
Subjective Response Measurement to Prosthesis or Device Use: Validation of the Prosthetic–Bionic Paradigm Questionnaire (PBP-Q)


 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
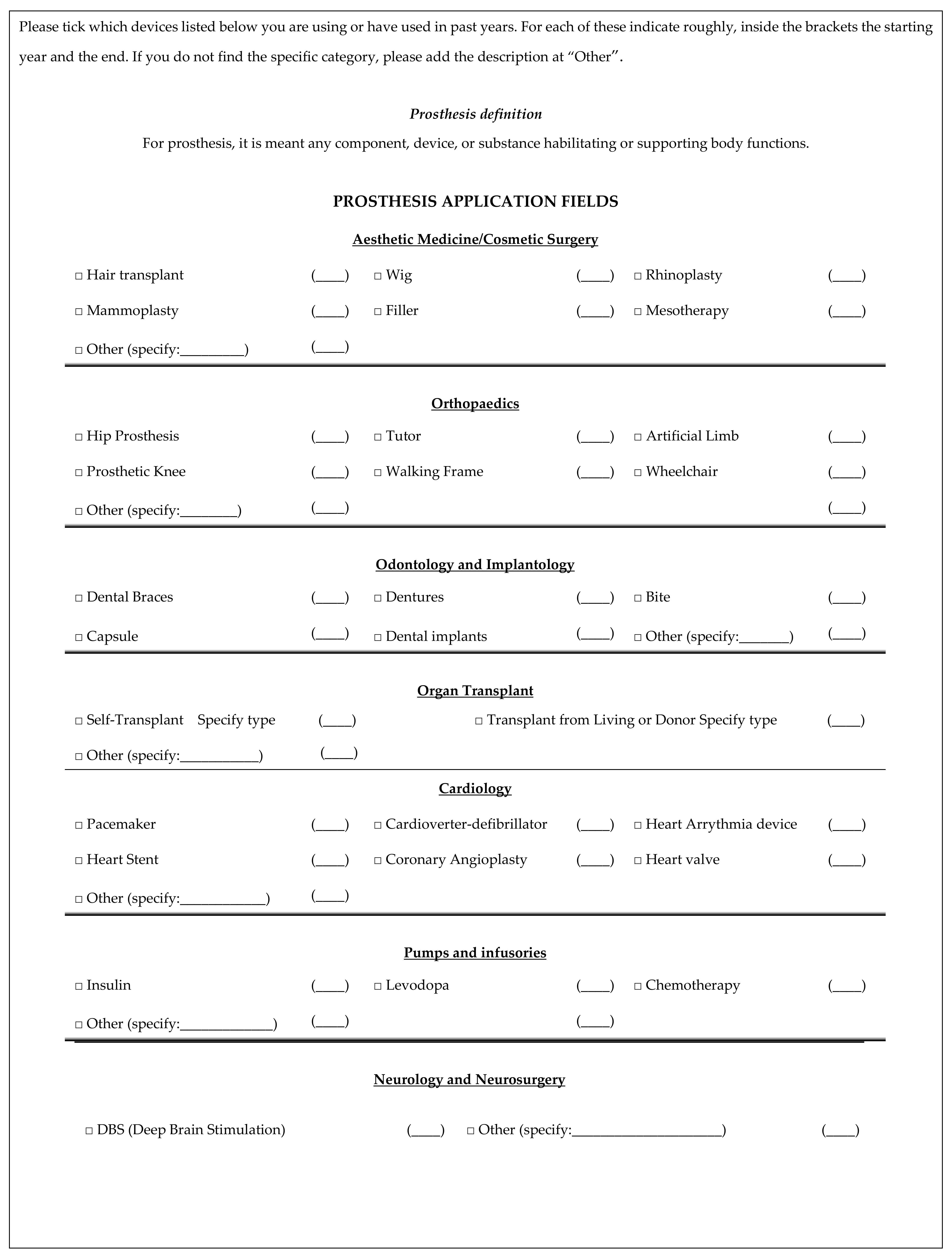
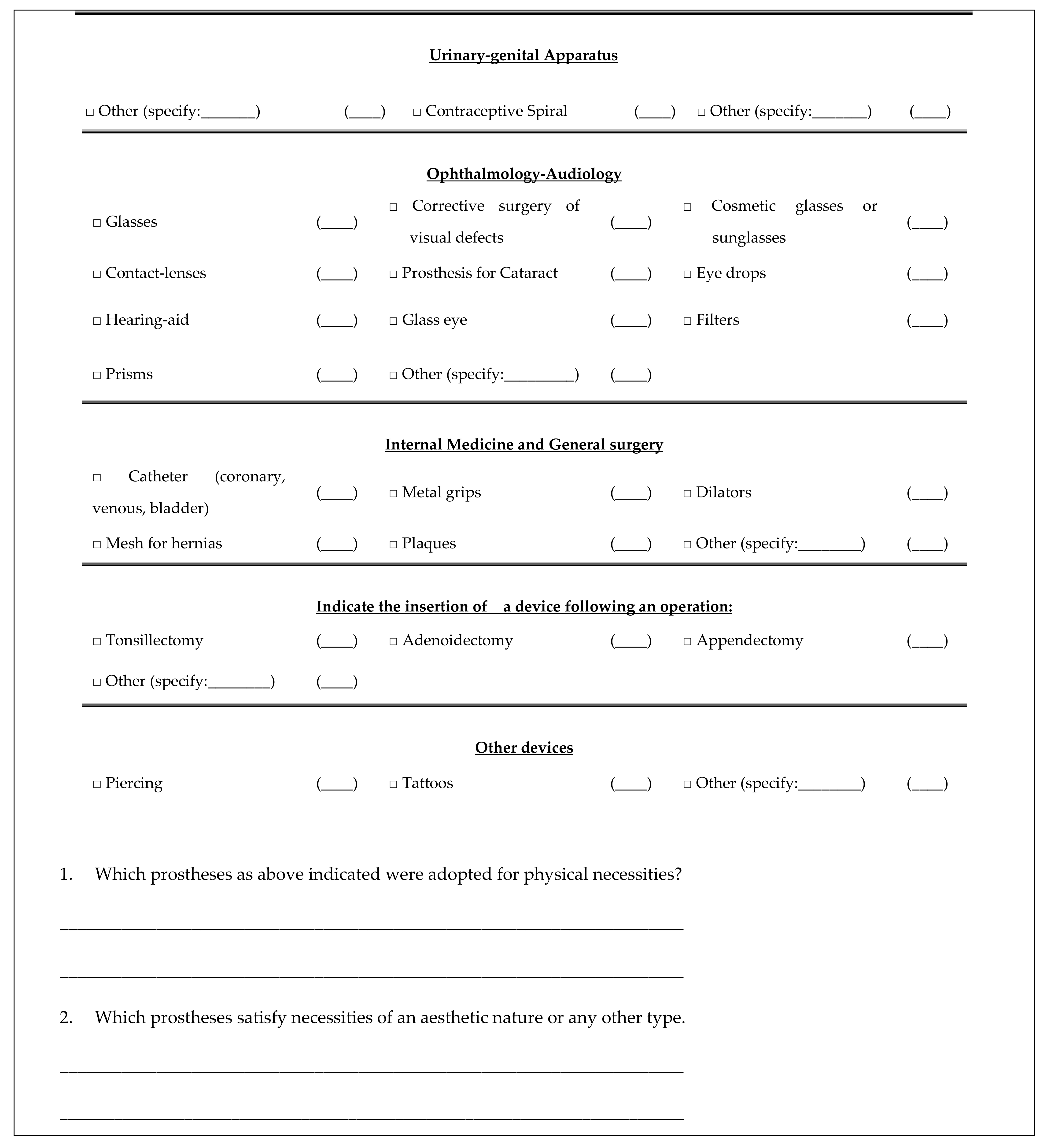
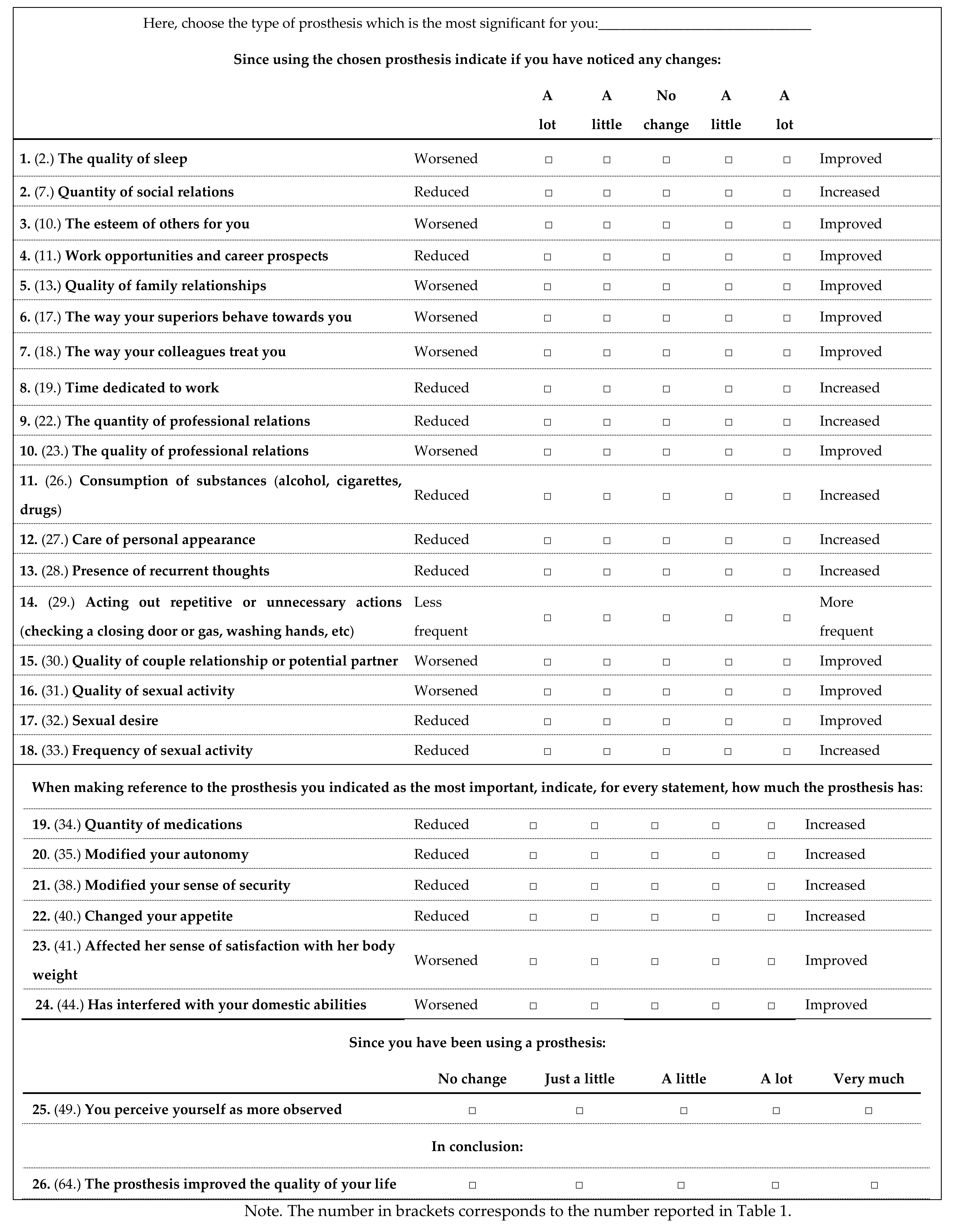
Appendix A. Prosthetic–Bionic Paradigm Questionnaire (PBP-Q)

References
- Udo, E.O.; van Hemel, N.M.; Zuithoff, N.P.; Nijboer, H.; Taks, W.; Doevendans, P.A.; Moons, K.G. Long term quality-of-life in patients with bradycardia pacemaker implantation. Int. J. Cardiol. 2013, 168, 2159–2163. [Google Scholar] [CrossRef] [Green Version]
- Silcox, H.; Rooks, M.; Vogel, R.R.; Fleming, L.L. Myoelectric prostheses. A long-term follow-up and a study of the use of alternate prostheses. J. Bone Jt. Surg. Am. 1993, 75, 1781–1789. [Google Scholar]
- Biddiss, E.; Chau, T. Upper-limb prosthetics: Critical factors in device abandonment. Am. J. Phys. Med. Rehabil. 2007, 86, 977–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, D.; Holloway, C.S.; Morgado Ramirez, D.Z.; Smitham, P.; Pappas, Y. What are user perspectives of exoskeleton thechnology? A litterature review. Int. J. Technol. Assess. Health Care 2017, 33, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Schüpbach, M.; Lohmann, E.; Anheim, M.; Lesage, S.; Czernecki, V.; Yaici, S.; Worbe, Y.; Charles, P.; Welter, M.L.; Pollak, P.; et al. Subthalamic nucleus stimulation is efficacious in patients with Parkinsonism and LRRK2 mutations. Mov. Disord. 2007, 22, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Liu, X.; Zhou, X.; Wang, H.; Zhou, W.; Jiang, J.; Peng, W.; Mo, L.; Tan, C.; Chen, L. Parkinson’s Disease-Related Risk of Suicide and Effect of Deep Brain Stimulation: Meta-Analysis. Parkinsons Dis. 2020, 2020, 8091963. [Google Scholar] [CrossRef]
