
Knee Kinetics and Kinematics of Young Asymptomatic Participants during Single-Leg Weight-Bearing Tasks: Task and Sex Comparison of a Cross-Sectional Study

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
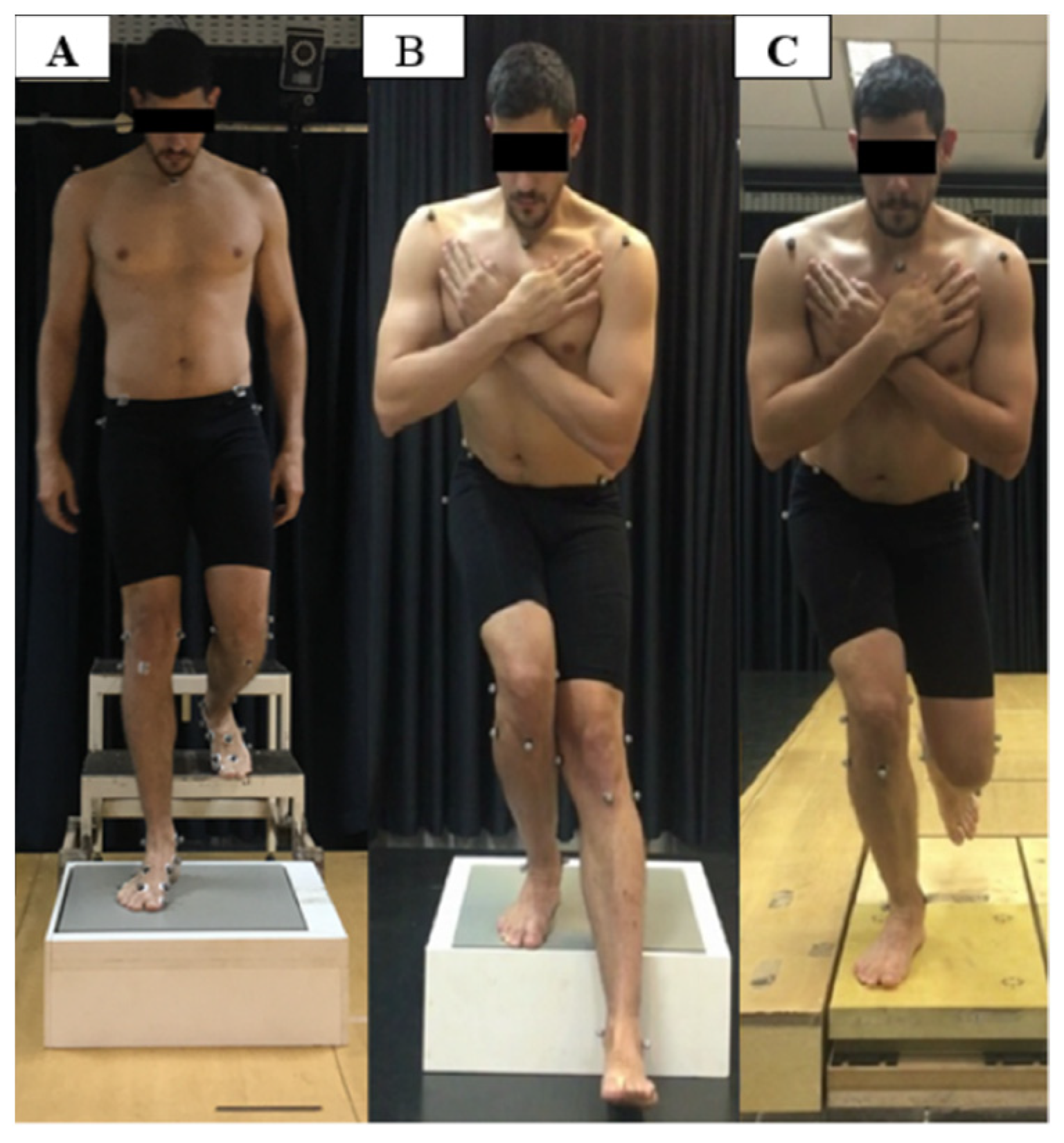
2.2. Procedures
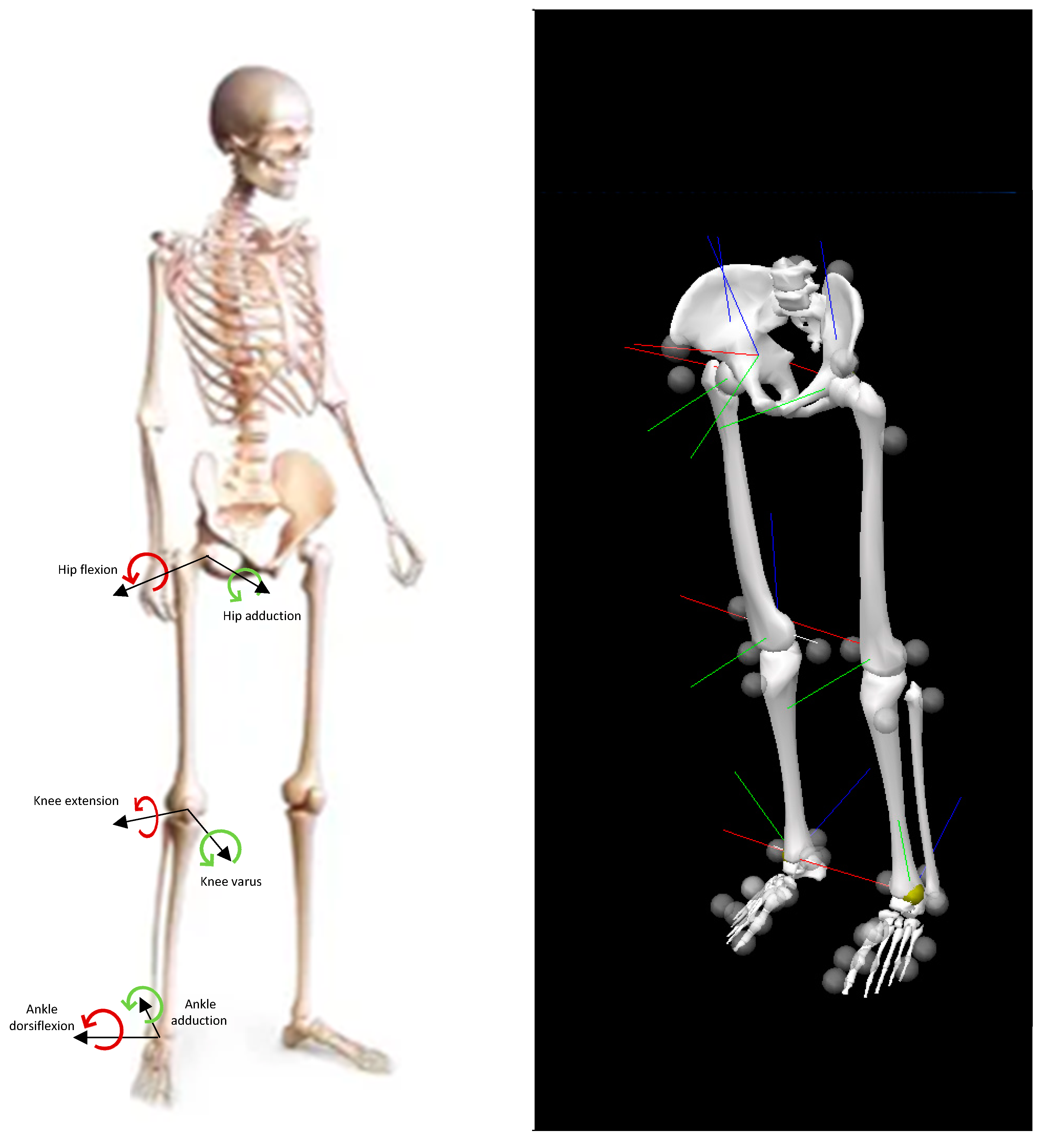
2.3. Data Processing
2.4. Statistical Analysis
3. Results
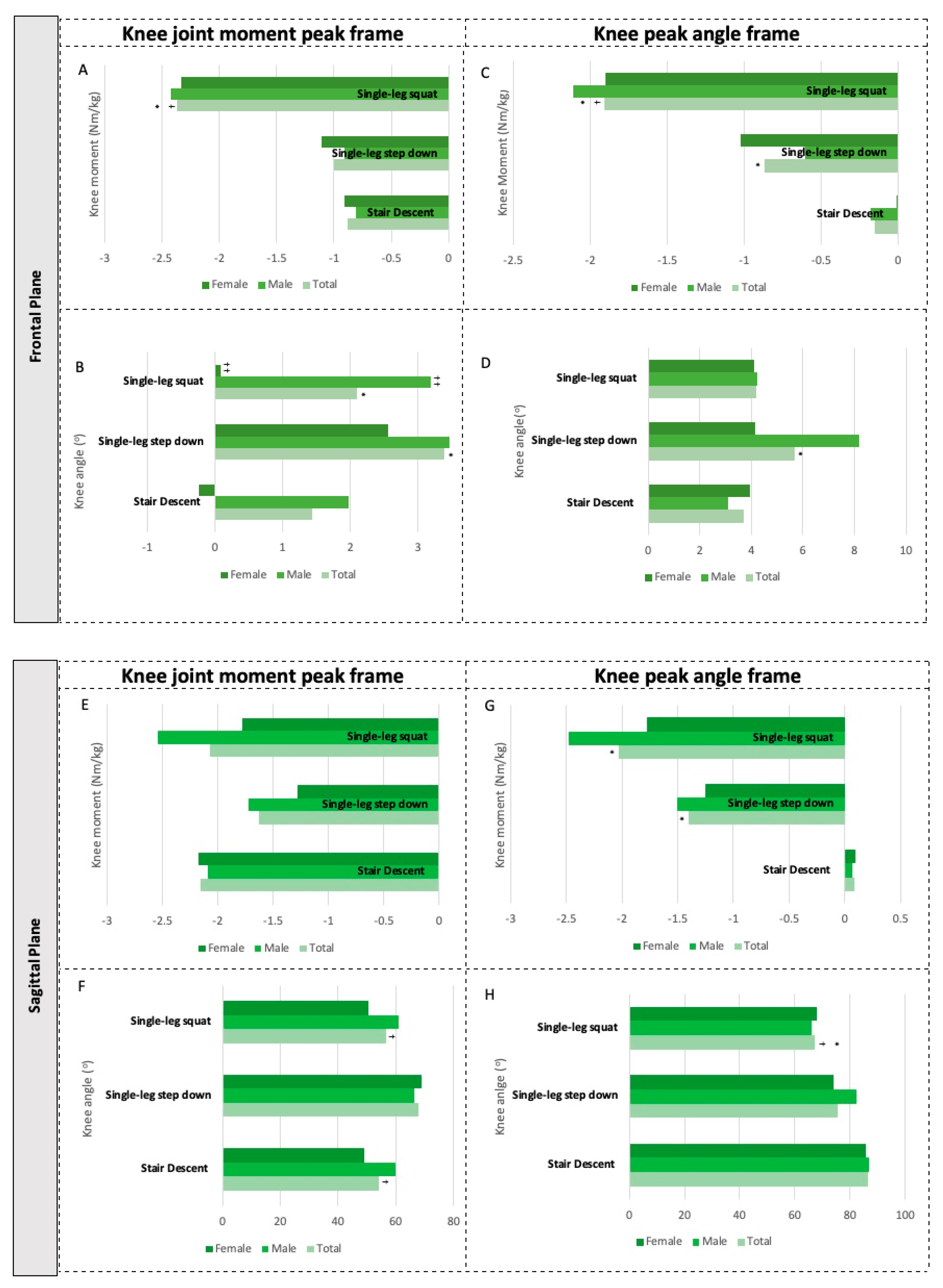
3.1. Knee Kinetics and Kinematics during Single-Leg Weight-Bearing Tasks
3.2. Sex Differences of Knee Kinetics and Kinematics
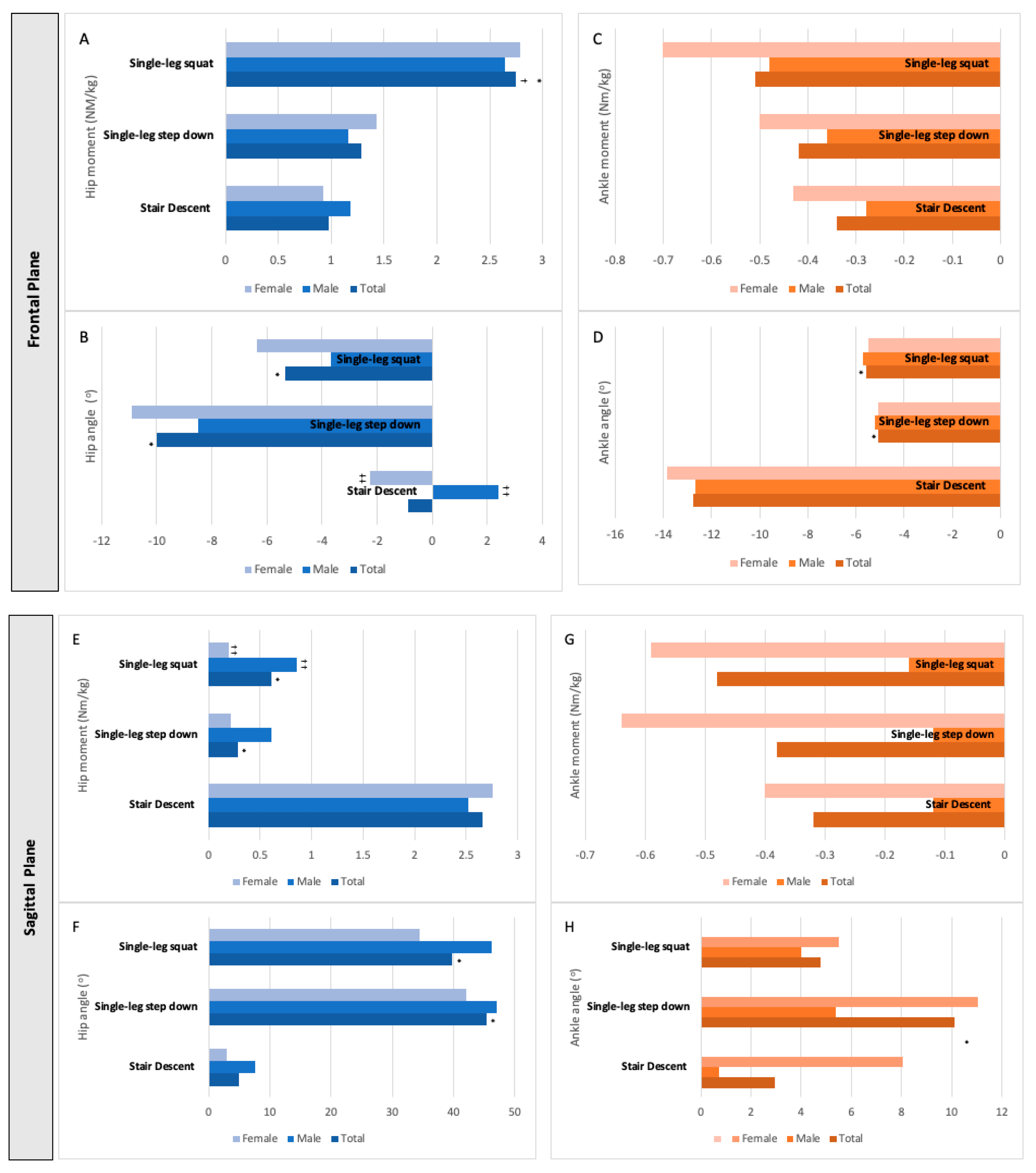
3.3. Hip and Ankle Kinetics and Kinematics at Peak Knee Joint Moment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ortiz, A.; Micheo, W. Biomechanical evaluation of the athlete’s Knee: From basic science to clinical application. PM R 2011, 3, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T. Structural correlates of pain in osteoarthritis. Clin. Exp. Rheumatol. 2017, 35, 75–78. [Google Scholar] [PubMed]
- Smith, B.; Selfe, J.; Thacker, D.; Hendrik, P.; Bateman, M.; Moffatt, F.; Rathleff, M.S.; Smith, T.O.; Logan, P. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilic, O.; Maas, M.; Verhagen, E.; Zwerver, J.; Gouttebarge, V. Incidence, aetiology and prevention of musculoskeletal injuries in volleyball: A systematic review of the literature. Eur. J. Sport Sci. 2017, 17, 765–793. [Google Scholar] [CrossRef] [Green Version]
- Mehrab, M.; de Vos, R.J.; Kraan, G.A.; Mathijssen, N.M.C. Injury Incidence and Patterns Among Dutch CrossFit Athletes. Orthop. J. Sport Med. 2017, 5, 2325967117745263. [Google Scholar] [CrossRef] [Green Version]
- Mohtasham, H.M.; Shahrbanian, S.; Khoshroo, F. Epidemiology and history of knee injury and its impact on activity limitation among football premier league professional referees. J. Inj. Violence Res. 2018, 8, 43–57. [Google Scholar]
