1. Introduction
Due to the demographic changes observed in terms of a longer life expectancy. several new challenges for health services have emerged [
1,
2].
In 2014, the term “new potential geriatric syndrome” was proposed for the oral health of the elderly. This means that geriatric syndromes (GS) such as frailty, falls, functional limitations, depression, malnutrition, polypharmacy, and cognitive impairment are considered to include oral health that deteriorates with age [
3].
Good oral health is important at any time of life, mainly due to its functions and the possibility of primary inflammatory foci. Primary foci of infection are chronic inflammatory conditions with the potential for harmful effects in distant tissues or organs. In the oral cavity these are mainly: dental caries, residual roots, chronic inflammation of periapical tissues, oral mucosa and periodontitis [
4,
5,
6]. Poor oral hygiene promotes their formation.
In old age, maintaining good oral hygiene can be difficult [
7]. An important factor that contributes to poor hygiene is a disorder of saliva secretion. It is most often a side effect of medications taken or a consequence of therapeutic irradiation [
8,
9]. The change in dietary habits often observed in old age favors the maintenance of the metabolism of dental plaque [
10].
In addition to local factors, general health, aforementioned multimorbidity, multidrug use and possible cognitive impairment increase the risk of poor hygiene and the development of plaque-related conditions [
11].
Regular and professional removal of pathological dental deposits and preventative procedures play an important role in maintaining good oral hygiene and health. For this reason, the independence of older people and easy access to a dentist are important.
In this study, we assumed that the degree of independence of the older people surveyed would have an impact on oral conditions. Taking into account the specificity of the care organization for the elderly in different countries or even regions of a single country, we wanted to learn about the specificity of the tested group, the inhabitants of Malopolska.
The aim was to analyze distribution of remaining dentition in relation to oral hygiene indicators among elderly people remaining in institutionalized care and those who participated in a 3-month rehabilitation program to increase the time of independent functioning in southern Poland.
2. Materials and Methods
The study involved 80 patients, 50 residents of a Municipal Health Centre for Older and Dependent Individuals (MHCOD) and 30 participants of a 3-month rehabilitation program at a Daily Medical Care House (DMCH). During a 3-month course, there were 15 residents of DMCH. MHCOD is an independent public health care institution supervised by the Health Office of the City of Krakow. DMCH is a form of activity of this facility that aims to extend the period of independent living for older people. In the MHCOD group, patients received 24-h care while participants in the 3-month rehabilitation stay lived independently or with their families. The evaluation of the cognitive abilities of the patients who participated in the study was carried out by a psychologist using the MMSE scale (Mini-Mental State Examination). MMSE was assessed in the following categories: normal >25 points, suspected cognitive impairment between 21 and 24 points, and severe cognitive impairment < 20 points. Patients who agreed to participate in the study signed an informed consent. The group examined by the psychologist did not show significant cognitive impairment.
Patients were subjected to a questionnaire and an intraoral clinical examination. The questionnaires included questions about the symptoms reported most frequently by senior patients in clinical practice. Due to the lack of medical knowledge among patients, these were questions about subjective sensations. Based on the symptoms reported, healthcare providers and dentists can perform additional diagnostics to confirm possible conditions. In the questionnaire the participants answered questions about pain in the mouth, bleeding gums, tooth mobility, bad breath, burning mucosa, excess saliva, or dryness, swallowing difficulties, pain in the temporomandibular joint. Questions related to hygiene habits were also asked: self-efficacy in performing hygiene tasks, use of additional oral hygiene utensils, mouthwash and frequency of cleaning teeth and dentures. For each question the respondent could answer yes or no.
The clinical examination was preceded by the investigator calibration and was performed by two dentists in a medical office setting, under headlight, using a dental mirror and a dental probe [
12]. An analysis of missing teeth was performed (FDI, 1970). Plaque Index (PI Silness & Löe 1964) and Gingival Index (GI, Löe & Silness 1963) were measured. Third morlars were excluded from the calculation.
Quantitative characteristics were described by the arithmetic mean, median, minimum, maximum and standard deviation. Qualitative characteristics were described by the number of teeth per group (n) and percentage (%), then tabulated in multivariate tables. Differences in quantitative characteristics between two groups were evaluated using the Student’s t-test, or the Mann-Whitney U test, depending on the distribution of the characteristics. The evaluation of differences and dependencies of qualitative traits was verified by the chi-square test or Fisher’s exact test. Spearman’s order correlation (rs) was used to assess the association of quantitative characteristics (PI and GI). Statistical calculations were performed with the STATISTICA 13 program.
