
Effects of Different Low-Intensity Exercise Types on Duration, Energy Expenditure and Perceived Exertion in Obese Individuals

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Testing Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsigos, C.; Hainer, V.; Basdevant, A.; Finer, N.; Fried, M.; Mathus-Vliegen, E.; Micic, A.; Maislos, M.; Roman, G.; Schutz, Y.; et al. Management of obesity in adults: European clinical practice guidelines. Obes. Facts 2008, 1, 106–116. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2018.
- World Health Organization. Attaining the Nine Global Noncommunicable Diseases Targets; A Shared Responsibility; Glob. Status Rep. NCDs; World Health Organization: Geneva, Switzerland, 2014.
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body fatness and cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X. The Medical Risks of Obesity. Postgrad. Med. 2009, 121, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Goldfield, G.S. Physical activity in the treatment of childhood overweight and obesity: Current evidence and research issues. Med. Sci. Sports Exerc. 1999, 31, S553–S559. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Marcus, B.H.; Gallagher, K.I.; Napolitano, M.; Lang, W. Effect of Exercise Duration and Intensity on Weight Loss in Overweight, Sedentary Women. JAMA 2003, 290, 1323–1330. [Google Scholar] [CrossRef]
- Duncan, J.J.; Gordon, N.F.; Scott, C.B. Women walking for health and fitness: How much is enough? JAMA 1991, 266, 3295–3299. [Google Scholar] [CrossRef]
- McQueen, M.A. Exercise Aspects of Obesity Treatment. Ochsner J. 2009, 9, 140–143. [Google Scholar]
- Whaley, M.H.; Brubaker, P.H.; Otto, R.M.; Armstrong, L.E. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; Volume 7, pp. 551–565. [Google Scholar]
- Poirier, P.; Després, J.P. Exercise in weight management of obesity. Cardiol. Clin. 2001, 19, 459–470. [Google Scholar] [CrossRef]
- Jakicic, J.M. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. American college of sports medicine. Med. Sci. Sports Exerc. 2001, 33, 2145–2156. [Google Scholar] [CrossRef]
- Wing, R.R.; Hill, J.O. Successful weight loss maintenance. Annu. Rev. Nutr. 2001, 21, 323–341. [Google Scholar] [CrossRef]
- Catenacci, V.A.; Ogden, L.G.; Stuht, J.; Phelan, S.; Wing, R.R.; Hill, J.O.; Wyatt, H.R. Physical Activity Patterns in the National Weight Control Registry. Obesity 2008, 16, 153–161. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.; Church, T.S. The Role of Exercise and Physical Activity in Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2013, 56, 441–447. [Google Scholar] [CrossRef]
