
Family Resilience and Adolescent Mental Health during COVID-19: A Moderated Mediation Model

Abstract
:1. Introduction
1.1. Adolescents’ Stress Perception and Metal Health during COVID-19
1.2. Family Resilience and Adolescent Mental Health
1.3. The Role of Meta-Mood
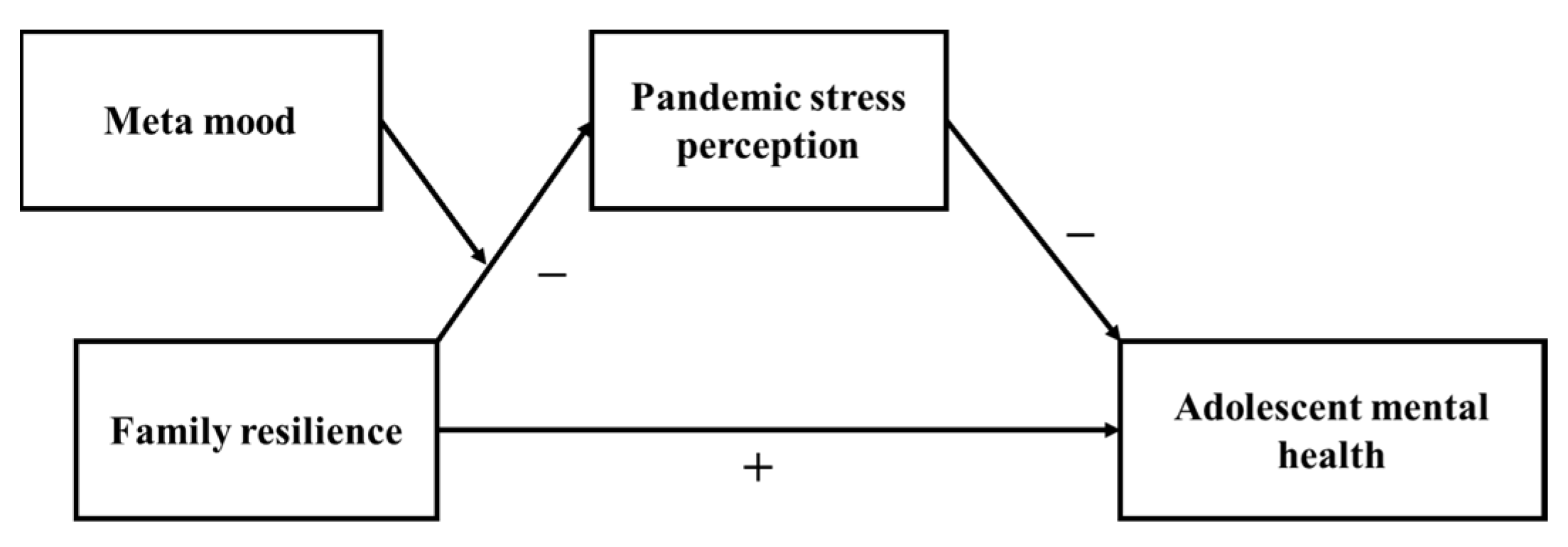
1.4. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Family Resilience
2.3.2. Pandemic Stress Perception Questionnaire
2.3.3. Meta-Mood
2.3.4. Adolescent Mental Health
2.4. Data Analysis Methods
3. Results
3.1. Data Screening
3.2. Descriptive Analysis
3.2.1. Adolescent Mental Health
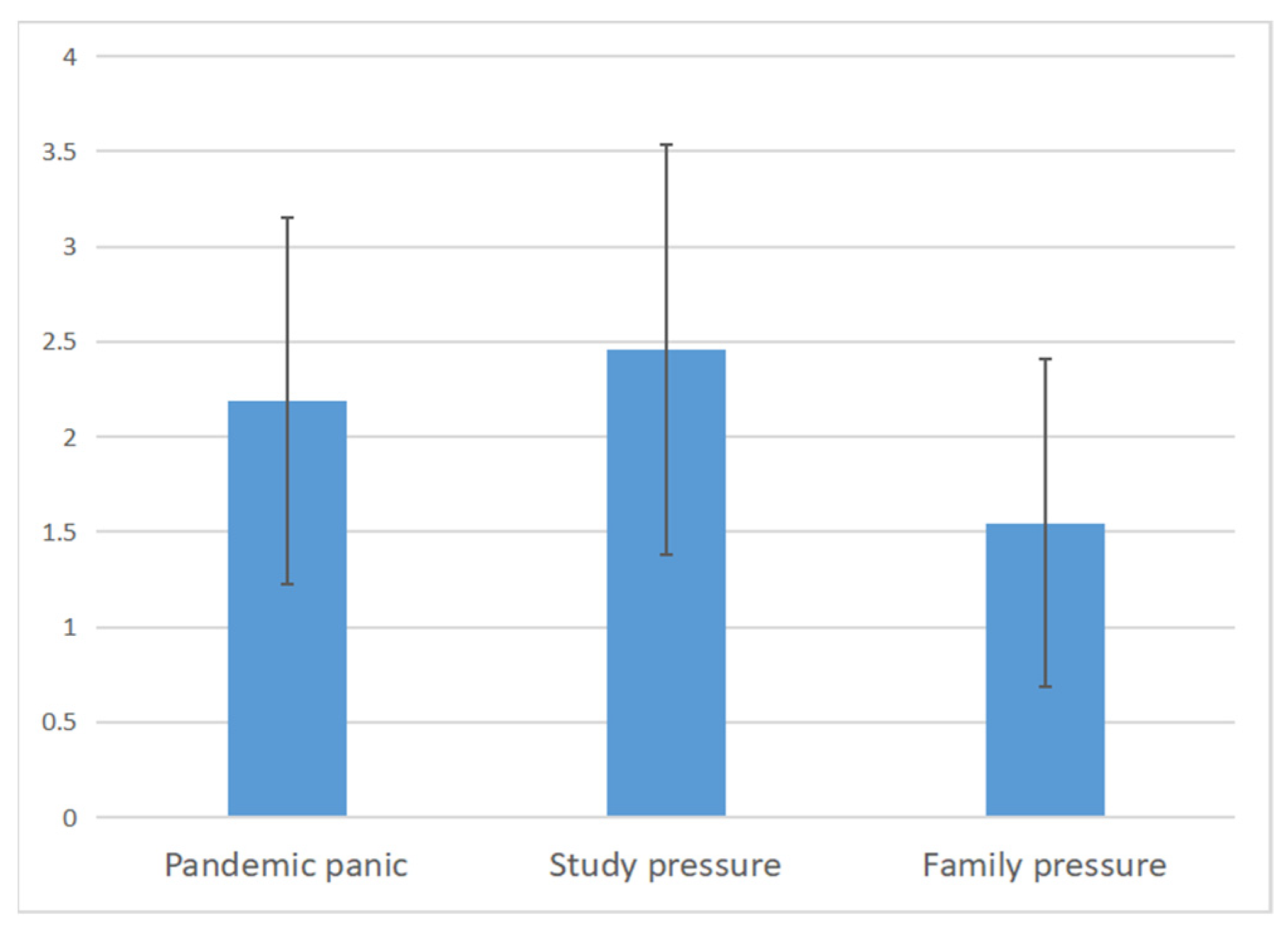
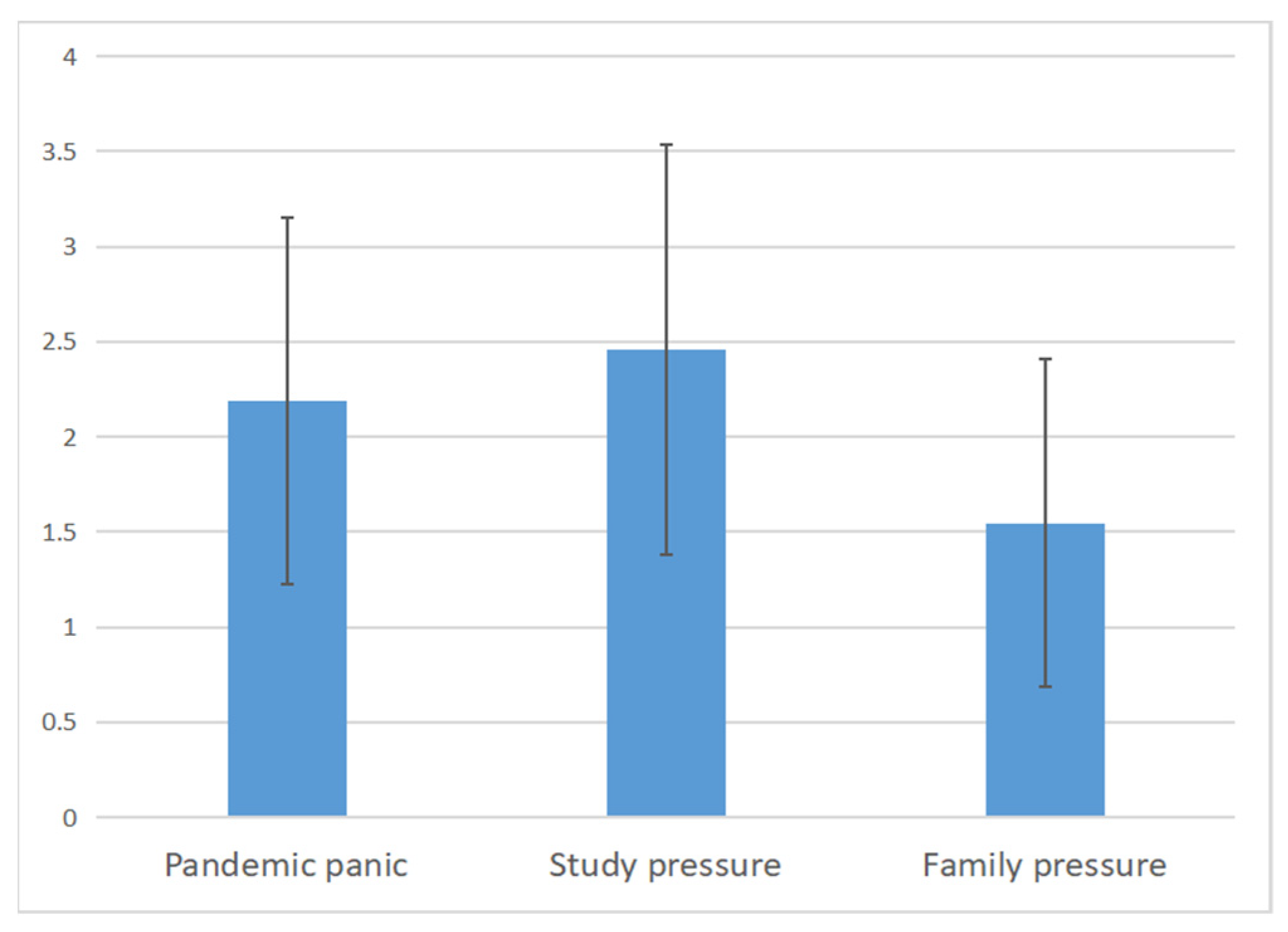
3.2.2. Adolescents’ Pandemic Stress Perception
3.2.3. Family Resilience
3.2.4. Adolescents’ Meta-Mood
3.3. Analysis of Differences in Adolescents’ Mental Health
3.4. Analysis of Differences in Adolescents’ Stress Perception
3.5. Correlation Analysis
3.6. Main Effects
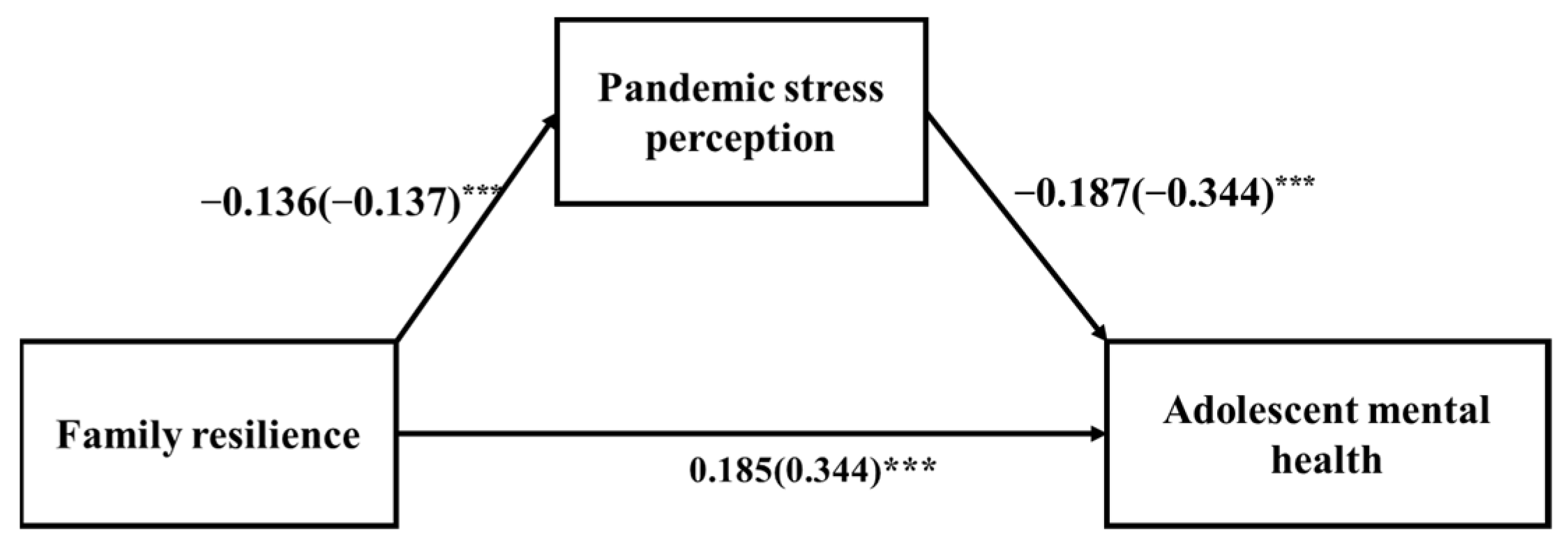
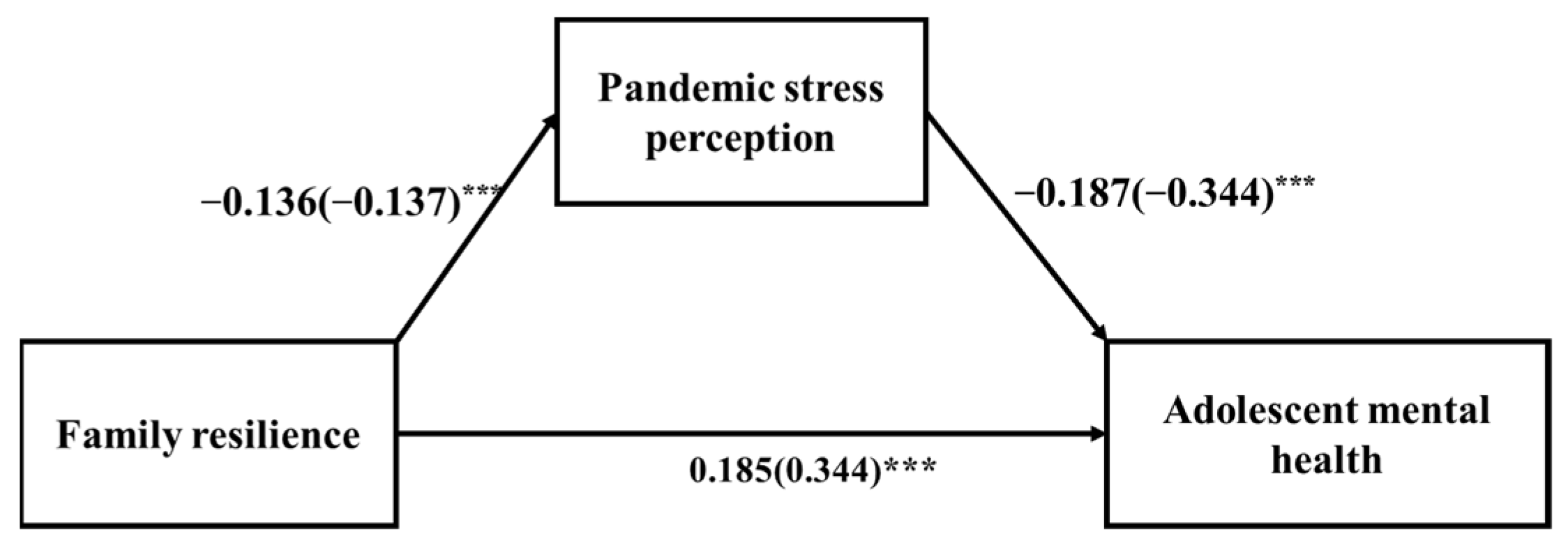
3.7. Mediation Effect
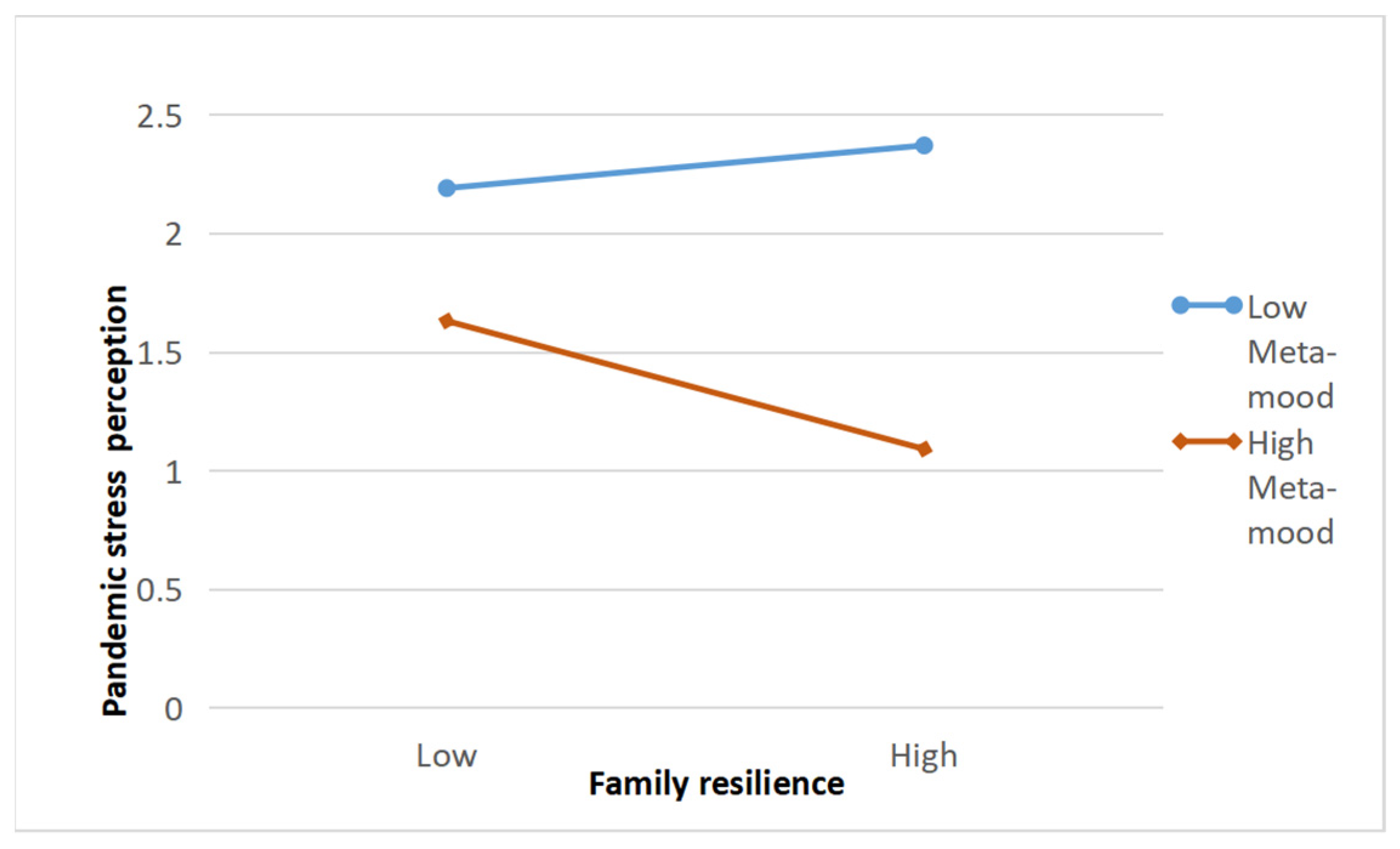
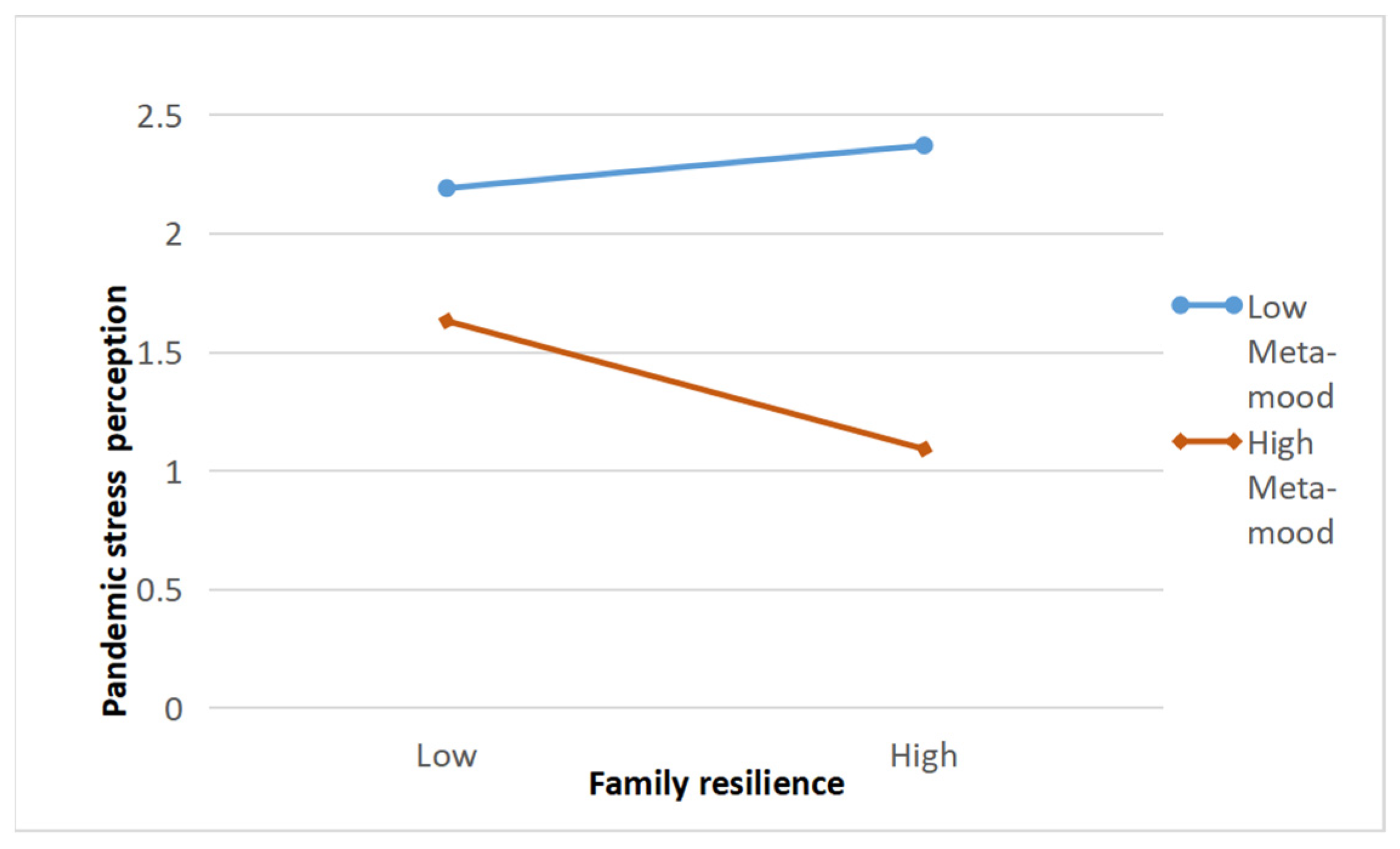
3.8. Moderated Mediation Effect
4. Discussion
4.1. Adolescent Mental Health and Pandemic Stress Perception during the Pandemic
4.2. The Impact of Family Resilience and Pandemic Stress Perception on Mental Health
4.3. The Mediation Role of Pandemic Stress Perception
4.4. The Moderation Role of Meta-Mood
4.5. Implications and Suggestions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cost, K.T.; Crosbie, J.; Anagnostou, E.; Birken, C.S.; Korczak, D.J. Mostly worse, occasionally better: Impact of COVID-19 pandemic on the mental health of Canadian children and adolescents. Eur. Child Adolesc. Psychiatry 2021, 1–14. [Google Scholar] [CrossRef]
