
Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals



Abstract
:1. Introduction
2. Method
2.1. Information Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Risk of Bias of Included Studies
2.4. Study Quality Assessment
2.5. Strategy for Data Synthesis and Analysis
3. Results
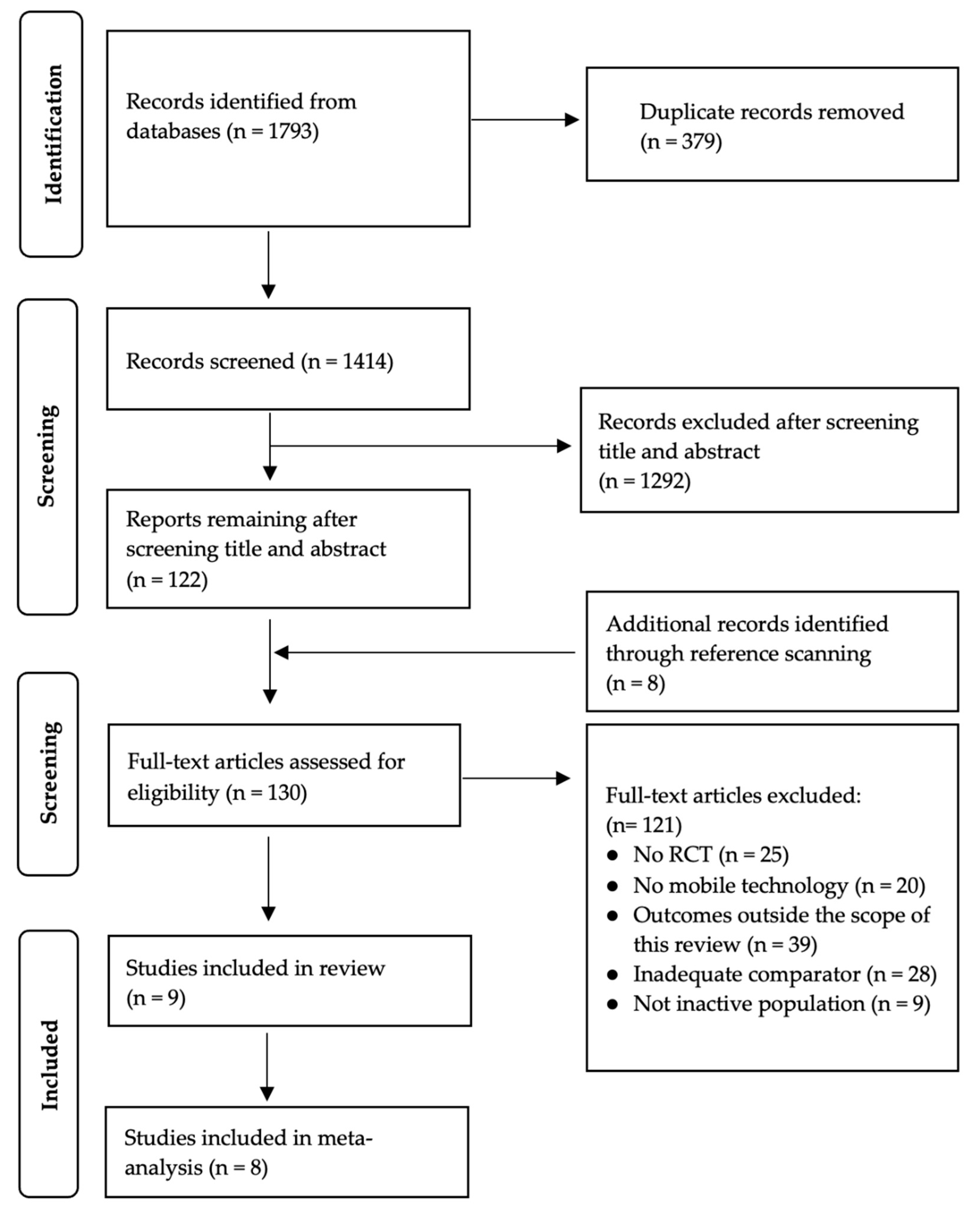
3.1. Search Results
3.2. Study Characteristics
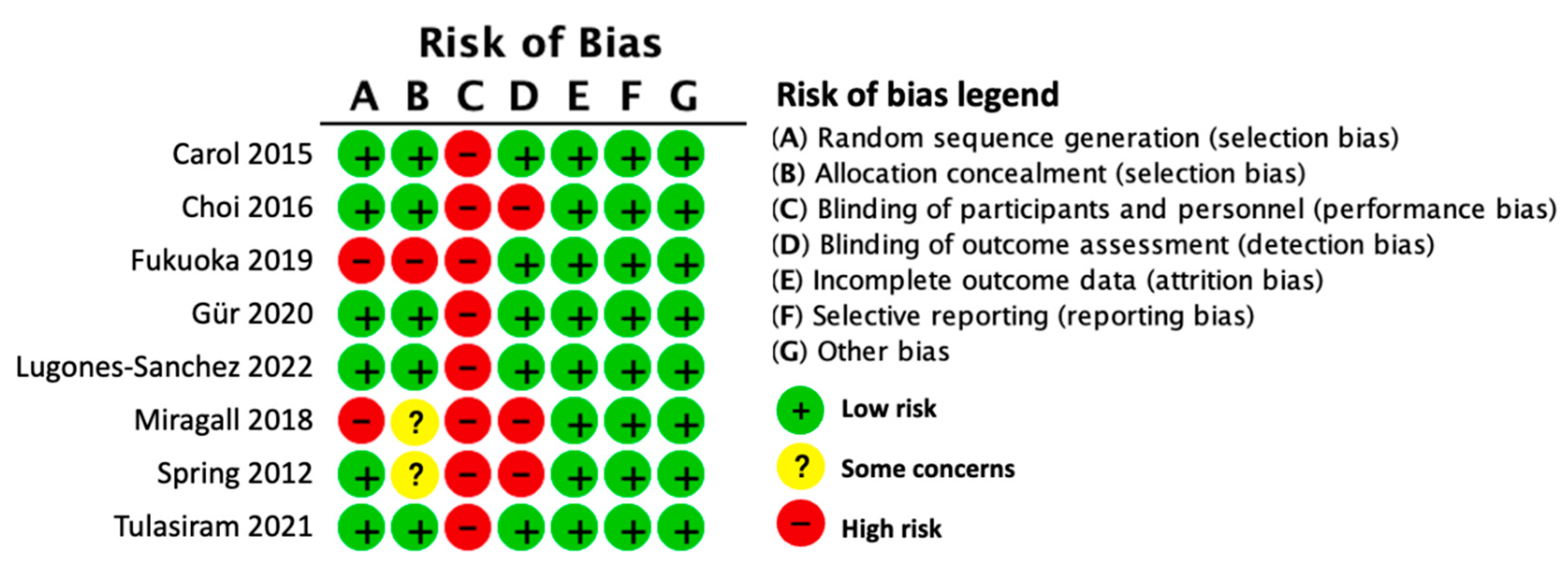
3.3. Risk of Bias
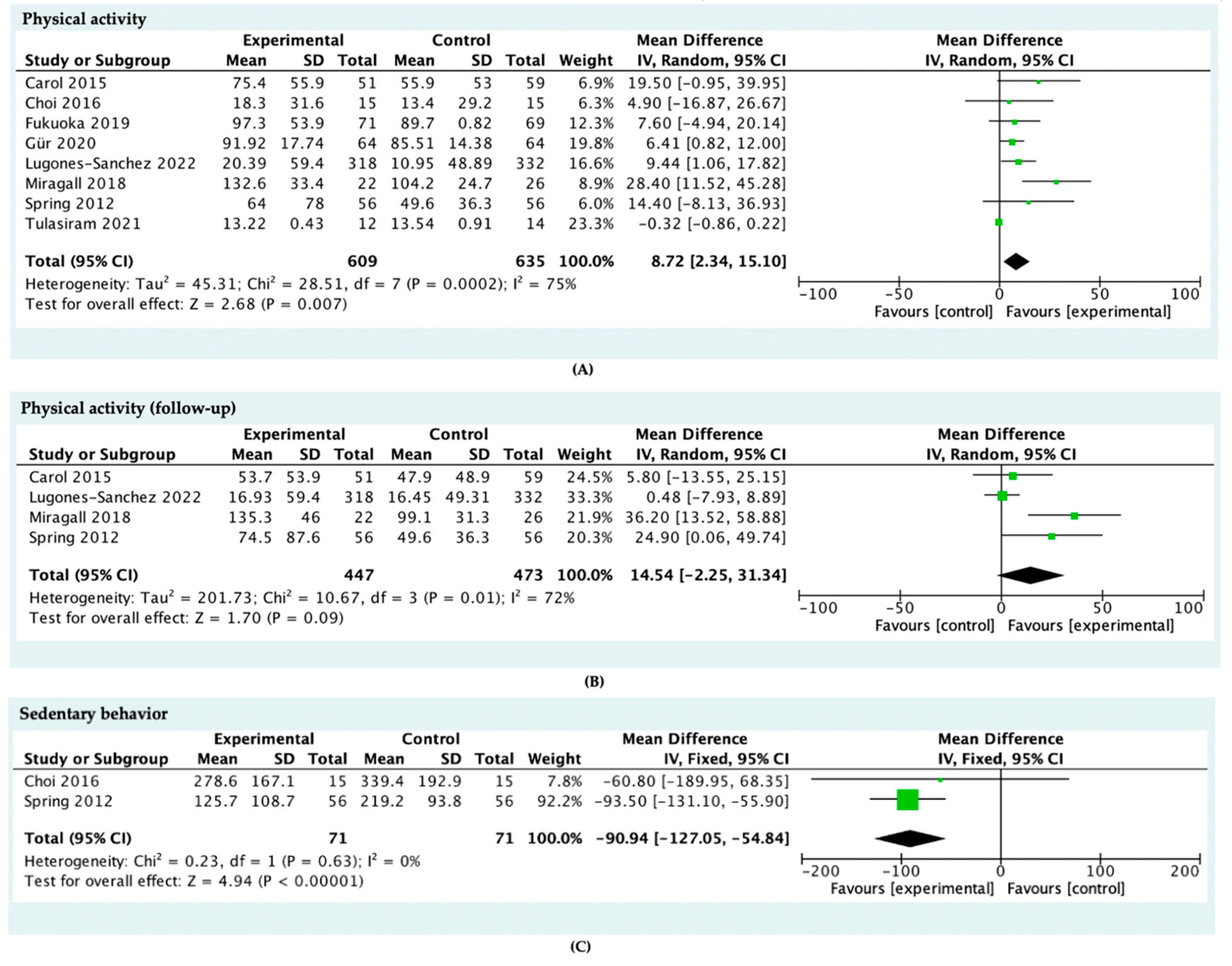
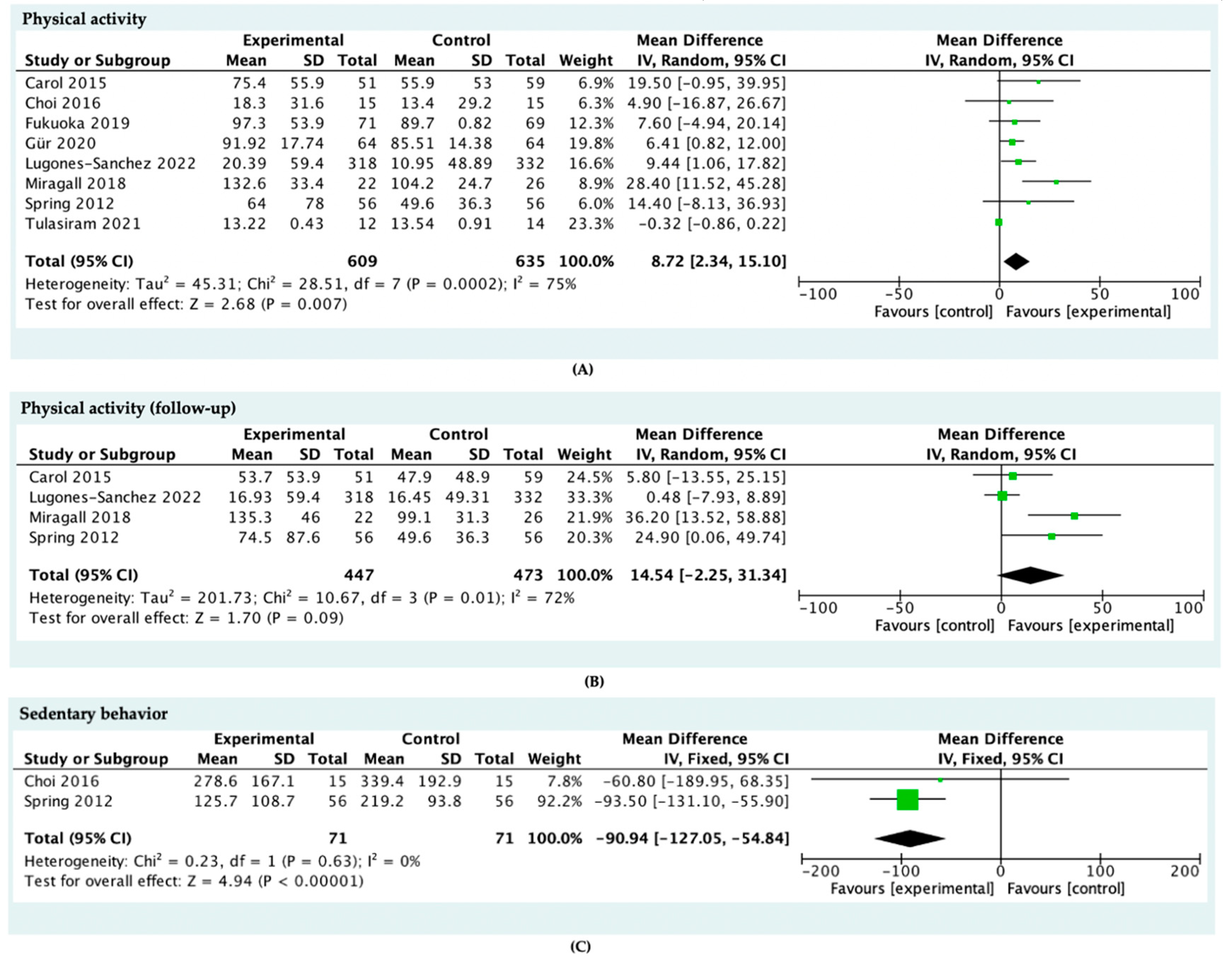
3.4. Effect of Intervention
3.5. Study Quality
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Duration | Participant Characteristic | Setting | Intervention | Dependent Variables | Outcome Measure | Comparison Group |
|---|---|---|---|---|---|---|---|---|
| [36] | RCT | Intervention exposure: 4 weeks | N = 26 Age 18~25 years Male (7) and Female (19) USA | Home | The SmPh app allows step tacking | App impact on cardiorespiratory fitness of college-going adults | Outcome: (i) Aerobic capacity; (ii) Ventilatory equivalent of carbondioxide (iii) Anaerobic threshold (iv) Treadmill distance and time; (v)Heart rate | Traditional walking prescription |
| [40] | RCT | Intervention exposure: 8 weeks | N = 95 Age >45 years Male (26) and Female (69) USA | Home | Three mobile apps shape the user towards more physical activity and fewer daily sedentary time | App impact on daily activity and sedentary time | Outcome: (i) Physical activity (i.e., accelerometer-derived moderate-to-vigorous physical activity) and (ii) Sedentary behavior (i.e., accelerometer-derived sedentary time, EMA-derived sitting time) | A diet-tracking control app |
| [35] | 2-group RCT | Intervention exposure: 3 week, 20 week follow-up | N = 204 Age 21~60 years Male (48) and Female (156) USA | Home | (i) Behavior treatment; (ii) Handheld tool to record and self-regulate their targeted behaviors | The effect of Remote coaching supported by mobile tech- nology and financial incentives to improve diet and activity. | Outcome: (i) Fat and fruit/vegetable consumption; (ii) the saturated fat goal: the Harris–Benedict equation; (iii) Minutes of physical and sedentary activity | No control group |
| [33] | 2-group RCT | Intervention exposure: 3-week intervention and a 3 months follow-up | N = 76 Age 18~40 years Female (65), Male (11) UK | Community, workplace home | (i) Fitbit One to measure steps and provides motivational messages; (ii) Internet-based motivational intervention | The effect of an Internet-based motivational intervention supported by pedometers on physical activity | Outcome: (i) Physical activity; (ii) Stages of Change Questionnaire for exercise; (iii) Decision Balance Questionnaire for exercise; (iv) Self-Efficacy Questionnaire; (v) Processes of Change Questionnaire | Without Fitbit one and internet-based motivational intervention |