- O’Kane, J.W.; Neradilek, M.; Polissar, N.; Sabado, L.; Tencer, A.; Schiff, M.A. Risk factors for lower extremity overuse injuries in female youth soccer players. Orthop. J. Sport Med. 2017, 5, 2325967117733963. [Google Scholar] [CrossRef] [Green Version]
- Panagodage Perera, N.K.; Joseph, C.; Kemp, J.L.; Finch, C.F. Epidemiology of Injuries in Women Playing Competitive Team Bat-or-Stick Sports: A Systematic Review and a Meta-Analysis. Sports Med. 2018, 48, 617–640. [Google Scholar] [CrossRef]
- Cavanaugh, J.T.; Powers, M. ACL rehabilitation progression: Where are we now? Curr. Rev. Musculoskelet. Med. 2017, 10, 289–296. [Google Scholar] [CrossRef]
- Crossley, K.M.; van Middelkoop, M.; Barton, C.J.; Culvenor, A.G. Rethinking patellofemoral pain: Prevention, management and long-term consequences. Best Pract. Res. Clin. Rheumatol. 2019, 33, 48–65. [Google Scholar] [CrossRef]
- Logerstedt, D.S.; Scalzitti, D.A.; Bennnell, K.L.; Hinnan, R.S.; Silvers-Granelli, H.; Ebert, J.; Hambly, K.; Carey, J.L.; Snyder-Mackler, L.; Axe, M.J.; et al. Knee pain and mobility impairments: Meniscal and articular cartilage lesions Revision 2018. J. Orthop. Sports Phys. Ther. 2018, 48, A1–A50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heebner, N.R.; Rafferty, D.M.; Wohleber, M.F.; Simonsons, A.J.; Lovalekar, M.; Reinert, A.; Sell, T.C. Landing Kinematics and Kinetics at the knee during different tasks. J. Athl. Train. 2017, 52, 1101–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khuu, A.; Foch, E.; Lewis, C.L. Not all single leg squats are equal : A biomechanical comparison of three variations. Int. J. Sports Phys. Ther. 2016, 11, 201–211. [Google Scholar] [PubMed]
- Khuu, A.; Lewis, C.L. Position of the non-stance leg during the single leg squat affects females and males differently. Hum. Mov. Sci. 2019, 67, 102506. [Google Scholar] [CrossRef] [PubMed]
