
Assessment of Acceptability and Initial Effectiveness of a Unified Protocol Prevention Program to Train Emotional Regulation Skills in Female Nursing Professionals during the COVID-19 Pandemic

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
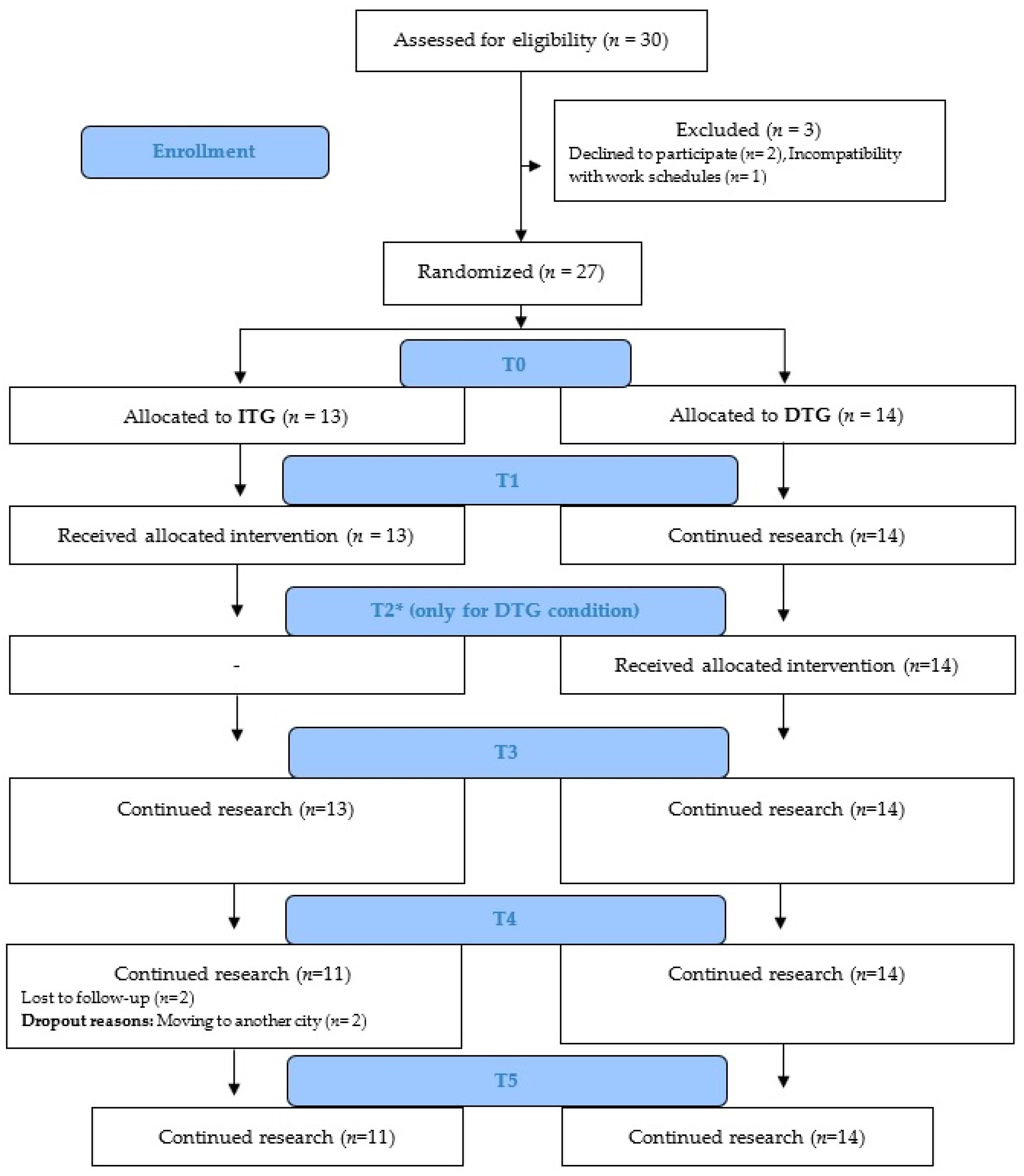
2.1. Participants
2.2. Instruments
2.2.1. Primary Instruments
2.2.2. Secondary Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Sociodemographic Outcomes and Virus Exposure of Participants
3.2. Immediate Treatment Group and Delayed Treatment Group Results
3.3. Results of the Brief up Preventive Program over Time for All Participants
3.4. Satisfaction Results of the Brief up Preventive Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Pérez, V.; Arango, C. Psychiatry in the aftermath of COVID-19. Rev. Psiquiatr. Salud Ment. (Engl. Ed.) 2020, 13, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Franza, F.; Basta, R.; Pellegrino, F.; Solomita, B.; Fasano, V. The role of fatigue of compassion, burnout and hopelessness in healthcare: Experience in the time of COVID-19 outbreak. Psychiatr. Danub. 2020, 32, 10–14. [Google Scholar]
- Bullis, J.R.; Boettcher, H.; Sauer-Zavala, S.; Barlow, D.H. What is an emotional disorder? A transdiagnostic mechanistic definition with implications for assessment, treatment, and prevention. Clin. Psychol. 2019, 26, e12278. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- de Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M. Impact of Coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of Coronavirus disease 2019 (COVID-19) on medical staff and general public–a systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Calero-Sierra, I.; Monzó-García, M.; Pérez-Martín, J.; Rodriguez-Jimenez, R. Mental health impact of COVID-19 pandemic on spanish healthcare workers. Psychol. Med. 2022, 52, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Menéndez, G.; Rubio-García, A.; Conde-Alvarez, P.; Armesto-Luque, L.; Garrido-Torres, N.; Capitan, L.; Luque, A.; Ruiz-Veguilla, M.; Crespo-Facorro, B. Short-term emotional impact of COVID-19 pandemic on spaniard health workers. J. Affect. Disord. 2021, 278, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Vilagut, G.; Mortier, P.; Ferrer, M.; Alayo, I.; Aragón-Peña, A.; Aragonès, E.; Campos, M.; Cura-González, I.D.; Emparanza, J.I. Mental health impact of the first wave of COVID-19 pandemic on Spanish healthcare workers: A large cross-sectional survey. Rev. Psiquiatr. Salud. Ment. 2021, 14, 90–105. [Google Scholar] [CrossRef] [PubMed]
- Eaton, W.W.; Martins, S.S.; Nestadt, G.; Bienvenu, O.J.; Clarke, D.; Alexandre, P. The burden of mental disorders. Epidemiol. Rev. 2008, 30, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Barlow, D.H.; Farchione, T.J.; Sauer-Zavala, S.; Latin, H.M.; Ellard, K.K.; Bullis, J.R.; Bentley, K.H.; Boettcher, H.T.; Cassiello-Robbins, C. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide, 2nd ed.; Oxford University Press: New York, NY, USA, 2018; ISBN 0190685980. [Google Scholar]
