
Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers

 ,
,  ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
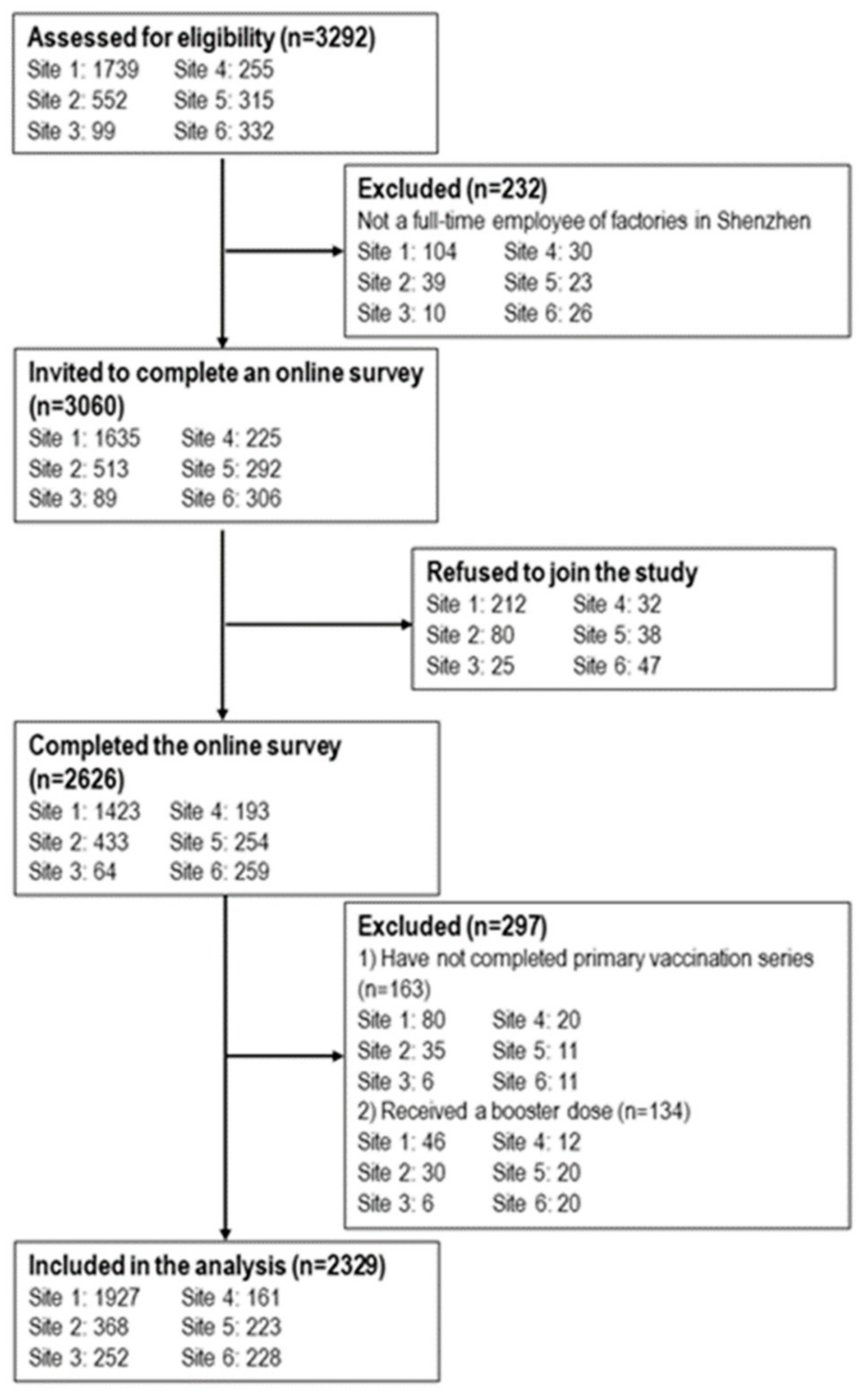
2.2. Participants and Data Collection
2.3. Measurements
2.3.1. Questionnaire Development
2.3.2. Background Characteristics
2.3.3. Dependent Variable: Behavioral Intention to Receive a Booster Dose of COVID-19 Vaccine
2.3.4. Independent Variables at the Individual Level
2.3.5. Independent Variables at the Interpersonal Level
2.4. Sample Size Calculation
2.5. Ethics Statement
2.6. Statistical Analysis
3. Results
3.1. Background Characteristics of the Participants
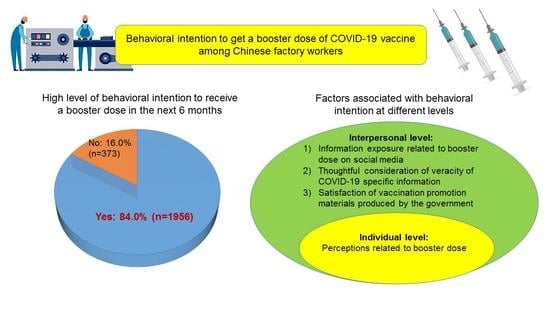
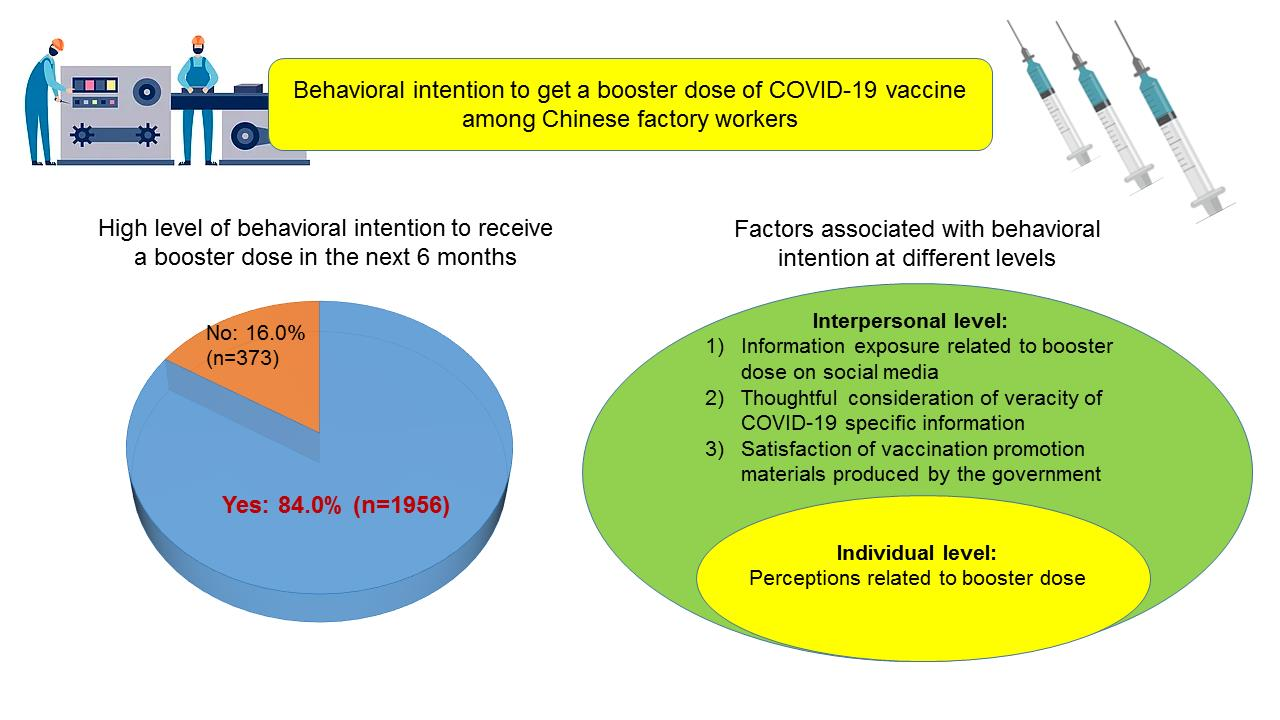
3.2. Behavioral Intention to Receive a Booster Dose of COVID-19 Vaccine
3.3. Independent Variables at Individual and Interpersonal Levels
3.4. Factors Associated with Behavioral Intention to Receive a Booster Dose of COVID-19 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). COVID-19 ACIP Vaccine Recommendations. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html (accessed on 24 September 2021).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. 2021. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 27 October 2021).
- Bayart, J.L.; Douxfils, J.; Gillot, C.; David, C.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Gerin, V.; et al. Waning of IgG, total and neutralizing antibodies 6 months post-vaccination with BNT162b2 in healthcare workers. Vaccines 2021, 9, 1092. [Google Scholar] [CrossRef] [PubMed]
- Yue, L.; Xie, T.; Yang, T.; Zhou, J.; Chen, H.; Zhu, H.; Li, H.; Xiang, H.; Wang, J.; Yang, H.J.; et al. A third booster dose may be necessary to mitigate neutralizing antibody fading after inoculation with two doses of an inactivated SARS-CoV-2 vaccine. J. Med. Virol. 2022, 94, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.M.; Oestreicher, J.; Colpitts, T.; et al. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters in healthy adults: An interim analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Interim Statement on Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 24 November 2021).