- van Rossom, S.V.; Smith, C.R.; Thelen, D.G.; Vanwanseele, B.; Assche, D.V.; Jonkers, I. Knee Joint Loading in Healthy Adults During Functional Exercises: Implications for Rehabilitation Guidelines. J. Orthop. Sport Phys. Ther. 2018, 48, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Cronström, A.; Creaby, M.W.; Ageberg, E. Do knee abduction kinematics and kinetics predict future anterior cruciate ligament injury risk? A systematic review and meta-analysis of prospective studies. BMC Musculoskelet. Disord. 2020, 21, 563. [Google Scholar] [CrossRef]
- Luz, B.C.; dos Santos, A.F.; Serrão, F.V. Are hip and knee kinematics and training load characteristics relate to pain intensity and physical function level in runners with Patellofemoral Pain? Gait Posture 2021, 84, 162–168. [Google Scholar] [CrossRef]
- Neal, B.S.; Lack, S.D.; Lankhorst, N.E.; Raye, A.; Morrissey, D.; van Middelkoop, M. Risk factors for patellofemoral pain: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 270–281. [Google Scholar] [CrossRef] [Green Version]
- Willwacher, S.; Kurz, M.; Robbin, J.; Thelen, M.; Hamill, J.; Kelly, L.; Mai, P. Running-Related Biomechanical Risk Factors for Overuse Injuries in Distance Runners: A Systematic Review Considering Injury Specificity and the Potentials for Future Research. Sports Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Comfort, P.; Jones, P.A.; Smih, L.C.; Herrington, L. Joint kinetics and kinematics during common lower limb rehabilitation exercises. J. Athl. Train. 2015, 50, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Donohue, M.R.; Ellis, S.M.; Heinbaugh, E.M.; Stephenson, M.L.; Zhu, Q.; Dai, B. Differences and correlations in knee and hip mechanics during single-leg landing, single-leg squat, double-leg landing, and double-leg squat tasks. Res. Sports Med. 2015, 23, 394–411. [Google Scholar] [CrossRef] [PubMed]