- Murray, C.D. An interpretative phenomenological analysis of the embodiment of artificial limbs. Disabil. Rehabil. 2004, 26, 963–973. [Google Scholar] [CrossRef]
- Wijk, U.; Carlsson, I. Forearm amputees’ views of prosthesis use and sensory feedback. J. Hand Ther. 2015, 28, 269–277. [Google Scholar] [CrossRef]
- Bekrater-Bodmann, R. Perceptual correlates of successful body-prosthesis interaction in lower limb amputees: Psychometric characterisation and development of the Prosthesis Embodiment Scale. Sci. Rep. 2020, 26, 14203. [Google Scholar] [CrossRef]
- Hallas, C.; Banner, N.R.; Wray, J. A qualitative study of the psychological experience of patients during and after mechanical cardiac support. J. Cardiovasc. Nurs. 2009, 24, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Voltolini, A.; Minotti, A.; Verde, A.; Cipriani, M.; Garascia, A.; Turazza, F.; Macera, F.; Perna, E.; Russo, C.F.; Fumagalli, E.; et al. Psychological evaluation and support in patients with left ventricular assist devices: Preliminary data at 6-month follow-up. G. Ital. Cardiol. 2016, 17, 940–946. [Google Scholar]
- Dougherty, D.D. Deep Brain Stimulation: Clinical Applications. Psychiatr. Clin. N. Am. 2018, 41, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.; Desmond, D.; MacLachlan, M. Psychoprosthetics; Springer: London, UK, 2008; pp. 1–161. [Google Scholar]