- Falsey, A.R.; Frenck, R.W., Jr.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 neutralization with BNT162b2 vaccine dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, A.; Marchevsky, N.G.; Jenkin, D.; Aboagye, J.; Aley, P.K.; Angus, B.; Belij-Rammerstorfer, S.; Bibi, S.; Bittaye, M.; Cappuccini, F.; et al. Reactogenicity and immunogenicity after a late second dose or a third dose of ChAdOx1 nCoV-19 in the UK: A substudy of two randomised controlled trials (COV001 and COV002). Lancet 2021, 398, 981–990. [Google Scholar] [CrossRef]
- Hause, A.M.; Baggs, J.; Gee, J.; Marquez, P.; Myers, T.R.; Shimabukuro, T.T.; Shay, D.K. Safety monitoring of an additional dose of COVID-19 vaccine—United States, August 12–September 19, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1379–1384. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. State Council COVID-19 Prevention and Control Press Release on November 20, 2021. Available online: http://www.nhc.gov.cn/wjw/xwfbh/xwzb.shtml (accessed on 24 November 2021).
- National Health Commission of the People’s Republic of China. Statistics on COVID-19 Vaccination October 27, 2021. Available online: http://www.nhc.gov.cn/xcs/yqjzqk/list_gzbd.shtml (accessed on 24 November 2021).
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 20 September 2021).
- Ipsos Survey for the World Economic Forum. Global Attitudes on COVID 19 Vaccine Booster Shots. Available online: https://www.ipsos.com/sites/default/files/ct/news/documents/2021-09/Global-attitudes-about-COVID-19-Vaccine-Booster-Shots-Sept-2021.pdf (accessed on 24 November 2021).
- Imperial College London. UK and USA Attitudes towards COVID-19 Booster Vaccines. Available online: https://www.imperial.ac.uk/media/imperial-college/institute-of-global-health-innovation/UK_US-vaccine-insights_ICL-YouGov-Covid-19-Behaviour-Tracker_20210625_final.pdf (accessed on 24 November 2021).
- KFF. KFF COVID-19 Vaccine Monitor: October 2021. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-october-2021/ (accessed on 24 November 2021).
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing acceptability of COVID-19 vaccine booster dose among adult Americans: A cross-sectional survey. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedzialek, B.; Fal, A. Willingness to receive the booster COVID-19 vaccine dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Bakicki, M.; Mastalerz-Migas, A. Attitudes of Poles towards the COVID-19 vaccine booster dose: An online survey in Poland. Vaccines 2022, 10, 68. [Google Scholar] [CrossRef]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a third dose of COVID-19 vaccine and associated factors in China based on Health Belief Model: A national cross-sectional study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 vaccine hesitancy and attitude toward booster doses among US healthcare workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef] [PubMed]
- Klugar, M.; Riad, A.; Mohanan, L.; Pokorna, A. COVID-19 vaccine booster hesitancy (VBH) of healthcare workers in Czechia: National cross-sectional study. Vaccines 2021, 9, 1437. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K. Attitudes of medical students toward COVID-19 vaccination: Who is willing to receive a third dose of the vaccine? Vaccines 2021, 9, 1295. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Fang, Y.; Xin, M.; Dong, W.; Zhou, L.; Hou, Q.; Li, F.P.; Sun, G.; Zheng, Z.L.; Yuan, J.Q.; et al. Self-reported compliance with personal preventive measures among Chinese factory workers at the beginning of work resumption following the COVID-19 outbreak: Cross-sectional survey study. J. Med. Internet Res. 2020, 22, e22457. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Xin, M.; Zhang, C.; Dong, W.; Fang, Y.; Wu, W.; Li, M.Z.; Pang, J.; Zheng, Z.L.; Wang, Z.X.; et al. Associations of mental health and personal preventive measure compliance with exposure to COVID-19 information during work resumption following the COVID-19 outbreak in China: Cross-sectional survey study. J. Med. Internet Res. 2020, 22, e22596. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Labor. Protecting Miners: MSHA Guidance on Migrating and Preventing the Spread of COVID-19. Available online: https://www.msha.gov/protecting-miners (accessed on 12 April 2022).