- Earl, J.E.; Monteiro, S.K.; Snyder, K.R. Differences in Lower Extremity Kinematics between a Bilateral Drop Vertical Jump and A Single-leg step down. J. Orthop. Sport Phys. Ther. 2007, 37, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.B.; Ford, K.R.; Nguyen, A.D.; Shultz, S.J. Biomechanical Comparison of Single and Double Leg Jump Landings in the Sagittal and Frontal Plane. Orthop. J. Sport Med. 2016, 4, 2325967116655158. [Google Scholar] [CrossRef] [Green Version]
- Wang, L. The lower extremity biomechanics of single- and double-leg stop-jump tasks. J Sports Sci Med 2011, 1, 151–156. [Google Scholar]
- Lewis, C.L.; Foch, E.; Luko, M.M.; Loverro, K.L.; Khuu, A. Differences in lower extremity and trunk kinematics between single leg squat and step down tasks. PLoS ONE 2015, 10, e0126258. [Google Scholar] [CrossRef]
- Cronström, A.; Creaby, M.W.; Nae, J.; Ageberg, E. Gender differences in knee abduction during weight-bearing activities: A systematic review and meta-analysis. Gait Posture 2016, 49, 315–328. [Google Scholar] [CrossRef]
- Baldon, R.M.; Lobato, D.F.M.; Furlan, L.; Serrão, F.V. Gender differences in lower limb kinematics during stair descent. J. Appl. Biomech. 2013, 29, 413–420. [Google Scholar] [CrossRef]
- Hong, Y.N.G.; Shin, C.S. Gender differences of sagittal knee and ankle biomechanics during stair to ground descent transition. Clin. Biomech. 2015, 30, 1210–1217. [Google Scholar] [CrossRef]
- Matsudo, S.; Araújo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. International Physical Activity Questionnaire (IPAQ): Study of validity and reliability in Brazil. Rev. Bras. Ativ. Física Saúde 2001, 6, 5–18. [Google Scholar]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.G.; Walker, K.; Ford, K.R.; Myer, G.D.; Hewett, T.E.; van den Bogert, A.J. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portinaro, N.; Leardini, A.; Panou, A.; Monzani, V.; Caravaggi, P. Modifying the Rizzoli foot model to improve the diagnosis of pes-planus: Application to kinematics of feet in teenagers. J. Foot Ankle Res. 2014, 7, 754–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brechter, J.H.; Powers, C.M. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002, 16, 115–123. [Google Scholar] [CrossRef]
- Cowan, S.M.; Bennell, K.L.; Crossley, K.M.; Hodges, P.W.; McConnell, J. Physical therapy alters recruitment of the vasti in patellofemoral pain syndrome. Med. Sci. Sports Exerc. 2002, 34, 1879–1885. [Google Scholar] [CrossRef]
- Bell, A.L.; Pedersen, D.R.; Brand, R.A. A comparison of the accuracy of several hip center location prediction methods. J. Biomech. 1990, 23, 617–621. [Google Scholar] [CrossRef]
- Suntay, W.J.; Grood, E.S.; Hefzy, M.S.; Butler, D.L.; Noyes, F.R. Error analysis of a system for measuring three-dimensional joint motion. J. Biomech. Eng. 1983, 105, 127–135. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Zawadka, M.; Smolka, J.; Skublewska-Paszkowska, M.; Lukasik, E.; Bys, A.; Zielinski, G.; Gawda, P. Sex-dependent differences in single-leg squat kinematics and their relationship to squat depth in physically active individuals. Sci. Rep. 2020, 10, 19601. [Google Scholar] [CrossRef]
- de Sire, A.; Demeco, A.; Marotta, N.; Spano, R.; Curci, C.; Farì, G.; Fortunato, F.; Ioa, T.; Lippi, L.; Paolucci, T.; et al. Neuromuscular impairment of knee stabilizer muscles in a COVID-19 cluster of female volleyball players: Which role for rehabilitation in the post-COVID-19 return-to-play? Appl. Sci. 2022, 12, 557. [Google Scholar] [CrossRef]