- Neculicioiu, V.S.; Colosi, I.A.; Costache, C.; Sevastre-Berghian, A.; Clichici, S. Time to Sleep—A Review of the Impact of the COVID-19 Pandemic on Sleep and Mental Health. Int. J. Environ. Res. Public Health 2022, 19, 3497. Available online: https://www.mdpi.com/1660-4601/19/6/3497 (accessed on 4 March 2021). [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Ho, C. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Larsen, L.; Helland, M.S.; Holt, T. The impact of school closure and social isolation on children in vulnerable families during COVID-19: A focus on children’s reactions. Eur. Child Adolesc. Psychiatry 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Qian, Y. COVID-19 and Adolescent Mental Health in the United Kingdom. J. Adolesc. Health 2021, 69, 26–32. [Google Scholar] [CrossRef]
- Tian, F.; Li, H.; Tian, S.; Yang, J.; Tian, C. Psychological Symptoms of Ordinary Chinese Citizens Based on SCL-90 during the Level I Emergency Response to COVID-19. Psychiatry Res. 2020, 288, 112992. [Google Scholar] [CrossRef]
- Mbanuzuru, A.V.; Uwakwe, R.; Adogu, P.O.; Nnebue, C.C.; Udigwe, I.B.; Mbanuzuru, C.M. Depressive Disorders Among in School Adolescents. Orient J. Med. 2021, 33, 41–51. [Google Scholar]
- Jusienė, R.; Breidokienė, R.; Sabaliauskas, S.; Mieziene, B.; Emeljanovas, A. The Predictors of Psychological Well-Being in Lithuanian Adolescents after the Second Prolonged Lockdown Due to COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 3360. Available online: https://www.mdpi.com/1660-4601/19/6/3360 (accessed on 2 December 2020). [CrossRef]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.E. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl. Psychiatry 2020, 10, 291. [Google Scholar] [CrossRef]
