The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers—A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
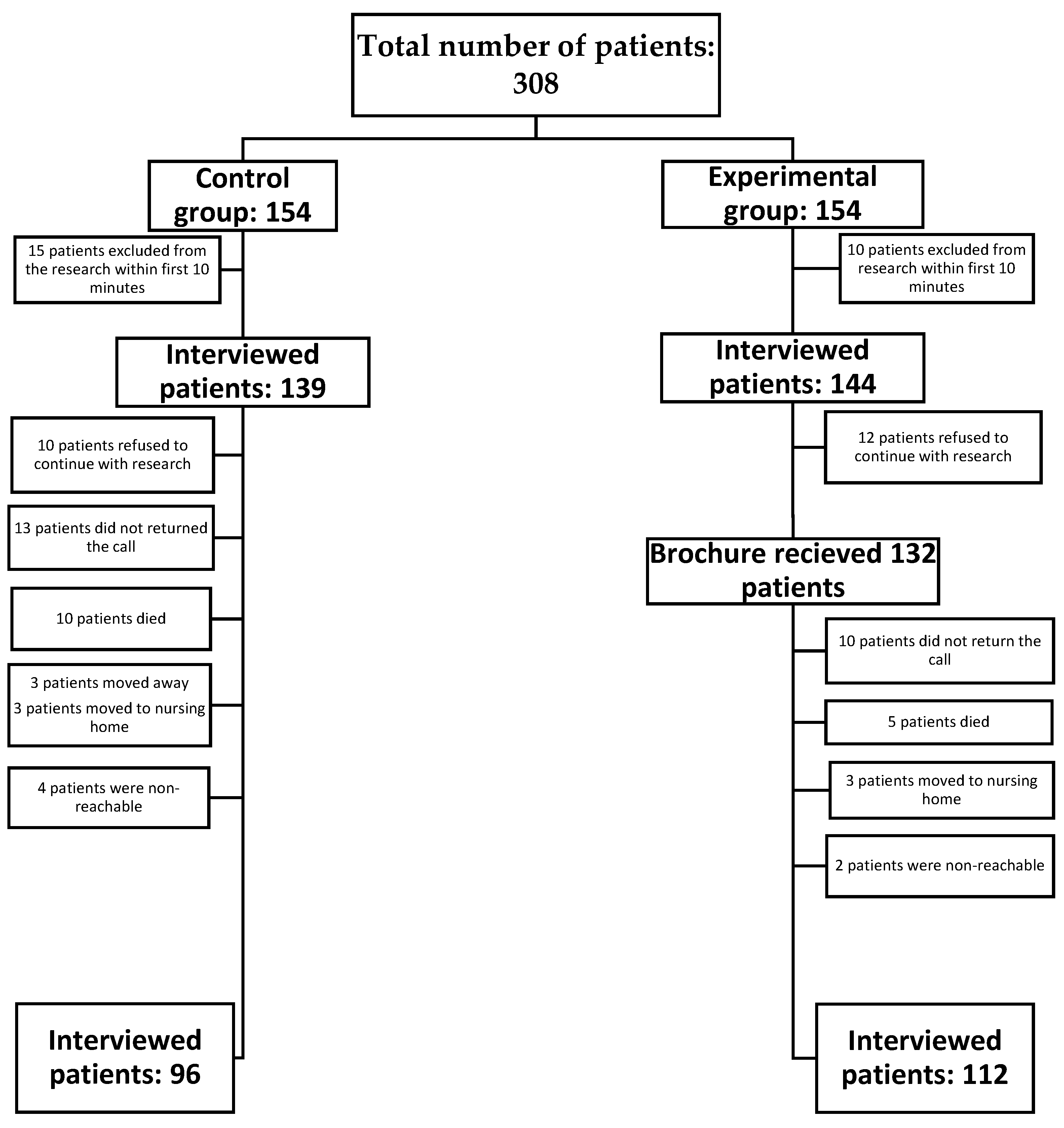
2.1. Study Design
2.2. Participants
2.3. Research Tool
2.3.1. Survey
- VLU duration and recurrence;
- attitude toward compression therapy and type and frequency of compression therapy used;
- knowledge of wound management and wound care.