- Murray, C.D.; Forshaw, M.J. The experience of amputation and prosthesis use for adults: A metasynthesis. Disabil. Rehabil. 2013, 35, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.D. Being like everybody else: The personal meanings of being a prosthesis user. Disabil. Rehabil. 2009, 31, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.; Buckmaster, A.; O’Carroll, S.; Kiernan, G.; Geraghty, J. Experiences in the provision, fitting and supply of external breast prostheses: Findings from a national survey. Eur. J. Cancer Care 2009, 18, 556–568. [Google Scholar] [CrossRef]
- Figueiredo, L.A.A.; Sampaio, A.A.; Souza, S.E.; Ferreira, F.J.R.; Buzzá, E.P.; Rizzatti-Barbosa, C.M. The Role of Prosthesis Spacer for Ocular Prostheses. J. Craniofac. Surg. 2017, 28, 360–363. [Google Scholar] [CrossRef]
- Mericske-Stern, R. Prosthetic considerations. Aust. Dent. J. 2008, 53 (Suppl. S1), 49–59. [Google Scholar] [CrossRef]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef] [Green Version]
- Maimon-Mor, R.O.; Makin, T.R. Is an artificial limb embodied as a hand? Brain decoding in prosthetic limb users. PLoS Biol. 2020, 18, e3000729. [Google Scholar] [CrossRef]
- Van Den Heiligenberg, F.M.Z.; Orlov, T.; MacDonald, S.N.; Duff, E.P.; Henderson Slater, D.; Beckmann, C.F.; Johansen-Berg, H.; Culham, J.C.; Makin, T.R. Artificial limb representation in amputees. Brain 2018, 141, 1422–1433. [Google Scholar] [CrossRef]
- de Vignemont, F. Mind the Body: An Exploration of Bodily Self-Awareness; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Ehrsson, H.H. Multisensory processes in body ownership. In Multisensory Perception: From Laboratory to Clinic; Sathian, K., Ramachandran, V.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 179–200. [Google Scholar]
