
Risk of Burnout among Emergency Department Staff as a Result of Violence and Aggression from Patients and Their Relatives


 ,
,
Abstract
:1. Introduction
1.1. Experience of Violence/Aggression and Risk of Burnout and Perceived High Stress
1.2. Prevention Measures and Risk of Burnout and Perceived Stress
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.2.1. Workplace Violence
2.2.2. Burnout
2.2.3. Resilience
2.2.4. Preparation by the Workplace and Perceived Stress
2.3. Statistical Analyses
Ethical Considerations
3. Results
3.1. Descriptive Statistics
3.1.1. Resilience
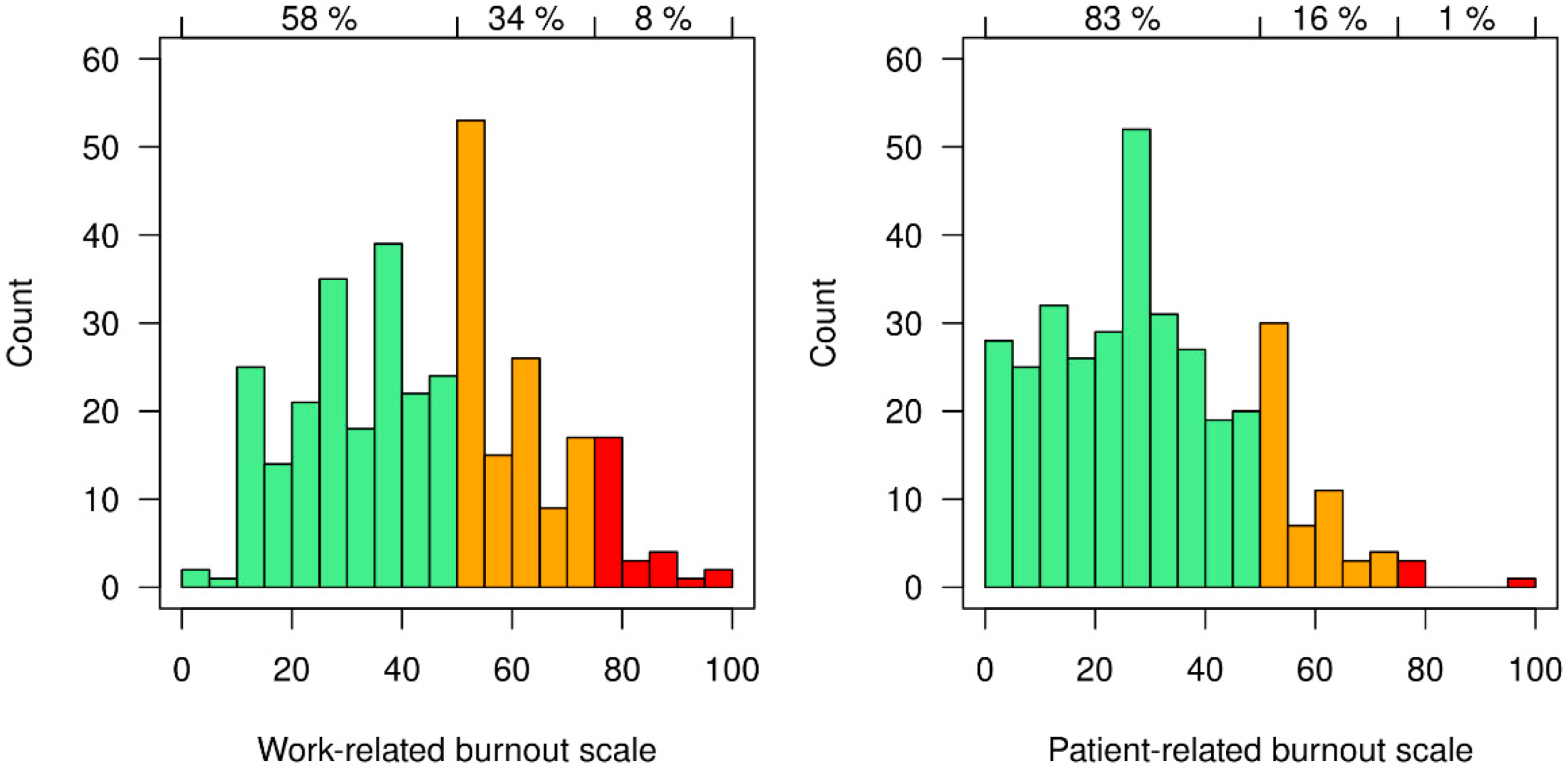
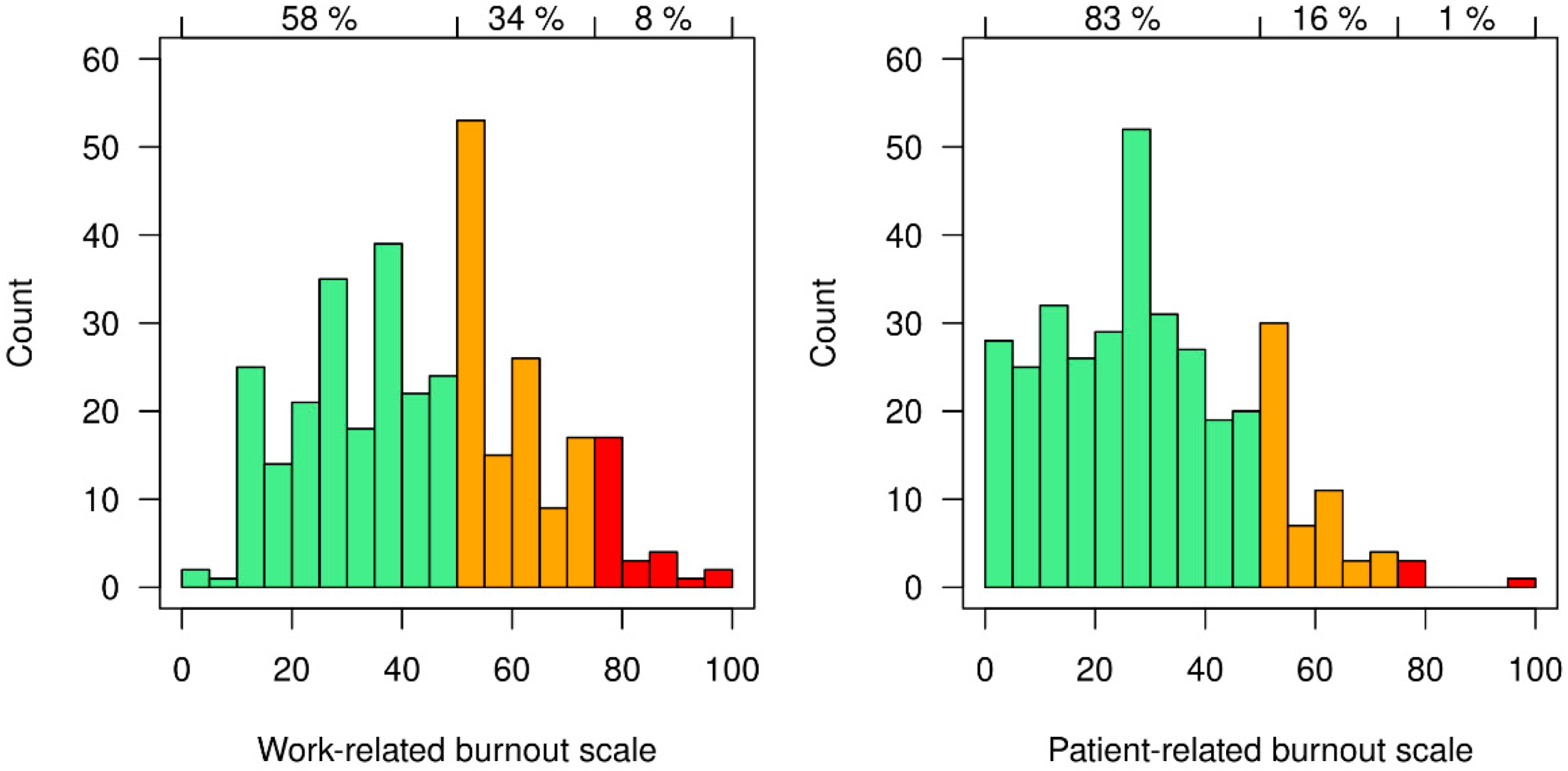
3.1.2. Burnout and Perceived Stress
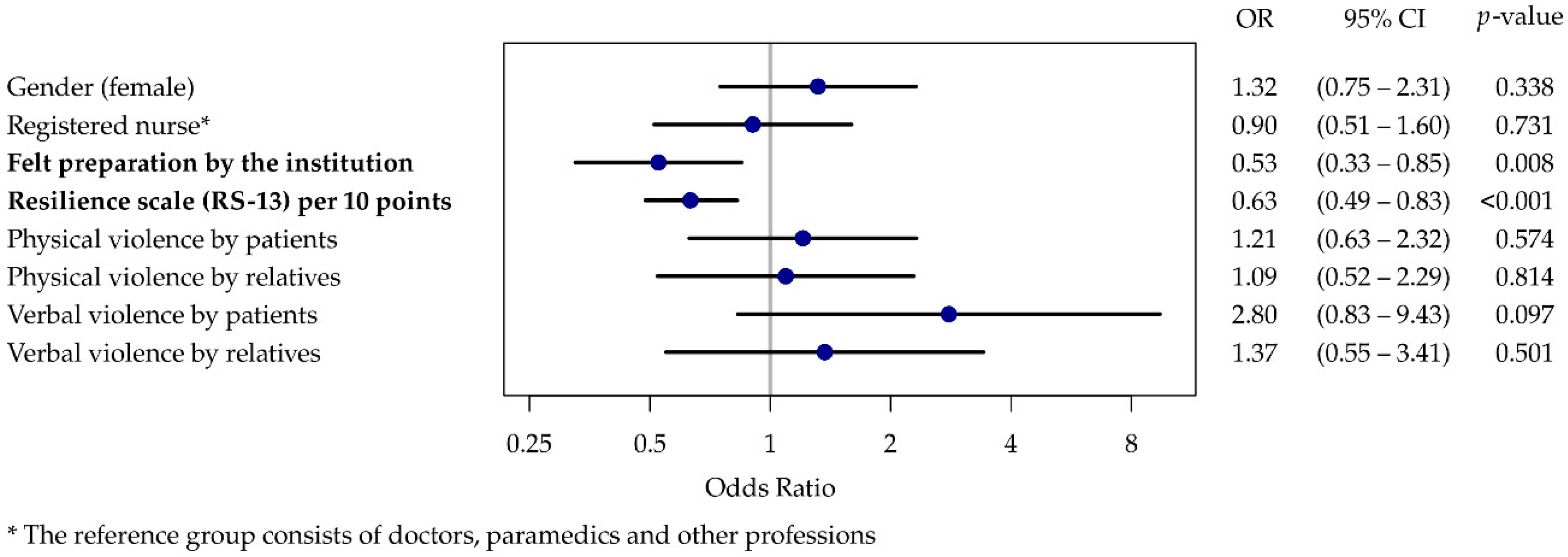
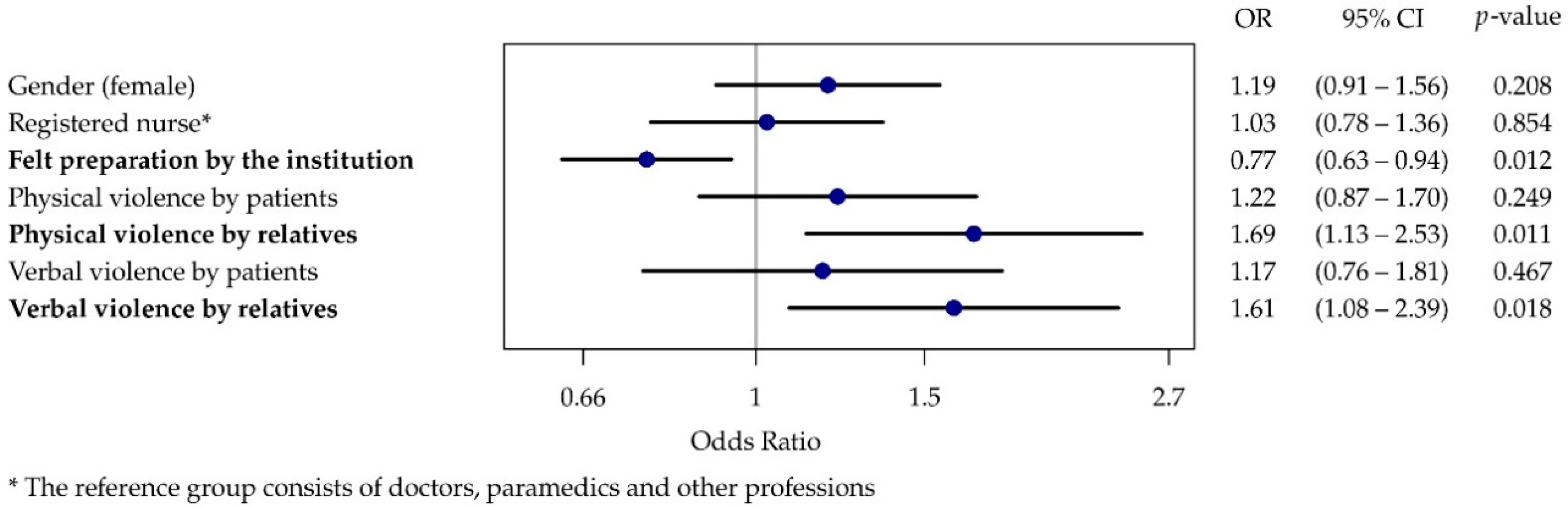
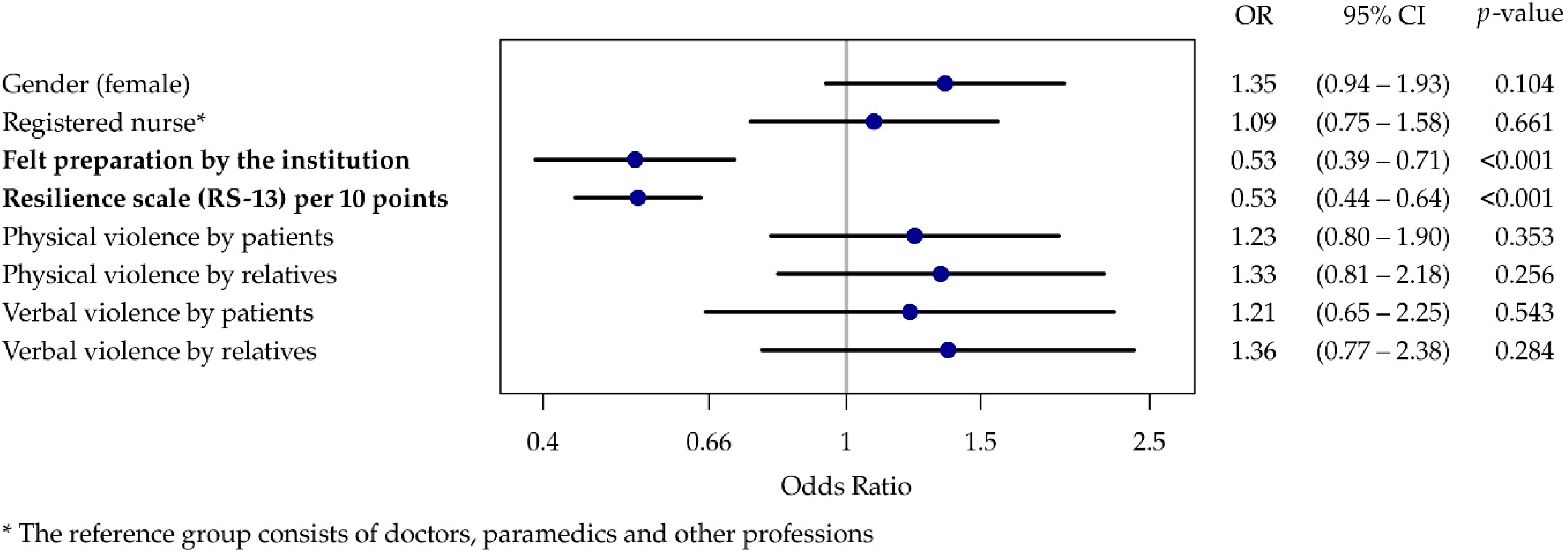
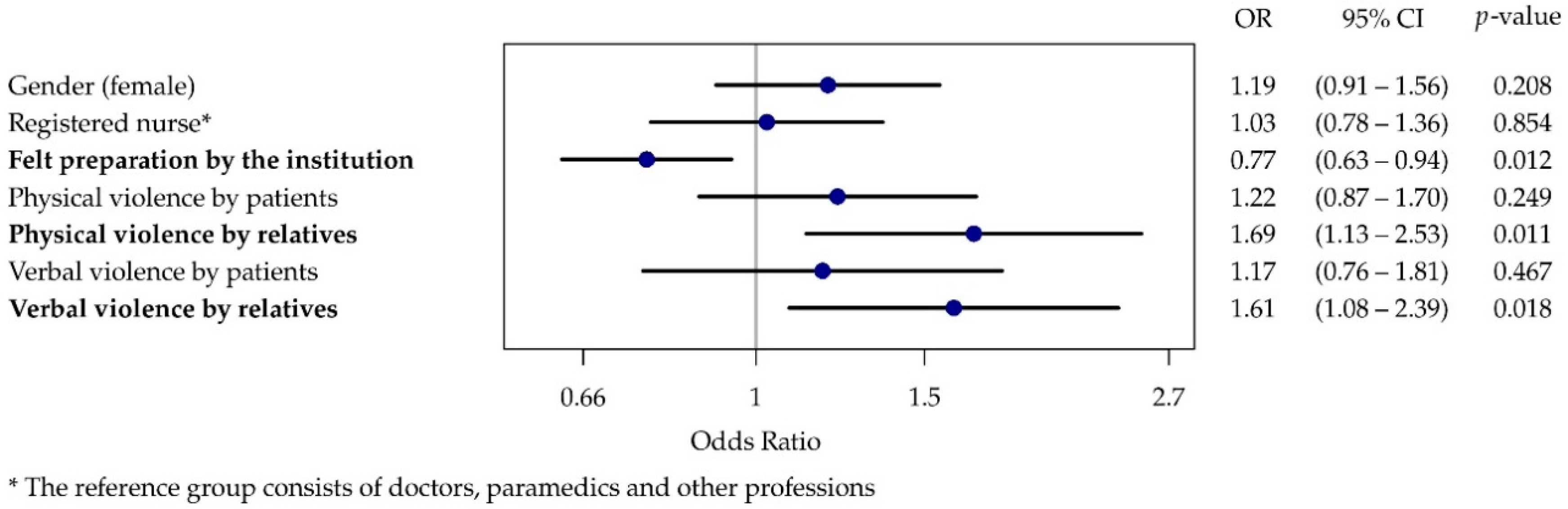
3.2. Regression Analyses
4. Discussion
4.1. Limitations and Future Directions
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schablon, A.; Wendeler, D.; Kozak, A.; Nienhaus, A.; Steinke, S. Prevalence and Consequences of Aggression and Violence towards Nursing and Care Staff in Germany-A Survey. Int. J. Environ. Res. Public Health 2018, 15, 1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeh, A.; Schablon, A.; Wohlert, C.; Richter, D.; Nienhaus, A. Violence and aggression in care-related jobs—A literature overview. Gesundheitswes 2009, 71, 449–459. [Google Scholar] [CrossRef]
- Li, Y.L.; Li, R.Q.; Qiu, D.; Xiao, S.Y. Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 299. [Google Scholar] [CrossRef] [Green Version]
- International Labour Office (ILO). Code of practice on workplace violence in services sectors and measures to combat this phenomenon. In Proceedings of the Meeting of Experts to Develop a Code of Practice on Violence and Stress at Work in Services: A Threat to Productivity and Decent Work, Geneva, Switzerland, 8–15 October 2003; Available online: https://www.ilo.org/wcmsp5/groups/public/ed_protect/protrav/safework/documents/normativeinstrument/wcms_107705.pdf (accessed on 9 March 2022).
