
Effects of Crawling before Walking: Network Interactions and Longitudinal Associations in 7-Year-Old Children



 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Size Estimation
2.3. Measures
2.3.1. Body Composition
2.3.2. Cardiovascular System
2.3.3. Lung Function
2.3.4. Motor Competence
2.3.5. Physical Fitness
2.3.6. Physical Activity
2.3.7. Crawling Assessment
2.4. Study Groups
2.5. Correlation Matrices and Networks
2.6. Data Analysis
3. Results
3.1. Study Population
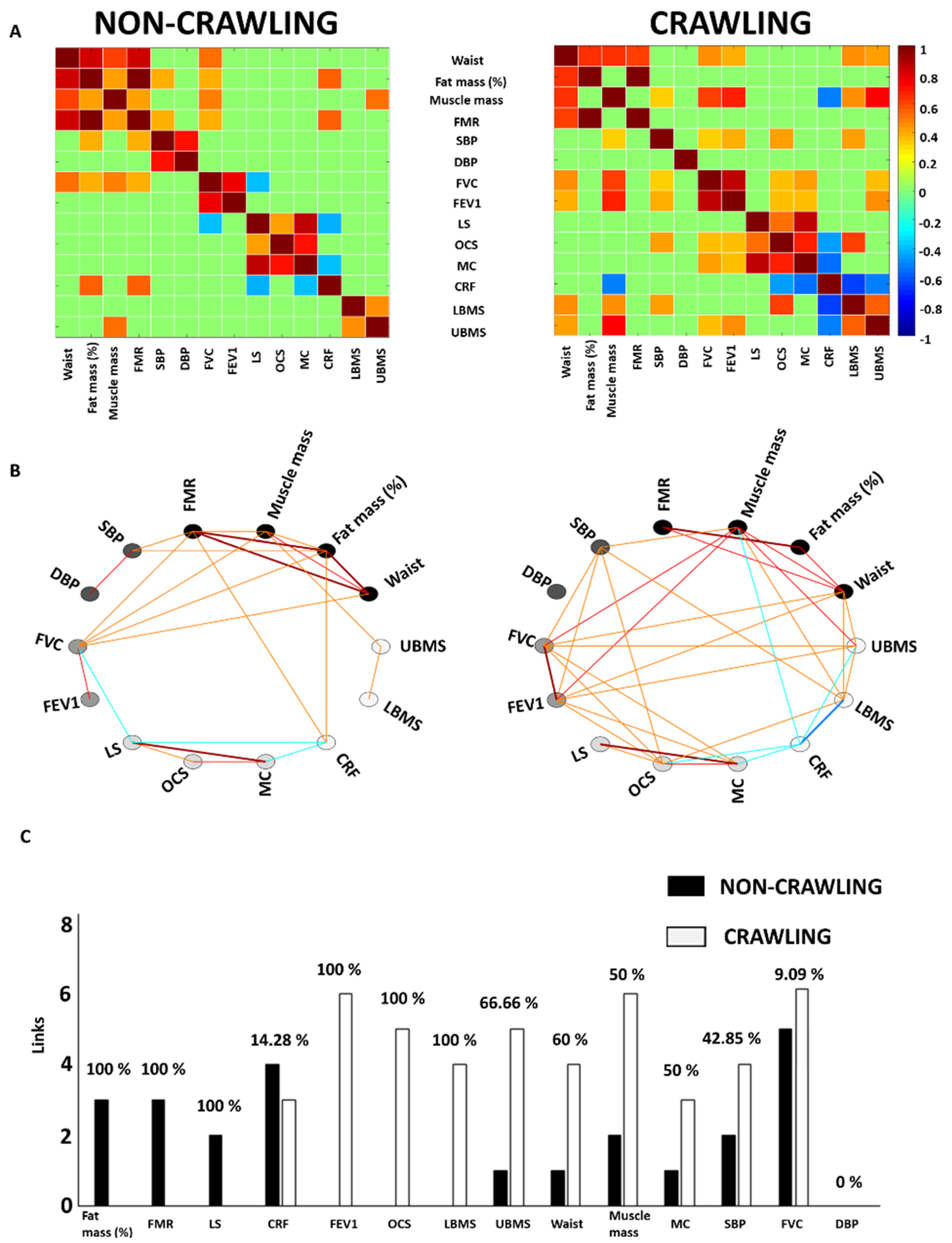
3.2. Network Interactions: The Impact of Crawling before Walking on the Body Systems at Age 7
3.3. Longitudinal Association between Crawling before Walking and the Studied Variables
4. Discussion
Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, L.; Deng, C.F.; Xiong, Q.L.; Wu, X.Y.; Chen, Y.X.; Liu, Y.; Mu, C.L.; Yi, Z.J.; Hou, W.S. Analysis of the Inter-Joints Synergistic Patterns of Limbs in Infant Crawling. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 4156–4159. [Google Scholar] [CrossRef]
- Freedland, R.L.; Bertenthal, B.I. Developmental Changes in Interlimb Coordination: Transition to Hands-and-Knees Crawling. Psychol. Sci. 1994, 5, 26–32. [Google Scholar] [CrossRef]
- Held, R.; Hein, A. Movement-produced stimulation in the development of visually guided behavior. J. Comp. Physiol. Psychol. 1963, 56, 872–876. [Google Scholar] [CrossRef] [PubMed]
- McEwan, M.H.; Dihoff, R.E.; Brosvic, G.M. Early infant crawling experience is reflected in later motor skill development. Percept. Mot. Ski. 1991, 72, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Adolph, K.E.; Vereijken, B.; Denny, M.A. Learning to crawl. Child Dev. 1998, 69, 1299–1312. [Google Scholar] [CrossRef]
- Benjamin Neelon, S.E.; Oken, E.; Taveras, E.M.; Rifas-Shiman, S.L.; Gillman, M.W. Age of achievement of gross motor milestones in infancy and adiposity at age 3 years. Matern. Child Health J. 2012, 16, 1015–1020. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Shoaibi, A.; Neelon, B.; Østbye, T.; Benjamin-Neelon, S.E. Longitudinal associations of gross motor development, motor milestone achievement and weight-for-length z score in a racially diverse cohort of US infants. BMJ Open 2019, 9, e024440. [Google Scholar] [CrossRef]
- Sánchez, G.F.L.; Williams, G.; Aggio, D.; Vicinanza, D.; Stubbs, B.; Kerr, C.; Johnstone, J.; Roberts, J.; Smith, L. Prospective associations between measures of gross and fine motor coordination in infants and objectively measured physical activity and sedentary behavior in childhood. Medicine (Baltim.) 2017, 96, e8424. [Google Scholar] [CrossRef][Green Version]