- Houston, A.; Fong, D.T.P.; Bennett, A.N.; Walters, V.; Barker-Davies, R.M. Biomechanical differences between military patients with patellar tendinopathy and asymptomatic controls during single-leg squatting and gait—A statistical parametric mapping study. Clin. Biomech. 2021, 90, 105514. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Pan, C.Y.; Diehl, L.H.; Wittstein, J.R.; Riboh, J.C.; Toth, A.P.; Amendola, A.; Faherty, M.S.; Killelea, C.; Le, D.T.; et al. Altered lower extremity biomechanics following anterior cruciate ligament reconstruction during single-leg and double-leg stop-jump tasks: A bilateral total support moment analysis. Clin. Biomech. 2022, 91, 105533. [Google Scholar] [CrossRef] [PubMed]
- Diniz, K.M.A.; Resende, R.A.; Mascarenhas, R.O.; Silva, H.J.; Filho, R.G.T.; Mendonça, L.M. Hip passive stiffness is associated with hip kinematics during single-leg squat. J. Bodyw. Mov. Ther. 2021, 28, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, G.; Han, B.; Wang, Z.; Yan, Y.; Ma, J.; Wei, P. Knee joint biomechanics in physiological conditions and how pathologies can affect it: A systematic review. Appl. Bionics Biomech. 2020, 2020, 7451683. [Google Scholar] [CrossRef] [PubMed]
- Luz, B.C.; dos Santos, A.F.; de Souza, M.C.; de Oliveira Sato, T.; Nawoczenski, D.A.; Serrão, F.V. Relationship between rearfoot, tibia and femur kinematics in runners with and without patellofemoral pain. Gait Posture 2018, 61, 416–422. [Google Scholar] [CrossRef]
- Warner, M.B.; Wilson, D.A.; Herrington, L.; Dixon, S.; Power, C.; Jones, R.; Heller, M.O.; Carden, P.; Lewis, C.L. A systematic review of the discriminating biomechanical parameters during the single leg squat. Phys. Ther. Sport 2019, 36, 78–91. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 30) | Males (n = 15) | Females (n = 15) | p Value of Sex Comparison | |
|---|---|---|---|---|
| Age (years old) | 21.93 (3.00) | 22.80 (3.28) | 21.07 (2.52) | 0.116 |
| Height (m) | 1.70 (0.08) | 1.76 (0.06) | 1.66 (0.06) | <0.001 |
| Weight (kg) | 71.80 (11.47) | 79.47 (6.06) | 64.13 (10.47) | <0.001 |
| Lower limb dominance | ||||