- Estryn-Behar, M.; van der Heijden, B.; Camerino, D.; Fry, C.; Le Nezet, O.; Conway, P.M.; Hasselhorn, H.M. Violence risks in nursing—Results from the European ‘NEXT’ Study. Occup. Med. 2008, 58, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Gan, Y.; Jiang, H.; Li, L.; Dwyer, R.; Lu, K.; Yan, S.; Sampson, O.; Xu, H.; Wang, C.; et al. Prevalence of workplace violence against healthcare workers: A systematic review and meta-analysis. Occup. Environ. Med. 2019, 76, 927–937. [Google Scholar] [CrossRef] [Green Version]
- Ohlbrecht, H.; Bartel, S.; von Kardoff, E.; Streibelt, M. Gewalt in der Notaufnahme. Ein aktuelles Problem und seine Hintergründe. Prävent. und Gesundh. 2009, 4, 7–14. [Google Scholar] [CrossRef]
- Nikathil, S.; Olaussen, A.; Gocentas, R.A.; Symons, E.; Mitra, B. Review article: Workplace violence in the emergency department: A systematic review and meta analysis. Emerg. Med. Australas. 2017, 29, 265–275. [Google Scholar] [CrossRef]
- Aljohani, B.; Burkholder, J.; Tran, Q.K.; Chen, C.; Beisenova, K.; Pourmand, A. Workplace violence in the emergency department: A systematic review and meta-analysis. Public Health 2021, 196, 186–197. [Google Scholar] [CrossRef]
- Verboket, R.; Sohling, N.; Schmitz, L.; Lustenberger, T.; Nau, C.; Marzi, I. Violence in the emergency department of a maximum care hospital. Chirurg 2019, 90, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Schuffenhauer, H.; Hettmannsperger-Lippol, R. Violence against nurses in emergency departments. An explorative analysis of stress, coping strategies and personality. ASU Arbeitsmed. Sozialmed. Umweltmed. 2022, 57, 98–105. [Google Scholar] [CrossRef]
- Murray, R.M.; Davis, A.L.; Shepler, L.J.; Moore-Merrell, L.; Troup, W.J.; Allen, J.A.; Taylor, J.A. A Systematic Review of Workplace Violence against Emergency Medical Services Responders. New Solut. 2020, 29, 487–503. [Google Scholar] [CrossRef]
- Pourshaikhian, M.; Abolghasem Gorji, H.; Aryankhesal, A.; Khorasani-Zavareh, D.; Barati, A. A Systematic Literature Review: Workplace Violence against Emergency Medical Services Personnel. Arch. Trauma Res. 2016, 5, e28734. [Google Scholar] [CrossRef]
- Ramacciati, N.; Ceccagnoli, A.; Addey, B.; Rasero, L. Violence towards Emergency Nurses. The Italian National Survey 2016: A qualitative study. Int. J. Nurs. Stud. 2018, 81, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Vrablik, M.M.; Chipman, A.K.; Rosenman, E.D.; Simcox, N.J.; Huynh, L.; Moore, M.; Fernandez, R. Identification of processes that mediate the impact of workplace violence on emergency department healthcare workers in the USA: Results from a qualitative study. BMJ Open 2019, 9, e031781. [Google Scholar] [CrossRef]
- D’Ettorre, G.; Pellicani, V.; Mazzotta, M.; Vullo, A. Preventing and managing workplace violence against healthcare workers in Emergency Departments. Acta Biomed. 2018, 89, 28–36. [Google Scholar] [CrossRef]
- Hofmann, T.; Hachenberg, T. Violence in the Emergency Medicine (Emergency Rescue Service and Emergency Departments) - Current Situation in Germany. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 2019, 54, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Kaeser, D.; Guerra, R.; Keidar, O.; Lanz, U.; Moses, M.; Kobel, C.; Exadaktylos, A.K.; Ricklin, M.E. Verbal and Non-Verbal Aggression in a Swiss University Emergency Room: A Descriptive Study. Int. J. Environ. Res. Public Health 2018, 15, 1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmins, F.; Catania, G.; Zanini, M.; Ottonello, G.; Napolitano, F.; Musio, M.E.; Aleo, G.; Sasso, L.; Bagnasco, A. Nursing management of emergency department violence-Can we do more? J. Clin. Nurs. 2022, 1–8. [Google Scholar] [CrossRef]
- Liu, W.; Zhao, S.; Shi, L.; Zhang, Z.; Liu, X.; Li, L.; Duan, X.; Li, G.; Lou, F.; Jia, X.; et al. Workplace violence, job satisfaction, burnout, perceived organisational support and their effects on turnover intention among Chinese nurses in tertiary hospitals: A cross-sectional study. BMJ Open 2018, 8, e019525. [Google Scholar] [CrossRef]
