
Effects of Single-Task, Dual-Task and Analogy Training during Gait Rehabilitation of Older Adults at Risk of Falling: A Randomized Controlled Trial



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Intervention
2.4. Procedures
2.5. Outcome Assessments
2.6. Sampling and Randomization
2.7. Data Processing
3. Results
3.1. Participants’ Characteristics at Baseline
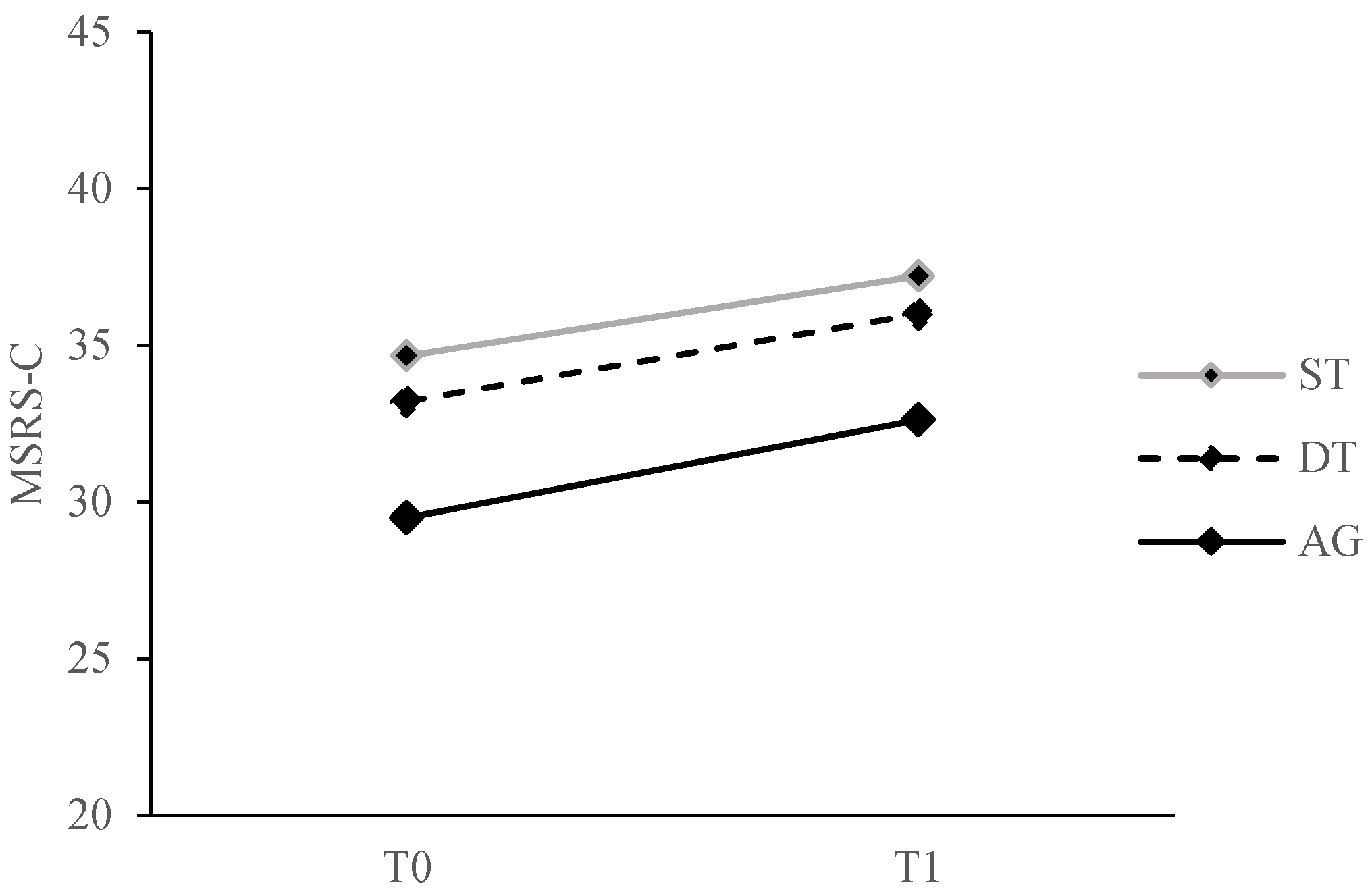
3.2. Intervention Effects on the Primary Outcome
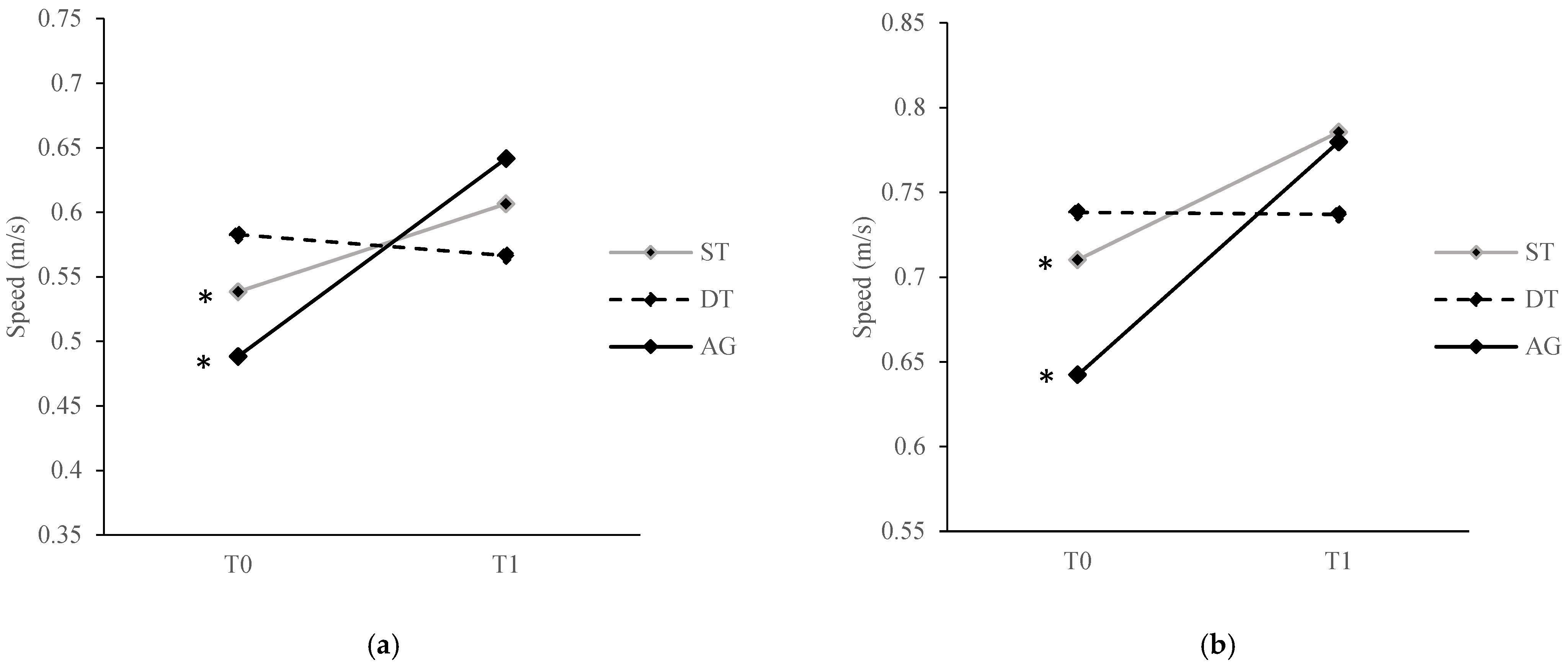
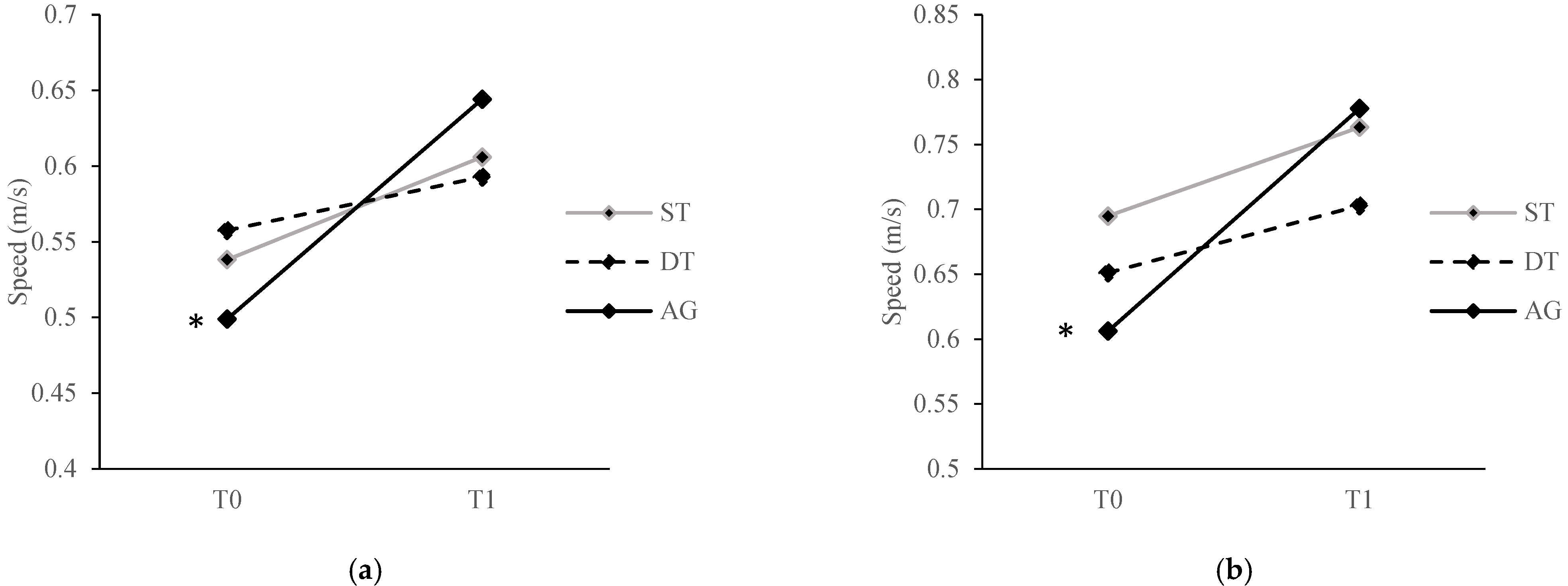
3.3. Intervention Effects on the Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kannus, P.; Parkkari, J.; Koskinen, S.; Niemi, S.; Palvanen, M.; Järvinen, M.; Vuori, I. Fall-Induced Injuries and Deaths among Older Adults. JAMA 1999, 281, 1895–1899. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Mendes de Leon, C.F.; Doucette, J.T.; Baker, D.I. Fear of Falling and Fall-Related Efficacy in Relationship to Functioning among Community-Living Elders. J. Gerontol. 1994, 49, M140–M147. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, C.S. Falls, Injuries Due to Falls, and the Risk of Admission to a Nursing Home. N. Engl. J. Med. 1997, 337, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in Older People: Epidemiology, Risk Factors and Strategies for Prevention. Age Ageing 2006, 35 (Suppl. S2), ii37–ii41. [Google Scholar] [CrossRef]
- Li, W.; Keegan, T.H.M.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P.; Kelsey, J.L. Outdoor Falls among Middle-Aged and Older Adults: A Neglected Public Health Problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef]
- Malone, L.A.; Bastian, A.J. Thinking About Walking: Effects of Conscious Correction Versus Distraction on Locomotor Adaptation. J. Neurophysiol. 2010, 103, 1954–1962. [Google Scholar] [CrossRef]
- Masters, R.; Maxwell, J. The Theory of Reinvestment. Int. Rev. Sport Exerc. Psychol. 2008, 1, 160–183. [Google Scholar] [CrossRef]
- Wulf, G.; McNevin, N.; Shea, C.H. The Automaticity of Complex Motor Skill Learning as a Function of Attentional Focus. Q. J. Exp. Psychol. Sect. A 2001, 54, 1143–1154. [Google Scholar] [CrossRef]