- Wall, R.; Cholak, A. COVID-19 Prevention for Manufacturing Industries. Available online: https://int-es.com/news/covid-19-prevention-for-manufacturing-industries/ (accessed on 12 April 2022).
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.F.; Wang, Z.X. Behavioral intention to receive a COVID-19 vaccination among Chinese factory workers: Cross-sectional online survey. J. Med. Internet Res. 2021, 23, e24673. [Google Scholar] [CrossRef]
- Zhang, K.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Parental acceptability of COVID-19 vaccination for children under the age of 18 years in China: Cross-sectional online survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef]
- Singh, A.; Lai, A.H.Y.; Wang, J.; Asim, S.; Chan, P.S.; Wang, Z.; Yeoh, E.K. Multilevel determinants of COVID-19 vaccine uptake among South Asian ethnic minorities in Hong Kong: Cross-sectional web-based survey. JMIR Public Health Surveill. 2021, 7, e31707. [Google Scholar] [CrossRef]
- Huang, X.; Yu, M.; Fu, G.; Lan, G.; Li, L.; Yang, J.; Qiao, Y.; Zhao, J.; Qian, H.Z.; Zhang, X.; et al. Willingness to receive COVID-19 vaccination among people living with HIV and AIDS in China: A nationwide cross-sectional online survey. JMIR Public Health Surveill. 2021, 7, e31125. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Chernev, A.; Bockenholt, U.; Goodman, J. Choice overload: A conceptual review and meta-analysis. J. Consum. Psychol. 2015, 25, 333–358. [Google Scholar] [CrossRef]
- Horton, R. Offline: Managing the COVID-19 vaccine infodemic. Lancet 2020, 396, 1474. [Google Scholar] [CrossRef]
- BBC News. Why Should We Pay More Attention to the Low Uptake Rate of COVID-19 Vaccination among Older Adults. 2021. Available online: https://www.bbc.com/zhongwen/simp/chinese-news-58497197 (accessed on 24 September 2021).
- Commerce Bureau of Shenzhen Municipality. Longhua District. Available online: http://commerce.sz.gov.cn/tzly/qyfb/gqcyjs/content/post_8571905.html (accessed on 18 January 2022).
- Yuan, J.; Cao, B.; Zhang, C.; Chan, P.S.F.; Xin, M.; Fang, Y.; Chen, Y.; Huang, D.; Li, L.; Xuan, X.; et al. Changes in compliance with personal preventive measures and mental health status among Chinese factory workers during the COVID-19 pandemic: An observational prospective cohort study. Front. Public Health 2022, 10, 831456. [Google Scholar] [CrossRef]
- The Ottawa Hospital Research Institute. The SURE Test Version of Decisional Conflict Scale. Available online: https://decisionaid.ohri.ca/docs/develop/Tools/DCS_SURE_Mandarin.pdf (accessed on 16 November 2021).
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccle, M. From theory to intervention: Mapping theoretically derived behavioral determinants to behavior change techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Stewart, G.L.; Courtright, S.H.; Barrick, M.R. Peer-based control in self-managing teams: Linking rational and normative influence with individual and group performance. J. Appl. Psychol. 2012, 97, 435–447. [Google Scholar] [CrossRef] [Green Version]
- Teyssou, E.; Delagrèverie, H.; Visseaux, B.; Lambert-Niclot, S.; Brichler, S.; Ferre, V.; Marot, S.; Jary, A.; Todesco, E.; Schnuriger, A.; et al. The Delta SARS-CoV-2 variant has a higher viral load than the Beta and the historical variants in nasopharyngeal samples from newly diagnosed COVID-19 patients. J. Infect. 2021, 83, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Deng, A.; Li, K.; Hu, Y.; Li, Z.; Xiong, Q.; Liu, Z.; Guo, Q.; Zou, L.; Zhang, H.; et al. Viral Infection and Transmission in a Large, Well-Traced Outbreak Caused by the SARS-CoV-2 Delta Variant. medRxiv Preprint. 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.07.07.21260122v2 (accessed on 2 December 2021).