- Pazzaglia, M.; Molinari, M. The embodiment of assistive devices-from wheelchair to exoskeleton. Phys. Life Rev. 2016, 16, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Berti, A.; Frassinetti, F. When far becomes near: Remapping of space by tool use. J. Cogn. Neurosci. 2000, 12, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, L.; Frassinetti, F.; Brozzoli, C.; Urquizar, C.; Roy, A.C.; Farnè, A. Tool-use induces morphological updating of the body schema. Curr. Biol. 2009, 19, 478–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iossa Fasano, A. Beside Oneself: From Freud to the Analysis of the Cyborg; Edizioni ETS: Pisa, Italy, 2013; pp. 1–152. [Google Scholar]
- Freud, S. The Ego and the Id. S.E., 19th ed.; Hogarth: London, UK, 1924. [Google Scholar]
- Freud, S. The Future of an Illusion. S.E., 21st ed.; Hogarth: London, UK, 1928. [Google Scholar]
- Iossa Fasano, A. Objects inside bodies. Redefining the posthuman. Atque 2016, 1, 133–154. [Google Scholar]
- Iossa Fasano, A. Psychoanalytic thinking on the phenomenon of bodily inflammation: Therapeutic method and clinical training. In How to Rejuvenate as You Age; Soresi, E., Garzia, P., Eds.; UTET: Torino, Italy, 2019. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2001. [Google Scholar]
- Bentler, P.M.; Bonnet, D.C. Significance Tests and Goodness of Fit in the Analysis of Covariance Structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: NewYork, NY, USA, 2015; pp. 1–534. [Google Scholar]
- Reeve, B.B.; Hays, R.; Bjorner, J.K.D.; Cook, K.F.; Crane, P.K.; Teresi, J.A.; Thissen, D.; Revicki, D.A.; Weiss, D.J.; Hambleton, R.K.; et al. Psychometric Evaluation and Calibration of Health-Related Quality of Life Item Banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45, 22–31. [Google Scholar] [CrossRef]