| [34] | 2-group RCT | Intervention exposure: 50-day, 20 week follow-up | N = 76 Age 18~65 years Female (82), Male (26) Australia | Home | (i) Active Team app to encourage friendly rivalry within friendship group; (ii)A pedometer to measure steps | The effect of an online social networking physical activity intervention with pedometers delivered via Facebook app | Outcome: Physical activities (Active Australia Survey, Assessment of Quality of Life-6D (AQoL-6D) scale, 36-item Short Form Health Survey) | Teams allocated to the control condition were placed on a waiting list to receive access to the intervention (app and pedometer) |
| [37] | 2-group RCT | Intervention exposure:12 weeks | N = 30 Age 30~36 years pregnant women between 10 and 20 weeks of gestation USA | Home | (i) Initial Brief In-Person Session; (ii) Mobile phone app plus Fitbit | The effect of mobile health intervention in promoting physical activity in Pregnant women | Outcome: Physical activities (The Stanford Brief Physical Activity Survey) Other measures: (i) The Self-Efficacy for Physical Activity; (ii) survey, quiz, scale and checklist | Fitbit Ultra only (accelerometer) |
| [38] | 3-group RCT | Intervention exposure:3 months | N = 210 Age 40~60 years Female (210) USA | Home | Use the app and accelerometer for 9 months | The effects of APP on levels of physical activity | Outcome: Physical activity Other measures: (i) Survey, quiz, scale | Control group: use accelerometer for 9 months |
| [21] | 2-group RCT | Intervention exposure: 8 weeks | N = 128 Age 19–26 years Female (112), Male (16) Turkey | Home | (i) ERVE smartphone app; (ii) An educational video each week under the exercise education component of the ap; (iii) Researchers sent a message once a week to increase motivation. | The effects of a smartphone app on physical activity, quality of life, self-efficacy, and exercise motivation for inactive people | Primary outcome: self-efficacy, health-related quality of life, and motivational orientation for exercise Secondary outcome: BMI and levels of physical activity | No intervention |
| [41] | 2-group RCT | Intervention exposure: 3 months | N = 650 Age 20–65 years Female (445) Male (205) Spain | Primary care center | (i) 5 min of lifestyle counseling before randomization; (ii) low-intensity intervention consisting of a smartphone with the EVIDENT 3 app and a smart band for 3 months; | The effects of a smartphone app combined with a smart band on weight loss, physical activity, and caloric intake in a population with overweight and obesity | (i) Body weight; (ii) Physical activity: International Physical Activity Questionnaire–Short Form; (iii) Caloric intake (kcal/day) and dietary habits: semiquantitative Food Frequency Questionnaire. | A brief counseling only |
Appendix B
| [36] | [40] | [35] | [33] | [34] | [37] | [38] | [21] | [41] | |
| Title and abstract | |||||||||
| (a) identification as randomized trial in title; (b) structured summary | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 |
| Introduction | |||||||||
| (a) scientific background/rationale; (b) specific objectives/hypotheses | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Methods | |||||||||