- Rasool, S.F.; Wang, M.; Zhang, Y.; Samma, M. Sustainable Work Performance: The Roles of Workplace Violence and Occupational Stress. Int. J. Environ. Res. Public Health 2020, 17, 912. [Google Scholar] [CrossRef] [Green Version]
- Copeland, D.; Henry, M. The relationship between workplace violence, perceptions of safety, and Professional Quality of Life among emergency department staff members in a Level 1 Trauma Centre. Int. Emerg. Nurs. 2018, 39, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.; Wirihana, L.; Eley, R.; Ossieran-Moisson, R.; Hegney, D. The Effects of Occupational Violence on the Well-being and Resilience of Nurses. J. Nurs. Admin. 2018, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Vincent-Höper, S.; Stein, M.; Nienhaus, A.; Schablon, A. Workplace Aggression and Burnout in Nursing-The Moderating Role of Follow-Up Counseling. Int. J. Environ. Res. Public Health 2020, 17, 3152. [Google Scholar] [CrossRef]
- Pina, D.; Llor-Zaragoza, P.; Lopez-Lopez, R.; Ruiz-Hernandez, J.A.; Puente-Lopez, E.; Galian-Munoz, I.; Martinez-Jarreta, B. Assessment of Non-physical User Violence and Burnout in Primary Health Care Professionals. The Modulating Role of Job Satisfaction. Front. Public Health 2022, 10, 777412. [Google Scholar] [CrossRef]
- Crowe, R.P.; Bower, J.K.; Cash, R.E.; Panchal, A.R.; Rodriguez, S.A.; Olivo-Marston, S.E. Association of Burnout with Workforce-Reducing Factors among EMS Professionals. Prehosp. Emerg. Care 2018, 22, 229–236. [Google Scholar] [CrossRef]
- Goyal, P.; Rustagi, N.; Belkic, K. Physicians’ Total Burden of Occupational Stressors: More than Threefold Increased Odds of Burnout. South Med. J. 2021, 114, 409–415. [Google Scholar] [CrossRef]
- Jimenez, R.E.; Bachelet, V.C.; Gomolan, P.; Lefio, L.A.; Goyenechea, M. Violence and burnout in health care emergency workers in Santiago, Chile: A survey-based cross-sectional study. Int. Emerg. Nurs. 2019, 47, 100792. [Google Scholar] [CrossRef] [PubMed]
- Wiskow, C. Giudelines on Workplace Violence in the Health Sector. Comparison of Major Known National Guidelines and Strategies: United Kingdom, Australia, Sweden, USA (OSHA and California); International Labour Office (ILO): Geneva, Switzerland; International Council of Nurses (ICN): Geneva, Switzerland; World Health Organisation (WHO): Geneva, Switzerland; Public Services International (PSI): Ferney-Voltaire, France, 2003; Available online: https://www.who.int/violence_injury_prevention/violence/interpersonal/en/WV_ComparisonGuidelines.pdf (accessed on 9 March 2022).
- International Labour Office (ILO); International Council of Nurses (ICN); World Health Organization (WHO); Public Services International (PSI). Framework Guidelines for Addressing Workplace Violence in the Health Sector; ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in the Health Sector: Geneva, Switzerland, 2002; Available online: https://apps.who.int/iris/rest/bitstreams/50528/retrieve (accessed on 9 March 2022).
- Occupational Safety and Health Administration (OSHA). Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers; U.S. Department of Labour: Washington, DC, USA, 2016. Available online: https://www.osha.gov/sites/default/files/publications/osha3148.pdf (accessed on 9 March 2022).
- Wirth, T.; Peters, C.; Nienhaus, A.; Schablon, A. Interventions for Workplace Violence Prevention in Emergency Departments: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8459. [Google Scholar] [CrossRef]