{kind=link}
| PBP-Q Item Change/Impact on… | PW | IR | PR | AS | ACO |
|---|---|---|---|---|---|
| 33. Frequency of sexual activity | 0.98 | ||||
| 31. Quality of sexual activity | 0.79 | ||||
| 32. Sexual desire | 0.78 | ||||
| 41. Satisfaction with weight | 0.65 | ||||
| 2. Quality of sleep | 0.35 | 0.32 | |||
| 13. Quality of family relationships | 0.82 | ||||
| 7. Quantity of social relations | 0.68 | ||||
| 30. Quality of couple relationship/potential partner | 0.62 | ||||
| 49. Perception of being more observed | 0.54 | ||||
| 27. Care of personal appearance | 0.41 | 0.33 | |||
| 40. Appetite | 0.39 | ||||
| 10. Esteem of others towards you | 0.38 | 0.32 | |||
| 17. The way your superiors behave towards you | 0.94 | ||||
| 18. The way your colleagues treat you | 0.83 | ||||
| 22. Quantity of professional relations | 0.60 | ||||
| 23. Quality of professional relations | 0.56 | ||||
| 11. Work opportunities and career prospects | 0.36 | 0.31 | |||
| 35. Autonomy | 0.75 | ||||
| 19. Time dedicated to work | 0.56 | ||||
| 38. Sense of security | 0.56 | ||||
| 44. Interference with domestic abilities | 0.54 | ||||
| 64. Improved quality of life thanks to the prosthesis | 0.39 | ||||
| 28. Recurrent thoughts | 0.74 | ||||
| 29. Acting out repetitive or unnecessary actions | 0.56 | ||||
| 26. Consumption of substances | 0.48 | ||||
| 34. Quantity of medications | 0.44 | ||||
| α (n = 118) | 0.82 | 0.70 | 0.84 | 0.71 | 0.55 |
| PBP-Q Scale | Num. Items | Min-Max | M(SD) |
|---|---|---|---|
| Psychological well-being | 5 | 5–25 | 14.57 (3.55) |
| Interpersonal relationships | 7 | 15–33 | 21.50 (3.76) |