- Ehrman, J.K.; Gordon, P.M.; Visich, P.S.; Keteyian, S.J. Exercise prescription for obese patients. Clinical Exercise Physiology, 3rd ed.; Humain Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Jakicic, J.M.; Rickman, A.D.; Lang, W.; Davis, K.K.; Gibbs, B.B.; Neiberg, R.; Marcus, M.D. Time-based physical activity interventions for weight loss: A randomized trial. Med. Sci. Sports Exerc. 2015, 47, 1061. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Winters, C.; Lang, W.; Wing, R.R. Effects of Intermittent Exercise and Use of Home Exercise Equipment on Adherence, Weight Loss, and Fitness in Overweight Women. JAMA 1999, 282, 1554–1560. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Marcus, B.H.; Lang, W.; A Janney, C. Effect of Exercise on 24-Month Weight Loss Maintenance in Overweight Women. Arch. Intern. Med. 2008, 168, 1550–1559. [Google Scholar] [CrossRef]
- Ekkekakis, P.; Hall, E.E.; Petruzzello, S. Practical markers of the transition from aerobic to anaerobic metabolism during exercise: Rationale and a case for affect-based exercise prescription. Prev. Med. 2004, 38, 149–159. [Google Scholar] [CrossRef]
- Blaak, E.E. Basic disturbances in skeletal muscle fatty acid metabolism in obesity and type 2 diabetes mellitus. Proc. Nutr. Soc. 2004, 63, 323–330. [Google Scholar] [CrossRef]
- Corpeleijn, E.; Mensink, M.; Kooi, M.E.; Roekaerts, P.M.; Saris, W.H.; Blaak, E.E. Impaired Skeletal Muscle Substrate Oxidation in Glucose-intolerant Men Improves After Weight Loss. Obesity 2008, 16, 1025–1032. [Google Scholar] [CrossRef]
- Corpeleijn, E.; Saris, W.H.M.; Blaak, E.E. Metabolic flexibility in the development of insulin resistance and type 2 diabetes: Effects of lifestyle. Obes. Rev. 2009, 10, 178–193. [Google Scholar] [CrossRef]
- Kelley, D.E.; Goodpaster, B.; Wing, R.R.; Simoneau, J.-A. Skeletal muscle fatty acid metabolism in association with insulin resistance, obesity, and weight loss. Am. J. Physiol. Metab. 1999, 277, E1130–E1141. [Google Scholar] [CrossRef]
- Mensink, M.; Blaak, E.E.; van Baak, M.A.; Wagenmakers, A.J.; Saris, W.H. Plasma Free Fatty Acid Uptake and Oxidation Are Already Diminished in Subjects at High Risk for Developing Type 2 Diabetes. Diabetes 2001, 50, 2548–2554. [Google Scholar] [CrossRef]
- Blaak, E.E.; Saris, W.H. Substrate oxidation, obesity and exercise training. Best Pract. Res. Clin. Endocrinol. Metab. 2002, 16, 667–678. [Google Scholar] [CrossRef][Green Version]
- Schrauwen, P.; Van Aggel-Leijssen, D.P.; Hul, G.; Wagenmakers, A.J.; Vidal, H.; Saris, W.H.; van Baak, M.A. The effect of a 3-month low-intensity endurance training program on fat oxidation and acetyl-CoA carboxylase-2 expression. Diabetes 2002, 51, 2220–2226. [Google Scholar] [CrossRef]
- Achten, J.; Gleeson, M.; Jeukendrup, A.E. Determination of the exercise intensity that elicits maximal fat oxidation. Med. Sci. Sports Exerc. 2002, 34, 92–97. [Google Scholar] [CrossRef]
- Perez-Martin, A.; Dumortier, M.; Raynaud, E.; Brun, J.F.; Fedou, C.; Bringer, J.; Mercier, J. Balance of substrate oxidation during submaximal exercise in lean and obese people. Diabetes Metab. 2001, 27, 466–475. [Google Scholar]