- Wong, W.L.; Masters, R.; Maxwell, J.; Abernethy, B. Reinvestment and Falls in Community-Dwelling Older Adults. Neurorehabil. Neural Repair 2008, 22, 410–414. [Google Scholar] [CrossRef]
- Mak, T.C.T.; Young, W.R.; Chan, D.C.L.; Wong, T.W.L. Gait Stability in Older Adults During Level-Ground Walking: The Attentional Focus Approach. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2020, 75, 274–281. [Google Scholar] [CrossRef]
- Mak, T.C.T.; Young, W.R.; Lam, W.-K.; Tse, A.C.Y.; Wong, T.W.L. The Role of Attentional Focus on Walking Efficiency among Older Fallers and Non-Fallers. Age Ageing 2019, 48, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.S.W.; Poolton, J. Advances in Implicit Motor Learning. In Skill Acquisition in Sport: Research, Theory and Practice; Hodges, N.W., Williams, A.M., Eds.; Routledge: Oxon, UK, 2012; pp. 59–75. ISBN 978-0-203-13371-2. [Google Scholar]
- Sternberg, R.J. The Nature of Cognition; MIT Press: Cambridge, UK, 1999; ISBN 978-0-262-69212-0. [Google Scholar]
- Masters, R.S.W. Knowledge, Knerves and Know-How: The Role of Explicit versus Implicit Knowledge in the Breakdown of a Complex Motor Skill under Pressure. Br. J. Psychol. 1992, 83, 343–358. [Google Scholar] [CrossRef]
- Berry, D.C.; Broadbent, D.E. Interactive Tasks and the Implicit-Explicit Distinction. Br. J. Psychol. 1988, 79, 251–272. [Google Scholar] [CrossRef]
- Masters, R.S.W. Theoretical Aspects of Implicit Learning in Sport. Int. J. Sport Psychol. 2000, 31, 530–541. [Google Scholar]
- Wollesen, B.; Voelcker-Rehage, C. Training Effects on Motor–Cognitive Dual-Task Performance in Older Adults. Eur. Rev. Aging Phys. Act. 2014, 11, 5–24. [Google Scholar] [CrossRef]
- Liao, C.M.; Masters, R.S. Analogy Learning: A Means to Implicit Motor Learning. J. Sports Sci. 2001, 19, 307–319. [Google Scholar] [CrossRef]
- Balota, D.A.; Dolan, P.O.; Duchek, J.M. Memory Changes in Healthy Older Adults. In The Oxford handbook of memory; Oxford University Press: New York, NY, USA, 2000; pp. 395–409. ISBN 978-0-19-512265-7. [Google Scholar]
