
Cancers: What Are the Costs in Relation to Disability-Adjusted Life Years? A Systematic Review and Meta-Analysis

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preliminary Considerations
2.2. Eligibility Criteria and Study Selection
2.3. Literature Search
2.4. Outcomes
2.5. Data Extraction
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
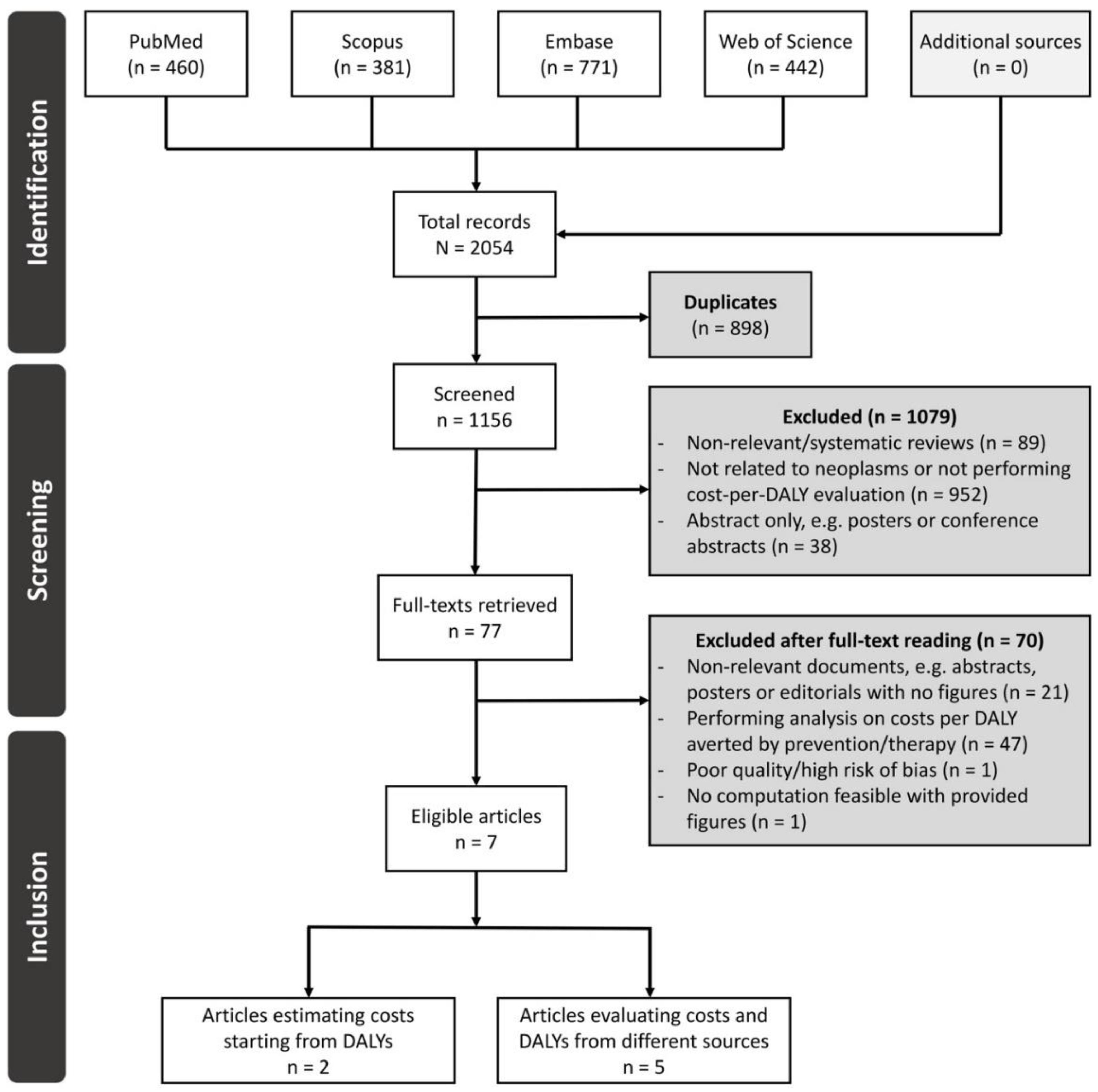
3.1. Study Selection
3.2. Characteristics of Included Studies
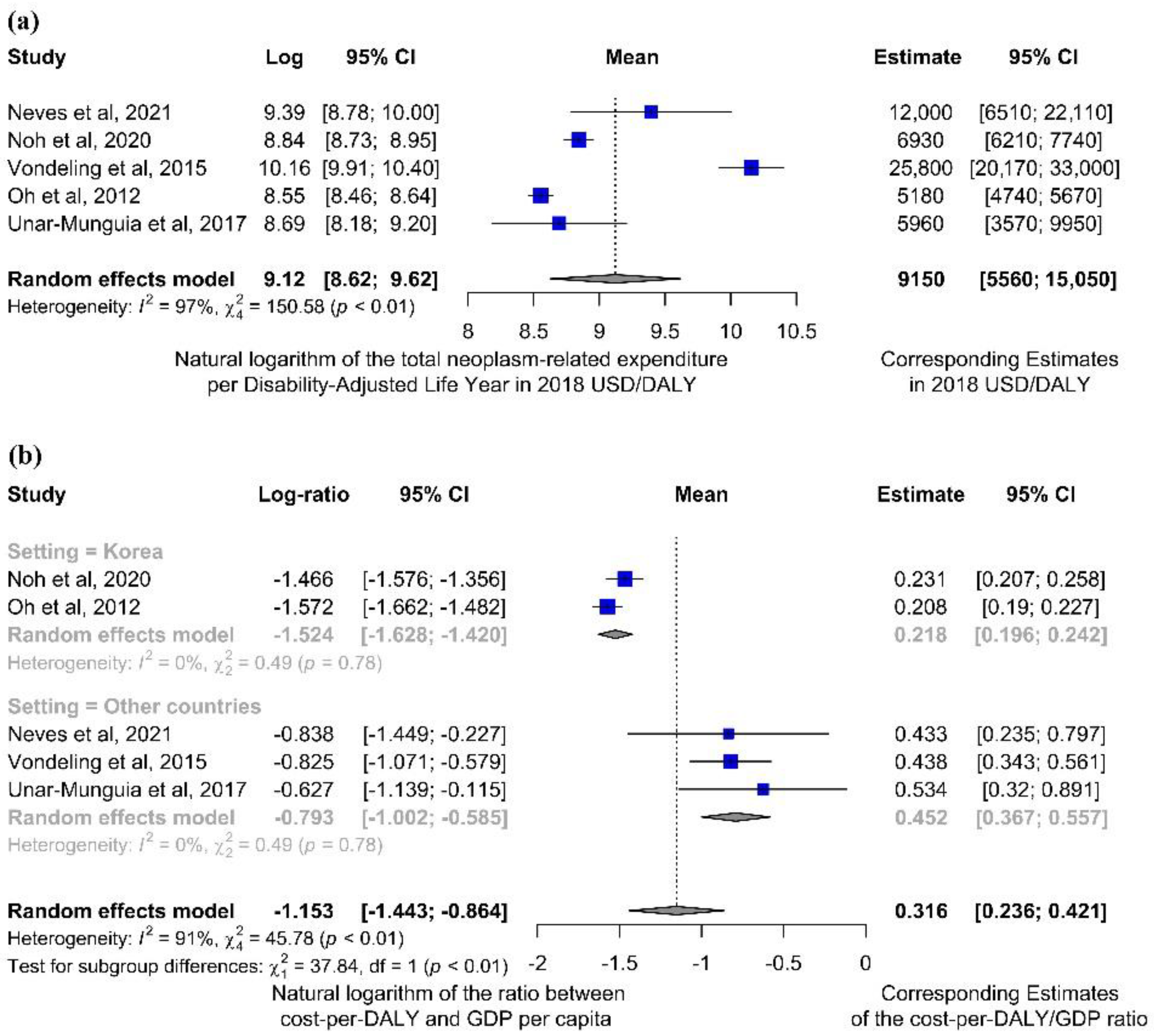