2.3.2. Educational Intervention
2.3.3. Data Analysis
- a z-test for independent samples
- a t-test and a chi-square test to measure the statistical difference between two groups (i.e., self-treating versus not self-treating), effect size d = 0.250
- one-way ANOVA to test differences within one group with more than two variables (i.e., reasons for self-treatment), effect size d = 0.250
- Mann–Whitney test and pairwise comparison to determine the statistical significance of differences between groups, effect size d = 0.498
3. Results
- compression therapy: the measurement results showed a statistically significant shift, Wilks Lambda = 0.88, F (1.11) = 15.38, p < 0.001. There are, therefore, compelling reasons to conclude that the educational brochure influenced the knowledge of compression therapy. In one-way ANOVA, Wilks Lambda = 0.768, F(1.11) = 33.459, p < 0.001 participants showed statistically significant increase in awareness that compression therapy is necessary after VLU healing.
- positioning: participants intuitively know that keeping their legs horizontally will lower edema and swelling, so before educational intervention, theiy often that legs should be kept “on the bed”; after education, the answer “on the bed, above the heart level” was more often given, with statistically significant difference. This also include opinion about positive effect of walking on VLU healing.
- hand hygiene: before the intervention, 89% of participants answered that washing hands was obligatory; however, after the intervention all of the answers were correct so in one-way ANOVA Wilks Lambda 0.904, F(1.11) = 11.729, p < 0.05 making a statistically significant improvement.
- warning signs (Table 4)
- nutrition (Table 5)
- knowledge of effective VLU treatment (Table 6)
4. Discussion
- Hand Hygiene and Dressing Change
- Skin Care
- Physical Activity
- Nutrition
- Compression Therapy
- Patient Empowerment
- Study Limitation
- Strengths of the Study
- Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Considerations
References
- Harding, K.; Dowset, C.; Fias, L.; Jeines, R.; Mosti, G.; Olen, R.; Partch, H.; Reeder, S.; Senet, P.; Soriano, J.V.; et al. Consensus Recommendations Wounds International 2015. Available online: https://www.woundsinternational.com/ (accessed on 15 December 2021).
- Margolis, D.J.; Bilker, W.; Santanna, J.; Baumgarten, M. Venous leg ulcer: Incidence and prevalence in the elderly. J. Am. Acad. Dermatol. 2002, 46, 381–386. [Google Scholar] [CrossRef]
- Cardinal, M.; Eisenbud, D.; Phillips, T.; Harding, K. Early healing rates and wound area measurements are reliable predictors of later complete wound closure. Wound Repair Regen. 2008, 16, 19–22. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Weller, C.; Evans, S. Venous leg ulcer management in general practice—Practice nurses and evidence based guidelines. Aust. Fam. Physician 2012, 41, 331–333, 335–337. [Google Scholar]
- Ashby, R.; Gabe, R.; Ali, S.; Saramago, P.; Chuang, L.; Adderley, U.; Bland, J.; Cullum, N.; Dumville, J.; Iglesias, C.; et al. Venus IV (venous leg ulcer study IV)—Compression hosiery compared with compression bandaging in the treatment of venous leg ulcers: A randomised controlled trial, mixed-treatment comparison and decision-analytic model. Health Technol. Assess. 2014, 18, 1–293. [Google Scholar] [CrossRef]
- Franks, P.; Barker, J.; Collier, M.; Gethin, G.; Haesler, E.; Jawien, A.; Weller, C. Management of patients with venous leg ulcer: Challenges and current best practice. J. Wound Care 2016, 25 (Suppl. S6), S1–S67. [Google Scholar] [CrossRef]
- Kimmel, H.; Robin, A. An evidence-based algorithm for treating venous leg ulcers utilizing the cochrane database of systematic reviews. Wounds 2013, 25, 242–250. [Google Scholar]
- Kelechi, T.; Brunette, G.; Bonham, P.; Crestodina, L.; Droste, L.; Ratliff, C.; Varnado, M.F. 2019 guideline for management of wounds in patients with lower-extremity venous disease (LEVD). J. Wound Ostomy Cont. Nurs. 2020, 47, 97–110. [Google Scholar] [CrossRef]
