
The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load


Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of Cohort
2.2. Blood Serum Measurements
2.3. PFASs Extraction and Quantitation
2.4. PFASs Detection Limits
2.5. Operationalizing Allostatic Load
2.6. Statistical Analysis
3. Results
- (a)
- Correlation coefficient for PFAS variables (Table 4)
- (b)
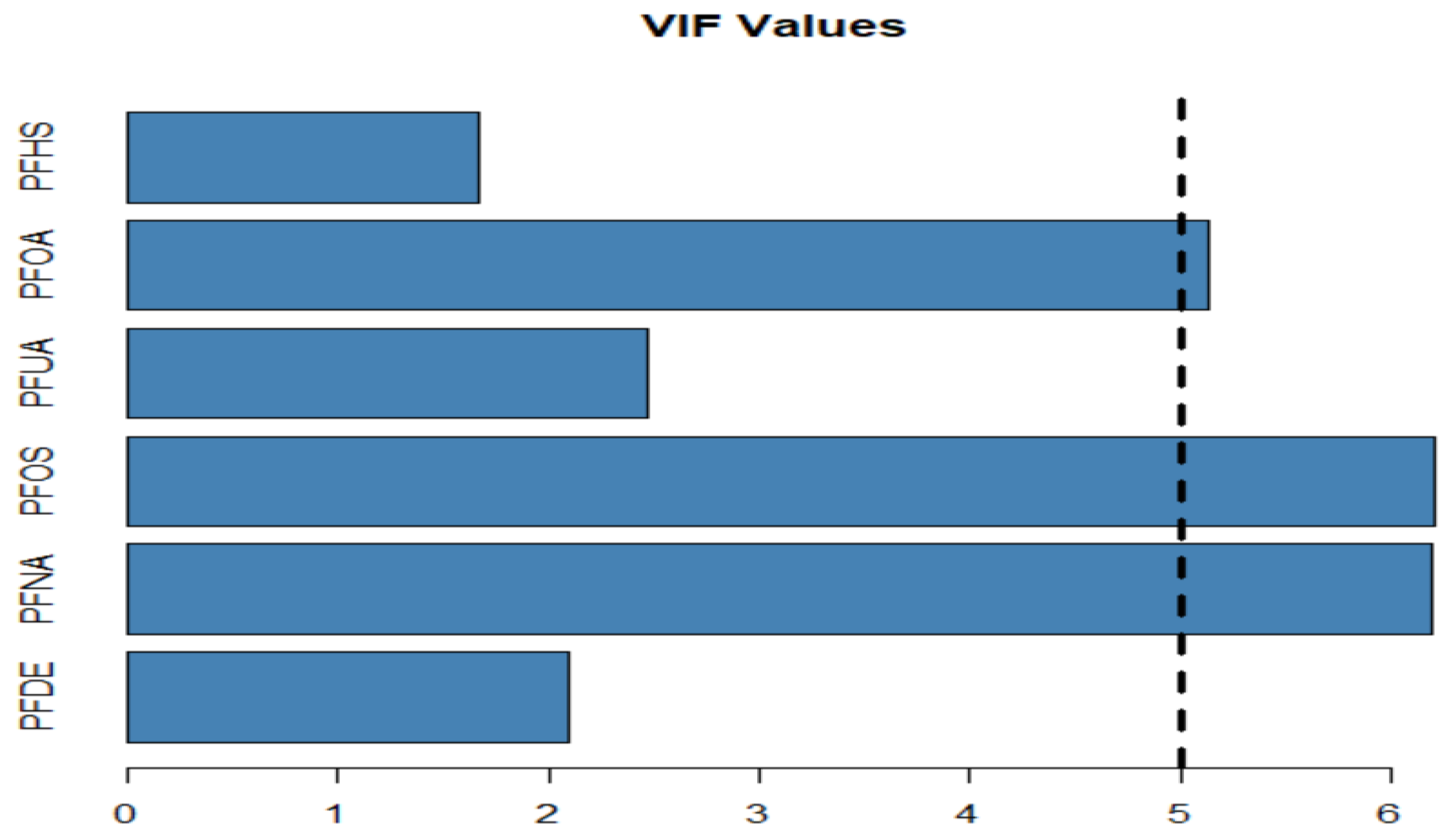
- Variance Inflation Factor (VIF) test (Table 5)
- (c)
- Plotting the VIF to show to values of VIF for each PFAS (Figure 4)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Obeng-Gyasi, E. Per- and Polyfluoroalkyl Substances: Toxic Chemicals of Concern in North Carolina. N. Carol. Med. J. 2022, 83, 90–93. [Google Scholar] [CrossRef]
- Glüge, J.; Scheringer, M.; Cousins, I.T.; DeWitt, J.C.; Goldenman, G.; Herzke, D.; Lohmann, R.; Ng, C.A.; Trier, X.; Wang, Z. An overview of the uses of per-and polyfluoroalkyl substances (PFAS). Environ. Sci. Processes Impacts 2020, 22, 2345–2373. [Google Scholar] [CrossRef]
- Birnbaum, L.S. (Department of Health and Human Services National Institutes of Health National Institute of Environmental Health Sciences) Hearing on “The Federal Role in the Toxic PFAS Chemical Crisis”. Hearing on “The Federal Role in the Toxic PFAS Chemical Crisis” Testimony before the Senate Committee on Homeland Security and Governmental Affairs, 2018. Available online: https://www.niehs.nih.gov/about/assets/docs/hearing_on_the_federal_role_in_the_toxic_pfas_chemical_crisis_508.pdf (accessed on 16 February 2022).