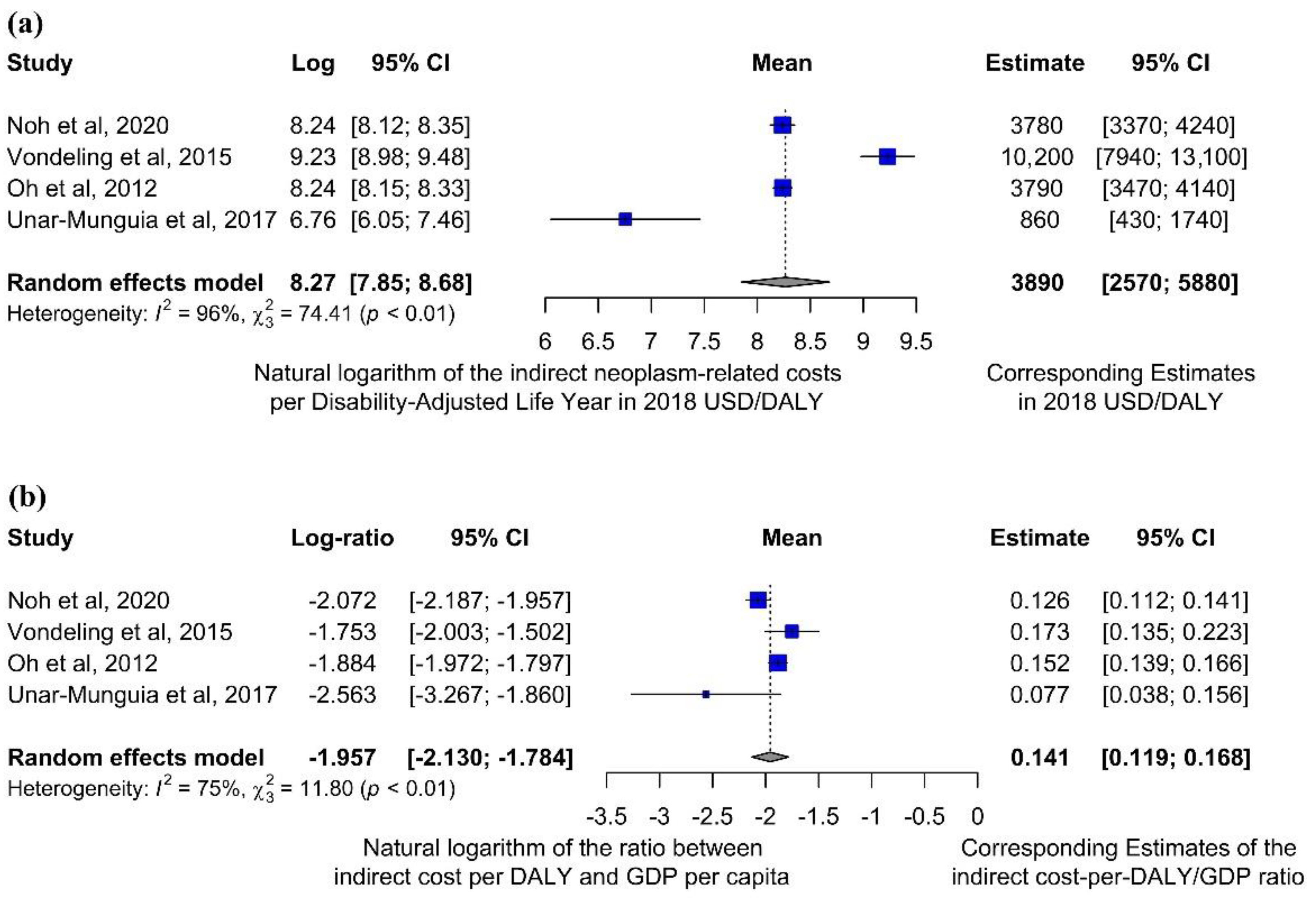
3.3. Quantitative Analyses
3.4. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-Adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, S.; Easterbrooke, L.; Taylor, S. The Financial Impacts of Cancer. Available online: https://www.bristol.ac.uk/media-library/sites/geography/pfrc/pfrc1210-financial-impacts-of-cancer-report.pdf (accessed on 13 April 2022).
- Brown, M.L.; Lipscomb, J.; Snyder, C. The Burden of Illness of Cancer: Economic Cost and Quality of Life. Annu. Rev. Public Health 2001, 22, 91–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, A.; Lundqvist, A.; Lorgelly, P.; Norrlid, H.; Schaffer, S.K.; Lewis, F.; Hernandez-Villafuerte, K.; Lindgren, P.; Garau, M.; Welin, K.-O.; et al. Improving Efficiency and Resource Allocation in Future Cancer Care. Available online: https://www.ohe.org/publications/improving-efficiency-and-resource-allocation-future-cancer-care (accessed on 13 April 2022).