The study was carried out with the approval of the Jagiellonian University Bioethics Committee 1072.6120.187.2017.
4. Discussion
Demographic ageing is a global and growing process, and the quality of ageing is an important factor in this process. As the number of seniors in the general population increases, the proportion of people 65 years and older in Poland reaching 18% in 2019, adequate care for the ageing population is becoming more important [
13].
Seniors face many challenges. These include multimorbidity, exclusion (“ageism”), poverty, loneliness, and dependence on carers for basic life activities [
3,
14,
15,
16]. Senior citizens’ centers address these issues. In Poland, the main sources of assistance for older people are the Municipal Health Centre for Older and Dependent Individuals (MHCOD) and the Daily Medical Care House (DMCH). In many countries, including Poland, there are no established standards of practice for the care of oral health and hygiene among residents of long-term residential care [
17].
Our study included 80 patients. Among them were 50 MHCOD and 30 residents of DMCH. The analysis showed that the main group of people within both MHCOD and DMCH was women, 62% and 70%, respectively. The mean age of women in the MHCOD and DMCH groups was higher than men (78.2 years and 72.9 years for women, 66.5 years and 70.6 years for men, respectively). The results obtained are in line with studies conducted by other authors [
17,
18,
19,
20,
21,
22,
23]. This may be due to the average life expectancy, which in 2030 in Poland is expected to be 84 years for women compared to 77.3 years for men [
13].
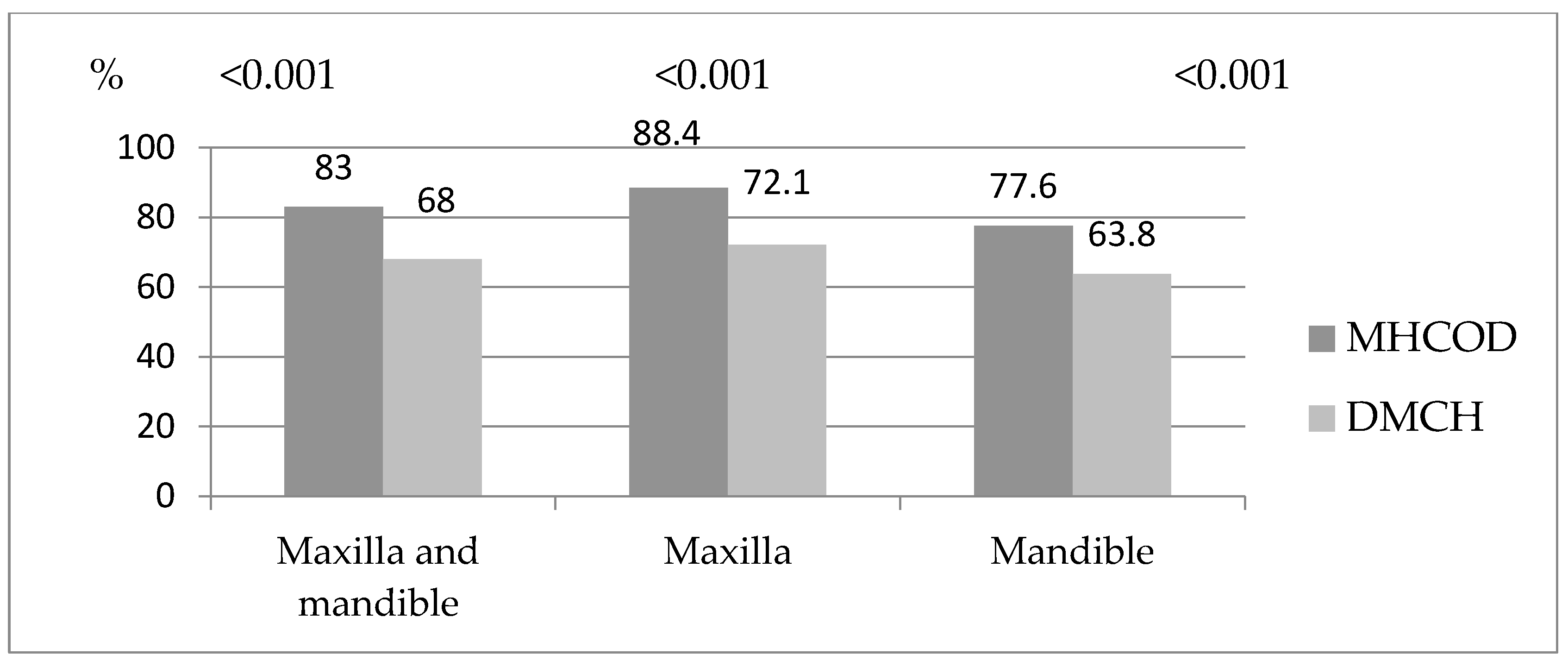
We observed that in the study groups, the most frequent missing teeth were molars followed by premolars. The frequency of missing teeth of each group is higher in MHCOD than in DMCH patients, in both maxilla and mandible. This is probably due to the poorer general health condition and greater dependence of nursing home patients on carers. Such assumptions are consistent with studies by other authors which show that seniors who need assistance with oral hygiene have more decayed teeth, fewer fillings, resulting in multiple missing teeth [
18]. With a high frequency of missing premolars, a lack of occlusal contacts creates a risk of nutritional disorders [