- Guo, Y.F.; Luo, Y.H.; Lam, L.; Cross, W.; Plummer, V.; Zhang, J.P. Burnout and its association with resilience in nurses: A cross-sectional study. J. Clin. Nurs. 2018, 27, 441–449. [Google Scholar] [CrossRef]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Creedy, D.K.; Sidebotham, M.; Gamble, J.; Pallant, J.; Fenwick, J. Prevalence of burnout, depression, anxiety and stress in Australian midwives: A cross-sectional survey. BMC Pregnancy Childbirth 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppert, K.; Koch, B.; Brähler, E.; Strauß, B. Die Resilienz-Skala (RS)—Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klin. Diagn. Eval. 2008, 1, 226–243. [Google Scholar]
- Al-Maskari, S.A.; Al-Busaidi, I.S.; Al-Maskari, M.A. Workplace violence against emergency department nurses in Oman: A cross-sectional multi-institutional study. Int. Nurs. Rev. 2020, 67, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, M.; Hamra, A.A. Burnout among workers in emergency Departments in Palestinian hospitals: Prevalence and associated factors. BMC Health Serv. Res. 2017, 17, 407. [Google Scholar] [CrossRef] [Green Version]
- Braun, D.; Reifferscheid, F.; Kerner, T.; Dressler, J.L.; Stuhr, M.; Wenderoth, S.; Petrowski, K. Association between the experience of violence and burnout among paramedics. Int. Arch. Occup. Environ. Health 2021, 94, 1559–1565. [Google Scholar] [CrossRef]
- Heckemann, B.; Siegrist-Dreier, S.; Thilo, F.J.S.; Hahn, S. Team efficacy and leadership in managing aggressive situations in the general hospital setting: A qualitative descriptive analysis of focus groups with ward managers. J. Clin. Nurs. 2020, 29, 974–986. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low | Moderate | High | |
|---|---|---|---|
| CBI, work-related | 0–<50 | 50–<75 | ->75–100 |
| CBI, patient-related | 0–<50 | 50–<75 | ->75–100 |
| RS-13 | 13–66 | 67–72 | 73–91 |
| Variables | N | % |
|---|---|---|
| Age | ||
| - 20 to 29 years | 100 | 28.7 |
| - 30 to 39 years | 98 | 28.1 |
| - 40 to 49 years | 80 | 22.9 |
| - 50 to 59 years | 59 | 16.9 |
| - ≥60 years | 11 | 3.2 |
| - N/A | 1 | |
| Gender | ||
| - Female | 202 | 57.9 |
| - Male | 146 | 41.8 |
| - N/A | 1 | |
| Occupation | ||
| - Doctor | 85 | 24.3 |
| - Nurse | 208 | 59.6 |
| - Paramedic | 25 | 7.2 |
| - Other | 31 | 8.9 |
| Type of institution | ||
| - Private | 63 | 18.1 |
| - Public | 183 | 52.4 |
| - Independent | 102 | 29.2 |
| - N/A | 1 | |
| Experiences of physical violence from patients | ||
| - Yes | 305 | 87.4 |
| - No | 42 | 12.0 |
| - N/A | 2 | |
| Experiences of physical violence from relatives | ||
| - Yes | 225 | 64.5 |
| - No | 121 | 34.7 |
| - N/A | 3 | |
| Experiences of verbal abuse from patients | ||
| - Yes | 339 | 97.1 |
| - No | 8 | 2.3 |
| - N/A | 2 | |
| Experiences of verbal abuse from relatives | ||
| - Yes | 329 | 94.3 |
| - No | 18 | 5.2 |
| - N/A | 2 | |
| Perceived stress due to violence experienced | ||
| - Low | 68 | 19.5 |
| - Moderate | 195 | 55.9 |
| - High | 79 | 22.6 |
| - N/A | 7 | |
| How effective were your workplace’s measures preparing you for violent incidents? | ||
| - Insufficient | 159 | 45.6 |
| - Moderate | 154 | 44.1 |
| - Good | 34 | 9.7 |
| - N/A | 2 | |
| Received support following incidents | ||
| -Received support from supervisors | 86 | 24.6 |
| - Received support from colleagues | 258 | 73.9 |
| - Received support from persons outside the workplace | 96 | 27.5 |
| - No support received | 71 | 20.3 |
| - N/A | 4 | |
| Resilience | ||
| - Low | 101 | 28.9 |
| - Moderate | 80 | 22.9 |
| - High | 155 | 44.4 |
| - N/A | 13 |
| Variable | CBI, Work-Related | CBI, Patient-Related | Perceived Stress |
|---|---|---|---|
| Gender | |||
| - Male | 40.4 ± 19.0 | 27.7 ± 17.1 | 5.4 ± 2.5 |
| - Female | 46.4 ± 20.2 | 31.3 ± 18.8 | 5.9 ± 2.2 |
| Age | |||
| - 20 to 29 years | 45.1 ± 21.1 | 32.7 ± 17.0 | 5.8 ± 2.4 |
| - 30 to 39 years | 45.5 ± 21.2 | 30.1 ± 20.1 | 5.6 ± 2.3 |
| - 40 to 49 years | 43.2 ± 17.6 | 29.8 ± 18.6 | 5.8 ± 2.6 |
| - 50 to 59 years | 40.5 ± 18.5 | 25.1 ± 16.0 | 5.5 ± 2.2 |
| - ≥60 years | 40.9 ± 19.8 | 26.3 ± 14.5 | 5.1 ± 1.7 |
| Occupation | |||
| - Doctor | 44.1 ± 19.1 | 26.8 ± 18.2 | 5.4 ± 2.6 |
| - Nurse | 44.8 ± 19.5 | 31.0 ± 17.3 | 5.8 ± 2.1 |