- Verhaeghen, P.; Salthouse, T.A. Meta-Analyses of Age-Cognition Relations in Adulthood: Estimates of Linear and Nonlinear Age Effects and Structural Models. Psychol. Bull. 1997, 122, 231–249. [Google Scholar] [CrossRef]
- Tse, A.C.Y.; Wong, T.W.L.; Masters, R.S.W. Examining Motor Learning in Older Adults Using Analogy Instruction. Psychol. Sport Exerc. 2017, 28, 78–84. [Google Scholar] [CrossRef]
- Guccione, A.A.; Avers, D.; Wong, R. Geriatric Physical Therapy—Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; ISBN 978-0-323-07241-0. [Google Scholar]
- Wong, T.W.L. Examining Conscious Motor Processing and the Effect of Single-Task, Dual-Task and Analogy Training on Walking during Rehabilitation by Older Adults at Risk of Falling in Hong Kong: Design and Methodology of a Randomized Controlled Trial. Contemp. Clin. Trials Commun. 2019, 15, 100398. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Chiu, H.F.K.; Lee, H.C.; Chung, W.S.; Kwong, P.K. Reliability and Validity of the Cantonese Version of Mini-Mental State Examination-A Preliminary Study. Hong Kong J. Psychiatry 1994, 4, 25. [Google Scholar]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.S.W.; Eves, F.F.; Maxwell, J.P. Development of a Movement Specific Reinvestment Scale; International Society of Sport Psychology (ISSP): Sydney, Australia, 2005. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Berg, K.; Wood-Dauphine, S.; Williams, J.I.; Gayton, D. Measuring Balance in the Elderly: Preliminary Development of an Instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Bohannon, R.W. Comfortable and Maximum Walking Speed of Adults Aged 20-79 Years: Reference Values and Determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef]
- Siu, K.-C.; Catena, R.D.; Chou, L.-S.; van Donkelaar, P.; Woollacott, M.H. Effects of Secondary Task on Obstacle Avoidance in Healthy Young Adults. Exp. Brain Res. Exp. Hirnforsch. Exp. Cerebrale 2008, 184, 115–120. [Google Scholar] [CrossRef][Green Version]
- Plummer-D’Amato, P.; Altmann, L.J.P.; Saracino, D.; Fox, E.; Behrman, A.L.; Marsiske, M. Interactions between Cognitive Tasks and Gait after Stroke: A Dual Task Study. Gait Posture 2008, 27, 683–688. [Google Scholar] [CrossRef]