- Severinsen, M.C.K.; Pedersen, B.K. Muscle–Organ Crosstalk: The Emerging Roles of Myokines. Endocr. Rev. 2020, 41, 594–609. [Google Scholar] [CrossRef]
- Balagué, N.; Hristovski, R.; Almarcha, M.D.C.; Garcia-Retortillo, S.; Ivanov, P.C. Network Physiology of Exercise: Vision and Perspectives. Front. Physiol. 2020, 11, 611550. [Google Scholar] [CrossRef]
- Bartsch, R.P.; Liu, K.K.L.; Bashan, A.; Ivanov, P.C. Network Physiology: How Organ Systems Dynamically Interact. PLoS ONE 2015, 10, e0142143. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation 2008, 117, 3171–3180. [Google Scholar] [CrossRef] [PubMed]
- Lauer, R.M.; Clarke, W.R. Childhood risk factors for high adult blood pressure: The Muscatine Study. Pediatrics 1989, 84, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, S. Validity of muscle-to-fat ratio as a predictor of adult metabolic syndrome. J. Phys. Ther. Sci. 2016, 28, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-Y.; Fang, W.-H.; Wang, C.-C.; Kao, T.-W.; Yang, H.-F.; Wu, C.-J.; Sun, Y.-S.; Wang, Y.-C.; Chen, W.-L. Fat-to-muscle ratio is a useful index for cardiometabolic risks: A population-based observational study. PLoS ONE 2019, 14, e0214994. [Google Scholar] [CrossRef]
- Han, T.S.; Al-Gindan, Y.Y.; Govan, L.; Hankey, C.R.; Lean, M.E.J. Associations of body fat and skeletal muscle with hypertension. J. Clin. Hypertens. 2019, 21, 230–238. [Google Scholar] [CrossRef]
- Kubicek, C.; Jovanovic, B.; Schwarzer, G. The relation between crawling and 9-month-old infants’ visual prediction abilities in spatial object processing. J. Exp. Child Psychol. 2017, 158, 64–76. [Google Scholar] [CrossRef]
- Puente, M.; Canela, J.; Alvarez, J.; Salleras, L.; Vicens-Calvet, E. Cross-sectional growth study of the child and adolescent population of Catalonia (Spain). Ann. Hum. Biol. 2009, 24, 435–452. [Google Scholar] [CrossRef]
- Xu, K.; Zhu, H.J.; Chen, S.; Chen, L.; Wang, X.; Zhang, L.Y.; Pan, L.; Wang, L.; Feng, K.; Wang, K.; et al. Fat-to-muscle Ratio: A New Anthropometric Indicator for Predicting Metabolic Syndrome in the Han and Bouyei Populations from Guizhou Province, China. Biomed. Environ. Sci. BES 2018, 31, 261–271. [Google Scholar] [CrossRef]
- Eigen, H.; Bieler, H.; Grant, D.; Christoph, K.; Terrill, D.; Heilman, D.K.; Ambrosius, W.T.; Tepper, R.S. Spirometric pulmonary function in healthy preschool children. Am. J. Respir. Crit. Care Med. 2001, 163 Pt 1, 619–623. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Boyer, C.; Lloyd, M.; Borghese, M.M.; Knight, E.; Saunders, T.J.; Boiarskaia, E.; Zhu, W.; Tremblay, M.S. Canadian Agility and Movement Skill Assessment (CAMSA): Validity, objectivity, and reliability evidence for children 8–12 years of age. J. Sport Health Sci. 2017, 6, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Font-Lladó, R.; López-Ros, V.; Montalvo, A.M.; Sinclair, G.; Prats-Puig, A.; Fort-Vanmeerhaeghe, A. A Pedagogical Approach to Integrative Neuromuscular Training to Improve Motor Competence in Children: A Randomized Controlled Trail. J. Strength Cond. Res. 2020, 34, 3078–3085. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Bodnarchuk, J.L.; Eaton, W.O. Can parent reports be trusted?: Validity of daily checklists of gross motor milestone attainment. Appl. Dev. Psychol. 2004, 25, 481–490. [Google Scholar] [CrossRef]
- Bashan, A.; Bartsch, R.P.; Kantelhardt, J.W.; Havlin, S.; Ivanov, P.C. Network physiology reveals relations between network topology and physiological function. Nat. Commun. 2012, 3, 702. [Google Scholar] [CrossRef]
- Kang, M.J. The adiposity rebound in the 21st century children: Meaning for what? Korean J. Pediatr. 2018, 61, 375–380. [Google Scholar] [CrossRef]
- Williams, S.; Davie, G.; Lam, F. Predicting BMI in young adults from childhood data using two approaches to modelling adiposity rebound. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 348–354. [Google Scholar] [CrossRef]
- Stanford, K.I.; Middelbeek, R.J.W.; Goodyear, L.J. Exercise Effects on White Adipose Tissue: Beiging and Metabolic Adaptations. Diabetes 2015, 64, 2361–2368. [Google Scholar] [CrossRef]
- Stanford, K.I.; Middelbeek, R.J.W.; Townsend, K.L.; Lee, M.-Y.; Takahashi, H.; So, K.; Hitchcox, K.M.; Markan, K.R.; Hellbach, K.; Hirshman, M.F.; et al. A novel role for subcutaneous adipose tissue in exercise-induced improvements in glucose homeostasis. Diabetes 2015, 64, 2002–2014. [Google Scholar] [CrossRef]
- Sakurai, T.; Endo, S.; Hatano, D.; Ogasawara, J.; Kizaki, T.; Oh-Ishi, S.; Izawa, T.; Ishida, H.; Ohno, H. Effects of exercise training on adipogenesis of stromal-vascular fraction cells in rat epididymal white adipose tissue. Acta Physiol. Oxf. Engl. 2010, 200, 325–338. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Motor Development Study: Windows of achievement for six gross motor development milestones. Acta Paediatr. Oslo Nor. 1992 Suppl. 2006, 450, 86–95. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Sharples, A.P.; Stewart, C.E.; Seaborne, R.A. Does skeletal muscle have an ‘epi’-memory? The role of epigenetics in nutritional programming, metabolic disease, aging and exercise. Aging Cell 2016, 15, 603–616. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.E.; Gilbody, H.J.; Dennison, E.M.; Cooper, C. Does sarcopenia originate in early life? Findings from the Hertfordshire cohort study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M930–M934. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017, a systematic analysis for the Global Burden of Disease Study 2017. Lancet Lond. Engl. 2018, 392, 1923–1994. [Google Scholar] [CrossRef]