| - Paramedic | 30.2 ± 16.6 | 22.9 ± 16.2 | 4.2 ± 2.4 |
| - Other | 48.3 ± 23.2 | 35.0 ± 22.4 | 6.2 ± 2.5 |
| Type of institution | |||
| - Private | 47.6 ± 22.6 | 30.8 ± 18.1 | 6.3 ± 2.5 |
| - Public | 45.2 ± 19.3 | 31.1 ± 18.2 | 5.6 ± 2.3 |
| - Independent | 39.5 ± 18.5 | 26.8 ± 17.5 | 5.4 ± 2.3 |
| Time working in emergency department | |||
| - 0 to 5 years | 46.7 ± 21.1 | 32.6 ± 16.5 | 5.8 ± 2.3 |
| - 6 to 10 years | 45.6 ± 18.7 | 31.0 ± 18.6 | 5.7 ± 2.3 |
| - 11 to 15 years | 45.8 ± 21.8 | 30.7 ± 20.7 | 5.8 ± 2.2 |
| - Longer than 15 years | 38.7 ± 17.7 | 25.3 ± 17.2 | 5.3 ± 2.5 |
| Verbal abuse from patients | |||
| - Never | 30.8 ± 20.5 | 16.2 ± 9.8 | 3.5 ± 3.0 |
| - Once a year | 36.6 ± 19.5 | 25.5 ± 17.9 | 4.8 ± 2.7 |
| - Once a quarter | 40.8 ± 19.2 | 24.5 ± 13.7 | 4.8 ± 2.2 |
| - Once a month | 39.9 ± 20.5 | 24.7 ± 15.8 | 5.2 ± 2.2 |
| - Once a week | 44.9 ± 17.9 | 32.4 ± 18.1 | 6.0 ± 2.3 |
| - Daily | 52.0 ± 20.5 | 37.5 ± 21.0 | 6.6 ± 2.0 |
| Verbal abuse from relatives | |||
| - Never | 31.2 ± 15.7 | 16.2 ± 12.7 | 2.6 ± 1.8 |
| - Once a year | 38.5 ± 18.0 | 22.7 ± 15.0 | 4.7 ± 2.6 |
| - Once a quarter | 41.6 ± 18.7 | 26.6 ± 15.0 | 5.1 ± 2.2 |
| - Once a month | 41.2 ± 20.6 | 26.8 ± 17.0 | 5.7 ± 2.2 |
| - Once a week | 47.2 ± 19.3 | 32.2 ± 17.2 | 6.0 ± 2.2 |
| - Daily | 50.6 ± 20.2 | 39.3 ± 21.4 | 6.7 ± 1.9 |
| Physical violence from patients | |||
| - Never | 36.5 ± 20.6 | 22.3 ± 14.0 | 4.4 ± 2.5 |
| - Once a year | 41.3 ± 18.1 | 27.4 ± 15.3 | 5.4 ± 2.3 |
| - Once a quarter | 43.7 ± 20.1 | 29.3 ± 18.6 | 5.6 ± 2.3 |
| - Once a month | 46.1 ± 19.5 | 31.1 ± 19.6 | 6.0 ± 2.2 |
| - Once a week | 52.8 ± 19.0 | 38.6 ± 18.7 | 6.8 ± 1.8 |
| - Daily | 40.0 ± 22.1 | 35.8 ± 17.1 | 7.0 ± 2.7 |
| Physical violence from relatives | |||
| - Never | 39.6 ± 20.1 | 25.7 ± 16.3 | 4.8 ± 2.3 |
| - Once a year | 46.0 ± 18.6 | 30.8 ± 18.6 | 5.8 ± 2.2 |
| - Once a quarter | 43.2 ± 19.3 | 30.6 ± 17.7 | 6.0 ± 2.2 |
| - Once a month | 50.7 ± 21.0 | 33.0 ± 21.8 | 6.7 ± 2.2 |
| - Once a week | 49.8 ± 20.0 | 38.5 ± 16.6 | 7.0 ± 1.4 |
| - Daily | 30.4 ± 17.7 | 29.2 ± 11.8 | 5.5 ± 3.5 |
| Preparation by institution | |||
| - Good | 35.7 ± 15.6 | 24.2 ± 16.2 | 4.6 ± 2.3 |
| - Average | 41.3 ± 18.8 | 27.3 ± 16.3 | 5.7 ± 2.2 |
| - Insufficient | 48.3 ± 20.9 | 33.3 ± 19.6 | 5.9 ± 2.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schablon, A.; Kersten, J.F.; Nienhaus, A.; Kottkamp, H.W.; Schnieder, W.; Ullrich, G.; Schäfer, K.; Ritzenhöfer, L.; Peters, C.; Wirth, T. Risk of Burnout among Emergency Department Staff as a Result of Violence and Aggression from Patients and Their Relatives. Int. J. Environ. Res. Public Health 2022, 19, 4945. https://doi.org/10.3390/ijerph19094945
Schablon A, Kersten JF, Nienhaus A, Kottkamp HW, Schnieder W, Ullrich G, Schäfer K, Ritzenhöfer L, Peters C, Wirth T. Risk of Burnout among Emergency Department Staff as a Result of Violence and Aggression from Patients and Their Relatives. International Journal of Environmental Research and Public Health. 2022; 19(9):4945. https://doi.org/10.3390/ijerph19094945
Chicago/Turabian StyleSchablon, Anja, Jan Felix Kersten, Albert Nienhaus, Hans Werner Kottkamp, Wilfried Schnieder, Greta Ullrich, Karin Schäfer, Lisa Ritzenhöfer, Claudia Peters, and Tanja Wirth. 2022. "Risk of Burnout among Emergency Department Staff as a Result of Violence and Aggression from Patients and Their Relatives" International Journal of Environmental Research and Public Health 19, no. 9: 4945. https://doi.org/10.3390/ijerph19094945
APA StyleSchablon, A., Kersten, J. F., Nienhaus, A., Kottkamp, H. W., Schnieder, W., Ullrich, G., Schäfer, K., Ritzenhöfer, L., Peters, C., & Wirth, T. (2022). Risk of Burnout among Emergency Department Staff as a Result of Violence and Aggression from Patients and Their Relatives. International Journal of Environmental Research and Public Health, 19(9), 4945. https://doi.org/10.3390/ijerph19094945