- Mattiuzzi, C.; Lippi, G. Cancer statistics: A comparison between World Health Organization (WHO) and Global Burden of Disease (GBD). Eur. J. Public Health 2020, 30, 1026–1027. [Google Scholar] [CrossRef]
- Murray, C.J. Quantifying the burden of disease: The technical basis for disability-adjusted life years. Bull. World Health Organ. 1994, 72, 429–445. [Google Scholar]
- Murray, C.J.L.; Acharya, A.K. Understanding DALYs. J. Health Econ. 1997, 16, 703–730. [Google Scholar] [CrossRef]
- McCormick, P.J. Cancer Tsunami: Emerging Trends, Economic Burden, and Perioperative Implications. Curr. Anesthesiol. Rep. 2018, 8, 348–354. [Google Scholar] [CrossRef]
- National Cancer Institute Financial Burden of Cancer Care. Available online: https://progressreport.cancer.gov/after/economic_burden#field_most_recent_estimates (accessed on 28 January 2022).
- Schlueter, M.; Chan, K.; Lasry, R.; Price, M. The cost of cancer—A comparative analysis of the direct medical costs of cancer and other major chronic diseases in Europe. PLoS ONE 2020, 15, e0241354. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Cancer—Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 8 December 2021).
- De la Jara, J.J.; Bastias, G.; Ferreccio, C.; Moscoso, C.; Sagues, S.; Cid, C.; Bronstein, E.; Herrera, C.; Nervi, B.; Corvalan, A.; et al. A snapshot of cancer in Chile: Analytical frameworks for developing a cancer policy. Biol. Res. 2015, 48, 10. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wohlin, C. Guidelines for Snowballing in Systematic Literature Studies and a Replication in Software Engineering. Available online: https://www.wohlin.eu/ease14.pdf (accessed on 13 April 2022).
- The World Bank GDP per Capita (Constant 2010 US$). Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.KD (accessed on 20 October 2021).
- Chiou, C.F.; Hay, J.W.; Wallace, J.F.; Bloom, B.S.; Neumann, P.J.; Sullivan, S.D.; Yu, H.T.; Keeler, E.B.; Henning, J.M.; Ofman, J.J. Development and validation of a grading system for the quality of cost-effectiveness studies. Med. Care 2003, 41, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Ofman, J.J.; Sullivan, S.D.; Neumann, P.J.; Chiou, C.F.; Henning, J.M.; Wade, S.W.; Hay, J.W. Examining the value and quality of health economic analyses: Implications of utilizing the QHES. J. Manag. Care Pharm. 2003, 9, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.G.; Wilson, R.F.; Ritu Sharma, M.; John Bridges, B.; Niessen, L.; Bass, E.B.; Kevin Frick, M. Methods Research Report Best Practices for Conducting Economic Evaluations in Health Care: A Systematic Review of Quality Assessment Tools. Agency Healthc. Res. Qual. 2012, 12, 1–50. [Google Scholar]
- Weir, C.J.; Butcher, I.; Assi, V.; Lewis, S.C.; Murray, G.D.; Langhorne, P.; Brady, M.C. Dealing with missing standard deviation and mean values in meta-analysis of continuous outcomes: A systematic review. BMC Med. Res. Methodol. 2018, 18, 25. [Google Scholar] [CrossRef]
- Organisation for European Co-operation and Development Purchasing Power Parities (PPP). Available online: https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm (accessed on 10 March 2022).
- Coin News, U.S. Inflation Calculator. Available online: https://www.usinflationcalculator.com (accessed on 5 October 2021).
- U.S. Bureau of Labor Statistics Consumer Price Index (CPI). Available online: https://www.bls.gov/cpi/ (accessed on 5 October 2021).
- Higgins, J.P.T.; White, I.R.; Anzures-Cabrera, J. Meta-analysis of skewed data: Combining results reported on log-transformed or raw scales. Stat. Med. 2008, 27, 6072–6092. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.; Baptista, J.; Azen, S.P.; Pike, M.C. Obtaining Confidence Intervals for the Risk Ratio in Cohort Studies. Biometrics 1978, 34, 469–474. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 10 February 2022).