- Gadermann, A.C.; Thomson, K.C.; Richardson, C.G.; Gagné, M.; Hirani, S.; Jenkins, E. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: Findings from a national cross-sectional study. BMJ Open 2021, 11, e042871. [Google Scholar] [CrossRef]
- Calvano, C.; Engelke, L.; Di Bella, J.; Kindermann, J.; Renneberg, B.; Winter, S.M. Families in the COVID-19 pandemic: Parental stress, parent mental health and the occurrence of adverse childhood experiences—results of a representative survey in Germany. Eur. Child Adolesc. Psychiatry 2021, 1–13. [Google Scholar] [CrossRef]
- Friborg, O.; Hjemdal, O.; Rosenvinge, J.H.; Martinussen, M.; Aslaksen, P.M.; Flaten, M.A. Resilience as a moderator of pain and stress. J. Psychosom. Res. 2006, 61, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Zhang, J.; Li, M.; Li, P.; Zhang, Y.; Zuo, X.; Xu, Y. Negative life events and mental health of Chinese medical students: The effect of resilience, personality and social support—ScienceDirect. Psychiatry Res. 2012, 196, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Juzhe, X.; Biao, S.; Biao, S. A review of resilience research. Chin. J. Health Psychol. 2002, 4, 314–317. [Google Scholar]
- Kerr, M.L.; Fanning, K.A.; Tuyen, H.; Inés, B.; Kim, C.N. Parents’ Self-Reported Psychological Impacts of COVID-19: Associations with Parental Burnout, Child Behavior, and Income. J. Pediatr. Psychol. 2021, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Conger, C.K.J. Resilience in Midwestern Families: Selected Findings from the First Decade of a Prospective, Longitudinal Study. J. Marriage Fam. 2010, 64, 361–373. [Google Scholar] [CrossRef]