- Barlow, D.H.; Farchione, T.J.; Fairholme, C.P.; Ellard, K.K.; Boisseau, C.L.; Allen, L.B.; Ehrenreich-May, J. The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Brown, T.A.; Campbell, L.A.; Lehman, C.L.; Grisham, J.R.; Mancill, R.B. Current and lifetime comorbidity of the dsm-iv anxiety and mood disorders in a large clinical sample. J. Abnorm. Psychol. 2001, 110, 585–599. [Google Scholar] [CrossRef]
- McHugh, R.K.; Murray, H.W.; Barlow, D.H. Balancing fidelity and adaptation in the dissemination of empirically-supported treatments: The promise of transdiagnostic interventions. Behav. Res. Ther. 2009, 47, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Ferreres-Galán, V.; Meseguer-Valero, M.C.; Ariza-Albinana, S.; Quilez-Orden, A.; Osma, J. Aplicación del Protocolo Unificado en el equipo específico de intervención con infancia y adolescencia (EEIIA): Estudio piloto en mujeres víctimas de violencia intrafamiliar y de pareja. In Aplicaciones Del Protocolo Unificado Para el Tratamiento Transdiagnóstico de la Disregulación Emocional; Osma López, J., Ed.; Alianza Editorial: Madrid, Spain, 2019; pp. 203–218. [Google Scholar]
- Sauer-Zavala, S.; Tirpak, J.W.; Eustis, E.H.; Woods, B.K.; Russell, K. Unified Protocol for the transdiagnostic prevention of emotional disorders: Evaluation of a brief, online course for college freshmen. Behav. Ther. 2021, 52, 64–76. [Google Scholar] [CrossRef]
- Reinholt, N.; Aharoni, R.; Winding, C.; Rosenberg, N.; Rosenbaum, B.; Arnfred, S. Transdiagnostic group CBT for anxiety disorders: The Unified Protocol in mental health services. Cogn. Behav. Ther. 2017, 46, 29–43. [Google Scholar] [CrossRef]
- Sandín, B.; García-Escalera, J.; Valiente, R.M.; Espinosa, V.; Chorot, P. Clinical utility of an internet-delivered version of the Unified Protocol for transdiagnostic treatment of emotional disorders in adolescents (IUP-A): A Pilot Open Trial. Int. J. Environ. Res. Public Health 2020, 17, 8306. [Google Scholar] [CrossRef]
- Sakiris, N.; Berle, D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin. Psychol. Rev. 2019, 72, 101751. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, L.; Saggino, A.; Balsamo, M. On the efficacy of the Unified Protocol for transdiagnostic treatment of emotional disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2021, 87, 101999. [Google Scholar] [CrossRef] [PubMed]
- Ellard, K.K.; Fairholme, C.P.; Boisseau, C.L.; Farchione, T.J.; Barlow, D.H. Unified Protocol for the transdiagnostic treatment of emotional disorders: Protocol development and initial outcome data. Cogn. Behav. Pract. 2010, 17, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, M.W.; Sauer-Zavala, S.E.; Boswell, J.F.; Carl, J.R.; Bullis, J.; Farchione, T.J.; Barlow, D.H. The impact of the Unified Protocol for emotional disorders on quality of life. Int. J. Cogn. Ther. 2013, 6, 57–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Escalera, J.; Chorot, P.; Sandín, B.; Ehrenreich-May, J.; Prieto, A.; Valiente, R.M. An open trial applying the Unified Protocol for transdiagnostic treatment of emotional disorders in adolescents (UP-A) adapted as a school-based prevention program. In Child & Youth Care Forum; Springer: Berlin/Heidelberg, Germany, 2019; Volume 48, pp. 29–53. [Google Scholar]