- Romain, A.; Fedou, C.; Mercier, J.; Brun, J. Exercise targeted at the level of maximal lipid oxidation in overweight and obesity: A meta-analysis: T3: PO. 23. Obes. Rev. 2010, 11, 229. [Google Scholar]
- Venables, M.C.; Jeukendrup, A.E. Endurance training and obesity: Effect on substrate metabolism and insulin sensitivity. Med. Sci. Sports Exerc. 2008, 40, 495–502. [Google Scholar] [CrossRef]
- Campbell, L.; Wallman, K.; Green, D. The effects of intermittent exercise on physiological outcomes in an obese population: Continuous versus interval walking. J. Sports Sci. Med. 2010, 9, 24–30. [Google Scholar]
- Coquart, J.B.; Lemaire, C.; Dubart, A.E.; Luttembacher, D.P.; Douillard, C.; Garcin, M. Intermittent versus continuous exercise: Effect of lower exercise in obese women. J. Am. Coll. Sport Med. 2008, 40, 2–7. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A.G. Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Mazurek, K.; Zmijewski, P.; Krawczyk, K.; Czajkowska, A.; Kęska, A.; Kapuściński, P.; Mazurek, T. High intensity interval and moderate continuous cycle training in a physical education programme improves health-related fitness in young females. Biol. Sport 2016, 33, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Bordenave, S.; Flavier, S.; Fédou, C.; Brun, J.; Mercier, J. Exercise calorimetry in sedentary patients: Procedures based on short 3 min steps underestimate carbohydrate oxidation and overestimate lipid oxidation. Diabetes Metab. 2007, 33, 379–384. [Google Scholar] [CrossRef]
- Péronnet, F.; Massicotte, D. Table of nonprotein respiratory quotient: An update. Can. J. Sport Sci. 1991, 16, 23–29. [Google Scholar] [PubMed]
- Shaw, K.A.; Gennat, H.C.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst. Rev. 2006, 4, 1–112. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine Position Stand. Appropriate Physical Activity Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Lupton, J.R.; Brooks, J.A.; Butte, N.F.; Caballero, B.; Flatt, J.P.; Fried, S.K. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2002; Volume 5, pp. 589–768. [Google Scholar]
- Hausswirth, C.; Brisswalter, J. Le coût énergétique de la course à pied de durée prolongée: Étude des paramètres d’influence. Sci. Sports 1999, 14, 59–70. [Google Scholar] [CrossRef]
- Browder, K.D.; Wilkerson, J.D. Relationship Between Mechanical and Physiological Energy Costs and Efficiency of Treadmill Walking in Active And Inactive Females, ISBS-Conference Proceedings Archive. In Proceedings of the International Conference of Biomechanics in Sport, Amherst, MA, USA, 23–26 June 1993. [Google Scholar]
- Hargreaves, M.; Spriet, L.L. Skeletal muscle energy metabolism during exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- Mendes, F.S.N.S.; Castro, C.L.B.D.; Araújo, C.G. Obesos apresentam menor aderência a programa de exercício supervisionado. Rev. Bras. Cardiol. 2010, 23, 230–237. [Google Scholar]