| Trial design: (a) description of trial design; (b) changes in methods after trial commencement | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| Participants | |||||||||
| (a) eligibility criteria; (b) settings and locations of data collection | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Interventions | |||||||||
| Descriptions of sufficient details to allow replication | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Outcomes | |||||||||
| (a) pre-specified primary and secondary outcomes; (b) changes to outcomes after trial commencement | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| Sample size | |||||||||
| (a) how sample size was determined; (b) if applicable, interim analysis/stopping guidelines | 0.5 | 0.5 | 0 | 0 | 0 | 0 | 0.5 | 0.5 | 0.5 |
| Randomization—sequence generation | |||||||||
| (a) method used; (b) type of randomization including any type of restriction | 0.5 | 1 | 1 | 0 | 0.5 | 0.5 | 0 | 0.5 | 0.5 |
| Allocation concealment mechanism | |||||||||
| Implementation of random allocation sequence, including concealment | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 |
| Implementation | |||||||||
| Who generated random allocation sequence, who enrolled participants, who assigned participants | 0 | 1 | 0 | 0 | 0.5 | 1 | 0 | 1 | 1 |
| Blinding | |||||||||
| (a) if done, who was blinded and how; (b) if relevant, similarity of interventions | 0 | 0.5 | 0 | 0 | 0.5 | NA | NA | NA | NA |
| Statistical methods | |||||||||
| Statistical methods used (a) for primary outcomes; (b) additional analyses | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Results | |||||||||
| Participant flow (a) number of participants randomized, receiving treatment, and analyzed; (b) losses and exclusions, with reasons | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 |
| Recruitment | |||||||||
| (a) dates of recruitment and follow-up; (b) why the trial ended | 0.5, NA | 0.5, NA | 0.5, NA | 0.5,NA | 0.5,NA | 0.5,NA | 0.5,NA | 0.5,NA | 0.5,NA |
| Baseline data | |||||||||
| A table with baseline demographic and clinical characteristics for each group | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 |
| Numbers analyzed | |||||||||
| For each group, number of participants included in each analyses | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Outcomes and Estimation | |||||||||
| (a) results for each group, and the estimated effect size and its precision; (b) absolute and relative effect sizes for binary outcomes | 0.5, NA | 0.5, NA | 0, NA | 0, NA | 0.5, NA | 0.5, NA | 0.5, NA | 0.5, NA | 0.5, NA |
| Ancillary analyses | |||||||||
| Results of any other analyses performed, distinguishing pre-specified from exploratory | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Harms | |||||||||
| Harms or unintended effects in each group | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| Discussion | |||||||||
| Limitations Trial limitations/bias/multiplicity of analyses | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Generalisability | |||||||||