- Walsh, F. Community-Based Practice Applications of a Family Resilience Framework; Springer: New York, NY, USA, 2013. [Google Scholar]
- Lee, I.; Lee, E.; Kim, H.S.; Park, Y.S.; Song, M.; Park, Y.H. Concept development of family resilience: A study of Korean families with a chronically ill child. J. Clin. Nurs. 2004, 13, 636–645. [Google Scholar] [CrossRef]
- Shin, S.H.; Choi, H.; Kim, M.J.; Kim, Y.H. Comparing adolescents’ adjustment and family resilience in divorced families depending on the types of primary caregiver. J. Clin. Nurs. 2010, 19, 1695–1706. [Google Scholar] [CrossRef]
- Gayatri, M.; Irawaty, D.K. Family Resilience during COVID-19 Pandemic: A Literature Review. Fam. J. 2021, 30, 132–138. [Google Scholar] [CrossRef]
- Xu, Y.; Lin, D. Family stress and adolescents’ depression, loneliness and happiness: The compensatory and moderating roles of family resilience. Psychol. Dev. Educ. 2015, 31, 594–602. [Google Scholar]
- Song, J.; Fogarty, K.; Suk, R.; Gillen, M. Behavioral and Mental Health Problems in Adolescents with ADHD: Exploring the Role of Family Resilience. J. Affect. Disord. 2021, 294, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Walsh, F. Loss and Resilience in the Time of COVID-19: Meaning Making, Hope, and Transcendence. Fam. Process 2020, 59, 898–911. [Google Scholar] [CrossRef] [PubMed]
- Brivio, E.; Guiddi, P.; Scotto, L.; Giudice, A.V.; Pravettoni, G. Patients Living with Breast Cancer During the Coronavirus Pandemic: The Role of Family Resilience, Coping Flexibility, and Locus of Control on Affective Responses. Front. Psychol. 2021, 11, 567230. [Google Scholar] [CrossRef] [PubMed]