- Sunderland, E.M.; Hu, X.C.; Dassuncao, C.; Tokranov, A.; Wagner, C.C.; Allen, J.G. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects. J. Expo. Sci. Environ. Epidemiol. 2018, 29, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Roostaei, J.; Colley, S.; Mulhern, R.; May, A.A.; Gibson, J.M. Predicting the risk of GenX contamination in private well water using a machine-learned Bayesian network model. J. Hazard. Mater. 2021, 411, 125075. [Google Scholar] [CrossRef] [PubMed]
- Meng, P.; Jiang, X.; Wang, B.; Huang, J.; Wang, Y.; Yu, G.; Cousins, I.T.; Deng, S. Role of the air-water interface in removing perfluoroalkyl acids from drinking water by activated carbon treatment. J. Hazard. Mater. 2019, 386, 121981. [Google Scholar] [CrossRef] [PubMed]
- Sterling, P. Allostasis: A new paradigm to explain arousal pathology. In Handbook of Life Stress, Cognition and Health; John Wiley & Sons: New York, NY, USA, 1988. [Google Scholar]
- McEwen, B.S.; Wingfield, J.C. The concept of allostasis in biology and biomedicine. Horm. Behav. 2003, 43, 2–15. [Google Scholar] [CrossRef]
- McEwen, B.S. Stress, adaptation, and disease: Allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- McEwen, B.S.; Stellar, E. Stress and the individual. Mechanisms leading to disease. Arch. Intern. Med. 1993, 153, 2093–2101. [Google Scholar] [CrossRef]
- Guidi, J.; Lucente, M.; Sonino, N.; Fava, G.A. Allostatic Load and Its Impact on Health: A Systematic Review. Psychother. Psychosom. 2020, 90, 11–27. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E.; Ferguson, A.; Stamatakis, K.; Province, M. Combined Effect of Lead Exposure and Allostatic Load on Cardiovascular Disease Mortality—A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 6879. [Google Scholar] [CrossRef]
- Mathew, A.; Doorenbos, A.Z.; Li, H.; Jang, M.K.; Park, C.G.; Bronas, U.G. Allostatic Load in Cancer: A Systematic Review and Mini Meta-Analysis. Biol. Res. Nurs. 2020, 23, 341–361. [Google Scholar] [CrossRef]
- Sabbah, W.; Watt, R.G.; Sheiham, A.; Tsakos, G. Effects of allostatic load on the social gradient in ischaemic heart disease and periodontal disease: Evidence from the Third National Health and Nutrition Examination Survey. J. Epidemiol. Community Health 2008, 62, 415–420. [Google Scholar] [CrossRef]
- Cui, Y.; Balshaw, D.M.; Kwok, R.K.; Thompson, C.L.; Collman, G.W.; Birnbaum, L.S. The Exposome: Embracing the Complexity for Discovery in Environmental Health. Environ. Health Perspect. 2016, 124, A137–A140. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Laboratory Procedure Manual for Perfluoroalkyl and Polyfluoroalkyl Substances (NHANES 2013−2014); (Method No. 6304.06); CDC: Atlanta, GA, USA, 2014. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/labmethods/PFAS_H_MET.pdf (accessed on 16 February 2022).
