
Exercise Dose Equalization in High-Intensity Interval Training: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
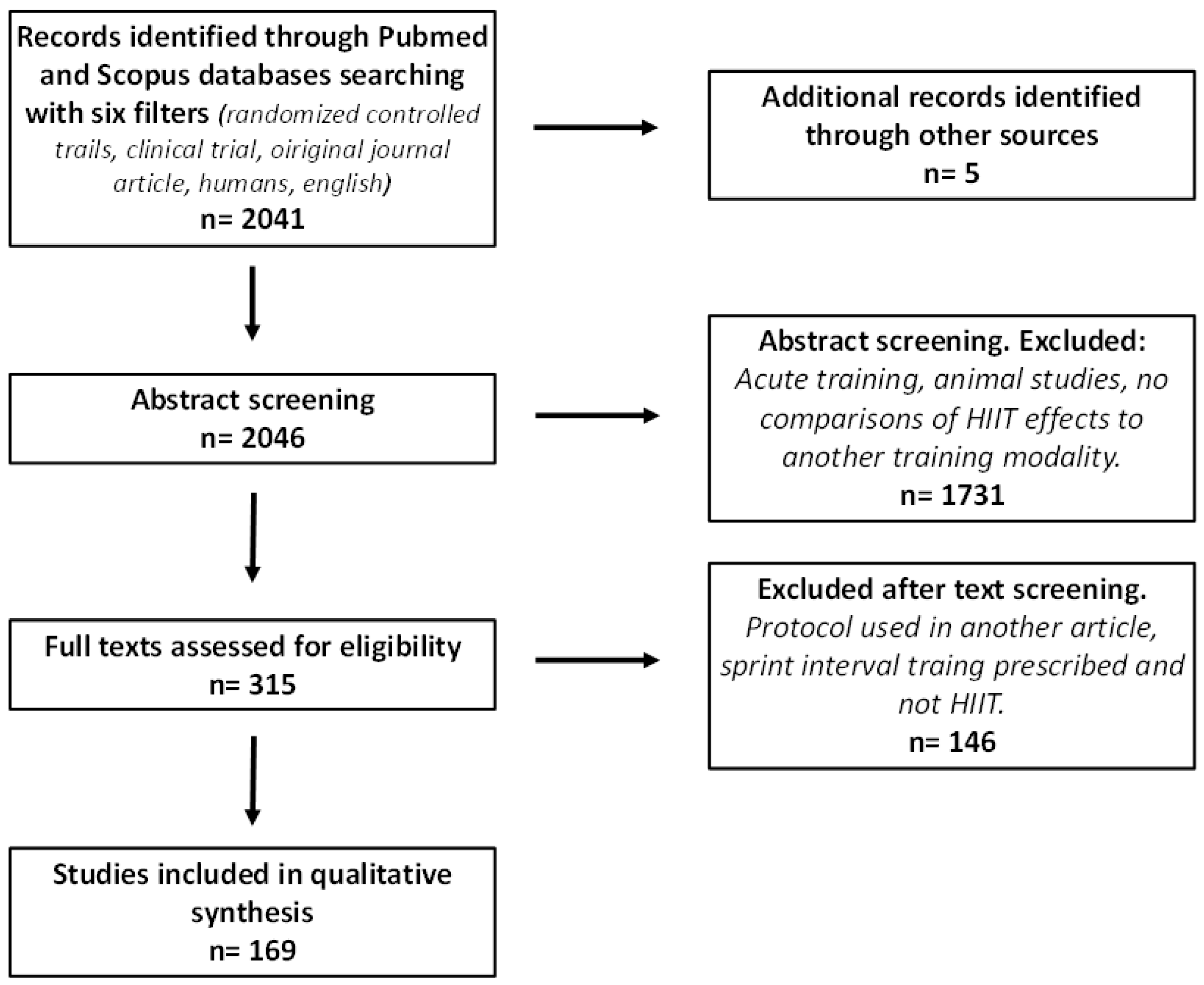
2.1. Search Strategy
2.2. Assessment of Reporting Quality
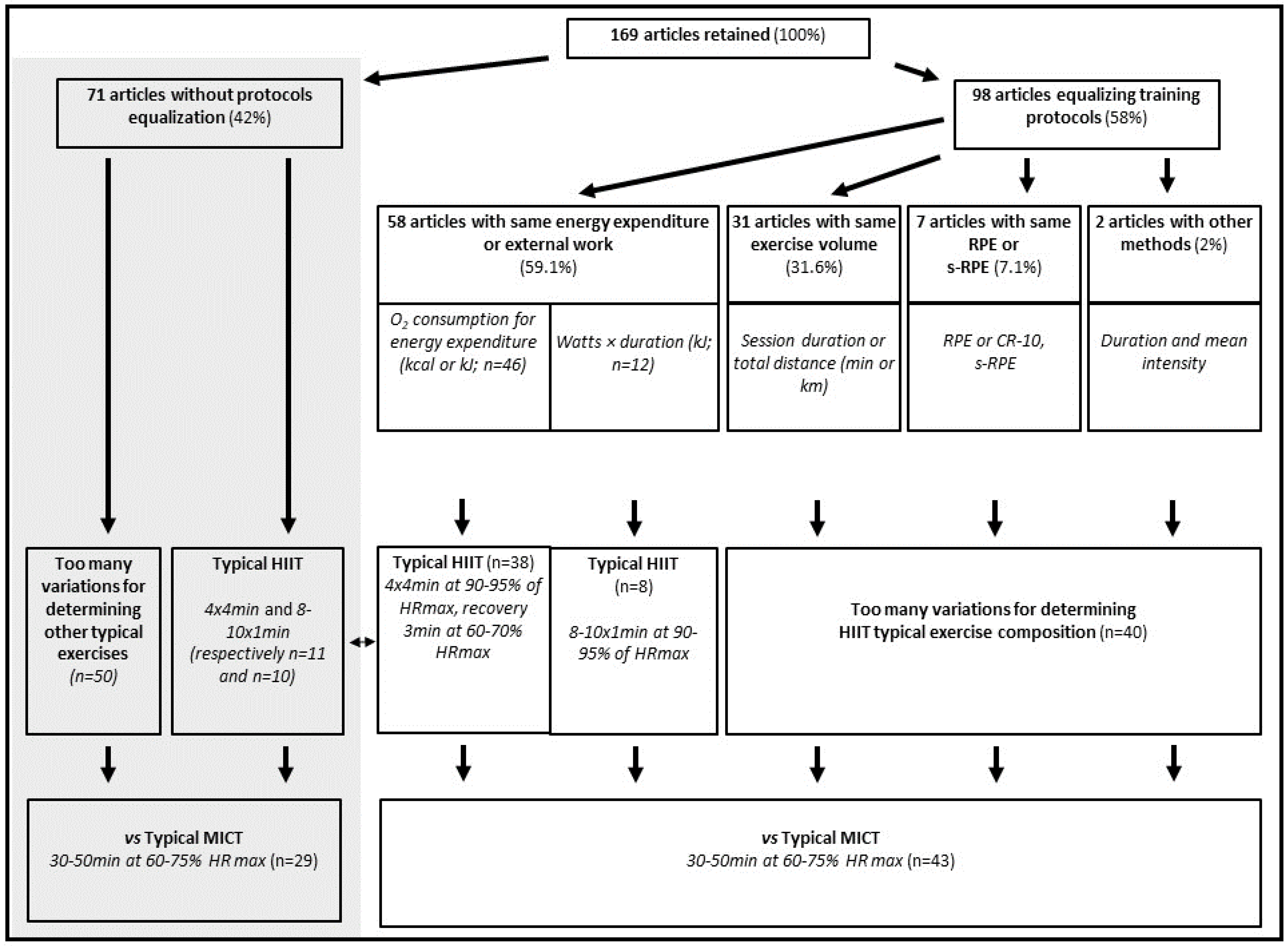
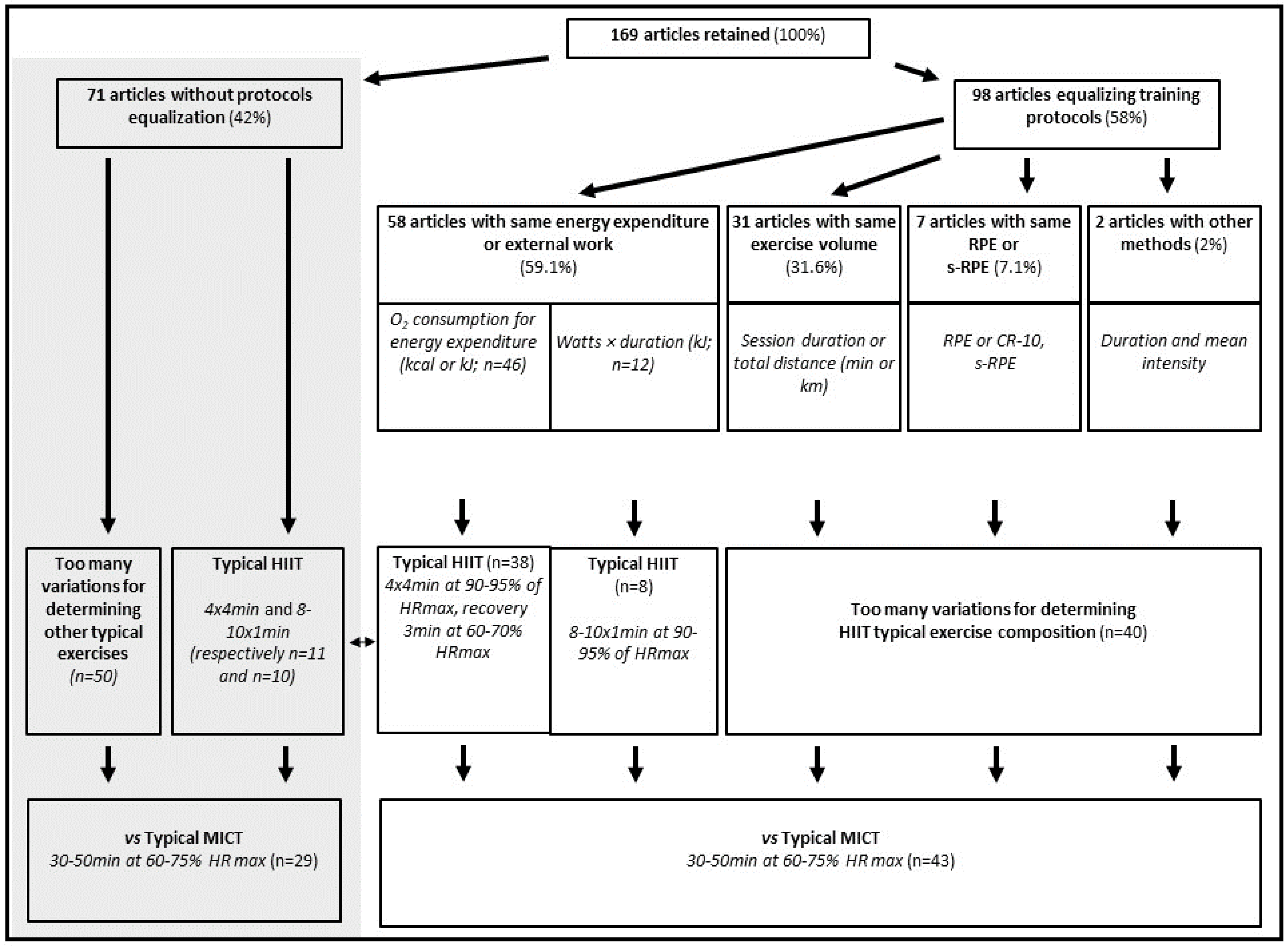
2.3. Terms Used and Methods Applied for Protocols Equalization
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wasfy, M.M.; Baggish, A.L. Exercise Dose in Clinical Practice. Circulation 2016, 133, 2297–2313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staunton, C.A.; Abt, G.; Weaving, D.; Wundersitz, D.W.T. Misuse of the Term “load” in Sport and Exercise Science. J. Sci. Med. Sport 2021, S1440-2440(21)00212-7. [Google Scholar] [CrossRef] [PubMed]
- Taha, T.; Thomas, S.G. Systems Modelling of the Relationship between Training and Performance. Sports Med. 2003, 33, 1061–1073. [Google Scholar] [CrossRef] [PubMed]
- Desgorces, F.-D.; Hourcade, J.-C.; Dubois, R.; Toussaint, J.-F.; Noirez, P. Training Load Quantification of High Intensity Exercises: Discrepancies between Original and Alternative Methods. PLoS ONE 2020, 15, e0237027. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Rodriguez-Marroyo, J.A.; de Koning, J.J. Monitoring Training Loads: The Past, the Present, and the Future. Int. J. Sports Physiol. Perform. 2017, 12, S22–S28. [Google Scholar] [CrossRef] [Green Version]
- Lambert, M.I.; Borresen, J. Measuring Training Load in Sports. Int. J. Sports Physiol. Perform. 2010, 5, 406–411. [Google Scholar] [CrossRef]
- Gronwald, T.; Törpel, A.; Herold, F.; Budde, H. Perspective of Dose and Response for Individualized Physical Exercise and Training Prescription. J. Funct. Morphol. Kinesiol. 2020, 5, E48. [Google Scholar] [CrossRef]
- Steele, J. What Is (Perception of) Effort? Objective and Subjective Effort during Attempted Task Performance. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Burd, N.A.; Mitchell, C.J.; Churchward-Venne, T.A.; Phillips, S.M. Bigger Weights May Not Beget Bigger Muscles: Evidence from Acute Muscle Protein Synthetic Responses after Resistance Exercise. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2012, 37, 551–554. [Google Scholar] [CrossRef]