| Professional relationships | 5 | 11–25 | 16.14 (2.64) |
| Autonomy and safety | 5 | 7–25 | 16.67 (3.48) |
| Addictions, compulsions, and obsessions | 4 | 7–19 | 12.38 (2.26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iossa Fasano, A.; Mandolillo, P.; Loscalzo, Y.; Giannini, M.; Grippo, G.; Imbimbo, I.; Lauro Grotto, R. Subjective Response Measurement to Prosthesis or Device Use: Validation of the Prosthetic–Bionic Paradigm Questionnaire (PBP-Q). Int. J. Environ. Res. Public Health 2022, 19, 4656. https://doi.org/10.3390/ijerph19084656
Iossa Fasano A, Mandolillo P, Loscalzo Y, Giannini M, Grippo G, Imbimbo I, Lauro Grotto R. Subjective Response Measurement to Prosthesis or Device Use: Validation of the Prosthetic–Bionic Paradigm Questionnaire (PBP-Q). International Journal of Environmental Research and Public Health. 2022; 19(8):4656. https://doi.org/10.3390/ijerph19084656
Chicago/Turabian StyleIossa Fasano, Augusto, Paolo Mandolillo, Yura Loscalzo, Marco Giannini, Gabriele Grippo, Isabella Imbimbo, and Rosapia Lauro Grotto. 2022. "Subjective Response Measurement to Prosthesis or Device Use: Validation of the Prosthetic–Bionic Paradigm Questionnaire (PBP-Q)" International Journal of Environmental Research and Public Health 19, no. 8: 4656. https://doi.org/10.3390/ijerph19084656
APA StyleIossa Fasano, A., Mandolillo, P., Loscalzo, Y., Giannini, M., Grippo, G., Imbimbo, I., & Lauro Grotto, R. (2022). Subjective Response Measurement to Prosthesis or Device Use: Validation of the Prosthetic–Bionic Paradigm Questionnaire (PBP-Q). International Journal of Environmental Research and Public Health, 19(8), 4656. https://doi.org/10.3390/ijerph19084656