- Centers for Disease Control and Prevention. Laboratory Procedure Manual for Perfluoroalkyl and Polyfluoroalkyl Substances (NHANES 2011−2012); (Method No. 6304.04); CDC: Atlanta, GA, USA, 2012. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2011-2012/labmethods/pfc_g_met.pdf (accessed on 16 February 2022).
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. Health and Nutrition Examination Survey Plan and Operations, 1999–2010; 2013. Available online: https://stacks.cdc.gov/view/cdc/21304 (accessed on 16 February 2022).
- McQuillan, G.M.; McLean, J.E.; Chiappa, M.; Harris Corporation; Lukacs, S.L. National Health and Nutrition Examination Survey Biospecimen Program: NHANES III (1988–1994) and NHANES 1999–2014; CDC: Atlanta, GA, USA, 2015. [Google Scholar]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES) MEC Laboratory Procedures Manual, 2013. Jan; CDC: Atlanta, GA, USA, 2013. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/manuals/MEC_Interviewer_2013.pdf (accessed on 16 February 2022).
- Mottaleb, M.A.; Petriello, M.C.; Morris, A.J. High-Throughput UHPLC-MS/MS Measurement of Per- and Poly-Fluorinated Alkyl Substances in Human Serum. J. Anal. Toxicol. 2020, 44, 339–347. [Google Scholar] [CrossRef]
- Kezios, K.L.; Suglia, S.F.; Doyle, D.M.; Susser, E.; Bradwin, G.; Cirillo, P.; Cohn, B.; Link, B.; Factor-Litvak, P. Comparing different operationalizations of allostatic load measured in mid-life and their patterning by race and cumulative life course socioeconomic status. Psychoneuroendocrinology 2022, 139, 105689. [Google Scholar] [CrossRef]
- Goldbourt, U.; Yaari, S.; Medalie, J.H. Isolated low HDL cholesterol as a risk factor for coronary heart disease mortality: A 21-year follow-up of 8000 men. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Mahon, N.G.; Blackstone, E.H.; Francis, G.S.; Starling, R.C.; Young, J.B.; Lauer, M.S. The prognostic value of estimated creatinine clearance alongside functional capacity in ambulatory patients with chronic congestive heart failure. J. Am. Coll. Cardiol. 2002, 40, 1106–1113. [Google Scholar] [CrossRef] [Green Version]
- Horwich, T.B.; Kalantar-Zadeh, K.; MacLellan, R.W.; Fonarow, G.C. Albumin levels predict survival in patients with systolic heart failure. Am. Heart J. 2008, 155, 883–889. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, R.T.; Cheng, Y.; Williamson, D.F.; Gregg, E. Identifying Adults at High Risk for Diabetes and Cardiovascular Disease Using Hemoglobin A1c: National Health and Nutrition Examination Survey 2005–2006. Am. J. Prev. Med. 2011, 40, 11–17. [Google Scholar] [CrossRef]
- Navas-Acien, A.; Guallar, E.; Silbergeld, E.K.; Rothenberg, S.J. Lead Exposure and Cardiovascular Disease—A Systematic Review. Environ. Health Perspect. 2007, 115, 472–482. [Google Scholar] [CrossRef] [Green Version]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsén, B.; Lahti, K.; Nissén, M.; Taskinen, M.-R.; Groop, L. Cardiovascular Morbidity and Mortality Associated with the Metabolic Syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weverling-Rijnsburger, A.W.; Blauw, G.J.; Lagaay, A.M.; Knock, D.L.; Meinders, A.E.; Westendorp, R.G. Total cholesterol and risk of mortality in the oldest old. Lancet 1997, 350, 1119–1123. [Google Scholar] [CrossRef]
- Kaestner, R.; Pearson, J.A.; Keene, D.; Geronimus, A.T. Stress, Allostatic Load, and Health of Mexican Immigrants. Soc. Sci. Q. 2009, 90, 1089–1111. [Google Scholar] [CrossRef] [PubMed]
- Suvarna, B.; Suvarna, A.; Phillips, R.; Juster, R.-P.; McDermott, B.; Sarnyai, Z. Health risk behaviours and allostatic load: A systematic review. Neurosci. Biobehav. Rev. 2020, 108, 694–711. [Google Scholar] [CrossRef]
- Park, S.K.; Peng, Q.; Ding, N.; Mukherjee, B.; Harlow, S.D. Determinants of per- and polyfluoroalkyl substances (PFAS) in midlife women: Evidence of racial/ethnic and geographic differences in PFAS exposure. Environ. Res. 2019, 175, 186–199. [Google Scholar] [CrossRef]
- Domazet, S.L.; Jensen, T.K.; Wedderkopp, N.; Nielsen, F.; Andersen, L.B.; Grøntved, A. Exposure to perfluoroalkylated substances (PFAS) in relation to fitness, physical activity, and adipokine levels in childhood: The european youth heart study. Environ. Res. 2020, 191, 110110. [Google Scholar] [CrossRef]
- Boronow, K.E.; Brody, J.G.; Schaider, L.A.; Peaslee, G.; Havas, L.; Cohn, B.A. Serum concentrations of PFASs and exposure-related behaviors in African American and non-Hispanic white women. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 206–217. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.B.; Ducatman, A. Roles of gender and obesity in defining correlations between perfluoroalkyl substances and lipid/lipoproteins. Sci. Total Environ. 2018, 653, 74–81. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Perfluoroalkyls (Draft for Public Comment). US Department of Health and Human Services, Public Health Service: Atlanta, GA, USA, 2018. Available online: https://www.congress.gov/116/meeting/house/109020/documents/HHRG-116-GO28-20190306-SD001.pdf (accessed on 16 February 2022).