- Neves, M.; Trigo, F.; Rui, B.; João, C.; Lúcio, P.; Mariana, N.; Mendes, J.; Pedrosa, H.; Geraldes, C. Multiple Myeloma in Portugal: Burden of Disease and Cost of Illness. Pharmacoeconomics 2021, 39, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Noh, J.; Jang, H.; Cho, J.; Kang, D.R.; Kim, T.H.; Shin, D.C.; Kim, C. Estimating the disease burden of lung cancer attributable to residential radon exposure in Korea during 2006–2015: A socio-economic approach. Sci. Total Environ. 2020, 749, 141573. [Google Scholar] [CrossRef] [PubMed]
- Vondeling, G.; Rozenbaum, M.; Dvortsin, E.; Postma, M.; Zeevat, F. Burden of Early and Advanced Breast Cancer in The Netherlands. Value Health 2016, 19, A756. [Google Scholar] [CrossRef]
- Oh, I.H.; Yoon, S.J.; Yoon, T.Y.; Choi, J.M.; Choe, B.K.; Kim, E.J.; Kim, Y.A.; Seo, H.Y.; Park, Y.H. Health and economic burden of major cancers due to smoking in Korea. Asian Pac. J. Cancer Prev. 2012, 13, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Unar-Munguía, M.; Meza, R.; Colchero, M.A.; Torres-Mejía, G.; de Cosío, T.G. Economic and disease burden of breast cancer associated with suboptimal breastfeeding practices in Mexico. Cancer Causes Control 2017, 28, 1381–1391. [Google Scholar] [CrossRef]
- John, R.M.; Ross, H. Economic value of disability adjusted life years lost to cancers. J. Clin. Oncol. 2010, 28, 1561. [Google Scholar] [CrossRef]
- Ranganathan, K.; Singh, P.; Raghavendran, K.; Wilkins, E.G.; Hamill, J.B.; Aliu, O.; Newman, L.A.; Hutton, D.; Momoh, A.O. The Global Macroeconomic Burden of Breast Cancer. Ann. Surg. 2021, 274, 1067–1072. [Google Scholar] [CrossRef]
- Ock, M.; Lee, J.Y.; Oh, I.H.; Park, H.; Yoon, S.J.; Jo, M.W. Disability weights measurement for 228 causes of disease in the Korean burden of disease study. J. Korean Med. Sci. 2016, 31, S129–S138. [Google Scholar] [CrossRef]
- Stouthard, M.E.A.; Essink-Bot, M.; Bonsel, G.; Barendregt, J.; Kramers, P.; Van de Water, H.; Gunning-Schepers, L.; Van Der Maas, P. Disability Weights for Diseases in the Netherlands. Available online: http://dare.uva.nl/document/174853 (accessed on 1 March 2022).
- EUROCARE Scientific Direction EUROCARE-4. Available online: http://www.eurocare.it/Eurocare4/tabid/62/Default.aspx (accessed on 14 December 2021).
- EpiGear International Pty Ltd. DisMod II. Available online: http://www.epigear.com/index_files/dismod_ii.html (accessed on 14 December 2021).
- Devleesschauwer, B.; McDonald, S.; Haagsma, J.; Praet, N.; Havelaar, A.; Speybroeck, N. The DALY Calculator—A Graphical User Interface for Stochastic DALY Calculation in R. Available online: https://cran.r-project.org/web/packages/DALY/index.html (accessed on 14 December 2021).
- Alkire, B.C.; Bergmark, R.W.; Chambers, K.; Lin, D.T.; Deschler, D.G.; Cheney, M.L.; Meara, J.G. Head and neck cancer in South Asia: Macroeconomic consequences and the role of the head and neck surgeon. Head Neck 2016, 38, 1242–1247. [Google Scholar] [CrossRef]
- Melaku, Y.A.; Appleton, S.L.; Gill, T.K.; Ogbo, F.A.; Buckley, E.; Shi, Z.; Driscoll, T.; Adams, R.; Cowie, B.C.; Fitzmaurice, C. Incidence, prevalence, mortality, disability-adjusted life years and risk factors of cancer in Australia and comparison with OECD countries, 1990–2015: Findings from the Global Burden of Disease Study. Cancer Epidemiol. 2018, 52, 43–54. [Google Scholar] [CrossRef]
- Safiri, S.; Sepanlou, S.G.; Ikuta, K.S.; Bisignano, C.; Salimzadeh, H.; Delavari, A.; Ansari, R.; Roshandel, G.; Merat, S.; Fitzmaurice, C.; et al. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study. Lancet Gastroenterol. Hepatol. 2019, 4, 913–933. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.Y.; Chen, H.M.; Liao, K.H.; Ko, B.S.; Hsiao, F.Y. Economic burden of cancers in Taiwan: A direct and indirect cost estimate for 2007–2017. BMJ Open 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Yabroff, K.R.; Lund, J.; Kepka, D.; Mariotto, A. Economic Burden of Cancer in the United States: Estimates, Projections, and Future Research. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2006–2014. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO)—Department of Data and Analytics. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2019; WHO Press: Geneva, Switzerland, 2020; pp. 1–41. [Google Scholar]
- Tsuchiya, A. Accounting for time and age in summary measures of population health. In Summary Measures of Population Health: Concepts, Ethics, Measurement and Applications; Murray, C.J.L., Salomon, J.A., Mathers, C.D., Lopez, A.D., Eds.; WHO Press: Geneva, Switzerland, 2002; pp. 657–662. [Google Scholar]
- Anand, S.; Hanson, K. Disability-adjusted life years: A critical review. J. Health Econ. 1997, 16, 685–702. [Google Scholar] [CrossRef]
- Barendregt, J.J.; Bonneux, L.; Van der Maas, P.J. DALYs: The age-weights on balance. Bull. World Health Organ. 1996, 74, 439–443. [Google Scholar]
- Callen, T. Gross Domestic Product: An Economy’s All. Available online: https://www.imf.org/external/pubs/ft/fandd/basics/gdp.htm (accessed on 13 December 2020).