| Generalisability (external validity/applicability) of findings | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
| Interpretation | |||||||||
| Consistent with results and balanced | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Other information | |||||||||
| RegistrationRegistration number and name of registry | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 |
| Protocol | |||||||||
| Where full trial protocol can be accessed | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 |
| Funding | |||||||||
| Sources of funding/ role of funders | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Study quality score attainable | 24 | 24 | 24 | 24 | 24 | 23 | 23 | 23 | 23 |
| Study quality score | 16 | 21.5 | 15.5 | 11.5 | 19 | 17 | 17.5 | 16 | 18 |
| Study quality percentage | 66.7 | 87.8 | 63.2 | 46.9 | 77.6 | 70.8 | 76.1 | 69.6 | 78.2 |
| Study quality rating | High | high | mid | low | high | High | High | High | High |
References
- Breda, J.; Jakovljevic, J.; Rathmes, G.; Mendes, R.; Fontaine, O.; Hollmann, S.; Rütten, A.; Gelius, P.; Kahlmeier, S.; Galea, G. Promoting health-enhancing physical activity in Europe: Current state of surveillance, policy development and implementation. Health Policy 2018, 122, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A. WHO global strategy on diet, physical activity and health. Food Nutr. Bull. 2004, 25, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Committee PAGA, Physical Activity Guidelines Advisory Committee Physical activity guidelines advisory committee report, 2008: To the Secretary of Health and Human Services. Nutr. Rev. 2009, 67, 114–120. [CrossRef]
- World Health Organization. Noncommunicable Diseases Progress Monitor 2015; WHO: Geneva, Switzerland, 2015; p. 232. [Google Scholar]
- Chastin, S.F.M.; Granat, M.H. Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2010, 31, 82–86. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Physical Activity 2018-2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018; Volume 28. [Google Scholar]
- Dounavi, K.; Tsoumani, O. Mobile Health Applications in Weight Management: A Systematic Literature Review. Am. J. Prev. Med. 2019, 56, 894–903. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.O.; Heron, T.E.; Heward, W.L. Improving and assessing the quality of behavioral measurement. Appl. Behav. Anal. 2007, 3, 102–124. [Google Scholar]
- Parrish, A.M.; Chong, K.H.; Moriarty, A.L.; Batterham, M.; Ridgers, N.D. Interventions to Change School Recess Activity Levels in Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 2145–2173. [Google Scholar] [CrossRef]
- Das, P.; Horton, R. Physical activity—time to take it seriously and regularly. Lancet 2016, 388, 1254–1255. [Google Scholar] [CrossRef]