- Tsao, S.F.; Chen, H.; Tisseverasinghe, T.; Yang, Y.; Li, L.; Butt, Z.A. What social media told us in the time of COVID-19: A scoping review. Lancet Digit. Health 2021, 3, e175–e194. [Google Scholar] [CrossRef]
- Blevins, D.; Farmer, M.S.; Edlund, C.; Sullivan, G.; Kirchner, J.E. Collaborative research between clinicians and researchers: A multiple case study of implementation. Implement. Sci. IS 2010, 5, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finegood, D.; Johnston, L.; Steinberg, M.; Matteson, C.L.; Deck, P.B. Complexity, Systems Thinking, and Health Behavior Change; Oxford University Press: New York, NY, USA, 2011; pp. 208–236. [Google Scholar]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Ver-loigne, M.; Chastin, S.F.M. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Galvagno, M.; Dalli, D. Theory of value co-creation: A systematic literature review. Manag. Serv. Qual. Int. J. 2014, 24, 643–683. [Google Scholar] [CrossRef]
- Sanders, E.B.N.; Stappers, P.J. Co-creation and the new landscapes of design. Co-Design 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute. Greater Than the Sum: Systems Thinking in Tobacco Control: Natl; Institutes Heal: Rockville, MD, USA, 2007; pp. 1–67. [Google Scholar]


{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Sociodemographic | |
| Age group, years | |
| 18–29 | 614 (26.4) |
| 30–39 | 1064 (45.7) |
| 40–49 | 514 (22.1) |
| ≥50 | 137 (5.9) |
| Gender | |
| Male | 1147 (49.2) |
| Female | 1182 (50.8) |
| Internal migrant | |
| No | 265 (11.4) |
| Yes | 2064 (88.6) |
| Relationship status | |
| Currently single | 492 (21.1) |
| Having a stable boyfriend/girlfriend | 164 (7.0) |
| Married | 1673 (71.8) |
| Having children | |
| No | 712 (30.6) |
| Yes | 1617 (69.4) |
| Highest education level attained | |
| Junior high or below | 580 (24.9) |
| Senior high or equivalent | 678 (29.1) |
| College/university or above | 1071 (46.0) |
| Monthly personal income, CNY (USD) | |
| <3000 (463.84) | 332 (14.3) |
| 3000–4999 (463.84–772.92) | 648 (27.8) |
| 5000–6999 (773.07, 1082.15) | 766 (32.9) |
| 7000–9999 (1082.30–1545.99) | 386 (16.6) |
| ≥10,000 (1546.14) | 197 (8.5) |
| Type of work | |
| Frontline workers | 1583 (68.0) |
| Management staff | 746 (32.0) |
| Type of factory | |
| Electronic device manufacturers | 1399 (60.1) |
| Other factories | 930 (39.9) |
| Uptake of COVID-19 vaccine | |
| Time interval between the completion of initial doses and the survey date | |
| <1 month | 40 (1.7) |
| 1–3 months | 872 (37.4) |
| 4–6 months | 1321 (56.7) |
| >6 months | 96 (4.1) |
| Self-reported severity of side-effects after COVID-19 vaccination | |
| Not at all | 1520 (65.3) |
| Very mild | 500 (21.5) |
| Mild | 276 (11.9) |
| Moderate | 28 (1.2) |
| Severe | 3 (0.1) |
| Very severe | 2 (0.1) |
| Have not received any COVID-19 vaccine | 0 (0.0) |
| Personal COVID-19 preventive measures in the past month | |
| Frequency of wearing a facemask in public places/transportation other than the workplace | |
| Every time | 1996 (85.7) |
| Often | 270 (11.6) |
| Sometimes | 60 (2.6) |
| Never | 3 (0.1) |
| Frequency of wearing a facemask when you have close contact with other people in the workplace | |
| Every time | 1706 (73.3) |
| Often | 470 (20.2) |
| Sometimes | 137 (5.9) |
| Never | 16 (0.7) |
| Self-reported sanitizing hands (using soaps, liquid soaps, or alcohol-based sanitizer) after returning from public spaces or touching public installation | |
| Every time | 1284 (55.1) |
| Often | 582 (25.0) |
| Sometimes | 409 (17.6) |
| Never | 54 (2.3) |
| Self-reported avoiding social gathering with other people who do not live together | |
| No | 946 (40.6) |
| Yes | 1383 (59.4) |
| Self-reported avoiding crowded places | |