- Martínez-Borba, V.; Osma, J.; Crespo-Delgado, E.; Andreu-Pejó, L.; Monferrer-Serrano, A. Emotional disorders and symptoms prevention under health conditions: A pilot study using the Unified Protocol in a fertility unit. Anal. Psicol. 2022, 38, 25–35. [Google Scholar] [CrossRef]
- Castro-Camacho, L.; Díaz, M.M.; Barbosa, S. Effect of a group prevention program based on the Unified Protocol for college students in colombia: A quasi-experimental study. Behav. Cogn. Psychother. 2021, in press. [Google Scholar] [CrossRef]
- Priede, A.; López-Álvarez, I.; Carracedo-Sanchidrián, D.; González-Blanch, C. Mental health interventions for healthcare workers during the first wave of COVID-19 pandemic in Spain. Rev. Psiquiatr. Salud. Ment. 2021, 14, 83–89. [Google Scholar] [CrossRef]
- Giordano, F.; Cipolla, A.; Ungar, M. Building resilience for healthcare professionals working in an italian red zone during the COVID-19 outbreak: A pilot study. Stress Health 2022, 38, 234–248. [Google Scholar] [CrossRef]
- Hooper, J.J.; Saulsman, L.; Hall, T.; Waters, F. Addressing the psychological impact of COVID-19 on healthcare workers: Learning from a systematic review of early interventions for frontline responders. BMJ Open 2021, 11, e044134. [Google Scholar] [CrossRef]
- Sun, Z.; Yu, C.; Zhou, Y.; Liu, Z. Psychological interventions for healthcare providers with PTSD in life-threatening pandemic: Systematic review and meta-analysis. Front. Psychiatry 2021, 12, 7783. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Bados, A.; Solanas, A.; Andrés, R. Psychometric properties of the spanish version of Depression, Anxiety and Stress Scales (DASS). Psicothema 2005, 17, 679–683. [Google Scholar]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Hervás, G.; Jódar, R. Adaptación al castellano de La Escala de Dificultades en la Regulación Emocional. Clin. Salud. 2008, 19, 139–156. [Google Scholar]
- Costa, P.T.; McCrae, R.R. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI); TEA Ediciones: Madrid, Spain, 1999. [Google Scholar]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. MBI: Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1996; ISBN 0810832313. [Google Scholar]
- Moreno-Jiménez, B.; Rodríguez-Carvajal, R.; Escobar Redonda, E. La evaluación del burnout profesional. Factorialización del MBI-GS. Un análisis preliminar. Ansiedad Estrés 2001, 7, 69–78. [Google Scholar]
- Weiss, D.S. The Impact of Event Scale: Revised. In Cross-Cultural Assessment of Psychological Trauma and PTSD; Springer: Berlin/Heidelberg, Germany, 2007; pp. 219–238. [Google Scholar]
- Baguena, M.J.; Villaroya, E.; Belena, A.; Díaz, A.; Roldán, C.; Reig, R. Psychometric properties of the Spanish version of the Impact of Event Scale-Revised (IES-R). Anál. Modif. Conducta 2001, 27, 581–604. [Google Scholar]
- Brooks, R. With the EuroQol Group. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. The Spanish version of EuroQol: A description and its applications. European Quality of Life Scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp: Armonk, NY, USA, 2013.