- Zaniqueli, D.; Alvim, R.D.O.; Baldo, M.P.; Morra, E.A.; Mill, J.G. Muscle mass is the main somatic growth indicator associated with increasing blood pressure with age in children and adolescents. J. Clin. Hypertens. 2020, 22, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Pillas, D.; Kaakinen, M.; Tzoulaki, I.; Netuveli, G.; Rodriguez, A.; Fung, E.; Tammelin, T.H.; Blane, D.; Millwood, I.Y.; Hardy, R.; et al. Infant locomotive development and its association with adult blood pressure. Eur. J. Pediatr. 2014, 173, 1309–1317. [Google Scholar] [CrossRef]
- Van Vliet, B.N.; Chafe, L.L.; Montani, J.-P. Characteristics of 24 h Telemetered Blood Pressure in eNOS-Knockout and C57Bl/6J Control Mice. J. Physiol. 2003, 549 Pt 1, 313–325. [Google Scholar] [CrossRef]
- Gillman, M.W. Early Infancy as a Critical Period for Development of Obesity and Related Conditions. Nestle Nutr. Workshop Ser. Paediatr. Program. 2010, 65, 13–24. [Google Scholar] [CrossRef]
- Thelen, E. Motor development. A new synthesis. Am. Psychol. 1995, 50, 79–95. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Non-Crawling | Crawling | p-Value |
|---|---|---|---|
| Clinical assessments | |||
| N | 35 | 42 | |
| Age (y) | 7.53 ± 0.36 | 7.46 ± 0.32 | 0.365 |
| Sex (% female) | 54 | 50 | |
| Weight z-score | −0.27 ± 0.76 | −0.52 ± 0.58 | 0.110 |
| Height z-score | −0.05 ± 1.05 | −0.07 ± 0.98 | 0.944 |
| BMI z-score | −0.27 ± 0.66 | −0.58 ± 0.48 | 0.022 |
| Body composition | |||
| Waist (cm) | 56.8 ± 5.20 | 55.4 ± 3.90 | 0.184 |
| Fat mass (%) | 20.1 ± 5.30 | 17.2 ± 3.91 | 0.009 |
| Muscle mass (kg) | 19.5 ± 2.36 | 19.0 ± 2.38 | 0.410 |
| Fat to muscle ratio (kg) | 0.27 ± 0.09 | 0.22 ± 0.06 | 0.008 |
| Cardiovascular system | |||
| SBP (mmHg) | 104 ± 10 | 97 ± 7 | 0.001 |
| DBP (mmHg) | 62 ± 9 | 56 ± 6 | 0.001 |
| Lung function | |||
| FVC (mL) | 1672.81 ± 261.9 | 1621.57 ± 255.31 | 0.413 |
| FEV1 (mL) | 1474.33 ± 264.44 | 1453.51 ± 250.86 | 0.744 |
| Motor competence | |||
| Locomotion skills (CAMSA points) | 0.29 ± 0.10 | 0.27 ± 0.11 | 0.540 |
| Object control skills (CAMSA points) | 0.14 ± 0.07 | 0.14 ± 0.06 | 0.820 |
| Motor competence (CAMSA points) | 14.7 ± 4.21 | 14.56 ± 4.16 | 0.882 |
| Physical fitness | |||
| Cardiorespiratory fitness (min) | 5.23 ± 0.62 | 4.94 ± 0.77 | 0.130 |