| No | 799 (34.3) |
| Yes | 1530 (65.7) |
| COVID-19 prevention measures implemented by the factories in the past month, n (%) yes | |
| Prohibiting non-employees from entering workplace | 1622 (69.6) |
| Taking body temperature and sanitizing hands for all employees entering the workplace | 1940 (83.3) |
| Providing facemasks to all employees | 1995 (85.7) |
| Keeping adequate distance (e.g., >1 m) between work stations | |
| Requiring employees to wear facemasks when they have close contact with other people | 1725 (74.1) |
| Frequent workplace disinfection | 1988 (85.4) |
| Maintaining adequate ventilation in workplace | 1953 (83.9) |
| Setting up partitions in factory canteens | 2089 (89.7) |
| Requiring employees to receive COVID-19 vaccination | 1724 (74.0) |
| Number of COVID-19 prevention measures implemented by the factories, mean (SD) | 7.2 (2.5) |
| n (%) | |
|---|---|
| Behavioral Intention | |
| Intention to get a booster dose of COVID-19 vaccine in the next six months | |
| Very unlikely/unlikely/neutral | 373 (16.0) |
| Likely/very likely | 1956 (84.0) |
| Individual-level factors | |
| Perceived risk of contracting Delta variant of COVID-19, n (%) high | 1397 (60.0) |
| Response score, mean (SD) | 2.6 (0.5) |
| Perceived chance of having severe consequence if contracting Delta variant of COVID-19, n (%) high | 1099 (47.2) |
| Response score, mean (SD) | 2.4 (0.6) |
| Perceived benefit of booster dose of COVID-19 vaccine, n (%) agree | |
| Receiving a booster dose can maintain your antibody level and strengthen the protection against COVID-19 | 1786 (76.7) |
| A booster dose is highly effective in protecting you from COVID-19 | 1728 (74.2) |
| China has sufficient supply of booster doses of COVID-19 vaccines | 1571 (67.5) |
| Perceived Benefit Scale 1 | |
| Scale score, mean (SD) | 8.1 (1.2) |
| Perceived barrier of receiving booster dose of COVID-19 vaccine, n (%) agree | |
| You will have severe side effects after receiving a booster dose | 331 (14.2) |
| The harms of a booster dose is unclear in long run | 383 (16.4) |
| The protection of a booster dose will only last for a short time | 393 (16.9) |
| Perceived Barrier Scale 2 | |
| Scale score, mean (SD) | 5.7 (1.6) |
| People who are important to you will suggest you to receive a booster dose of COVID-19 vaccine, n (%) agree | 1708 (73.3) |
| Response score, mean (SD) | 2.7 (0.5) |
| It is easy for you to receive a booster dose of COVID-19 vaccine if you want to, n (%) agree | 1454 (62.4) |
| Response score, mean (SD) | 2.6 (0.6) |
| The SURE test version of Decisional Conflict Scale, n (%) Yes | |
| There are different choices of a booster dose… | |
| Do you feel sure about the best choice for you? | 856 (36.8) |
| Do you know the benefits and risks of each option? | 767 (32.9) |
| Are you clear about which benefits and risks matter most to you? | 669 (28.7) |
| Do you have enough support and advice to make a choice? | 918 (39.4) |
| The SURE test version of Decisional Conflict Scale 3 | |
| Scale score, mean (SD) | 1.4 (1.6) |
| Interpersonal-level variables | |
| Frequency of exposing to the following information on social media (e.g., WeChat, WeChat moments, Weibo, TikTok) in the past month | |
| COVID-19 pandemic is not under control in some countries after scaling up COVID-19 vaccination | |
| Almost none | 464 (19.9) |
| Seldom | 725 (31.1) |
| Sometimes | 705 (30.3) |
| Always | 435 (18.7) |
| Response score, mean (SD) | 2.5 (1.0) |
| Infectiousness and harms of the Delta variant of COVID-19 | |
| Almost none | 299 (12.8) |
| Seldom | 590 (25.3) |
| Sometimes | 803 (34.5) |
| Always | 637 (27.4) |
| Response score, mean (SD) | 2.8 (1.0) |
| Outbreak of Delta variant of COVID-19 in some places of China | |