- O’Donnell, T.F.; Passman, M.A.; Marston, W.A.; Ennis, W.J.; Dalsing, M.; Kistner, R.L.; Lurie, F.; Henke, P.K.; Gloviczki, M.L.; Eklöf, B.G.; et al. Management of venous leg ulcers: Clinical practice guidelines of the society for vascular surgery® and the american venous forum. J. Vasc. Surg. 2014, 60, 3S–59S. [Google Scholar] [CrossRef]
- World Health Organization. Self-Care in the Context of Primary Health Care; World Health Organization Regional Office for South-East Asia: Bangkok, Thailand, 2009. [Google Scholar]
- Bergsten, U.; Bergman, S.; Fridlund, B.; Arvidsson, A. “Delivering knowledge and advice”: Healthcare providers’ experiences of their interaction with patients’ management of rheumatoid arthritis. Int. J. Qual. Stud. Health Well-Being 2011, 6, 8473. [Google Scholar] [CrossRef]
- Auld, J.P.; Mudd, J.O.; Gelow, J.M.; Hiatt, S.O.; Lee, C.S. Self-care moderates the relationship between symptoms and health-related quality of life in heart failure. J. Cardiovasc. Nurs. 2018, 33, 217–224. [Google Scholar] [CrossRef]
- Buck, H.G.; Lee, C.S.; Moser, D.K.; Albert, N.M.; Lennie, T.; Bentley, B.; Worrall-Carter, L.; Riegel, B. Relationship between self-care and health-related quality of life in older adults with moderate to advanced heart failure. J. Cardiovasc. Nurs. 2012, 27, 8–15. [Google Scholar] [CrossRef]
- Lee, C.S.; Mudd, J.O.; Hiatt, S.O.; Gelow, J.M.; Chien, C.; Riegel, B. Trajectories of heart failure self-care management and changes in quality of life. Eur. J. Cardiovasc. Nurs. 2015, 14, 486–494. [Google Scholar] [CrossRef]
- Lee, C.; Bidwell, J.; Paturzo, M.; Alvaro, R.; Cocchieri, A.; Jaarsma, T.; Strömberg, A.; Riegel, B.; Vellone, E. Patterns of self-care and clinical events in a cohort of adults with heart failure: 1 year follow-up. Heart Lung 2018, 47, 40–46. [Google Scholar] [CrossRef]
- Xu, J.; Gallo, J.; Wenzel, J.; Nolan, M.; Budhathoki, C.; Abshire, M.; Bower, K.; Arruda, S.; Flowers, D.; Szanton, S.L.; et al. Heart failure rehospitalization and delayed decision making. J. Cardiovasc. Nurs. 2018, 33, 30–39. [Google Scholar] [CrossRef]
- Vellone, E.; Fida, R.; Ghezzi, V.; D’Agostino, F.; Biagioli, V.; Paturzo, M.; Strömberg, A.; Alvaro, R.; Jaarsma, T. Patterns of self-care in adults with heart failure and their associations with sociodemographic and clinical characteristics, quality of life, and hospitalizations. J. Cardiovasc. Nurs. 2017, 32, 180–189. [Google Scholar] [CrossRef]
- Kessing, D.; Denollet, J.; Widdershoven, J.; Kupper, N. Self-care and all-cause mortality in patients with chronic heart failure. JACC Heart Fail. 2016, 4, 176–183. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy mechanism in human agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Vellone, E. First steps toward a theory of caregiver contribution to self-care in heart failure. J. Cardiovasc. Nurs. 2017, 32, 584–586. [Google Scholar] [CrossRef]
- Al Mutair, A.; Al Shaer, A.; Al Ghamdi, F.; Al Ghamdi, A. The experiences of muslim family members of critically ill patients during end-of-life care in Saudi Arabia: A qualitative phenomenological study. Clin. Nurs. Res. 2018, 29, 375–381. [Google Scholar] [CrossRef]
- Chiao, C.; Wu, H.; Hsiao, C. Caregiver burden for informal caregivers of patients with dementia: A systematic review. Int. Nurs. Rev. 2015, 62, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Ma, S. Observations on the prevalence, characteristics, and effects of self-treatment. Front. Public Health 2016, 4, 69. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, H. Mother’s education and child health: Is there a nurturing effect? J. Health Econ. 2009, 28, 413–426. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Australia’s Health 2014; Australia’s Health Series No. 14. Cat. No. AUS 178; Australian Institute of Health and Welfare: Canberra, Australia, 2014.
