 0.402 | 4.36 | 0.634 | |||||||
| I feel free to express my own ideas when making decisions about my travel. | 0.217 | 0.181 | 0.403 | 4.36 | 0.635 | ||||||
| Relatedness | 0.923 | 0.524 | 0.765 | ||||||||
| Connection | I feel comfortable asking for help from strangers during travel. | 1.198 | 3.55 | 1.094 | 0.787 | 0.516 | |||||
| I am happy to meet new people during travel. | 0.256 | 0.592 | 4.21 | 0.769 | |||||||
| I feel connected to people with whom I travel. | 0.196 | 0.262 | 0.704 | 4.01 | 0.839 | ||||||
| I feel respected by people I meet on a trip. | 0.35 | 0.294 | 0.326 | 0.753 | 3.72 | 0.868 | |||||
| I feel I can easily connect with the people I meet during travel. | 0.362 | 0.291 | 0.29 | 0.434 | 0.655 | 3.85 | 0.809 | ||||
| Easy to find help | There is someone around to help me travel to places. | 1.231 | 3.82 | 1.110 | 0.789 | 0.557 | |||||
| I have someone to discuss my travel plans with if needed. | 0.506 | 0.844 | 4.11 | 0.920 | |||||||
| (Reversed) It is difficult for me to find the help I need to travel long distances. | 0.317 | 0.29 | 1.231 | 3.48 | 1.110 | ||||||
| Social comfort | (Reversed) People I meet during travel often do not engage with me. | 1.007 | 3.65 | 1.004 | 0.753 | 0.505 | |||||
| (Reversed) I feel disappointed when people I meet on a trip treat me poorly. | 0.33 | 1.307 | 2.45 | 1.143 | |||||||
| (Reversed) During travel, I often feel people are talking around me but not to me. | 0.41 | 0.401 | 1.141 | 3.39 | 1.068 | ||||||
| Travel Participation | 0.887 | 0.499 | 0.710 | ||||||||
| Travel to accessible destination | (Reversed) I try to limit the number of trips I take due to environmental or service barriers for travelers with disabilities. | 1.831 | 3.38 | 1.353 | 0.793 | 0.435 | |||||
| (Reversed) I only travel to places that I know are accessible to me. | 0.775 | 1.683 | 2.59 | 1.297 | |||||||
| (Reversed) I avoid traveling to places where I have never been before. | 0.442 | 0.272 | 1.041 | 3.95 | 1.020 | ||||||
| (Reversed) I mostly travel to places where I do not have to stay overnight. | 0.476 | 0.445 | 0.386 | 1.399 | 3.69 | 1.182 | |||||
| (Reversed) I avoid flying in airplanes when I travel to places | 0.64 | 0.375 | 0.238 | 0.41 | 1.649 | 3.19 | 1.284 | ||||
| Travel as I want | I have been traveling as often as I can. | 1.649 | 3.19 | 1.284 | 0.818 | 0.606 | |||||
| My level of participation in travel so far is how I want it. | 0.248 | 1.606 | 3.13 | 1.267 | |||||||