- Townsend, J.; Greenland, K.; Curtis, V. Costs of diarrhoea and acute respiratory infection attributable to not handwashing: The cases of India and China. Trop. Med. Int. Health 2017, 22, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Dalal, K.; Svanström, L. Economic Burden of Disability Adjusted Life Years (DALYs) of Injuries. Health 2015, 7, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Mo, X.; Gai, R.T.; Tachibana, Y.; Bolt, T.; Takahashi, Y.; Nakayama, T. The burden of disease and the cost of illness attributable to child maltreatment in Japan: Long-term health consequences largely matter. BMC Public Health 2020, 20, 1296. [Google Scholar] [CrossRef]
- Ashenfelter, O.; Greenstone, M. Estimating the Value of a Statistical Life: The Importance of Omitted Variables and Publication Bias. Am. Econ. Rev. 2004, 94, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Kniesner, T.J.; Viscusi, W.K. The Value of a Statistical Life. Vanderbilt Law Research Paper No. 19-15. 2019. Available online: https://law.vanderbilt.edu/phd/faculty/w-kip-viscusi/368_Value_of_Statistical_Life_Oxford.pdf (accessed on 14 December 2021).
- Bellavance, F.; Dionne, G.; Lebeau, M. The value of a statistical life: A meta-analysis with a mixed effects regression model. J. Health Econ. 2009, 28, 444–464. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Cheung, S.; Fasso-Opie, A.; Galvin, O.; Moniz, L.S.; Earle, D.; Durham, T.; Menzo, J.; Li, N.; Duffy, S.; et al. The impact of inherited retinal diseases in the united states of america (Us) and canada from a cost-of-illness perspective. Clin. Ophthalmol. 2021, 15, 2855–2866. [Google Scholar] [CrossRef] [PubMed]
- Lebeau, M.; Duguay, P.; Boucher, A. Costs of occupational injuries and diseases in Québec. J. Saf. Res. 2014, 50, 89–98. [Google Scholar] [CrossRef]
- Herrera-Araujo, D.; Mikecz, O.; Pica-Ciamarra, U. Placing a monetary value on the human health component of zoonotic diseases: A methodological note with an application to cysticercosis in Africa. Prev. Vet. Med. 2020, 175, 104862. [Google Scholar] [CrossRef]
- Miller, T.R.; Waehrer, G.M.; Oh, D.L.; Boparai, S.P.; Walker, S.O.; Marques, S.S.; Harris, N.B. Adult health burden and costs in California during 2013 associated with prior adverse childhood experiences. PLoS ONE 2020, 15, e0228019. [Google Scholar] [CrossRef] [Green Version]
- Hirth, R.A.; Chernew, M.E.; Miller, E.; Fendrick, A.M.; Weissert, W.G. Willingness to pay for a quality-adjusted life year: In search of a standard. Med. Decis. Mak. 2000, 20, 332–342. [Google Scholar] [CrossRef]
- Viscusi, W.K.; Masterman, C.J. Income Elasticities and Global Values of a Statistical Life. J. Benefit-Cost Anal. 2017, 8, 226–250. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Leaders’ Summit. The Economics of Cancer Prevention & Control. 2014. Available online: https://www.uicc.org/sites/main/files/atoms/files/WCLS2014_economics_of_cancer_FINAL.pdf (accessed on 13 April 2022).