- Dekkers, T.; Melles, M.; Groeneveld, B.; de Ridder, H. Web-based patient education in orthopedics: Systematic review. J. Med. Internet Res. 2018, 20, E143. [Google Scholar] [CrossRef]
- Conn, V.; Ruppar, T.; Maithe Enriquez, R.; Cooper, P. Patient-centered outcomes of medication adherence interventions: Systematic review and meta-analysis. Value Health 2016, 19, 277–285. [Google Scholar] [CrossRef]
- Woolley, A.; Hadjiconstantinou, M.; Davies, M.; Khunti, K.; Seidu, S. Online patient education interventions in type 2 diabetes or cardiovascular disease: A systematic review of systematic reviews. Prim. Care Diabetes 2019, 13, 16–27. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Žulec, M.; Rotar-Pavlič, D.; Puharić, Z.; Žulec, A. “Wounds home alone”—Why and how venous leg ulcer patients self-treat their ulcer: A qualitative content study. Int. J. Environ. Res. Public Health 2019, 16, 559. [Google Scholar] [CrossRef]
- Wilson, F.L.; Williams, B.N. Assessing the readability of skin care and pressure ulcer patient education materials. J. WOCN 2003, 30, 224–230. [Google Scholar]
- Zirwas, M.; Holder, J. Patient education strategies in dermatology part 2: Methods. J. Clin. Aesthet. Dermatol. 2009, 1, 28–34. [Google Scholar]
- Chen, Y.; Wang, Y.; Chen, W.; Smith, M.; Huang, H.; Huang, L. The effectiveness of a health education intervention on self-care of traumatic wounds. J. Clin. Nurs. 2012, 22, 2499–2508. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Lai, C. The effect of patient education with telephone follow-up on wound healing in adult patients with clean wounds. J. Wound Ostomy Cont. Nurs. 2014, 41, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Kuan, Y.; Wang, T.; Guo, C.; Tang, F.; Hou, I. Wound care knowledge, attitudes, and practices and mobile health technology use in the home environment: Cross-sectional survey of social network users. JMIR MHealth UHealth 2020, 8, E15678. [Google Scholar] [CrossRef] [PubMed]
- Visser, A.; Visagie, S. Pressure ulcer knowledge, beliefs and practices in a group of South Africans with spinal cord injury. Spinal Cord Ser. Cases 2019, 5, 83. [Google Scholar] [CrossRef]
- Guihan, M.; Bombardier, C. Potentially modifiable risk factors among veterans with spinal cord injury hospitalized for severe pressure ulcers: A descriptive study. J. Spinal Cord Med. 2012, 35, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Team, V.; Bouguettaya, A.; Richards, C.; Turnour, L.; Jones, A.; Teede, H.; Weller, C.D. Patient education materials on pressure injury prevention in hospitals and health services in Victoria, Australia: Availability and content analysis. Int. Wound J. 2019, 17, 370–379. [Google Scholar] [CrossRef]
- Dorresteijn, J.; Kriegsman, D.; Assendelft, W.; Valk, G. Patient education for preventing diabetic foot ulceration. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Goodall, R.; Ellauzi, J.; Tan, M.; Onida, S.; Davies, A.; Shalhoub, J. A systematic review of the impact of foot care education on self efficacy and self care in patients with diabetes. Eur. J. Vasc. Endovasc. Surg. 2020, 60, 282–292. [Google Scholar] [CrossRef]
- Shanley, E.; Moore, Z.; Patton, D.; O’Connor, T.; Nugent, L.; Budri, A.M.V.; Avsar, P. Patient education for preventing recurrence of venous leg ulcers: A systematic review. J. Wound Care 2020, 29, 79–91. [Google Scholar] [CrossRef]
- Gonzalez, A. The effect of a patient education intervention on knowledge and venous ulcer recurrence: Results of a prospective intervention and retrospective analysis. Ostomy Wound Manag. 2017, 63, 16–28. [Google Scholar]