- Walsh, F. Strengthening Family Resilience, 2nd ed.; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Sourani, A.T. Family Sense of Coherence and Family Adaptation. J. Marriage Fam. 1988, 50, 79–92. [Google Scholar]
- Tiet, Q.Q.; Bird, H.R.; Davies, M.; Hoven, C.; Cohen, P.; Jensen, P.S.; Goodman, S. Adverse life events and resilience. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure, & Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Beer, N.; Moneta, G.B. Coping and perceived stress as a function of positive Metacognitions and positive meta-emotions. Individ. Differ. Res. 2012, 10, 105–116. [Google Scholar]
- Guil, R.; Ruiz-González, P.; Merchán-Clavellino, A.; Morales-Sánchez, L.; Zayas, A.; Gómez-Molinero, R. Breast Cancer and Resilience: The Controversial Role of Perceived Emotional Intelligence. Front. Psychol. 2020, 11, 595713. [Google Scholar] [CrossRef]
- Rockhill, C.M.; Greener, S.H. Development of the Trait Meta-Mood Scale for Elementary School Children. In Poster Presented at the Biennial Meeting of the Society for Research in Child Development; U.S. Department of Education: Albuquerque, NM, USA, 1999. Available online: https://files.eric.ed.gov/fulltext/ED430688.pdf (accessed on 10 October 2020).
- Extremera, N.; Durán, A.; Rey, L. The moderating effect of trait meta-mood and perceived stress on life satisfaction. Personal. Individ. Differ. 2009, 47, 116–121. [Google Scholar] [CrossRef]