- Ekkekakis, P.; Parfitt, G.; Petruzzello, S.J. The Pleasure and Displeasure People Feel When they Exercise at Different Intensities. Sports Med. 2011, 41, 641–671. [Google Scholar] [CrossRef]
- Dishman, R.K. Compliance/adherence in health-related exercise. Health Psychol. 1982, 1, 237–267. [Google Scholar] [CrossRef]
- Walter, R. Thompson. ACSM’s Guidelines to Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; Volume 8, pp. 183–206. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Mean ± SD | [Range] |
|---|---|---|
| Age (years) | 26.1 ± 6.0 | [19; 35] |
| Body weight (kg) | 104.2 ± 19,4 | [87; 150] |
| Height (cm) | 175.7 ± 8.8 | [166; 190] |
| Body mass index (kg/m2) | 33.5 ± 3.6 | [30.1; 41.6] |
| VO2 peak (ml/min/kg) | 30 ± 8.9 | [16.2; 46.6] |
| Maximal fat oxidation rate (mg/min) | 133.8 ± 33.4 | [88.7; 220.4] |
| % VO2 peak at FAT max | 30.3 ± 5.3 | [24; 37] |
| Variables | Mean ± SD | ANOVA | ||||
|---|---|---|---|---|---|---|
| Continuous | Intermittent ½ | Intermittent ¼ | F(2,18) | p-Value | ηp2 | |
| Exercise duration (min) | 55.4 ± 6.0 | 61.6 ± 6.6 | 65.1 ± 13.4 * (p = 0.017; d = 0.75) | 5.23 | 0.016 | 0.368 |
| Total energy (kcal) | 372 ± 98.2 | 374.4 ± 116.1 | 398 ± 145.5 | 0.58 | 0.569 | 0.060 |
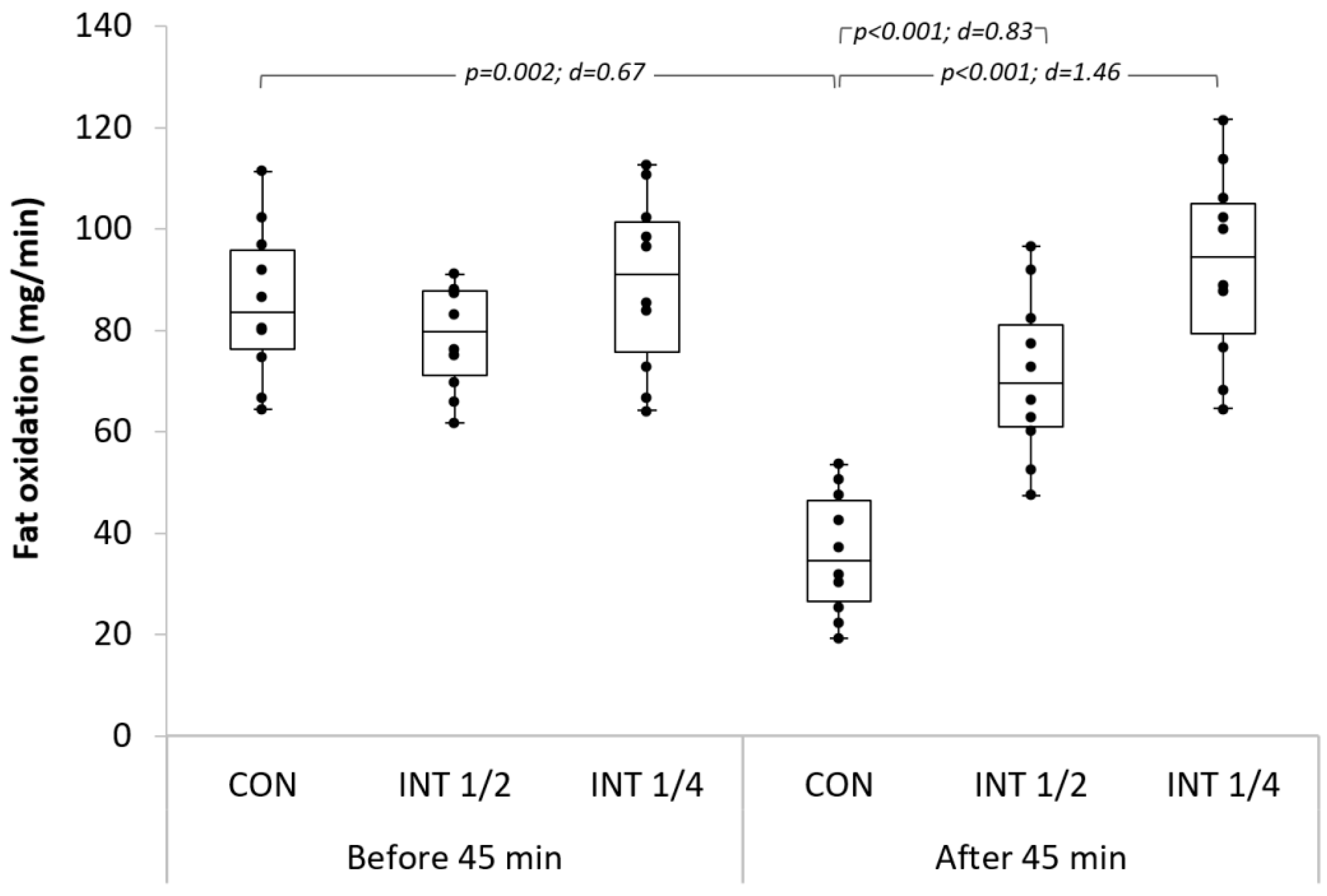
| Fat energy after 45 min (kcal) | 3.9 ± 3.8 | 14.4 ± 13.2 * (p = 0.045; d = 0.72) | 16.2 ± 16.5 * (p = 0.029; d = 0.73) | 5.09 | 0.018 | 0.361 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanfir, M.A.; Awicha, H.B.; Masmoudi, L.; Hmadou, F.B.; Dardouri, W.; Alardan, S.; Nouira, S.; Zouch, M. Effects of Different Low-Intensity Exercise Types on Duration, Energy Expenditure and Perceived Exertion in Obese Individuals. Int. J. Environ. Res. Public Health 2022, 19, 4893. https://doi.org/10.3390/ijerph19084893
Khanfir MA, Awicha HB, Masmoudi L, Hmadou FB, Dardouri W, Alardan S, Nouira S, Zouch M. Effects of Different Low-Intensity Exercise Types on Duration, Energy Expenditure and Perceived Exertion in Obese Individuals. International Journal of Environmental Research and Public Health. 2022; 19(8):4893. https://doi.org/10.3390/ijerph19084893
Chicago/Turabian StyleKhanfir, Mohamed Ali, Hassen Ben Awicha, Liwa Masmoudi, Faten Ben Hmadou, Wajdi Dardouri, Sultan Alardan, Sabeur Nouira, and Mohamed Zouch. 2022. "Effects of Different Low-Intensity Exercise Types on Duration, Energy Expenditure and Perceived Exertion in Obese Individuals" International Journal of Environmental Research and Public Health 19, no. 8: 4893. https://doi.org/10.3390/ijerph19084893
APA StyleKhanfir, M. A., Awicha, H. B., Masmoudi, L., Hmadou, F. B., Dardouri, W., Alardan, S., Nouira, S., & Zouch, M. (2022). Effects of Different Low-Intensity Exercise Types on Duration, Energy Expenditure and Perceived Exertion in Obese Individuals. International Journal of Environmental Research and Public Health, 19(8), 4893. https://doi.org/10.3390/ijerph19084893