- Weller, C.D.; Buchbinder, R.; Johnston, R.V. Interventions for helping people adhere to compression treatments for venous leg ulceration. Cochrane Database Syst. Rev. 2016, 3, CD008378. [Google Scholar] [CrossRef] [PubMed]
- Clarke Moloney, M.; Moore, A.A.O.; Burke, P.; McGee, H.; Grace, P. Information leaflets for venous leg ulcer patients: Are they effective? J. Wound Care 2005, 14, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Protz, K.; Dissemond, J.; Seifert, M.; Hintner, M.; Temme, B.; Verheyen-Cronau, I.; Augustin, M.; Otten, M. Education in people with venous leg ulcers based on a brochure about compression therapy: A quasi-randomised controlled trial. Int. Wound J. 2019, 16, 1252–1262. [Google Scholar] [CrossRef] [PubMed]
- Scholz, R.; Smith, B.; Adams, M.; Shah, M.; Brudner, C.; Datta, A.; Hirsch, E. A multifaceted surgical site infection prevention bundle for cesarean delivery. Am. J. Perinatol. 2019, 38, 690–697. [Google Scholar] [CrossRef] [PubMed]
- O’Kelly, S.; Moore, Z. Antenatal maternal education for improving postnatal perineal healing for women who have birthed in a hospital setting. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Jull, A.; Slark, J.; Parsons, J. Prescribed exercise with compression vs. compression alone in treating patients with venous leg ulcers. JAMA Dermatol. 2018, 154, 1304. [Google Scholar] [CrossRef]
- Smith, D.; Team, V.; Barber, G.; O’Brien, J.; Wynter, K.; McGinnes, R.; Tsiamis, E.; Weller, C.D. Factors associated with physical activity levels in people with venous leg ulcers: A multicentre, prospective, cohort study. Int. Wound J. 2017, 15, 291–296. [Google Scholar] [CrossRef]
- Barber, G.; Weller, C.; Gibson, S. Effects and associations of nutrition in patients with venous leg ulcers: A systematic review. J. Adv. Nurs. 2017, 74, 774–787. [Google Scholar] [CrossRef]
- Croatian Burreau of Statistics. Indicators of Poverty And Social Exclusion, 2015—Final Results; Croatian Burreau of Statistics: Zagreb, Croatia, 2015. [Google Scholar]
- Bobridge, A.; Sandison, S.; Paterson, J.; Puckridge, P.; Esplin, M. A pilot study of the development and implementation of a ‘best practice’ patient information booklet for patients with chronic venous insufficiency. Phlebol. J. Venous Disease. 2011, 26, 338–343. [Google Scholar] [CrossRef]
- Green, L.; Ratcliffe, D.; Masters, K.; Story, L. Educational intervention for nutrition education in patients attending an outpatient wound care clinic. J. Wound Ostomy Cont. Nurs. 2016, 43, 365–368. [Google Scholar] [CrossRef]
- Mosti, G.; Partsch, H. Bandages or double stockings for the initial therapy of venous oedema? A randomized, controlled pilot study. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Mosti, G.; Picerni, P.; Partsch, H. Compression stockings with moderate pressure are able to reduce chronic leg oedema. Phlebology 2012, 27, 289–296. [Google Scholar] [CrossRef]
- Mosti, G.; Mattaliano, V.; Partsch, H. Inelastic compression increases venous ejection fraction more than elastic bandages in patients with superficial venous reflux. Phlebology 2008, 23, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Aujoulat, W.; d’Hoore, A. Deccache patient empowerment in theory and practice: Polysemy or cacophony? Patient Educ. Couns. 2007, 66, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Bobbink, P.; Pugliese, M.; Larkin, P.; Probst, S. Nurse-led patient education for persons suf-fering from a venous leg ulcer in outpatient’s clinics and homecare settings: A scoping review. J. Tissue Viability 2020, 29, 297–309. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Group | Control Group | p Value | z Value | ||