- Hellström, K.; Lindmark, B. Fear of Falling in Patients with Stroke: A Reliability Study. Clin. Rehabil. 1999, 13, 509–517. [Google Scholar] [CrossRef]
- Mak, T.C.T.; Wong, T.W.L. Do Attentional Focus Instructions Affect Real-Time Reinvestment during Level-Ground Walking in Older Adults? Cogn. Process. 2022, 23, 121–128. [Google Scholar] [CrossRef]
- Mak, T.C.T.; Young, W.R.; Wong, T.W.L. Conscious Control of Gait Increases with Task Difficulty and Can Be Mitigated by External Focus Instruction. Exp. Aging Res. 2021, 47, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.F.; Poolton, J.M.; Wilson, M.R.; Maxwell, J.P.; Masters, R.S.W. Neural Co-Activation as a Yardstick of Implicit Motor Learning and the Propensity for Conscious Control of Movement. Biol. Psychol. 2011, 87, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Ellmers, T.J.; Machado, G.; Wong, T.W.-L.; Zhu, F.; Williams, A.M.; Young, W.R. A Validation of Neural Co-Activation as a Measure of Attentional Focus in a Postural Task. Gait Posture 2016, 50, 229–231. [Google Scholar] [CrossRef]
- Chu, C.K.H.; Wong, T.W.L. Conscious Postural Control During Standing on Compliant Surface by Older Adults. J. Mot. Behav. 2019, 51, 342–350. [Google Scholar] [CrossRef]
- Chow, V.W.K.; Ellmers, T.J.; Young, W.R.; Mak, T.C.T.; Wong, T.W.L. Revisiting the Relationship Between Internal Focus and Balance Control in Young and Older Adults. Front. Neurol. 2019, 9, 1131. [Google Scholar] [CrossRef] [PubMed]
- Gentner, D. Structure-Mapping: A Theoretical Framework for Analogy. Cogn. Sci. 1983, 7, 155–170. [Google Scholar] [CrossRef]
- Gentner, D.; Anggoro, F.K.; Klibanoff, R.S. Structure Mapping and Relational Language Support Children’s Learning of Relational Categories. Child Dev. 2011, 82, 1173–1188. [Google Scholar] [CrossRef] [PubMed]
- Schustack, M.W.; Anderson, J.R. Effects of Analogy to Prior Knowledge on Memory for New Information. J. Verbal Learn. Verbal Behav. 1979, 18, 565–583. [Google Scholar] [CrossRef]