24]. The prevention of malnutrition is crucial for seniors staying in long-term care. Malnutrition leads to reduced ability to perform basic life activities, lower quality of life (QoL), longer hospital stays and rehabilitation, higher risk of falls, more frequent infections, impaired wound healing and higher mortality [
25,
26,
27,
28]. Our study also showed that the number of completely edentulous seniors was higher in MHCOD than in DMCH, 50% and 36.66%, respectively. Publications by other authors that analyze the risk of edentulousness according to sex have shown that older women are at higher risk compared to their male peers [
19]. A study conducted in Poland showed that 47.1% of seniors over 65 years of age are completely edentulous, and more than half are women [
29]. The higher risk of edentulousness among women is most likely due to the risk of periodontitis and a higher propensity for caries. Awareness of and attention to oral hygiene mean that women receive more dental treatment, have fewer residual roots, and use dentures more often [
29,
30].
In our study, we performed a detailed analysis of the distribution of missing teeth. This allowed us to present statistically significant relationships between missing tooth and its location. Molars were missing more frequently in the mandible compared to the other tooth groups. The distribution of the remaining dentition coincides with the outlets of the large salivary glands. Together they are responsible for the secretion of 90% of total saliva [
31]. Saliva components, both organic and inorganic, play an important role in caries prevention [
32]. Elderly patients suffer from hyposalivation as a result of general illness and complex pharmacotherapy [
33]. A study in the Netherlands found that among residents of nursery homes, the incidence of hyposalivation ranges from 24% for resting saliva to 60% for stimulated saliva. Additionally, the volume of saliva secreted was significantly lower in women than in men and in older people than in younger residents [
34]. The negative effect of reduced salivary secretion is enhanced by a decrease in the efficiency of saliva flow and mixing within the oral cavity. It is a consequence of the progressive decrease in muscle tone of the tongue, cheeks, and lips observed with age [
35,
36]. The cumulative effect of these factors may explain our results, which indicated that teeth located near salivary glands’ duct are more likely to remain in the oral cavity.