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Gender | male | 51 (46) | 45 (47) | 0.037 | 0.86 |
| female | 61 (54) | 51 (53) | 0.846 | 0.14 | |
| Age | younger than 65 years | 39 (35) | 31 (32) | 0.148 | 0.46 |
| older than 65 years | 73 (65) | 65 (68) | 0.700 | 1.24 | |
| Employment status | employed | 10 (9) | 10 (10) | 0.315 | |
| retired | 88 (79) | 76 (79) | 0.853 | ||
| not employed | 14 (13) | 10 (10) | 0.68 | ||
| Housing | lives alone | 18 (16) | 17 (18) | 0.348 | 0.38 |
| lives with a spouse | 28 (25) | 23 (24) | 0.479 | 0.17 | |
| lives with a spouse and children | 52 (46) | 38 (40) | 0.87 | ||
| retirement home | 5 (5) | 3 (3) | 0.74 | ||
| living with relatives | 9 (8) | 15 (16) | 1.75 | ||
| Educational level | completed primary school or lower level of education | 62 (55) | 51 (53) | 0.142 | 0.29 |
| completed secondary school | 44 (39) | 39 (41) | 0.931 | 0.28 | |
| completed college or higher level of education | 6 (5) | 6 (6) | 0.31 | ||
| Residence | urban | 55 (49) | 48 (50) | 0.016 | 0.14 |
| rural | 57 (51) | 48 (50) | 0.14 |
| Control Group | Experimental Group | Wilks’s Lambda | F | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Statement | Measurement Point | M | SD | M | SD | |||
| Compression therapy reduces swelling | First | 3.24 | 0.86 | 3.27 | 0.96 | 0.972 | (1, 20) = 5.954 | <0.05 |
| Second | 3.26 | 0.87 | 3.80 | 1.07 | ||||
| Compression therapy doesn’t help at my wound | First | 2.49 | 1.20 | 2.62 | 1.11 | 0.972 | (1, 20) = 5.954 | <0.05 |
| Second | 3.97 | 1.16 | 3.07 | 1.52 | ||||
| When I’m resting, the best position for legs is … | First | 2.28 | 0.59 | 2.36 | 0.68 | 0.830 | (1, 20) = 42.263 | <0.001 |
| Second | 2.28 | 0.59 | 2.88 | 0.35 | ||||
| Before dressing change, I have to wash my hands | First | 1.05 | 0.27 | 1.15 | 0.47 | 0.975 | (1, 20) = 5.276 | <0.05 |
| Second | 1.02 | 0.14 | 1.00 | 0.00 | ||||
| When proceed dressing change, it is necessary to use gloves | First | 1.40 | 0.79 | 1.46 | 0.72 | 0.852 | (1, 20) = 35.561 | <0.001 |
| Second | 1.40 | 0.79 | 1.01 | 0.09 | ||||
| Number of pair of gloves | First | 0.80 | 0.55 | 0.71 | 0.59 | 0.928 | (1, 20) = 15.808 | <0.001 |
| Second | 0.84 | 0.60 | 1.01 | 0.09 | ||||
| When my ulcer heals, I still need to wear compression therapy | First | 1.80 | 0.96 | 1.81 | 0.85 | 0.887 | (1, 20) = 26.140 | <0.001 |
| Second | 1.78 | 0.94 | 1.25 | 0.53 | ||||
| Statement | Mean | D | SE Mean | Lower | Upper | t | df | p Value |
|---|---|---|---|---|---|---|---|---|
| Compression therapy reduces swelling | −0.53571 | 1.44527 | 0.13657 | −0.80633 | −0.2651 | −3.923 | 111 | <0.001 |
| Compression therapy does not help my ulcer | 0.33929 | 1.57431 | 0.14876 | 0.04451 | 0.63406 | 2.281 | 111 | 0.024 |
| The more I walk, the sooner my ulcer will heal | −0.3125 | 1.64416 | 0.15536 | −0.62035 | −0.00465 | −2.011 | 111 | 0.047 |
| The more I rest, the sooner my ulcer will heal | 0.39286 | 1.6998 | 0.16062 | 0.07459 | 0.71113 | 2.446 | 111 | 0.016 |
| When I’m resting, the best position for my legs is… | −0.52679 | 0.79367 | 0.07499 | −0.67539 | −0.37818 | −7.024 | 111 | <0.001 |
| Cream can be applied to the skin around the ulcer | 0.09821 | 1.41396 | 0.13361 | −0.16654 | 0.36296 | 0.735 | 111 | 0.464 |
| Before changing my dressing, it is necessary to wash my hands | 0.15179 | 0.46904 | 0.04432 | 0.06396 | 0.23961 | 3.425 | 111 | 0.243 |
| Before changing my dressings, it is necessary to disinfect my hands | 0.08036 | 0.72458 | 0.06847 | −0.05531 | 0.21603 | 1.174 | 111 | 0.243 |