- Parker, H.W.; Abreu, A.M.; Sullivan, M.C.; Vadiveloo, M.K. Allostatic Load and Mortality: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E.; Obeng-Gyasi, B. Chronic Stress and Cardiovascular Disease among Individuals Exposed to Lead: A Pilot Study. Diseases 2020, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Obeng-Gyasi, E. Cumulative Effects of Low-Level Lead Exposure and Chronic Physiological Stress on Hepatic Dysfunction—A Preliminary Study. Med. Sci. 2020, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Rodriquez, E.J.; Livaudais-Toman, J.; Gregorich, S.E.; Jackson, J.S.; Nápoles, A.M.; Pérez-Stable, E.J. Relationships between allostatic load, unhealthy behaviors, and depressive disorder in U.S. adults, 2005–2012 NHANES. Prev. Med. 2018, 110, 9–15. [Google Scholar] [CrossRef]
- Seeman, T.E.; Lusignolo, T.M.; Albert, M.; Berkman, L. Social relationships, social support, and patterns of cognitive aging in healthy, high-functioning older adults: MacArthur studies of successful aging. Health Psychol. 2001, 20, 243. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, P.D.; Culhane, J.F.; Rauh, V.; Barve, S.S.; Hogan, V.; Sandman, C.A.; Hobel, C.J.; Chicz-DeMet, A.; Dunkel-Schetter, C.; Garite, T.J.; et al. Stress, infection and preterm birth: A biobehavioural perspective. Paediatr. Périnat. Epidemiol. 2001, 15, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-J.; Heo, S.-H.; Lee, D.-S.; Hwang, I.G.; Lee, Y.-B.; Cho, H.-Y. Gender differences in pharmacokinetics and tissue distribution of 3 perfluoroalkyl and polyfluoroalkyl substances in rats. Food Chem. Toxicol. 2016, 97, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Cheng, Y.; Xie, Z.; Zeng, F. Perfluorinated alkyl substances in serum of the southern Chinese general population and potential impact on thyroid hormones. Sci. Rep. 2017, 7, 43380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.S.; Choi, J.-S.; Park, J.-W. Transcriptional changes in steroidogenesis by perfluoroalkyl acids (PFOA and PFOS) regulate the synthesis of sex hormones in H295R cells. Chemosphere 2016, 155, 436–443. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | |||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Ethnicity | Race | Number | Percent | Number | Percent |
| Hispanic | Mexican American | 1715 | 49.3 | 1765 | 50.7 |
| Other Hispanic | 1060 | 44.5 | 1324 | 55.5 | |
| Non-Hispanic | Non-Hispanic White | 5052 | 49.3 | 5198 | 50.7 |
| Non-Hispanic Black | 2419 | 48.6 | 2562 | 51.4 | |
| * Other Race Including Multi-Racial | 1168 | 48.9 | 1219 | 51.1 | |
| Total | 11,414 | 48.12 | 12,068 | 51.88 | |
| PFAS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | PFDE | PFNA | PFOS | PFUA | PFOA | PFHS | ||||||
| AL | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| high | 0.159 | 0.613 | 0.440 | 1.244 | 3.295 | 10.108 | 0.133 | 0.857 | 0.828 | 1.894 | 0.730 | 1.954 |