- Komar, J.; Chow, J.-Y.; Chollet, D.; Seifert, L. Effect of Analogy Instructions with an Internal Focus on Learning a Complex Motor Skill. J. Appl. Sport Psychol. 2014, 26, 17–32. [Google Scholar] [CrossRef]
- Lam, W.K.; Maxwell, J.P.; Masters, R. Analogy Learning and the Performance of Motor Skills under Pressure. J. Sport Exerc. Psychol. 2009, 31, 337–357. [Google Scholar] [CrossRef]
- Law, J.; Masters, R.; Bray, S.R.; Eves, F.; Bardswell, I. Motor Performance as a Function of Audience Affability and Metaknowledge. J. Sport Exerc. Psychol. 2003, 25, 484–500. [Google Scholar] [CrossRef]
- Poolton, J.M.; Masters, R.S.W.; Maxwell, J.P. The Development of a Culturally Appropriate Analogy for Implicit Motor Learning in a Chinese Population. Sport Psychol. 2007, 21, 375–382. [Google Scholar] [CrossRef]
- Lam, W.K.; Maxwell, J.P.; Masters, R.S.W. Analogy versus Explicit Learning of a Modified Basketball Shooting Task: Performance and Kinematic Outcomes. J. Sports Sci. 2009, 27, 179–191. [Google Scholar] [CrossRef]
- Jie, L.-J.; Goodwin, V.; Kleynen, M.; Braun, S.; Nunns, M.; Wilson, M. Analogy Learning in Parkinson’s Disease: A Proof-of-Concept Study. Int. J. Ther. Rehabil. 2016, 23, 123–130. [Google Scholar] [CrossRef]
- Meier, C.; Frank, C.; Gröben, B.; Schack, T. Verbal Instructions and Motor Learning: How Analogy and Explicit Instructions Influence the Development of Mental Representations and Tennis Serve Performance. Front. Psychol. 2020, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, C.M.; McDaniel, M.A. Use of Analogy in Learning Scientific Concepts. J. Exp. Psychol. Learn. Mem. Cogn. 1993, 19, 975–987. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.-S.; Mayr, U.; Woollacott, M.H. Effects of Single-Task versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Weightman, M.M.; McCulloch, K. Dual-Task Assessment and Intervention. In Mild Traumatic Brain Injury Rehabilitation Toolkit; Borden Institute: Fort Sam Houston, TX, USA, 2014; pp. 321–333. [Google Scholar]