- Gardner, B.; Smith, L.; Lorencatto, F.; Hamer, M.; Biddle, S.J.H. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health Psychol. Rev. 2016, 10, 89–112. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, N.; Godfrey, A.; Lara, J.; Errington, L.; Meyer, T.D.; Rochester, L.; White, M.; Mathers, J.C.; Sniehotta, F.F. Are behavioral interventions effective in increasing physical activity at 12 to 36 months in adults aged 55 to 70 years? A systematic review and meta-analysis. BMC Med. 2013, 11, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, A.; Fitzsimons, C.; Jepson, R.; Saunders, D.H.; Van Der Ploeg, H.P.; Teixeira, P.J.; Gray, C.M.; Mutrie, N. Interventions with potential to reduce sedentary time in adults: Systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1056–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pate, R.R.; Saunders, R.P.; O’Neill, J.R.; Dowda, M. Overcoming barriers to physical activity: Helping youth be more active. ACSM’s Heal. Fit. J. 2011, 15, 7–12. [Google Scholar] [CrossRef]
- Ebben, W.; Brudzynski, L. Motivations and barriers to exercise among college students. J. Exerc. Physiol. Online 2008, 11, 1–11. [Google Scholar]
- Ryu, S. Book Review: mHealth: New Horizons for Health through Mobile Technologies: Based on the Findings of the Second Global Survey on eHealth (Global Observatory for eHealth Series, Volume 3). Healthc. Inform. Res. 2012, 18, 231. [Google Scholar] [CrossRef]
- Tate, E.B.; Spruijt-Metz, D.; O’Reilly, G.; Jordan-Marsh, M.; Gotsis, M.; Pentz, M.A.; Dunton, G.F. mHealth approaches to child obesity prevention: Successes, unique challenges, and next directions. Transl. Behav. Med. 2013, 3, 406–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Kong, X.; Cao, J.; Chen, S.; Li, C.; Huang, J.; Gu, D.; Kelly, T.N. Mobile phone intervention and weight loss among overweight and obese adults: A meta-analysis of randomized controlled trials. Am. J. Epidemiol. 2015, 181, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Logan, A.G. Transforming hypertension management using mobile health technology for telemonitoring and self-care support. Can. J. Cardiol. 2013, 29, 579–585. [Google Scholar] [CrossRef]
- Gür, F.; Gür, G.C.; Ayan, V. The Effect of the ERVE Smartphone App on Physical Activity, Quality of Life, Self-Efficacy, and Exercise Motivation for Inactive People: A Randomized Controlled Trial. Eur. J. Integr. Med. 2020, 39, 101198. [Google Scholar] [CrossRef]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile app-based health promotion programs: A systematic review of the literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef] [Green Version]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laranjo, L.; Ding, D.; Heleno, B.; Kocaballi, B.; Quiroz, J.C.; Tong, H.L.; Chahwan, B.; Neves, A.L.; Gabarron, E.; Dao, K.P.; et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br. J. Sports Med. 2021, 55, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Can smartphone apps increase physical activity? systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef] [PubMed]