- Montero, D.; Lundby, C. Refuting the Myth of Non-Response to Exercise Training: “non-Responders” Do Respond to Higher Dose of Training. J. Physiol. 2017, 595, 3377–3387. [Google Scholar] [CrossRef]
- Viana, R.B.; de Lira, C.A.B.; Naves, J.P.A.; Coswig, V.S.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Vieira, C.A.; Gentil, P. Can We Draw General Conclusions from Interval Training Studies? Sports Med. 2018, 48, 2001–2009. [Google Scholar] [CrossRef]
- Andreato, L.V. High-Intensity Interval Training: Methodological Considerations for Interpreting Results and Conducting Research. Trends Endocrinol. Metab. TEM 2020, 31, 812–817. [Google Scholar] [CrossRef]
- Vollaard, N.B.J.; Metcalfe, R.S. Those Apples Don’t Taste Like Oranges! Why “Equalising” HIIT and MICT Protocols Does Not Make Sense. Trends Endocrinol. Metab. TEM 2021, 32, 131–132. [Google Scholar] [CrossRef]
- Hansen, D.; Abreu, A.; Ambrosetti, M.; Cornelissen, V.; Gevaert, A.; Kemps, H.; Laukkanen, J.A.; Pedretti, R.; Simonenko, M.; Wilhelm, M.; et al. Exercise Intensity Assessment and Prescription in Cardiovascular Rehabilitation and beyond: Why and How: A Position Statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 230–245. [Google Scholar] [CrossRef]
- Yan, Z.-W.; Li, W.-G. Battle between High-Intensity Interval Training and Moderate-Intensity Continuous Training in Cardiac Rehabilitation Practice. Eur. J. Prev. Cardiol. 2022, 96, 1533–1544. [Google Scholar] [CrossRef]
- Passfield, L.; Murias, J.M.; Sacchetti, M.; Nicolò, A. Validity of the Training-Load Concept. Int. J. Sports Physiol. Perform. 2022, 17, 507–514. [Google Scholar] [CrossRef]
- MacInnis, M.J.; Gibala, M.J. Physiological Adaptations to Interval Training and the Role of Exercise Intensity. J. Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef] [Green Version]