| Almost none | 376 (16.1) |
| Seldom | 782 (33.6) |
| Sometimes | 820 (35.2) |
| Always | 351 (15.1) |
| Response score, mean (SD) | 2.5 (0.9) |
| People contract COVID-19 after receiving primary series of COVID-19 vaccination | |
| Almost none | 522 (22.4) |
| Seldom | 1048 (35.0) |
| Sometimes | 622 (26.7) |
| Always | 137 (5.9) |
| Response score, mean (SD) | 2.1 (0.8) |
| Thoughtful consideration of the veracity of COVID-19-specific information | |
| Almost none | 368 (15.8) |
| Seldom | 523 (22.5) |
| Sometimes | 790 (33.9) |
| Always | 648 (27.8) |
| Response score, mean (SD) | 2.7 (1.0) |
| Satisfaction of COVID-19 vaccination health promotion materials (e.g., advertisement, poster, and others) produced by the government | |
| Amount of information | |
| Just right | 1695 (72.8) |
| Too much | 431 (18.5) |
| Too little | 203 (8.7) |
| Can address your concerns related to COVID-19 vaccination | |
| No/uncertain | 795 (34.1) |
| Yes | 1534 (65.9) |
| Helpful for you to make decision on whether to receive a COVID-19 vaccine | |
| No/uncertain | 293 (12.6) |
| Yes | 2036 (87.4) |
| OR (95% CI) | p Values | |
|---|---|---|
| Sociodemographic | ||
| Age group, years | ||
| 18–29 | 1.0 | |
| 30–39 | 0.86 (0.66, 1.13) | 0.27 |
| 40–49 | 1.04 (0.75, 1.45) | 0.81 |
| ≥50 | 1.20 (0.70, 2.06) | 0.52 |
| Gender | ||
| Male | 1.0 | |
| Female | 1.26 (1.01, 1.58) | 0.04 |
| Internal migrant | ||
| No | 1.0 | |
| Yes | 1.18 (0.85, 1.65) | 0.32 |
| Relationship status | ||
| Currently single | 1.0 | |
| Having a stable boyfriend/girlfriend | 1.78 (1.05, 3.02) | 0.03 |
| Married | 1.26 (0.97, 1.64) | 0.08 |
| Having children | ||
| No | 1.0 | |
| Yes | 1.23 (0.97, 1.55) | 0.09 |
| Highest education level attained | ||
| Junior high or below | 1.0 | |
| Senior high or equivalent | 1.26 (0.95, 1.68) | 0.11 |
| College/university or above | 1.64 (1.25, 2.15) | <0.001 |
| Monthly personal income, CNY (USD) | ||
| <3000 (463.84) | 1.0 | |
| 3000–4999 (463.84–772.92) | 1.32 (0.94, 1.86) | 0.11 |
| 5000–6999 (773.07, 1082.15) | 1.59 (1.14, 2.23) | 0.01 |
| 7000–9999 (1082.30–1545.99) | 1.23 (0.84, 1.79) | 0.29 |
| ≥10,000 (1546.14) | 1.35 (0.85, 2.16) | 0.20 |
| Type of work | ||
| Frontline workers | 1.0 | |
| Management staff | 1.46 (1.14, 1.88) | 0.003 |
| Type of factory | ||
| Electronic device manufacturers | 1.0 | |
| Other factories | 1.03 (0.82, 1.29) | 0.82 |
| Uptake of COVID-19 vaccine | ||
| Time interval between the completion of initial doses and the survey date | ||
| ≤3 month | 1.0 | |
| 4–6 months | 1.10 (0.87, 1.38) | 0.43 |
| >6 months | 1.76 (0.90, 3.50) | 0.10 |
| Self-reported severity of side-effects after COVID-19 vaccination | ||
| Not at all | 1.0 | |
| Very mild/mild | 1.09 (0.86, 1.39) | 0.47 |
| Moderate/severe/very severe | 0.52 (0.24, 1.13) | 0.09 |
| Personal COVID-19 preventive measures in the past month | ||
| Frequency of wearing a facemask in public places/transportation other than the workplace | ||
| Never/sometimes/often | 1.0 | |
| Every time | 1.46 (1.09, 1.95) | 0.01 |
| Frequency of wearing a facemask when you have close contact with other people in the workplace | ||
| Never/sometimes/often | 1.0 | |
| Every time | 1.14 (0.89, 1.46) | 0.29 |
| Self-reported sanitizing hands (using soaps, liquid soaps, or alcohol-based sanitizer) after returning from public spaces or touching public installation | ||
| Never/sometimes/often | 1.0 | |
| Every time | 0.96 (0.77, 1.20) | 0.70 |
| Self-reported avoiding social gathering with other people who do not live together | ||
| No | 1.0 | |
| Yes | 1.55 (1.24, 1.93) | <0.001 |
| Self-reported avoiding crowded places | ||
| No | 1.0 | |
| Yes | 1.61 (1.29, 2.02) | <0.001 |