- Bu, T.; Liu, H. Development of fthe family resilience questionnaire. Psychol. Tech. Appl. 2019, 7, 173–182. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=XLJS201903006&DbName=CJFQ2019 (accessed on 9 May 2021).
- Wong, T.W.; Gao, Y.; Tam, W.W.S. Anxiety among university students during the SARS epidemic in Hong Kong. Stress Health 2007, 23, 31–35. Available online: https://onlinelibrary.wiley.com/doi/10.1002/smi.1116https://onlinelibrary.wiley.com/doi/full/10.1002/smi.1116 (accessed on 2 March 2021). [CrossRef]
- Jing, S.; Le, G. Structural equation modeling: Stressful life events, coping styles and emotional disorder of junior middle students. Chin. J. Clin. Psychol. 2004, 12, 256. [Google Scholar]
- McDowel, I. The General Health Questionnaire. In Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, L.P.; Nelson, D.L.; Barr, S.H. Person-environment fit and creativity: An examination of supply-value and demand-ability versions of fit. J. Manag. 1997, 23, 119–146. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Raw, J.; Waite, P.; Pearcey, S.; Creswell, C.; Patalay, P. Examining changes in parent-reported child and adolescent mental health throughout the UK’s first COVID-19 national lockdown. J. Child Psychol. Psychiatry 2021, 62, 1391–1401. [Google Scholar] [CrossRef]
- Friedman, R.S.; Rster, F.J. The effects of promotion and prevention cues on creativity. J. Personal. Soc. Psychol. 2001, 81, 1001–1013. [Google Scholar] [CrossRef]
- Chen, H. Analysis on the Difference of Teenagers’ Psychological Resilience in the Disaster Area of Southern Shaanxi after the May 12 Earthquake. China Electr. Educ. 2010, 166–167. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZGDI201030073&DbName=CJFQ2010 (accessed on 10 January 2021).