- Feter, N.; dos Santos, T.S.; Caputo, E.L.; da Silva, M.C. What is the role of smartphones on physical activity promotion? A systematic review and meta-analysis. Int. J. Public Health 2019, 64, 679–690. [Google Scholar] [CrossRef]
- Stephens, J.; Allen, J. Mobile phone interventions to increase physical activity and reduce weight: A systematic review. J. Cardiovasc. Nurs. 2013, 28, 320–329. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- McCulloch, M. Systematic reviews and meta-analyses: An illustrated step-by-step guide. Natl. Med. J. India 2004, 17, 86–95. [Google Scholar]
- Davies, C.A.; Spence, J.C.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Meta-analysis of internet-delivered interventions to increase physical activity levels. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.; McDonough, S.M.; Murphy, M.H.; Nugent, C.D.; Mair, J.L. Using computer, mobile and wearable technology enhanced interventions to reduce sedentary behaviour: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 105. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: New York, NY, USA, 2019; ISBN 9781119536604. [Google Scholar]
- Miragall, M.; Domínguez-Rodríguez, A.; Navarro, J.; Cebolla, A.; Baños, R.M. Increasing physical activity through an Internet-based motivational intervention supported by pedometers in a sample of sedentary students: A randomised controlled trial. Psychol. Health 2018, 33, 465–482. [Google Scholar] [CrossRef]
- Maher, C.; Ferguson, M.; Vandelanotte, C.; Plotnikoff, R.; De Bourdeaudhuij, I.; Thomas, S.; Nelson-Field, K.; Olds, T. A web-based, social networking physical activity intervention for insufficiently active adults delivered via Facebook app: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e4086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spring, B.; Schneider, K.; McFadden, H.G.; Vaughn, J.; Kozak, A.T.; Smith, M.; Moller, A.C.; Epstein, L.H.; DeMott, A.; Hedeker, D.; et al. Multiple behavior changes in diet and activity: A randomized controlled trial using mobile technology. Arch. Intern. Med. 2012, 172, 789–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tulasiram, B.; Chandrasekaran, B. Are smartphones better in guiding physical activity among sedentary young adults? A randomised controlled trial. Muscles Ligaments Tendons J. 2021, 11, 83–91. [Google Scholar] [CrossRef]
- Choi, J.W.; Lee, J.H.; Vittinghoff, E.; Fukuoka, Y. mHealth Physical Activity Intervention: A Randomized Pilot Study in Physically Inactive Pregnant Women. Matern. Child Health J. 2016, 20, 1091–1101. [Google Scholar] [CrossRef]
- Fukuoka, Y.; Haskell, W.; Lin, F.; Vittinghoff, E. Short- And long-term effects of a mobile phone app in conjunction with brief in-person counseling on physical activity among Physically InactiveWomen the mPED Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e194281. [Google Scholar] [CrossRef] [Green Version]
- Master, H.; Bley, J.A.; Coronado, R.A.; Robinette, P.E.; White, D.K.; Pennings, J.S.; Archer, K.R. Effects of physical activity interventions using wearables to improve objectively-measured and patient-reported outcomes in adults following orthopaedic surgical procedures: A systematic review. PLoS ONE 2022, 17, e0263562. [Google Scholar] [CrossRef]