- Bell, M.L.; Whitehead, A.L.; Julious, S.A. Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin. Epidemiol. 2018, 10, 153. [Google Scholar] [CrossRef] [Green Version]
- d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística (INE). Profesionales Sanitarios Colegiados por Sexo. Available online: https://www.ine.es/jaxi/Tabla.htm?tpx=30726&L=0 (accessed on 22 April 2022).
- Carvajal, A.; Centeno, C.; Watson, R.; Martínez, M.; Rubiales, A.S. How is an instrument for measuring health to be validated? An. Sist. Sanit. Navar. 2011, 34, 63–72. [Google Scholar] [PubMed] [Green Version]

{kind=link}
| ITG (n = 13) n (%) | DTG (n = 14) n (%) | TOTAL (N = 27) n (%) | |
|---|---|---|---|
| Marital Status | |||
| Married/living with partner | 10 (76.9) | 11 (78.6) | 21 (77.8) |
| Single | 3 (23.1) | 2 (14.3) | 5 (18.5) |
| Widowed | 0 (0.0) | 1 (7.1) | 1 (3.7) |
| Occupation | |||
| Nurse | 6 (46.2) | 8 (57.1) | 14 (51.9) |
| Auxiliary nursing care technician | 7 (53.8) | 5 (35.7) | 12 (44.4) |
| Anatomic pathology technician | - | 1 (7.1) | 1 (3.7) |
| Hospital Unit | |||
| Internal Medicine B | 4 (30.8) | 4 (28.6) | 8 (29.6) |
| Internal Medicine A | 3 (23.1) | 3 (21.4) | 6 (22.2) |
| COVID-19 Surgery | 3 (23.1) | 0 (0.0) | 3 (11.1) |
| Emergencies | 0 (0.0) | 2 (14.3) | 2 (7.4) |
| COVID-19 plant | 1 (7.7) | 0 (0.0) | 1 (3.7) |
| Others | 2 (15.4) | 5 (35.6) | 7 (25.9) |
| Work experience | |||
| More than 5 years | 11 (84.6) | 13 (92.9) | 24 (88.9) |
| 2–5 years | 2 (15.4) | 1 (7.1) | 3 (11.1) |
| Virus Exposure (0 “no contact” to 10 “close contact”) | |||
| Less than 8 | 4 (30.8) | 4 (28.6) | 8 (29.6) |
| More than 8 | 9 (69.2) | 10 (71.4) | 19 (70.4) |
| 8 | 3 (23.1) | 0 (7.1) | 3 (11.1) |
| 9 | 1 (7.7) | 1 (7.1) | 2 (7.4) |
| 10 | 5 (38.5) | 9 (64.3) | 14 (51.9) |
| COVID infection | |||
| No | 10 (76.9) | 12 (85.7) | 22 (81.5) |
| Yes | 3 (23.1) | 2 (14.3) | 5 (18.5) |
| Severity of Symptoms (0 “no symptoms” to 10 “severe symptoms”) | |||
| 0 | 1 (33.3) | 1 (50.0) | 2 (40.0) |
| 2 | 1 (33.3) | 1 (50.0) | 2 (40.0) |
| 3 | 1 (33.3) | 0 (0.0) | 1 (20.0) |
| Family members infected | |||
| No | 8 (61.5) | 10 (71.4) | 18 (66.7) |
| Yes | 5 (38.5) | 4 (28.6) | 9 (33.3) |
| T0 | T1 | T2 | T3 | T4 | T5 | |||
|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |||
| Primary outcomes | DASS_Stress | ITG | 6.62 (4.52) | 4.54 (3.99) | - | 4.77 (4.04) | 5.18 (4.79) | 4.18 (3.19) |
| DTG | 7.36 (3.59) | 5.42 (2.23) | 5.29 (2.09) | 5.45 (2.66) | 5.17 (2.44) | 7.17 (3.19) | ||
| DASS_Anxiety | ITG | 4.00 (3.56) | 2.15 (1.95) | - | 1.85 (2.34) | 2.27 (3.90) | 1.36 (1.96) | |
| DTG | 3.50 (1.7) | 2.92 (2.15) | 3.00 (2.83) | 2.18 (1.72) | 1.83 (2.21) | 4.17 (2.86) | ||