- Atakan, M.M.; Li, Y.; Koşar, Ş.N.; Turnagöl, H.H.; Yan, X. Evidence-Based Effects of High-Intensity Interval Training on Exercise Capacity and Health: A Review with Historical Perspective. Int. J. Environ. Res. Public. Health 2021, 18, 7201. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for Conducting Systematic Scoping Reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Colquhoun, H.; Garritty, C.M.; Hempel, S.; Horsley, T.; Langlois, E.V.; Lillie, E.; O’Brien, K.K.; Tunçalp, Ö.; et al. Scoping Reviews: Reinforcing and Advancing the Methodology and Application. Syst. Rev. 2021, 10, 263. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helgerud, J.; Høydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjerkaas, M.; Simonsen, T.; Helgesen, C.; Hjorth, N.; Bach, R.; et al. Aerobic High-Intensity Intervals Improve VO2max More than Moderate Training. Med. Sci. Sports Exerc. 2007, 39, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Lanzi, S.; Codecasa, F.; Cornacchia, M.; Maestrini, S.; Capodaglio, P.; Brunani, A.; Fanari, P.; Salvadori, A.; Malatesta, D. Short-Term HIIT and Fat Max Training Increase Aerobic and Metabolic Fitness in Men with Class II and III Obesity. Obesity 2015, 23, 1987–1994. [Google Scholar] [CrossRef]
- Billat, L.V. Interval Training for Performance: A Scientific and Empirical Practice. Special Recommendations for Middle- and Long-Distance Running. Part I: Aerobic Interval Training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- LaForgia, J.; Withers, R.T.; Gore, C.J. Effects of Exercise Intensity and Duration on the Excess Post-Exercise Oxygen Consumption. J. Sports Sci. 2006, 24, 1247–1264. [Google Scholar] [CrossRef]
- Desgorces, F.D.; Berthelot, G.; Dietrich, G.; Testa, M.S.A. Local Muscular Endurance and Prediction of 1 Repetition Maximum for Bench in 4 Athletic Populations. J. Strength Cond. Res. 2010, 24, 394–400. [Google Scholar] [CrossRef]
- Monod, H.; Scherrer, J. Capacity for static work in a synergistic muscular group in man. Comptes Rendus Seances Soc. Biol. Fil. 1957, 151, 1358–1362. [Google Scholar]