| I feel I have been traveling the way I want. | 0.362 | 0.81 | 1.596 | 3.21 | 1.263 | ||||||
| Life Satisfaction | 0.917 | 0.691 | 0.833 | ||||||||
| Life satisfaction | In most ways my life is close to my ideal. | 3.735 | 3.95 | 1.933 | |||||||
| The conditions of my life are excellent. | 2.622 | 3.167 | 4.13 | 1.780 | |||||||
| I am satisfied with my life. | 2.62 | 2.328 | 3.263 | 4.64 | 1.806 | ||||||
| Thus far, I have gotten the important things I want in life. | 1.9 | 1.844 | 2.069 | 3.113 | 4.81 | 1.764 | |||||
| If I could live my life over, I would change almost nothing. | 2.087 | 1.767 | 2.004 | 1.764 | 3.989 | 3.37 | 1.997 | ||||
| Com1 | Com2 | Auto1 | Auto2 | Rela1 | Rela2 | Rela3 | TP1 | TP2 | LS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Com1 | 0.723 | |||||||||
| Com2 | 0.411 ** | 0.660 | ||||||||
| Auto1 | 0.503 ** | 0.276 ** | 0.738 | |||||||
| Auto2 | 0.400 ** | 0.389 ** | 0.431 ** | 0.730 | ||||||
| Rela1 | 0.444 ** | 0.247 ** | 0.406 ** | 0.306 ** | 0.719 | |||||
| Rela2 | 0.242 ** | 0.191 * | 0.235 ** | 0.197 * | 0.359 ** | 0.746 | ||||
| Rela3 | 0.237 ** | 0.186 * | 0.257 ** | 0.144 * | 0.351 ** | 0.162 | 0.711 | |||
| TP1 | 0.474 ** | 0.213 ** | 0.387 ** | 0.255 ** | 0.343 ** | 0.269 ** | 0.253 ** | 0.660 | ||
| TP2 | 0.328 ** | 0.148 * | 0.487 ** | 0.140 * | 0.264 ** | 0.316 ** | 0.170 ** | 0.373 ** | 0.778 | |
| LS | 0.413 ** | 0.128 * | 0.370 ** | 0.162 * | 0.420 ** | 0.278 ** | 0.174 ** | 0.202 ** | 0.370 ** | 0.832 |
| Variables | Category | Frequency (Percent, %) | Variables | Category | Frequency (Percent, %) |
|---|---|---|---|---|---|
| Age (y) | 21–30 y | 16 (6.2%) | Family Household Income | Less than $25,000 | 38 (14.7%) |
| 31–40 y | 90 (22.5%) | $25,000–$49,999 | 49 (19%) | ||
| 41–50 y | 42 (16.3%) | $50,000–$74,999 | 47 (18.2%) | ||
| 51–60 y | 41 (15.8%) | $75,000–$99,999 | 45 (17.4%) | ||
| >60 y | 52 (20.2%) | $100,000–$124,999 | 21 (8.1%) | ||
| Declined, Unknown | 49 (19.0%) | $125,000 and above | 34 (13.2%) | ||
| Age at Injury (y) | 11–20 y | 66 (25.6%) | Declined, Unknown | 24 (9.3%) | |
| 21–30 y | 88 (34.1%) | Marital Status | Never married (Single) | 73 (28.3%) | |
| 31–40 y | 38 (14.7%) | Married | 125 (48.4%) | ||
| 41–50 y | 24 (9.3%) | Divorced | 26 (10.1%) | ||
| >50 y | 37 (14.3%) | Separated | 4 (1.6%) | ||
| Declined, Unknown | 5 (1.9%) | Widow | 5 (1.9%) | ||
| Gender | Men | 174 (67.4%) | Living with Significant Other/Partner | 23 (8.9%) | |