| When my dressing is changed, it is necessary to wear gloves | 0.44643 | 0.73324 | 0.06928 | 0.30914 | 0.58372 | 6.443 | 111 | <0.001 |
| Even after my ulcer heals, I will still need to wear compression therapy | 0.5625 | 1.02914 | 0.09724 | 0.3698 | 0.7552 | 5.784 | 111 | <0.001 |
| I need to see a doctor or a nurse when … | ||||||||
| My ulcer smells unpleasant | 0.375 | 0.88149 | 0.08329 | 0.20995 | 0.54005 | 4.502 | 111 | <0.001 |
| My ulcer is bleeding | 0.38393 | 0.77396 | 0.07313 | 0.23901 | 0.52885 | 5.25 | 111 | <0.001 |
| My ulcer is leaking a lot | 0.45536 | 0.86876 | 0.08209 | 0.29269 | 0.61802 | 5.547 | 111 | <0.001 |
| The colour of my ulcer is turning yellow and green | 0.51786 | 0.84876 | 0.0802 | 0.35893 | 0.67678 | 6.457 | 111 | <0.001 |
| The area around my ulcer is painful | 0.48214 | 0.77089 | 0.07284 | 0.3378 | 0.62648 | 6.619 | 111 | <0.001 |
| The number of pair of gloves that should be used in a dressing changes | −0.29464 | 0.59485 | 0.05621 | −0.40602 | −0.18326 | −5.242 | 111 | <0.001 |
| Value | F | Hypothesis DF | Error DF | p | Partial Eta Squared | Noncent. Parameter | Observed Powerc | ||
|---|---|---|---|---|---|---|---|---|---|
| My ulcer smells unpleasant | Wilks′ Lambda | 0.846 | 20.27 0 | 1 | 111 | 0.000 | 0.154 | 20.270 | 0.994 |
| My ulcer is bleeding. | 0.801 | 27.56 0 | 1.000 | 111,000 | 0.000 | 0.199 | 27,560 | 0.999 | |
| My ulcer is leaking a lot. | 0.783 | 30.77 0 | 1.000 | 111,000 | 0.000 | 0.217 | 30,770 | 1.000 | |
| The color of my ulcer is turning yellow and green. | 0.727 | 41.69 3 | 1.000 | 111,000 | 0.000 | 0.273 | 41,693 | 1.000 | |
| the pain is higher | 0.717 | 43.81 1 | 1.000 | 111,000 | 0.000 | 0.283 | 43,811 | 1.000 |
| % | ||||
|---|---|---|---|---|
| First Measurement | Second Measurement | z Value | p Value | |
| Meat, fish and eggs | 40% | 64% | 2.56 | p < 0.050 |
| I dont know | 34% | 11% | 3.86 | p < 0.050 |
| Bread, pasta and potatoes | 18% | 24% | ||
| Fruits and vegetables | 7% | 10% | ||
| All of the above | 2% | 0% | ||
| % | ||||
|---|---|---|---|---|
| First Measurement | Second Measurement | z Value | p Value | |
| Dressing change | 38% | 10% | ||
| I dont know | 37% | 4% | 6.35 | p < 0.001 |
| Regular check ups | 6% | 8% | ||
| Resting | 4% | 1% | ||
| Activity | 4% | 9% | ||
| Dressing change | 4% | 55% | 9.04 | p < 0.001 |
| Compression therapy | 4% | 18% | 3.31 | p < 0.050 |
| Hygiene | 3% | 26% | 5 | p < 0.001 |
| Nutrition | 1% | 1% | ||
| Cream | 1% | |||
| Desinfictant | 1% | 2% | ||
| Painless treatment | 1% | |||
| Antibiotics | 3% | |||
| Ointment | 3% | |||
| Gloves | 2% | |||
| Medication | 2% | |||
| More frequent nurse visits | 1% | |||
| Infusion | 1% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Žulec, M.; Rotar Pavlič, D.; Žulec, A. The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers—A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 4657. https://doi.org/10.3390/ijerph19084657
Žulec M, Rotar Pavlič D, Žulec A. The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers—A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(8):4657. https://doi.org/10.3390/ijerph19084657
Chicago/Turabian StyleŽulec, Mirna, Danica Rotar Pavlič, and Ana Žulec. 2022. "The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers—A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 8: 4657. https://doi.org/10.3390/ijerph19084657
APA StyleŽulec, M., Rotar Pavlič, D., & Žulec, A. (2022). The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers—A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(8), 4657. https://doi.org/10.3390/ijerph19084657