| COVID-19 prevention measures implemented by the factories in the past month | ||
| Number of COVID-19 prevention measures implemented by the factories | 1.12 (1.08, 1.17) | <0.001 |
| OR (95% CI) | p Values | AOR (95% CI) | p Values | |
|---|---|---|---|---|
| Individual-Level Factors | ||||
| Perceived risk of contracting Delta variant of COVID-19 | 1.67 (1.36, 2.05) | <0.001 | 1.53 (1.24, 1.90) | <0.001 |
| Perceived chance of having severe consequence if contracting Delta variant of COVID-19 | 1.59 (1.31, 1.93) | <0.001 | 1.45 (1.18, 1.77) | <0.001 |
| Perceived Benefit Scale | 1.73 (1.59, 1.88) | <0.001 | 1.71 (1.57, 1.87) | <0.001 |
| Perceived Barrier Scale | 0.80 (0.74, 0.85) | <0.001 | 0.80 (0.74, 0.85) | <0.001 |
| People who are important to you will suggest you to receive a booster dose of COVID-19 vaccine | 3.22 (2.67, 3.89) | <0.001 | 2.53 (2.09, 3.77) | <0.001 |
| It is easy for you to receive a booster dose of COVID-19 vaccine if you want to | 2.20 (1.86, 2.60) | <0.001 | 2.04 (1.72, 2.43) | <0.001 |
| The SURE test version of Decisional Conflict Scale | 1.12 (1.04, 1.20) | 0.003 | 1.07 (0.99, 1.15) | 0.10 |
| Interpersonal-level variables | ||||
| Frequency of exposing to the following information on social media (e.g., WeChat, WeChat moments, Weibo, TikTok) in the past month | ||||
| COVID-19 pandemic is not under control in some countries after scaling up COVID-19 vaccination | 1.26 (1.12, 1.40) | <0.001 | 1.26 (1.13, 1.41) | <0.001 |
| Infectiousness and harms of the Delta variant of COVID-19 | 1.40 (1.25, 1.56) | <0.001 | 1.38 (1.23, 1.54) | <0.001 |
| Outbreak of Delta variant of COVID-19 in some places of China | 1.31 (1.16, 1.48) | <0.001 | 1.32 (1.16, 1.49) | <0.001 |
| People contract COVID-19 after receiving primary series of COVID-19 vaccination | 1.14 (1.00, 1.31) | 0.051 | 1.13 (0.99, 1.30) | 0.08 |
| Thoughtful consideration of the veracity of COVID-19-specific information | 1.38 (1.24, 1.54) | <0.001 | 1.35 (1.21, 1.50) | <0.001 |
| Acceptance of COVID-19 vaccination health promotion materials (e.g., advertisement, poster, and others) produced by the government | ||||
| Amount of information | ||||
| Just right | 1.0 | 1.0 | ||
| Too much | 0.79 (0.60, 1.05) | 0.10 | 0.77 (0.58, 1.03) | 0.08 |
| Too little | 0.57 (0.40, 0.81) | 0.002 | 0.70 (0.48, 1.00) | 0.052 |
| Can address your concerns related to COVID-19 vaccination | ||||
| No/uncertain | 1.0 | 1.0 | ||
| Yes | 2.32 (1.85, 2.90) | <0.001 | 2.04 (1.62, 2.57) | <0.001 |
| Helpful for you to make decision on whether to receive a COVID-19 vaccine | ||||
| No/uncertain | 1.0 | 1.0 | ||
| Yes | 4.45 (3.40, 5.82) | <0.001 | 3.87 (2.91, 5.14) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, K.; Fang, Y.; Chan, P.S.-f.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers. Int. J. Environ. Res. Public Health 2022, 19, 5245. https://doi.org/10.3390/ijerph19095245
Zhang K, Fang Y, Chan PS-f, Cao H, Chen H, Hu T, Chen Y, Zhou X, Wang Z. Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers. International Journal of Environmental Research and Public Health. 2022; 19(9):5245. https://doi.org/10.3390/ijerph19095245
Chicago/Turabian StyleZhang, Kechun, Yuan Fang, Paul Shing-fong Chan, He Cao, Hongbiao Chen, Tian Hu, Yaqi Chen, Xiaofeng Zhou, and Zixin Wang. 2022. "Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers" International Journal of Environmental Research and Public Health 19, no. 9: 5245. https://doi.org/10.3390/ijerph19095245
APA StyleZhang, K., Fang, Y., Chan, P. S.-f., Cao, H., Chen, H., Hu, T., Chen, Y., Zhou, X., & Wang, Z. (2022). Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers. International Journal of Environmental Research and Public Health, 19(9), 5245. https://doi.org/10.3390/ijerph19095245