- Evans, J.J.; Greenfield, E.; Wilson, B.A.; Bateman, A. Walking and Talking Therapy: Improving Cognitive-Motor Dual-Tasking in Neurological Illness. J. Int. Neuropsychol. Soc. JINS 2009, 15, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Lugade, V.; Shumway-Cook, A.; van Donkelaar, P.; Chou, L.-S.; Mayr, U.; Woollacott, M.H. Training-Related Changes in Dual-Task Walking Performance of Elderly Persons with Balance Impairment: A Double-Blind, Randomized Controlled Trial. Gait Posture 2009, 29, 634–639. [Google Scholar] [CrossRef]
- Muir-Hunter, S.W.; Wittwer, J.E. Dual-Task Testing to Predict Falls in Community-Dwelling Older Adults: A Systematic Review. Physiotherapy 2016, 102, 29–40. [Google Scholar] [CrossRef]
- Daley, M.J.; Spinks, W.L. Exercise, Mobility and Aging. Sports Med. Auckl. NZ 2000, 29, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Powers, C.M.; MacLean, C.H. Quality Indicators for the Management and Prevention of Falls and Mobility Problems in Vulnerable Elders. Ann. Intern. Med. 2001, 135, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.A.; Keyl, P.M.; Guralnik, J.M.; Foley, D.J.; Marottoli, R.A.; Wallace, R.B. Characteristics of Older Pedestrians Who Have Difficulty Crossing the Street. Am. J. Public Health 1997, 87, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, C.; Miller, M.; Crotty, M. Falls in Community-Dwelling Older Persons Followinig Hip Fracture: Impact on Self-Efficacy, Balance and Handicap. Clin. Rehabil. 2003, 17, 899–906. [Google Scholar] [CrossRef]
- Hardy, S.E.; Perera, S.; Roumani, Y.F.; Chandler, J.M.; Studenski, S.A. Improvement in Usual Gait Speed Predicts Better Survival in Older Adults. J. Am. Geriatr. Soc. 2007, 55, 1727–1734. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (SD) | p Value | |||
|---|---|---|---|---|---|
| Total (n = 56) | ST (n = 9) | DT (n = 23) | AG (n = 24) | ||
| Age | 82.17 (6.63) | 80.11 (7.08) | 81.96 (6.51) | 82.38 (6.36) | 0.67 |
| Sex, male, n (%) | 10 (17.86) | 2 (22.22) | 4 (17.39) | 4 (16.67) | 0.93 |
| With a history of falls, n (%) | 36 (64.29) | 6 (66.67) | 18 (78.26) | 12 (50.00) | 0.13 |
| MSRS-C | 32.07 (12.78) | 34.67 (12.43) | 33.22 (11.19) | 29.50 (14.40) | 0.48 |