| Right | 26 (87%) | 13 (87%) | 13 (87%) | 1.000 |
| Left | 4 (13%) | 2 (13%) | 2 (13%) | |
| IPAQ classification | ||||
| Active | 3 (10%) | 3 (20%) | 1 (7%) | 0.28 |
| Irregularly active | 27 (90%) | 12(80%) | 14 (93%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellizzi, G.L.; Will-Lemos, T.; Resende, R.A.; Cervi, A.C.C.; Santiago, P.R.P.; Fernández-de-las-Peñas, C.; Bevilaqua-Grossi, D.; Florencio, L.L. Knee Kinetics and Kinematics of Young Asymptomatic Participants during Single-Leg Weight-Bearing Tasks: Task and Sex Comparison of a Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5590. https://doi.org/10.3390/ijerph19095590
Bellizzi GL, Will-Lemos T, Resende RA, Cervi ACC, Santiago PRP, Fernández-de-las-Peñas C, Bevilaqua-Grossi D, Florencio LL. Knee Kinetics and Kinematics of Young Asymptomatic Participants during Single-Leg Weight-Bearing Tasks: Task and Sex Comparison of a Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5590. https://doi.org/10.3390/ijerph19095590
Chicago/Turabian StyleBellizzi, Gustavo Luís, Tenysson Will-Lemos, Renan Alves Resende, Ana Cristina Corrêa Cervi, Paulo Roberto Pereira Santiago, César Fernández-de-las-Peñas, Débora Bevilaqua-Grossi, and Lidiane Lima Florencio. 2022. "Knee Kinetics and Kinematics of Young Asymptomatic Participants during Single-Leg Weight-Bearing Tasks: Task and Sex Comparison of a Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 9: 5590. https://doi.org/10.3390/ijerph19095590
APA StyleBellizzi, G. L., Will-Lemos, T., Resende, R. A., Cervi, A. C. C., Santiago, P. R. P., Fernández-de-las-Peñas, C., Bevilaqua-Grossi, D., & Florencio, L. L. (2022). Knee Kinetics and Kinematics of Young Asymptomatic Participants during Single-Leg Weight-Bearing Tasks: Task and Sex Comparison of a Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(9), 5590. https://doi.org/10.3390/ijerph19095590