- King, A.C.; Hekler, E.B.; Grieco, L.A.; Winter, S.J.; Sheats, J.L.; Buman, M.P.; Banerjee, B.; Robinson, T.N.; Cirimele, J. Effects of three motivationally targeted mobile device applications on initial physical activity and sedentary behavior change in midlife and older adults: A randomized trial. PLoS ONE 2016, 11, e0156370. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Repiso-Gento, I.; Adalia, E.G.; Ramirez-Manent, J.I.; Sanchez-Calavera, M.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Garcia-Ortiz, L. Long-term Effectiveness of a Smartphone App Combined With a Smart Band on Weight Loss, Physical Activity, and Caloric Intake in a Population With Overweight and Obesity (Evident 3 Study): Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e30416. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Shin, Y.H.; Kim, S.K.; Lee, M. Mobile phone interventions to improve adolescents’ physical health: A systematic review and meta-analysis. Public Health Nurs. 2019, 36, 787–799. [Google Scholar] [CrossRef]
- Pradal-Cano, L.; Lozano-Ruiz, C.; Pereyra-Rodríguez, J.J.; Saigí-Rubió, F.; Bach-Faig, A.; Esquius, L.; Xavier Medina, F.; Aguilar-Martínez, A. Using mobile applications to increase physical activity: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 8238. [Google Scholar] [CrossRef] [PubMed]
- Gal, R.; May, A.M.; van Overmeeren, E.J.; Simons, M.; Monninkhof, E.M. The Effect of Physical Activity Interventions Comprising Wearables and Smartphone Applications on Physical Activity: A Systematic Review and Meta-analysis. Sports Med.-Open 2018, 4, 42. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-León, C.; Villalonga, C.; Munoz-Torres, M.; Ruiz, J.R.; Banos, O. Mobile and wearable technology for the monitoring of diabetes-related parameters: Systematic review. JMIR mHealth uHealth 2021, 9, e25138. [Google Scholar] [CrossRef] [PubMed]
- Cudejko, T.; Button, K.; Willott, J.; Al-Amri, M. Applications of wearable technology in a real-life setting in people with knee osteoarthritis: A systematic scoping review. J. Clin. Med. 2021, 10, 5645. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Cowgill, B.O.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Schuster, M.A. Two-Year BMI outcomes from a school-based intervention for nutrition and exercise: A randomized trial. Pediatrics 2016, 137, e20152493. [Google Scholar] [CrossRef] [Green Version]
- Quelly, S.B.; Norris, A.E.; Dipietro, J.L. Impact of mobile apps to combat obesity in children and adolescents: A systematic literature review. J. Spec. Pediatr. Nurs. 2016, 21, 5–17. [Google Scholar] [CrossRef]
| Concept | Description of Detail |
|---|---|
| Population | Inactive Population |
| Intervention | Mobile health intervention |
| Comparison | Control group without the mobile health intervention |
| Outcomes | Effects of mobile health intervention on physical activity and sedentary behavior |