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [Green Version]
- Hafstad, G.S.; Augusti, E.M. A lost generation? COVID-19 and adolescent mental health. Lancet Psychiatry 2021, 8, 640–641. [Google Scholar] [CrossRef]
- Cui, C.A.; Li, S.; Wjc, B.; Tw, B. Mediating effects of coping styles on the relationship between family resilience and self-care status of adolescents with epilepsy transitioning to adult healthcare: A cross-sectional study in China. J. Pediatri. Nurs. 2022, 63, 143–150. [Google Scholar] [CrossRef]
- Guo, K.H.S.M. Family resilience and flourishment: Well-being among children with mental, emotional, and behavioral disorders. Res. Nurs. Health 2020, 43, 465–477. [Google Scholar] [CrossRef]
- Wang, S.; Shi, X.; Chen, X.; Zhu, Y.; Chen, H.; Fan, F. Earthquake Exposure and PTSD Symptoms among Disaster-Exposed Adolescents: A Moderated Mediation Model of Sleep Problems and Resilience. Front. Psychiatry 2021, 12, 577328. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.; Ye, B. Different Methods for Testing Moderated Mediation Models: Competitors or Backups? Acta Psychol. Sin. 2014, 46, 714–726. [Google Scholar] [CrossRef]
- Fa Rmer, R.F.; Sundberg, N.D. Buffering Hypothesis. In The Corsini Encyclopedia of Psychology; Weiner, I.B., Craighead, W.E., Eds.; John Wiley & Sons, Inc: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Coll, M.G.; Navarro-Mateu, D.; Giménez-Espert, M.D.C.; Prado-Gascó, V.J. Emotional Intelligence, Empathy, Self-Esteem, and Life Satisfaction in Spanish Adolescents: Regression vs. QCA Models. Front. Psychol. 2020, 11, 1629. [Google Scholar] [CrossRef]
- Salovey, P.; Stroud, L.R.; Woolery, A.; Epel, E.S. Perceived Emotional Intelligence, Stress Reactivity, and Symptom Reports: Further Explorations Using the Trait Meta-Mood Scale. Psychol. Health 2002, 17, 611–627. [Google Scholar] [CrossRef]
- Ghafoor, H.; Ahmad, R.A.; Nordbeck, P.; Ritter, O.; Pauli, P.; Schulz, S.M. A cross-cultural comparison of the roles of emotional intelligence, metacognition, and negative coping for health-related quality of life in German versus Pakistani patients with chronic heart failure. Br. J. Health Psychol. 2019, 24, 828–846. [Google Scholar] [CrossRef]
- Alconerocamarero, A.R.; Sarabiacobo, C.M.; Gonzálezgómez, S.; Ibáñezrementería, I.; Lavínalconero, L.; Sarabiacobo, A.B. Nursing students’ emotional intelligence, coping styles and learning satisfaction in clinically simulated palliative care scenarios: An observational study. Nurse Educ. Today 2018, 61, 94. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | Number | Percentage |
|---|---|---|---|
| Gender | Boy | 1244 | 46.2% |
| Girl | 1447 | 53.8% | |
| Grade | Year 7 | 765 | 28.4% |
| Year 8 | 534 | 19.8% | |
| Year 9 | 369 | 13.7% | |
| Year 10 | 69 | 2.6% | |
| Year 11 | 81 | 3.0% | |
| Year 12 | 873 | 32.5% | |
| Infection condition | Uninfected | 2633 | 97.8% |
| Infected | 58 | 2.2% |
| Good Mental Health | Poor Mental Health | χ2 | p | ||
|---|---|---|---|---|---|
| Junior | Number | 1139 | 529 | 93.34 | 0.00 |
| Percentage | 68.3% | 31.7% | |||
| Senior | Number | 564 | 459 | ||
| Percentage | 55.1% | 44.9% | |||
| Boy | Number | 768 | 476 | 2.38 | 0.12 |
| Percentage | 61.7% | 38.3% | |||
| Girl | Number | 935 | 512 | ||
| Percentage | 64.6% | 35.4% | |||
| Total | Number | 1703 | 988 | ||
| Percentage | 63.3% | 36.7% | |||
| N | Minimum Value | Maximum Value | M | SE | |
|---|---|---|---|---|---|
| Tenacity | 2691 | 1.00 | 5.00 | 4.26 | 0.90 |
| Harmony | 2691 | 1.00 | 5.00 | 4.35 | 0.90 |
| Openness | 2691 | 1.00 | 5.00 | 3.90 | 0.94 |
| Support | 2691 | 1.00 | 5.00 | 4.38 | 0.89 |
| Overall | 2691 | 1.00 | 5.00 | 4.23 | 0.82 |
| N | Minimum Value | Maximum Value | M | SE | |
|---|---|---|---|---|---|
| Emotion attention | 2691 | 1.90 | 5.00 | 3.49 | 0.54 |
| Emotion recognition | 2691 | 1.70 | 5.00 | 3.48 | 0.58 |
| Emotion recovery | 2691 | 1.00 | 5.00 | 3.90 | 0.76 |
| Overall score | 2691 | 1.92 | 5.00 | 3.58 | 0.52 |
| N | M | SD | t/F | p | ||
|---|---|---|---|---|---|---|
| Gender | Boy | 1244 | 2.89 | 0.43 | 0.006 | 0.995 |
| Girl | 1447 | 2.89 | 0.45 | |||
| School level | Junior high | 1668 | 2.80 | 0.44 | 8.73 *** | 0.000 |