- Cheatley, J.; Aldea, A.; Lerouge, A.; Devaux, M.; Vuik, S.; Cecchini, M. Tackling the cancer burden: The economic impact of primary prevention policies. Mol. Oncol. 2021, 15, 779–789. [Google Scholar] [CrossRef]
- Emmons, K.M.; Colditz, G.A. Realizing the Potential of Cancer Prevention—The Role of Implementation Science. N. Engl. J. Med. 2017, 376, 986–990. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| 1st Author, Year | Scope and Setting | Study Period | Study Aim | Study Type | Nr. Patients/Simulations | Perspective | Neoplasm Type |
|---|---|---|---|---|---|---|---|
| Neves et al., 2021 | National: Portugal | 2014–2018 * | To assess the burden and costs of multiple myeloma in Portugal | Longitudinal retrospective study | 1941 | Healthcare system | Multiple myeloma |
| Noh et al., 2020 | National: Korea | 2006–2015 * | To compute lung cancer burdens related to radon | Longitudinal retrospective study | 69,168 | Societal | Lung cancer |
| Vondeling et al., 2018 | National: Netherlands | 1995–2014 * | To report the total health and economic burden ascribable to breast cancer | Longitudinal retrospective study | 73,261 | Societal | Breast cancer |
| Oh et al., 2012 | National: Korea | 2008 | To quantify the health and economic burden of smoking-related cancers in Korea | Cross-sectional study | NA † | Societal | 11 major smoking- related cancers |
| Unar-Munguia et al., 2017 | National: Mexico | 2012 | To estimate breast cancer’s lifetime economic and disease burden, attributable to suboptimal breastfeeding practices | Simulated prospective study | 100,000 (virtual) | Societal | Breast cancer |
| John et al., 2010 | Worldwide: 205 countries | 2004 (country- level data), 2008 (data by GNI group) | To estimate global economic losses due to cancers, starting from the economic burden expressed in DALYs | Economic evaluation | NA § | Societal | 17 types of cancer |
| Ranganathan et al., 2020 | International: Low-middle-income countries | 2005–2015 * | To estimate breast cancer survival trends and to quantify the economic burden of breast cancer in low-middle-income countries | Cross-sectional study and economic evaluation | NA § | Societal | Breast cancer |
| 1st Author, Year | Currency (Year) | Age- Weighting | DALY Discounting | Data Source(s) for DALY Burden | Data Source(s) for Costs |
|---|---|---|---|---|---|
| Neves et al., 2021 | EUR, 2018 | NA | NA | YLLs: mortality data from European Cancer Information System, life expectancy data from the Portuguese Institute of Statistics YLDs: prevalence from Portuguese National Healthcare System hospitals, disability weight from WHO expert panels and GBD Study 2016 | Direct: National tariffs, cost by diagnosis-related-groups, Iqvia databases Indirect: NA |
| Noh et al., 2020 | USD, 2013 (for indirect costs) and 2017 (for direct costs) | NA | NA | YLLs: mortality data and life expectancy tables from Statistics Korea YLDs: population statistics and prevalence from Korean National Health Insurance database and cancer registry, disability weights from the literature [38] | Direct: National Health Insurance Service and Out-of-Pocket payments from the National Health Insurance Corporation survey Indirect: morbidity, unemployment or premature death from the Labour Statistics Bureau (Ministry of Health) |
| Vondeling et al., 2018 | EUR, 2014 | NA | 1.5% | YLLs: Netherlands Life Expectancy Tables and mortality data from Netherlands Comprehensive Cancer Organization (IKNL) and National Cancer Registry (NCR) YLDs: incidence data from IKNL and NCR, disability weight from literature [39] and duration of disease from EUROCARE-4 project [40] | Direct: National Institute for Public Health and the Environment and Central Statistics Bureau Indirect: socio-economic data from the Central Statistics Bureau |
| Oh et al., 2012 | USD, 2008 | NA | NA | YLLs: Mortality data and specific frequency measures from Korean National Health Insurance Corporation database and the National Statistical Office YLDs: incidence data from Korean National Health Insurance Corporation database and the National Cancer Information Center, disability duration through DISMOD II software [41] | Direct: National Health Insurance Corporation records and 2009 national survey for out-of-pocket costs. Korea Health Panel survey for direct non-medical costs and caregivers’ costs Indirect: socio-economic data from the Ministry of Employment and Labour and cause of death from the National Statistical Office |