- Péronnet, F.; Thibault, G. Mathematical Analysis of Running Performance and World Running Records. J. Appl. Physiol. 1989, 67, 453–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billat, L.V.; Koralsztein, J.P.; Morton, R.H. Time in Human Endurance Models. From Empirical Models to Physiological Models. Sports Med. 1999, 27, 359–379. [Google Scholar] [CrossRef] [PubMed]
- Seiler, S.; Jøranson, K.; Olesen, B.V.; Hetlelid, K.J. Adaptations to Aerobic Interval Training: Interactive Effects of Exercise Intensity and Total Work Duration. Scand. J. Med. Sci. Sports 2013, 23, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Klonizakis, M.; Moss, J.; Gilbert, S.; Broom, D.; Foster, J.; Tew, G.A. Low-Volume High-Intensity Interval Training Rapidly Improves Cardiopulmonary Function in Postmenopausal Women. Menopause 2014, 21, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, E.M.; Loukov, D.; Bowdish, D.M.E.; Heisz, J.J. Exercise Reduces Depression and Inflammation but Intensity Matters. Biol. Psychol. 2018, 133, 79–84. [Google Scholar] [CrossRef]
- Sandbakk, Ø.; Sandbakk, S.B.; Ettema, G.; Welde, B. Effects of Intensity and Duration in Aerobic High-Intensity Interval Training in Highly Trained Junior Cross-Country Skiers. J. Strength Cond. Res. 2013, 27, 1974–1980. [Google Scholar] [CrossRef] [Green Version]
- Soh, S.-H.; Joo, M.C.; Yun, N.R.; Kim, M.-S. Randomized Controlled Trial of the Lateral Push-Off Skater Exercise for High-Intensity Interval Training vs. Conventional Treadmill Training. Arch. Phys. Med. Rehabil. 2020, 101, 187–195. [Google Scholar] [CrossRef]
- Álvarez, C.; Ramírez-Campillo, R.; Ramírez-Vélez, R.; Izquierdo, M. Effects and Prevalence of Nonresponders after 12 Weeks of High-Intensity Interval or Resistance Training in Women with Insulin Resistance: A Randomized Trial. J. Appl. Physiol. 2017, 122, 985–996. [Google Scholar] [CrossRef]