| low | 0.159 | 0.418 | 0.422 | 0.861 | 3.167 | 8.879 | 0.132 | 0.497 | 0.883 | 2.154 | 0.709 | 1.808 |
| Physical Activity | ||||||||||||
| 1 day | 0.163 | 0.285 | 0.459 | 0.971 | 3.341 | 8.386 | 0.136 | 0.290 | 0.976 | 2.022 | 0.796 | 2.085 |
| 2 days | 0.154 | 0.239 | 0.460 | 1.078 | 3.214 | 8.443 | 0.129 | 0.220 | 0.892 | 2.211 | 0.767 | 1.945 |
| 3 days | 0.159 | 0.539 | 0.423 | 1.062 | 3.182 | 9.326 | 0.134 | 0.765 | 0.846 | 2.062 | 0.701 | 1.863 |
| 4 days | 0.151 | 0.203 | 0.426 | 0.804 | 3.025 | 8.089 | 0.121 | 0.175 | 0.844 | 1.758 | 0.724 | 1.730 |
| 5 days | 0.171 | 0.758 | 0.448 | 0.839 | 3.426 | 10.991 | 0.126 | 0.222 | 0.895 | 1.860 | 0.788 | 1.757 |
| 6 days | 0.152 | 0.258 | 0.416 | 0.685 | 4.155 | 17.440 | 0.132 | 0.254 | 0.997 | 2.240 | 0.819 | 2.124 |
| 7 days | 0.161 | 0.278 | 0.422 | 0.850 | 3.251 | 8.358 | 0.137 | 0.272 | 0.856 | 2.178 | 0.674 | 1.615 |
| Smoking | ||||||||||||
| yes | 0.156 | 0.375 | 0.441 | 0.900 | 3.476 | 10.214 | 0.129 | 0.556 | 0.926 | 2.040 | 0.782 | 1.891 |
| no | 0.161 | 0.581 | 0.420 | 1.112 | 3.016 | 8.660 | 0.136 | 0.728 | 0.813 | 2.071 | 0.668 | 1.844 |
| Alcohol | ||||||||||||
| 1 day | 0.1626 | 0.2847 | 0.4591 | 0.9708 | 3.341 | 8.386 | 0.1358 | 0.2896 | 0.976 | 2.0225 | 0.7956 | 2.0852 |
| 2 days | 0.154 | 0.2389 | 0.4599 | 1.0781 | 3.214 | 8.443 | 0.1291 | 0.2198 | 0.8924 | 2.2108 | 0.767 | 1.9453 |
| 3 days | 0.1589 | 0.5388 | 0.4231 | 1.0619 | 3.182 | 9.326 | 0.1337 | 0.7649 | 0.8456 | 2.0616 | 0.7013 | 1.8627 |
| 4 days | 0.1512 | 0.2028 | 0.4256 | 0.8036 | 3.025 | 8.089 | 0.1213 | 0.1745 | 0.8445 | 1.7576 | 0.7242 | 1.7302 |
| 5 days | 0.1708 | 0.7576 | 0.4478 | 0.8389 | 3.426 | 10.99 | 0.126 | 0.2216 | 0.8952 | 1.8603 | 0.7876 | 1.7571 |
| 6 days | 0.1521 | 0.2577 | 0.416 | 0.685 | 4.155 | 17.44 | 0.1324 | 0.2543 | 0.9971 | 2.2396 | 0.8193 | 2.1238 |
| 7 days | 0.1611 | 0.278 | 0.4221 | 0.8499 | 3.251 | 8.358 | 0.1372 | 0.2722 | 0.8561 | 2.1779 | 0.674 | 1.6147 |
| Age Group | Mean Score Allostatic Load | Percentage of 3 or More (High) | Percentage of Less Than 3 (Low) |
|---|---|---|---|
| Age 20 to 39 | |||
| Mexican | 2.90 | 28.60 | 71.40 |
| NH/Black | 3.32 | 40.00 | 60.00 |
| NH/White | 2.66 | 22.70 | 77.30 |
| O/Hispanic | 2.69 | 23.40 | 76.60 |
| ONH/Mul/Asian | 2.63 | 19.70 | 80.30 |
| Age 40 to 59 | |||
| Mexican | 3.49 | 44.80 | 55.20 |
| NH/Black | 3.92 | 57.60 | 42.40 |
| NH/White | 3.26 | 38.50 | 61.50 |
| O/Hispanic | 3.47 | 43.30 | 56.70 |
| ONH/Mul/Asian | 3.08 | 32.60 | 67.40 |
| Age 60 and up | |||
| Mexican | 3.58 | 47.40 | 52.60 |
| NH/Black | 3.83 | 56.00 | 44.00 |
| NH/White | 3.37 | 41.10 | 58.90 |
| O/Hispanic | 3.64 | 47.50 | 52.50 |
| ONH/Mul/Asian | 3.13 | 33.20 | 66.80 |
| PFASs | ||||||