| Women | 84 (32.6%) | ||||
| Other, Unknown | 0 (0.00%) | Declined, Unknown | 2 (0.8%) | ||
| Race/Ethnicity | White, Caucasian | 215 (83.3%) | Level of Education | High school or GED or less | 35 (13.6%) |
| Black, African American | 17 (6.6%) | Associate degree | 44 (17.1%) | ||
| American Indian, Alaska Native | 1 (0.4%) | Bachelor’s degree | 69 (26.7%) | ||
| Asian, Pacific Islander | 10 (3.9%) | Graduate degree or above | 55 (21.3%) | ||
| Other Race, Multiracial | 14 (5.4%) | Declined, Unknown | 55 (21.3%) | ||
| Declined, Unknown | 1 (0.4%) | Total | 258 (100%) | ||
| Χ2 | df | p | RMSEA | GFI | CFI | TLI | |
|---|---|---|---|---|---|---|---|
| Suggested value * | <0.08 | >0.95 | >0.95 | >0.95 | |||
| CFA Model | 150.548 | 67.0 | 0.000 | 0.073 | 0.914 | 0.932 | 0.908 |
| Hypothesis Model | 155.556 | 70.0 | 0.000 | 0.072 | 0.912 | 0.931 | 0.910 |
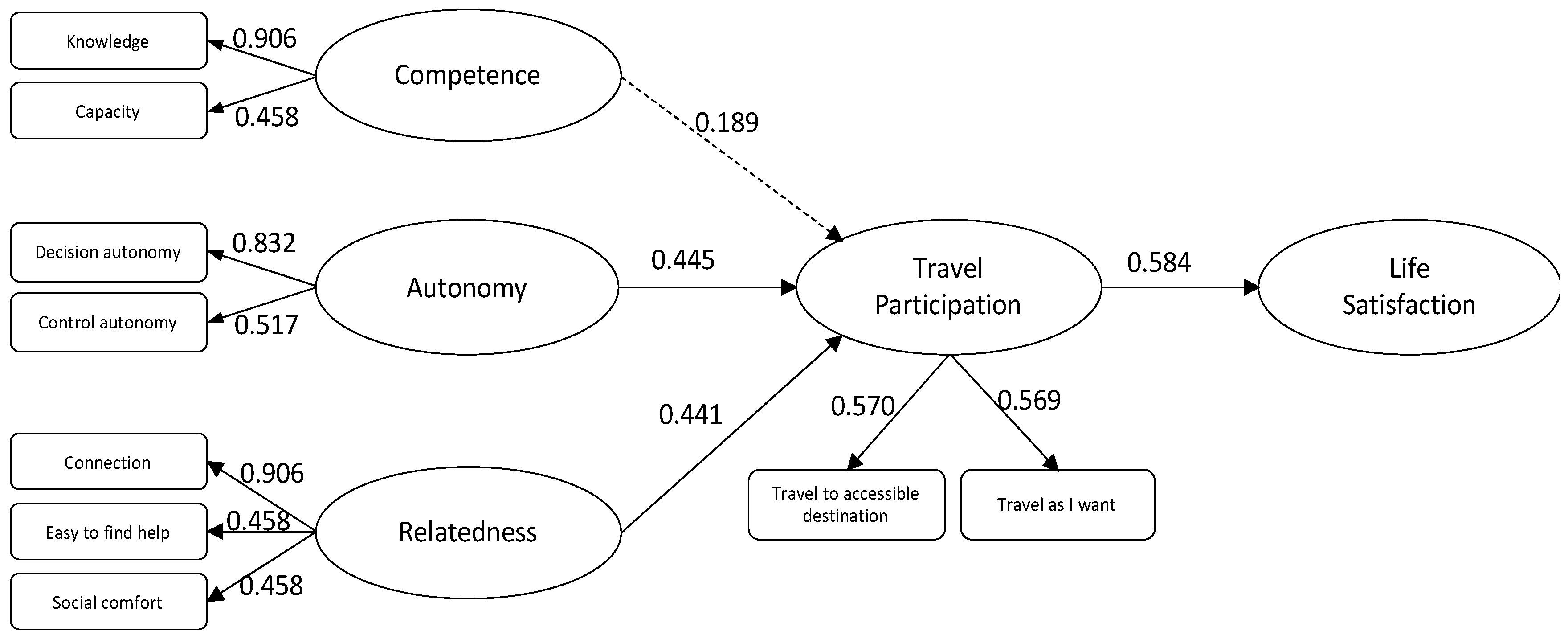
| Pathways | β | Std. Err | z-value | p (>|z|) | Test Results |
|---|---|---|---|---|---|
| Competence → TP | 0.189 | 0.103 | 1.258 | 0.208 | H1: Rejected |
| Relatedness → TP | 0.445 | 0.124 | 2.526 | 0.012 * | H2: Accepted |
| Autonomy → TP | 0.441 | 0.151 | 2.749 | 0.006 ** | H3: Accepted |
| TP → LS | 0.584 | 0.336 | 6.405 | 0.000 *** | H4: Accepted |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hua, C.; Cole, S. Influence of Psychological Factors on Participation and Life Satisfaction in the Context of Travel and Tourism after Spinal Cord Injury. Int. J. Environ. Res. Public Health 2023, 20, 516. https://doi.org/10.3390/ijerph20010516
Hua C, Cole S. Influence of Psychological Factors on Participation and Life Satisfaction in the Context of Travel and Tourism after Spinal Cord Injury. International Journal of Environmental Research and Public Health. 2023; 20(1):516. https://doi.org/10.3390/ijerph20010516
Chicago/Turabian StyleHua, Chenggang, and Shu Cole. 2023. "Influence of Psychological Factors on Participation and Life Satisfaction in the Context of Travel and Tourism after Spinal Cord Injury" International Journal of Environmental Research and Public Health 20, no. 1: 516. https://doi.org/10.3390/ijerph20010516
APA StyleHua, C., & Cole, S. (2023). Influence of Psychological Factors on Participation and Life Satisfaction in the Context of Travel and Tourism after Spinal Cord Injury. International Journal of Environmental Research and Public Health, 20(1), 516. https://doi.org/10.3390/ijerph20010516