| POMA | 20.72 (2.71) | 21.33 (1.80) | 20.43 (2.71) | 20.83 (3.07) | 0.70 |
| BBS | 43.12 (6.40) | 44.11 (4.43) | 42.48 (6.16) | 43.79 (7.14) | 0.72 |
| TUG (seconds) | 21.95 (8.30) | 21.55 (7.16) | 22.45 (7.04) | 21.64 (10.21) | 0.94 |
| FES-13 | 100.90 (21.67) | 104.89 (15.17) | 99.00 (20.98) | 101.63 (24.50) | 0.78 |
| Single-task walking ability | |||||
| Comfortable speed (m/s) | 0.54 (0.20) | 0.54 (0.17) | 0.58 (0.25) | 0.49 (0.16) | 0.29 |
| Fast speed (m/s) | 0.69 (0.25) | 0.71 (0.22) | 0.74 (0.32) | 0.64 (0.18) | 0.42 |
| Dual-task walking ability | |||||
| Verbal, comfortable speed (m/s) | 0.53 (0.20) | 0.54 (0.20) | 0.56 (0.24) | 0.50 (0.16) | 0.60 |
| Verbal, fast speed (m/s) | 0.64 (0.24) | 0.69 (0.25) | 0.65 (0.30) | 0.61 (0.19) | 0.63 |
| Visual-spatial, comfortable speed (m/s) | 0.54 (0.22) | 0.54 (0.19) | 0.56 (0.28) | 0.52 (0.17) | 0.79 |
| Visual-spatial, fast speed (m/s) | 0.64 (0.24) | 0.68 (0.21) | 0.64 (0.29) | 0.61 (0.18) | 0.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mak, T.C.T.; Capio, C.M.; Wong, T.W.L. Effects of Single-Task, Dual-Task and Analogy Training during Gait Rehabilitation of Older Adults at Risk of Falling: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 315. https://doi.org/10.3390/ijerph20010315
Mak TCT, Capio CM, Wong TWL. Effects of Single-Task, Dual-Task and Analogy Training during Gait Rehabilitation of Older Adults at Risk of Falling: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(1):315. https://doi.org/10.3390/ijerph20010315
Chicago/Turabian StyleMak, Toby C. T., Catherine M. Capio, and Thomson W. L. Wong. 2023. "Effects of Single-Task, Dual-Task and Analogy Training during Gait Rehabilitation of Older Adults at Risk of Falling: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 1: 315. https://doi.org/10.3390/ijerph20010315
APA StyleMak, T. C. T., Capio, C. M., & Wong, T. W. L. (2023). Effects of Single-Task, Dual-Task and Analogy Training during Gait Rehabilitation of Older Adults at Risk of Falling: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(1), 315. https://doi.org/10.3390/ijerph20010315