- Wens, I.; Dalgas, U.; Vandenabeele, F.; Grevendonk, L.; Verboven, K.; Hansen, D.; Eijnde, B.O. High Intensity Exercise in Multiple Sclerosis: Effects on Muscle Contractile Characteristics and Exercise Capacity, a Randomised Controlled Trial. PloS ONE 2015, 10, e0133697. [Google Scholar] [CrossRef]
- Eston, R. Use of Ratings of Perceived Exertion in Sports. Int. J. Sports Physiol. Perform. 2012, 7, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Joseph, T.; Johnson, B.; Battista, R.A.; Wright, G.; Dodge, C.; Porcari, J.P.; de Koning, J.J.; Foster, C. Perception of Fatigue during Simulated Competition. Med. Sci. Sports Exerc. 2008, 40, 381–386. [Google Scholar] [CrossRef]
- Noakes, T.D. Linear Relationship between the Perception of Effort and the Duration of Constant Load Exercise That Remains. J. Appl. Physiol. 2004, 96, 1571–1573. [Google Scholar] [CrossRef] [PubMed]
- Barroso, R.; Salgueiro, D.F.; do Carmo, E.C.; Nakamura, F.Y. The Effects of Training Volume and Repetition Distance on Session Rating of Perceived Exertion and Internal Load in Swimmers. Int. J. Sports Physiol. Perform. 2015, 10, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Hourcade, J.-C.; Noirez, P.; Sidney, M.; Toussaint, J.-F.; Desgorces, F.D. Effects of Intensity Distribution Changes on Performance and on Training Loads Quantification. Biol. Sport 2018, 35, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Seiler, S.; Hetlelid, K.J. The Impact of Rest Duration on Work Intensity and RPE during Interval Training. Med. Sci. Sports Exerc. 2005, 37, 1601–1607. [Google Scholar] [CrossRef] [Green Version]
- Agostinho, M.F.; Philippe, A.G.; Marcolino, G.S.; Pereira, E.R.; Busso, T.; Candau, R.B.; Franchini, E. Perceived Training Intensity and Performance Changes Quantification in Judo. J. Strength Cond. Res. 2015, 29, 1570–1577. [Google Scholar] [CrossRef]
- Cavar, M.; Marsic, T.; Corluka, M.; Culjak, Z.; Cerkez Zovko, I.; Müller, A.; Tschakert, G.; Hofmann, P. Effects of 6 Weeks of Different High-Intensity Interval and Moderate Continuous Training on Aerobic and Anaerobic Performance. J. Strength Cond. Res. 2019, 33, 44–56. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total Score | Recruitment in Same Population (%) | Subjects Ramdomization (%) | Physical Condition Matching (%) | Training Direct Supervision (%) | Exercise Control (%) | Adherence to Training (%) | Subjects Follow-Up (%) | Statistical Power (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 169) | 5.1 ± 1.5 | 47.6 | 70.8 | 53.0 | 73.8 | 88.7 | 61.3 | 84.5 | 29.8 |
| Equalized protocols (n = 98) | 5.2 ± 1.5 | 46.4 | 71.1 | 51.5 | 75.3 | 91.7 | 61.9 | 89.7 | 28.9 |
| Non-equalized protocols (n = 71) | 5.0 ± 1.6 | 49.3 | 70.4 | 54.9 | 71.8 | 84.5 | 60.5 | 77.4 | 31.0 |
| Older people and patients (n = 99) | 5.1 ± 1.7 | 50.5 | 67.0 | 44.4 | 76.7 | 85.8 | 62.6 | 85.8 | 29.3 |
| Untrained (n = 41) | 5.3 ± 1.3 | 52.5 | 85.0 | 47.5 | 75.0 | 92.5 | 57.5 | 87.5 | 32.5 |
| Trained (n = 29) | 5.0 ± 1.2 | 34.5 | 62.1 | 89.6 * | 62.1 | 93.1 | 62.1 | 75.9 | 24.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Normand-Gravier, T.; Britto, F.; Launay, T.; Renfree, A.; Toussaint, J.-F.; Desgorces, F.-D. Exercise Dose Equalization in High-Intensity Interval Training: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 4980. https://doi.org/10.3390/ijerph19094980
Normand-Gravier T, Britto F, Launay T, Renfree A, Toussaint J-F, Desgorces F-D. Exercise Dose Equalization in High-Intensity Interval Training: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(9):4980. https://doi.org/10.3390/ijerph19094980
Chicago/Turabian StyleNormand-Gravier, Tom, Florian Britto, Thierry Launay, Andrew Renfree, Jean-François Toussaint, and François-Denis Desgorces. 2022. "Exercise Dose Equalization in High-Intensity Interval Training: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 9: 4980. https://doi.org/10.3390/ijerph19094980
APA StyleNormand-Gravier, T., Britto, F., Launay, T., Renfree, A., Toussaint, J.-F., & Desgorces, F.-D. (2022). Exercise Dose Equalization in High-Intensity Interval Training: A Scoping Review. International Journal of Environmental Research and Public Health, 19(9), 4980. https://doi.org/10.3390/ijerph19094980