| DASS_Depression | ITG | 5.85 (5.8) | 3.69 (5.02) | - | 3.08 (3.57) | 4.09 (4.61) | 4.27 (4.34) | |
| DTG | 5.00 (4.76) | 2.67 (1.92) | 4.14 (3.7) | 2.70 (2.87) | 3.08 (2.31) | 3.67 (2.77) | ||
| Secondary outcomes | DERS | ITG | 58.92 (17.54) | 54.23 (18.21) | - | 51.54 (15.69) | 50.55 (14.47) | 49.36 (13.84) |
| DTG | 56.57 (14.85) | 55.75 (11.14) | 55.23 (12.06) | 49.4 (9.99) | 55.27 (15.51) | 53.83 (12.08) | ||
| Neuroticism | ITG | 21.77 (9.64) | 21.46 (8.25) | - | 18.17 (8.70) | 18.00 (9.19) | 18.00 (9.30) | |
| DTG | 21.79 (4.64) | 19.00 (5.77) | 19.36 (5.53) | 19.5 (5.10) | 19.5 (5.65) | 19.25 (4.96) | ||
| Extraversion | ITG | 25.46 (5.09) | 26.92 (5.92) | - | 28.42 (6.99) | 28.9 (5.57) | 28.00 (6.45) | |
| DTG | 24.21 (6.96) | 25.92 (4.89) | 26.00 (6.8) | 27.67 (7.78) | 26.67 (7.02) | 27.08 (6.52) | ||
| MBI_Emotional Exhaustion | ITG | 11.00 (9.21) | 9.69 (6.97) | - | 10.15 (7.36) | 11.36 (5.73) | 13.45 (9.70) | |
| DTG | 16.00 (11.64) | 17.17 (10.17) | 16.21 (7.68) | 15.3 (8.65) | 14.18 (8.81) | 17.33 (11.11) | ||
| MBI_Depersonalization | ITG | 5.85 (4.24) | 5.69 (3.84) | - | 5.08 (4.09) | 5.45 (5.35) | 5.55 (4.18) | |
| DTG | 4.79 (5.18) | 5.33 (3.87) | 4.57 (3.80) | 2.91 (2.39) | 3.42 (3.32) | 3.92 (4.78) | ||
| MBI_Personal accomplishment | ITG | 40.92 (4.92) | 35.15 (6.57) | - | 38.23 (6.37) | 40.00 (3.9) | 36.82 (5.51) | |
| DTG | 38.79 (5.92) | 40.42 (5.07) | 38.57 (7.90) | 40.6 (4.43) | 39.18 (6.6) | 37.42 (6.69) | ||
| IESR_Intrusion | ITG | 23.15 (13.63) | 19.85 (13.56) | - | 15.33 (13.25) | 16.73 (12.64) | 14.27 (11.88) | |
| DTG | 18.5 (9.59) | 20.33 (9.16) | 19.85 (8.22) | 18.45 (13.02) | 15.42 (8.51) | 14.5 (6.97) | ||
| IESR_Avoidance | ITG | 15.08 (7.58) | 13.08 (6.60) | - | 11 (6.78) | 11.36 (6.87) | 9.82 (7.21) | |
| DTG | 11.21 (5.94) | 13.75 (6.31) | 12.79 (4.12) | 10.18 (6.21) | 11.58 (5.43) | 9.75 (4.65) | ||
| EuroQol | ITG | 74.23 (18.13) | 76.54 (17.37) | - | 82.67 (13.61) | 79.55 (15.92) | 81.36 (16.45) | |
| DTG | 77.86 (7.77) | 78.00 (7.51) | 83.75 (7.72) | 86.36 (5.52) | 78.17 (24.48) | 78.33 (14.51) | ||
| Time | Condition | Time*Condition | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | Cohen’s d | F | p | Cohen’s d | F | p | Cohen’s d | |
| DASS_Stress | 1.04 | 0.390 | 0.41 | 0.02 | 0.895 | 0.18 | 1.59 | 0.184 | 0.50 |
| DASS_Anxiety | 1.94 | 0.110 | 0.56 | 0.38 | 0.541 | 0.25 | 3.16 | 0.018 | 0.71 |
| DASS_Depression | 1.26 | 0.290 | 0.45 | 0.99 | 0.328 | 0.40 | 1.94 | 0.110 | 0.56 |
| DERS | 2.36 | 0.060 | 0.61 | 0.01 | 0.917 | 0.04 | 0.97 | 0.425 | 0.39 |
| Neuroticism | 2.58 | 0.043 | 0.64 | 0.31 | 0.583 | 0.22 | 1.61 | 0.179 | 0.51 |