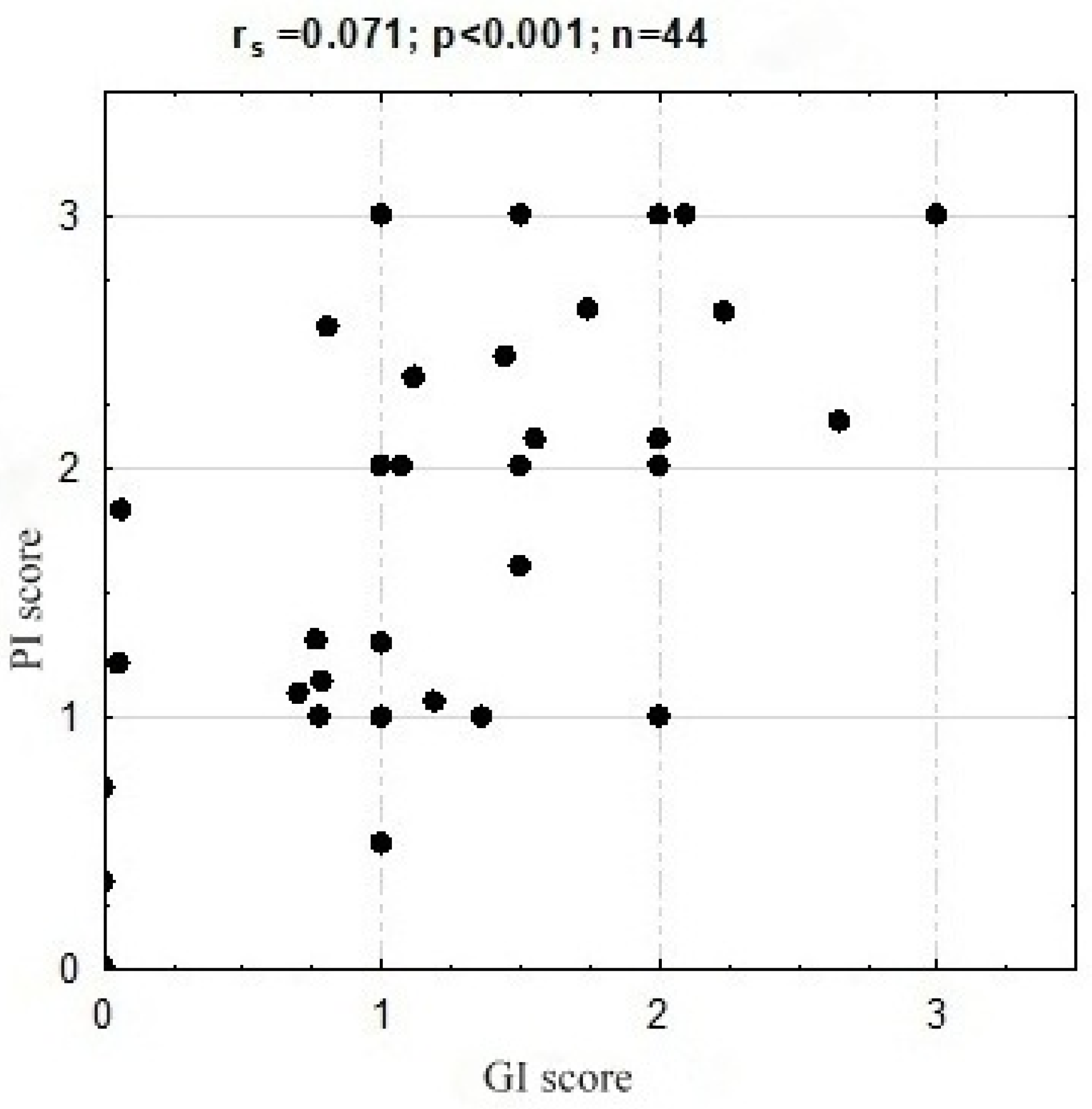
The analysis showed statistically significant relationships with respect to PI and GI. The high correlation between these indicators is the evidence that plaque accumulation and poor oral hygiene are risk factors for gingivitis and periodontitis also among seniors. This relationship was confirmed by many other studies [
37,
38]. Furthermore, we showed a correlation between PI and dry mouth. More than half of the residents who complained of dry mouth had the highest PI (53.8%,
p = 0.047). This relationship was confirmed in studies involving ‘younger adults’, indicating that xerostomia is an indirect risk factor for gingival inflammation due to increased plaque accumulation [
39].