|---|---|---|---|---|---|---|
| PFHS | PFDE | PFNA | PFUA | PFOA | PFOS | |
| PFHS | 1.000 | 0.196 | 0.404 | 0.112 | 0.516 | 0.539 |
| PFDE | 0.196 | 1.000 | 0.362 | 0.792 | 0.240 | 0.447 |
| PFNA | 0.404 | 0.362 | 1.000 | 0.260 | 0.542 | 0.566 |
| PFUA | 0.112 | 0.792 | 0.260 | 1.000 | 0.115 | 0.231 |
| PFOA | 0.516 | 0.240 | 0.542 | 0.115 | 1.000 | 0.674 |
| PFOS | 0.539 | 0.447 | 0.566 | 0.231 | 0.674 | 1.000 |
| Variable | Coeff | SE | p-Value | (95% CI) | VIF | |
|---|---|---|---|---|---|---|
| PFDE | 0.082 | 0.068 | 0.234 | −0.054 | 0.219 | 2.092 |
| PFNA | −0.081 | 0.051 | 0.119 | −0.184 | 0.021 | 6.197 |
| PFOS | 0.002 | 0.002 | 0.391 | −0.002 | 0.125 | 6.212 |
| PFUA | 0.030 | 0.048 | 0.542 | −0.067 | 0.126 | 2.467 |
| PFOA | 0.023 | 0.008 | 0.006 | 0.007 | 0.395 | 5.139 |
| PFHS | 0.002 | 0.002 | 0.391 | −0.002 | 0.102 | 1.667 |
| Variable | Coeff | SE | p Value |
|---|---|---|---|
| PFDE | −0.089 | 0.027 | 0.002 |
| PFNA | −0.111 | 0.035 | 0.002 |
| PFOS | 0.005 | 0.002 | 0.032 |
| PFUA | 0.053 | 0.083 | 0.531 |
| PFOA | 0.027 | 0.008 | 0.002 |
| PFHS | 0.005 | 0.002 | 0.032 |
| Gender | |||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Behavioral Health Covariates | Status | Number | Percent | Number | Percent |
| Alcohol | yes | 9385 | 55.2 | 7605 | 44.8 |
| no | 1630 | 28.7 | 4053 | 71.3 | |
| Smoking | yes | 5986 | 58.6 | 4229 | 41.4 |
| no | 5029 | 40.4 | 7429 | 59.6 | |
| Physical Activities | |||||
| 1 day | At least ten minutes/day | 842 | 61.5 | 528 | 49.5 |
| 2 days | At least ten minutes/day | 878 | 49.5 | 896 | 50.5 |
| 3 days | At least ten minutes/day | 7559 | 47.4 | 8393 | 52.6 |
| 4 days | At least ten minutes/day | 420 | 44.9 | 515 | 55.1 |
| 5 days | At least ten minutes/day | 572 | 47.5 | 632 | 52.5 |
| 6 days | At least ten minutes/day | 153 | 48.3 | 164 | 51.7 |
| 7 days | At least ten minutes/day | 591 | 52.7 | 530 | 47.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bashir, T.; Obeng-Gyasi, E. The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load. Int. J. Environ. Res. Public Health 2022, 19, 5455. https://doi.org/10.3390/ijerph19095455
Bashir T, Obeng-Gyasi E. The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load. International Journal of Environmental Research and Public Health. 2022; 19(9):5455. https://doi.org/10.3390/ijerph19095455
Chicago/Turabian StyleBashir, Tahir, and Emmanuel Obeng-Gyasi. 2022. "The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load" International Journal of Environmental Research and Public Health 19, no. 9: 5455. https://doi.org/10.3390/ijerph19095455
APA StyleBashir, T., & Obeng-Gyasi, E. (2022). The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load. International Journal of Environmental Research and Public Health, 19(9), 5455. https://doi.org/10.3390/ijerph19095455