| Lower-body muscular strength (cm) | 91.58 ± 14.11 | 94.88 ± 13.98 | 0.393 |
| Upper-body muscular strength (kg) | 20.86 ± 3.89 | 19.67 ± 6.25 | 0.329 |
| Physical Activity | |||
| MVPA per day (min/day) | 60.33 ± 20.16 | 62.28 ± 24.03 | 0.718 |
| Beta | Sig. | R² | ||
|---|---|---|---|---|
| Fat Mass (%) | ||||
| Crawling | −0.185 | 0.038 | ||
| Age (y) | 0.048 | 0.575 | ||
| Sex | −0.178 | 0.031 | ||
| MVPA per day | 0.018 | 0.223 | ||
| Weight z-score | 0.687 | <0.0001 | ||
| 0.563 | ||||
| Fat-to-Muscle Ratio | ||||
| Crawling | −0.188 | 0.024 | ||
| Age (y) | 0.437 | 0.664 | ||
| Sex | −0.198 | 0.017 | ||
| MVPA per day | −0.085 | 0.312 | ||
| Weight z-score | 0.689 | <0.0001 | ||
| 0.567 | ||||
| Systolic Blood Pressure | ||||
| Crawling | −0.316 | 0.005 | ||
| Age (y) | 0.053 | 0.622 | ||
| Sex | 0.137 | 0.190 | ||
| MVPA per day | 0.290 | 0.008 | ||
| Fat-to-muscle ratio | 0.305 | 0.008 | ||
| 0.299 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazorla-González, J.; García-Retortillo, S.; Gacto-Sánchez, M.; Muñoz-Castro, G.; Serrano-Ferrer, J.; Román-Viñas, B.; López-Bermejo, A.; Font-Lladó, R.; Prats-Puig, A. Effects of Crawling before Walking: Network Interactions and Longitudinal Associations in 7-Year-Old Children. Int. J. Environ. Res. Public Health 2022, 19, 5561. https://doi.org/10.3390/ijerph19095561
Cazorla-González J, García-Retortillo S, Gacto-Sánchez M, Muñoz-Castro G, Serrano-Ferrer J, Román-Viñas B, López-Bermejo A, Font-Lladó R, Prats-Puig A. Effects of Crawling before Walking: Network Interactions and Longitudinal Associations in 7-Year-Old Children. International Journal of Environmental Research and Public Health. 2022; 19(9):5561. https://doi.org/10.3390/ijerph19095561
Chicago/Turabian StyleCazorla-González, Jorge, Sergi García-Retortillo, Mariano Gacto-Sánchez, Gerard Muñoz-Castro, Juan Serrano-Ferrer, Blanca Román-Viñas, Abel López-Bermejo, Raquel Font-Lladó, and Anna Prats-Puig. 2022. "Effects of Crawling before Walking: Network Interactions and Longitudinal Associations in 7-Year-Old Children" International Journal of Environmental Research and Public Health 19, no. 9: 5561. https://doi.org/10.3390/ijerph19095561
APA StyleCazorla-González, J., García-Retortillo, S., Gacto-Sánchez, M., Muñoz-Castro, G., Serrano-Ferrer, J., Román-Viñas, B., López-Bermejo, A., Font-Lladó, R., & Prats-Puig, A. (2022). Effects of Crawling before Walking: Network Interactions and Longitudinal Associations in 7-Year-Old Children. International Journal of Environmental Research and Public Health, 19(9), 5561. https://doi.org/10.3390/ijerph19095561