| Extraversion | 2.09 | 0.089 | 0.58 | 0.00 | 0.992 | 0.00 | 0.33 | 0.859 | 0.23 |
| MBI_Emotional Exhaustion | 1.19 | 0.321 | 0.44 | 3.03 | 0.093 | 0.70 | 0.62 | 0.653 | 0.31 |
| MBI_Depersonalization | 0.80 | 0.527 | 0.36 | 1.70 | 0.204 | 0.52 | 0.20 | 0.939 | 0.18 |
| MBI_Personal accomplishment | 3.95 | 0.005 | 0.80 | 0.52 | 0.476 | 0.29 | 1.14 | 0.343 | 0.43 |
| IESR_Intrusion | 4.91 | 0.001 | 0.89 | 0.29 | 0.597 | 0.22 | 1.26 | 0.290 | 0.45 |
| IESR_Avoidance | 4.81 | 0.001 | 0.88 | 0.39 | 0.535 | 0.25 | 0.10 | 0.983 | 0.13 |
| EuroQol | 1.88 | 0.121 | 0.55 | 0.43 | 0.520 | 0.26 | 0.64 | 0.638 | 0.32 |
| Main Effects | Cohen’s d | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | T5 | F | p | Pre-T-to-Post-T | Post-T-to-6-MFU | Pre-T-to-6-MFU | ||
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |||||||
| DASS_Anxiety | ITG | 4.00 (3.56) | 2.15 (1.95) | - | 1.85 (2.34) | 2.27 (3.90) | 1.36 (1.96) | 2.20 | 0.084 | −0.64 | −0.40 | −0.92 |
| DTG | 3.50 (1.7) | 2.92 (2.15) | 3.00 (2.83) | 2.18 (1.72) | 1.83 (2.21) | 4.17 (2.85) | 3.51 | 0.014 | 0.03 | 0.41 | 0.49 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreres-Galán, V.; Navarro-Haro, M.V.; Peris-Baquero, Ó.; Guillén-Marín, S.; de Luna-Hermoso, J.; Osma, J. Assessment of Acceptability and Initial Effectiveness of a Unified Protocol Prevention Program to Train Emotional Regulation Skills in Female Nursing Professionals during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 5715. https://doi.org/10.3390/ijerph19095715
Ferreres-Galán V, Navarro-Haro MV, Peris-Baquero Ó, Guillén-Marín S, de Luna-Hermoso J, Osma J. Assessment of Acceptability and Initial Effectiveness of a Unified Protocol Prevention Program to Train Emotional Regulation Skills in Female Nursing Professionals during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(9):5715. https://doi.org/10.3390/ijerph19095715
Chicago/Turabian StyleFerreres-Galán, Vanesa, María Vicenta Navarro-Haro, Óscar Peris-Baquero, Silvia Guillén-Marín, Jordi de Luna-Hermoso, and Jorge Osma. 2022. "Assessment of Acceptability and Initial Effectiveness of a Unified Protocol Prevention Program to Train Emotional Regulation Skills in Female Nursing Professionals during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 9: 5715. https://doi.org/10.3390/ijerph19095715
APA StyleFerreres-Galán, V., Navarro-Haro, M. V., Peris-Baquero, Ó., Guillén-Marín, S., de Luna-Hermoso, J., & Osma, J. (2022). Assessment of Acceptability and Initial Effectiveness of a Unified Protocol Prevention Program to Train Emotional Regulation Skills in Female Nursing Professionals during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(9), 5715. https://doi.org/10.3390/ijerph19095715