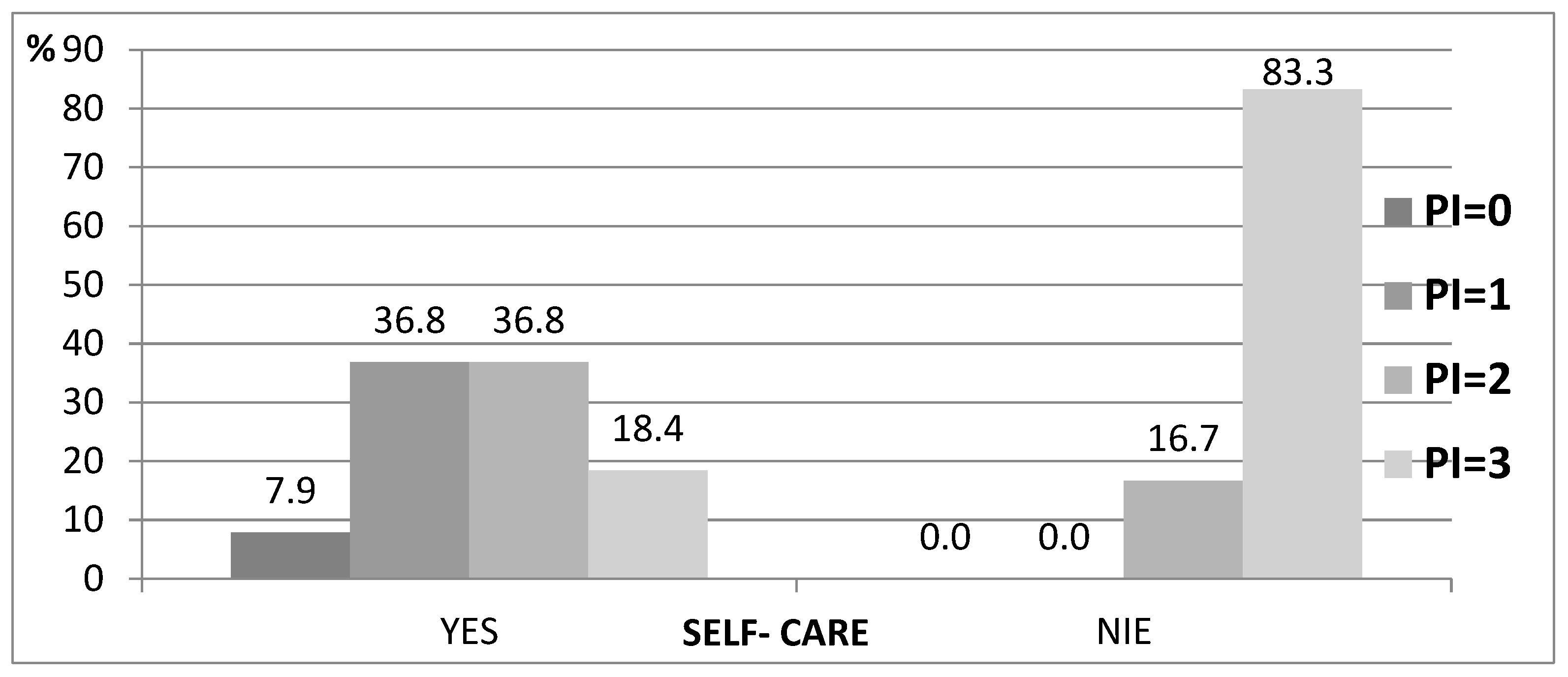
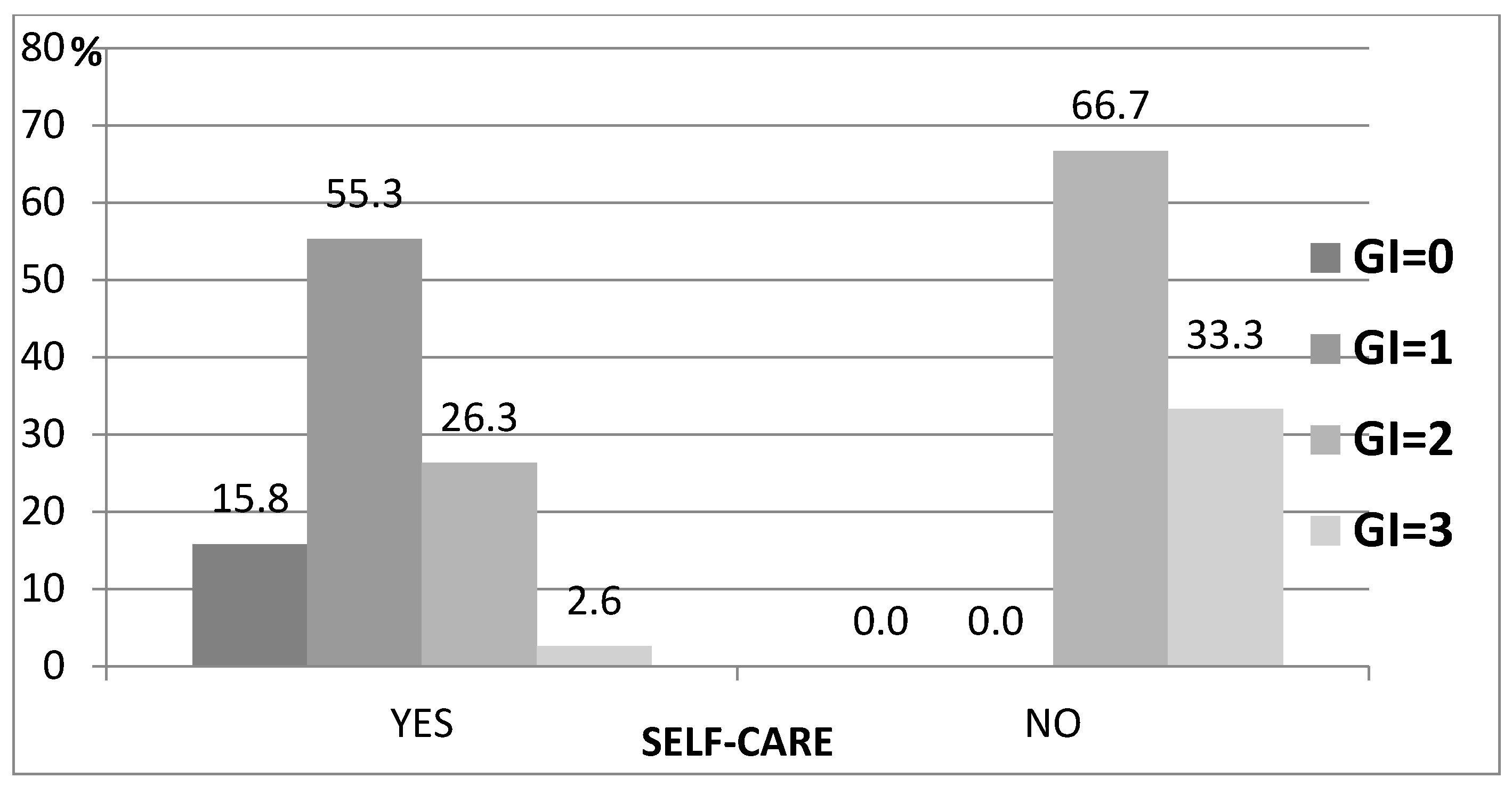
Our research has shown that among patients who depend on the help of caregivers, oral hygiene is neglected. PI and GI scores, among the analyzed groups, showed greater plaque accumulation and risk of gingival inflammation. This may suggest a lack of training for those caring for seniors in MHCOD and DMCH or caring for them at home. Furthermore, many caregivers, including nursing staff, do not have adequate knowledge of the role of plaque and diet in the etiology of dental caries [
40]. This problem is raised in many studies, mentioning the need to implement educational programs and standardize procedures [
3,
18,
19,
41,
42,
43]. The assessment of the ability and frequency of patients to perform hygiene procedures revealed that residents of DMCH reported significantly more frequent teeth cleaning, and this relationship was statistically significant (
p = 0.033). This result may be related to the complexity of dental deficiencies, which more often affected residents of nursery houses. Research in this field has been carried out in Korea and has shown that oral hygiene performance is related to the degree of dependence of patients and the presence of teeth and is not affected by cognitive decline due to dementia [
17].
It should be noted that the results presented in our study come from a centre with residents from the southern part of Poland. Therefore, they reflect the specificity of the region. Furthermore, the analysis was carried out in a group of only 80 people. The small number of DMHC patients is due to the fact that for a 3-month course, there were only 15 participants. In addition, older people who participated in the study had to sign an informed consent. The patients selected for the study were qualified on the basis of the MMSE score and the lack of a cognitively impaired control group is a limitation of the study. A comparison of our results with results from future studies conducted in other parts of Poland will provide more sufficient conclusions.
5. Conclusions
DMCH patients brush their teeth and clean their dentures more often.
There is a higher prevalence of missing teeth among residents of MHCOD compared to DMCH. The distribution of the remaining teeth, in both groups, corresponds to the outlets of the large salivary glands.
Residents with dry mouth are more likely to have plaque deposits and gingival inflammation.
An assessment of missing teeth, interview and psychical examinations for xerostomia should be an important element of geriatric examinations.
Further studies conducted in institutionalized long-term care facilities for older people should be based on a group of residents with salivary disorders. It will enable the development of standardized procedures, appropriate support programs, and prophylaxis for residents in long-term care facility.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}