| Unar-Munguia et al., 2017 | USD, 2015 | NA | 3% | YLLs and YLDs: computation provided by the DALY calculator (R software) [42] based on parameters from Global Cancer Observatory and Global Burden of Disease 2010 | Direct: Mexican National Previdence Institute and Ministry of Health Indirect: socio-economic data from the National survey of Occupation and Employment |
| John et al., 2010 | USD, 2008 | NA | NA | YLLs and YLDs: Global Burden of Disease 2004 and 2008 | Estimated as GDP * DALY |
| Ranganathan et al., 2020 | USD, 2015 | NA | 3% | YLLs: incidence data from a variety of sources including WHO, censuses, vital registrations, and population-based cancer registries, life expectancy tables from Institute for Health Metrics and Evaluation YLDs: data from Institute for Health Metrics and Evaluation, Global Health Data Exchange | Estimated as VSL * DALY, where VSL was computed according to population and socio-economic statistics from literature [43] |
| (a) Studies performing separate economic analyses related to costs and DALYs. | |||||
| 1st Author, Year | Income Group | Costs (2018 USD mlns) | DALYs (Thousands) | Cost-per-DALY Ratio (a Posteriori) (2018 USD/DALY) | GDP per Capita (2018 USD) |
| Neves et al., 2021 | High | 106.9 | 8.93 | 12,000 | 27,736 |
| Noh et al., 2020 | High | 2460 | 355 | 6900 | 30,015 |
| Vondeling et al., 2018 | High | 1666 | 64.6 | 25,800 | 58,846 |
| Oh et al., 2012 | High | 3515 | 679 | 5200 | 24,949 |
| Unar-Munguia et al., 2017 | Upper-middle | 94.23 | 15.8 | 6000 | 11,160 |
| (b) Studies estimating costs based on disease burden (DALYs) and a priori assumed cost-per-DALY ratios. | |||||
| 1st Author, Year | Income Group | Costs (2018 USD mlns) | DALYs (thousands) | Cost-per-DALY Ratio (a priori) (2018 USD/DALY) † | |
| John et al., 2010 | All groups represented | High income: 853,000 Upper-middle income: 90,600 Low-middle income: 85,700 Low income: 14,700 Total costs: 1044,000 | High income: 18,094 Upper-middle income: 8727 Low-middle income: 34,389 Low income: 21,645 Total DALYs: 82,855 | High income: 47,100 * Upper-middle income: 10,400 * Low-middle income: 2500 * Low income: 680 * | |
| Ranganathan et al., 2020 | Low-middle | Sub-Saharan Africa: 1964 Southern Asia: 2090 India: 1419 Bangladesh: 153 Bhutan: 1.235 Nepal: 14.3 Pakistan: 473 | Sub-Saharan Africa: 604.9 Southern Asia: 1294 India: 840.4 Bangladesh: 119 Bhutan: 0.439 Nepal: 18.2 Pakistan: 311 | Sub-Saharan Africa: 3250 * Southern Asia: 1615 * India: 1689 * (GDP per capita: 1701) Bangladesh: 1285 * (GDP per capita: 1323) Bhutan: 2813 * (GDP per capita: 2916) Nepal: 786 * (GDP per capita: 955) Pakistan: 1521 * (GDP per capita: 1437) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garlasco, J.; Nurchis, M.C.; Bordino, V.; Sapienza, M.; Altamura, G.; Damiani, G.; Gianino, M.M. Cancers: What Are the Costs in Relation to Disability-Adjusted Life Years? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4862. https://doi.org/10.3390/ijerph19084862
Garlasco J, Nurchis MC, Bordino V, Sapienza M, Altamura G, Damiani G, Gianino MM. Cancers: What Are the Costs in Relation to Disability-Adjusted Life Years? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(8):4862. https://doi.org/10.3390/ijerph19084862
Chicago/Turabian StyleGarlasco, Jacopo, Mario Cesare Nurchis, Valerio Bordino, Martina Sapienza, Gerardo Altamura, Gianfranco Damiani, and Maria Michela Gianino. 2022. "Cancers: What Are the Costs in Relation to Disability-Adjusted Life Years? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 8: 4862. https://doi.org/10.3390/ijerph19084862
APA StyleGarlasco, J., Nurchis, M. C., Bordino, V., Sapienza, M., Altamura, G., Damiani, G., & Gianino, M. M. (2022). Cancers: What Are the Costs in Relation to Disability-Adjusted Life Years? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(8), 4862. https://doi.org/10.3390/ijerph19084862