| Senior high | 1023 | 2.95 | 0.43 | |||
| Graduating (non-graduating) | Non-graduating | 1449 | 2.93 | 0.43 | −4.53 *** | 0.000 |
| Graduating | 1242 | 2.86 | 0.45 | |||
| Grade | Year 7 | 765 | 2.99 | 0.18 | 37.49 *** | 0.000 |
| Year 8 | 534 | 2.92 | 0.43 | |||
| Year 9 | 369 | 2.90 | 0.47 | |||
| Year 10 | 69 | 2.55 | 0.28 | |||
| Year 11 | 81 | 2.67 | 0.37 | |||
| Year 12 | 873 | 2.83 | 0.43 | |||
| N | M | SD | t/F | p | ||
|---|---|---|---|---|---|---|
| Gender | Boy | 1244 | 2.07 | 0.83 | 0.56 | 0.57 |
| Girl | 1447 | 2.05 | 0.79 | |||
| School level | Junior high | 1668 | 1.84 | 0.74 | −0.11 *** | 0.000 |
| Senior high | 1023 | 2.59 | 0.98 | |||
| Graduating (non-graduating) | Non-graduating | 1449 | 2.21 | 0.78 | 9.28 *** | 0.000 |
| Graduating | 1242 | 1.93 | 0.81 | |||
| Grade | Year 7 | 765 | 1.82 | 0.75 | 75.11 *** | 0.000 |
| Year 8 | 534 | 1.89 | 0.76 | |||
| Year 9 | 369 | 1.82 | 0.71 | |||
| Year 10 | 69 | 2.99 | 0.94 | |||
| Year 11 | 81 | 2.27 | 0.92 | |||
| Year 12 | 873 | 2.38 | 0.75 | |||
| M | SD | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|---|
| Family resilience | 4.22 | 0.82 | 1 | |||
| Pandemic stress perception | 2.06 | 0.81 | −0.19 ** | 1 | ||
| Meta-mood | 3.50 | 0.520 | 0.58 ** | −0.28 ** | 1 | |
| Adolescent mental health | 2.89 | 0.44 | 0.41 ** | −0.41 ** | 0.61 ** | 1 |
| Value | R2 | B (SE) | β | p |
|---|---|---|---|---|
| Constant | 0.29 | 2.52(0.04) | 0.00 | |
| Year 8 | −0.04(0.02) | −0.04 ** | 0.02 | |
| Year 9 | −0.07(0.02) | −0.05 ** | 0.003 | |
| Year 10 | −0.06(0.04) | −0.02 | 0.201 | |
| Year 11 | −0.12(0.04) | −0.04 ** | 0.006 | |
| Year 12 | −0.01(0.01) | −0.01 | 0.535 | |
| Family resilience | 0.18(0.00) | 0.34 *** | 0.000 | |
| Pandemic stress perception | −0.18(0.01) | −0.34 *** | 0.000 |
| Effect | SE | p | 95% CIs | ||
|---|---|---|---|---|---|
| Lower CI | Upper CI | ||||
| Total effect | 0.211 | 0.01 | 0.000 | 0.192 | 0.229 |
| Direct effect | 0.185 | 0.01 | 0.000 | 0.167 | 0.203 |
| Indirect effect | 0.025 | 0.004 | 0.017 | 0.034 | |
| Standardized indirect effect | 0.047 | 0.008 | 0.032 | 0.062 | |
| Regression Equation | Fitting Index | Regression Coefficient | ||||
|---|---|---|---|---|---|---|
| Result Variable | Predictive Variable | R² | F | β | 95%CI | t |
| Pandemic Stress perception | Year 8 | 0.18 | 78.19 | 0.053 | [−0.02, 0.13] | 1.27 |
| Year 9 | −0.04 | [−0.13, 0.04] | −0.92 | |||
| Year 10 | 0.98 *** | [0.79, 1.16] | 10.44 | |||
| Year 11 | 0.29 *** | [0.12, 0.46] | 3.36 | |||
| Year 12 | 0.48 *** | [0.41, 0.55] | 13.18 | |||
| Family resilience | −0.09 *** | [−0.14, −0.04] | −3.43 | |||
| Meta mood | −0.28 *** | [−0.35, −0.21] | −8.12 | |||
| Family resilience × Meta-mood | −0.18 *** | [−0.25, −0.11] | −4.98 | |||
| Adolescent mental health | Year 8 | 0.29 | 157.91 | −0.04 *** | [−0.08, −0.00] | −2.29 |
| Year 9 | −0.07 *** | [−0.11, −0.02] | −3.00 | |||
| Year 10 | −0.06 | [−0.15, 0.03] | −1.27 | |||
| Year 11 | −0.12 *** | [−0.20, −0.03] | −2.72 | |||
| Year 12 | −0.01 | [−0.049, 0.02] | −0.62 | |||
| Family resilience | 0.18 *** | [0.16, 0.20] | 20.45 | |||
| Pandemic Stress perceived | −0.18 *** | [−0.20, −0.16] | −19.52 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhuo, R.; Yu, Y.; Shi, X. Family Resilience and Adolescent Mental Health during COVID-19: A Moderated Mediation Model. Int. J. Environ. Res. Public Health 2022, 19, 4801. https://doi.org/10.3390/ijerph19084801
Zhuo R, Yu Y, Shi X. Family Resilience and Adolescent Mental Health during COVID-19: A Moderated Mediation Model. International Journal of Environmental Research and Public Health. 2022; 19(8):4801. https://doi.org/10.3390/ijerph19084801
Chicago/Turabian StyleZhuo, Ran, Yanhua Yu, and Xiaoxue Shi. 2022. "Family Resilience and Adolescent Mental Health during COVID-19: A Moderated Mediation Model" International Journal of Environmental Research and Public Health 19, no. 8: 4801. https://doi.org/10.3390/ijerph19084801
APA StyleZhuo, R., Yu, Y., & Shi, X. (2022). Family Resilience and Adolescent Mental Health during COVID-19: A Moderated Mediation Model. International Journal of Environmental Research and Public Health, 19(8), 4801. https://doi.org/10.3390/ijerph19084801