| Concept | Description of Detail |
|---|---|
| Intervention | Application OR App OR Smartphone OR Smart Phone |
| Outcomes | Sedentary OR sedentary behavior OR sedentary behavior OR sitting OR screen time OR inactive OR inactivity |
| Digital Library. | Query String | Scope | Limitation |
|---|---|---|---|
| Web of science | AB = (application OR app OR smartphone OR smartphone OR tablet) AND AB = (sedentary OR sedentary behavior OR sedentary behavior OR sitting OR screen time OR inactive OR inactivity) | Abstract | Limited to journals, English, 2006–2022 |
| CINAHL | AB = (application OR app OR smartphone OR smartphone OR tablet) AND AB = (sedentary OR sedentary behavior OR sedentary behavior OR sitting OR screen time OR inactive OR inactivity) | Abstract | Limited to journals, English, 2006–2022 |
| Scopus | (TITLE-ABS-KEY (application OR app OR smartphone OR smart AND phone OR tablet) AND TITLE-ABS-KEY (sedentary OR sedentary AND behavior OR sedentary AND behavior OR sitting OR screen AND time OR inactive OR inactivity)) AND PUBYEAR > 2006 AND (LIMIT-TO (PUBSTAGE, “final”)) AND (LIMIT-TO (DOCTYPE, “ar”) OR LIMIT-TO (DOCTYPE, “cp”)) AND (LIMIT-TO (LANGUAGE, “English”)) | Title, Abstract and keywords | Limited to journals, English, publication stage: final, 2006–2022 |
| PsychInfo | (application OR app OR smartphone OR smartphone OR tablet).tw. AND (sedentary OR sedentary behavior OR sedentary behavior OR sitting OR screen time OR inactive OR inactivity).tw. | Title and Abstract | Limited to journals, English, human, 2006–2022 |
| PubMed | (application [Title/Abstract] OR app [Title/Abstract] OR smartphone [Title/Abstract] OR smartphone [Title/Abstract] OR tablet [Title/Abstract]) AND (sedentary [Title/Abstract] OR sedentary behavior [Title/Abstract] OR sedentary behavior [Title/Abstract] OR sitting [Title/Abstract] OR screen time [Title/Abstract] OR inactive [Title/Abstract] OR inactivity [Title/Abstract]) | Title and Abstract | Limited to journals, English, human, 2006–2022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Wang, W.; Li, M.; Sheng, H.; Zhai, Y. Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals. Int. J. Environ. Res. Public Health 2022, 19, 4905. https://doi.org/10.3390/ijerph19084905
Zhang M, Wang W, Li M, Sheng H, Zhai Y. Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals. International Journal of Environmental Research and Public Health. 2022; 19(8):4905. https://doi.org/10.3390/ijerph19084905
Chicago/Turabian StyleZhang, Meng, Wei Wang, Mingye Li, Haomin Sheng, and Yifei Zhai. 2022. "Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals" International Journal of Environmental Research and Public Health 19, no. 8: 4905. https://doi.org/10.3390/ijerph19084905
APA StyleZhang, M., Wang, W., Li, M., Sheng, H., & Zhai, Y. (2022). Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals. International Journal of Environmental Research and Public Health, 19(8), 4905. https://doi.org/10.3390/ijerph19084905