
Attitudes of Patients with Chronic Diseases toward Management eHealth Applications Systems in Post-COVID-19 Times


Abstract
1. Introduction
2. Methods
2.1. Questionnaire Design
2.2. Sampling and Participants
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Survey Questionnaire
Appendix A.1. Part A: Demographics
- Name
- Gender
- Age
- Education
- Suffering with any chronic condition? Yes, No
- Are you currently using/used any eHealth application in the past? Yes/No
Appendix A.2. Part B: Survey Questions
- (1)
- In general, how would you rate your overall health?
- Excellent
- Very good
- Good
- Fair
- Poor
- (2)
- In the next 6 months, do you plan to take any of the following actions that would help your overall health?
- Install and use eHealth application for managing my condition (first-time)
- Continue to use existing eHealth application for managing my condition
- Do nothing
- (3)
- How confident are you that you can manage your own health?
- Very confident
- Somewhat confident
- Not too confident
- Not at all confident
- (4)
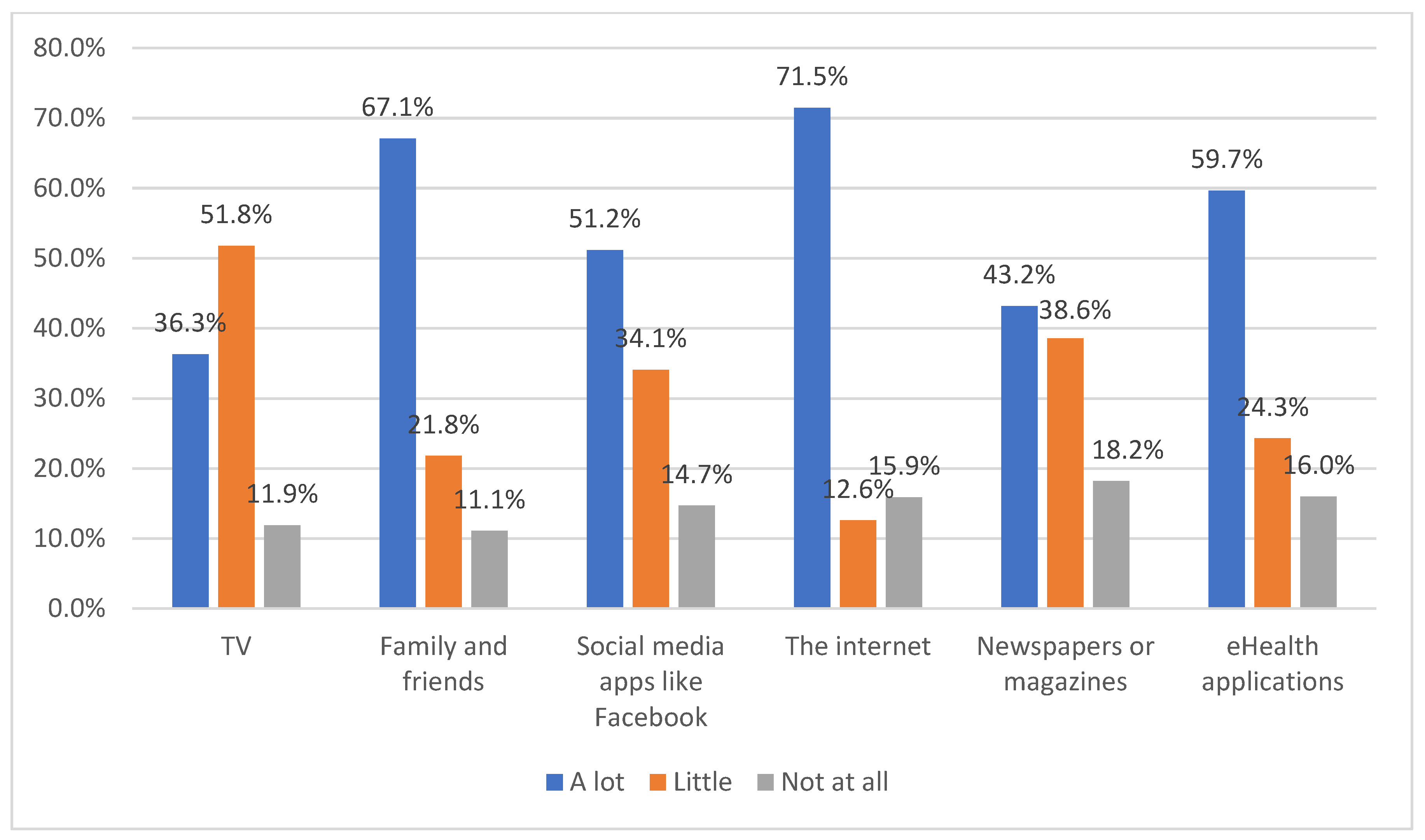
- Over the past year, how much information about health and health care did you get from: (Options: A lot, a little, none at all)
- TV
- Family and friends
- Social media apps like Facebook
- The internet
- Newspapers or magazines
- eHealth applications
- (5)
- Here are some statements about comfort with getting and using health information. Do you agree or disagree with each one? (Options: strongly disagree; disagree; neutral; agree; strongly agree)
- I know exactly what it is that I want to learn about my health
- I can figure out how and where to get health information I need
- I am satisfied with the way I currently learn about health
- I feel that I am in control over how and what I learn about health
- (6)
- Have you ever done any of these things online? (Mark all that apply)
- Searched online for information about a disease or medical problem
- Searched online for information about a doctor
- Typed information on an application about what you eat, how much you exercise, or your weight
- Typed information on an application about a chronic illness you have
- Renewed a prescription online
- consulted your doctor
- Used a personal health record
- Looked at a test result online
- Used a device that measures health information (like blood pressure; blood glucose levels) that connects to your mobile/website application
- Posted anything online about your health or health care
- Joined an online group that is for a health issue that you or your family member has
- Booked appointment with doctors
- (7)
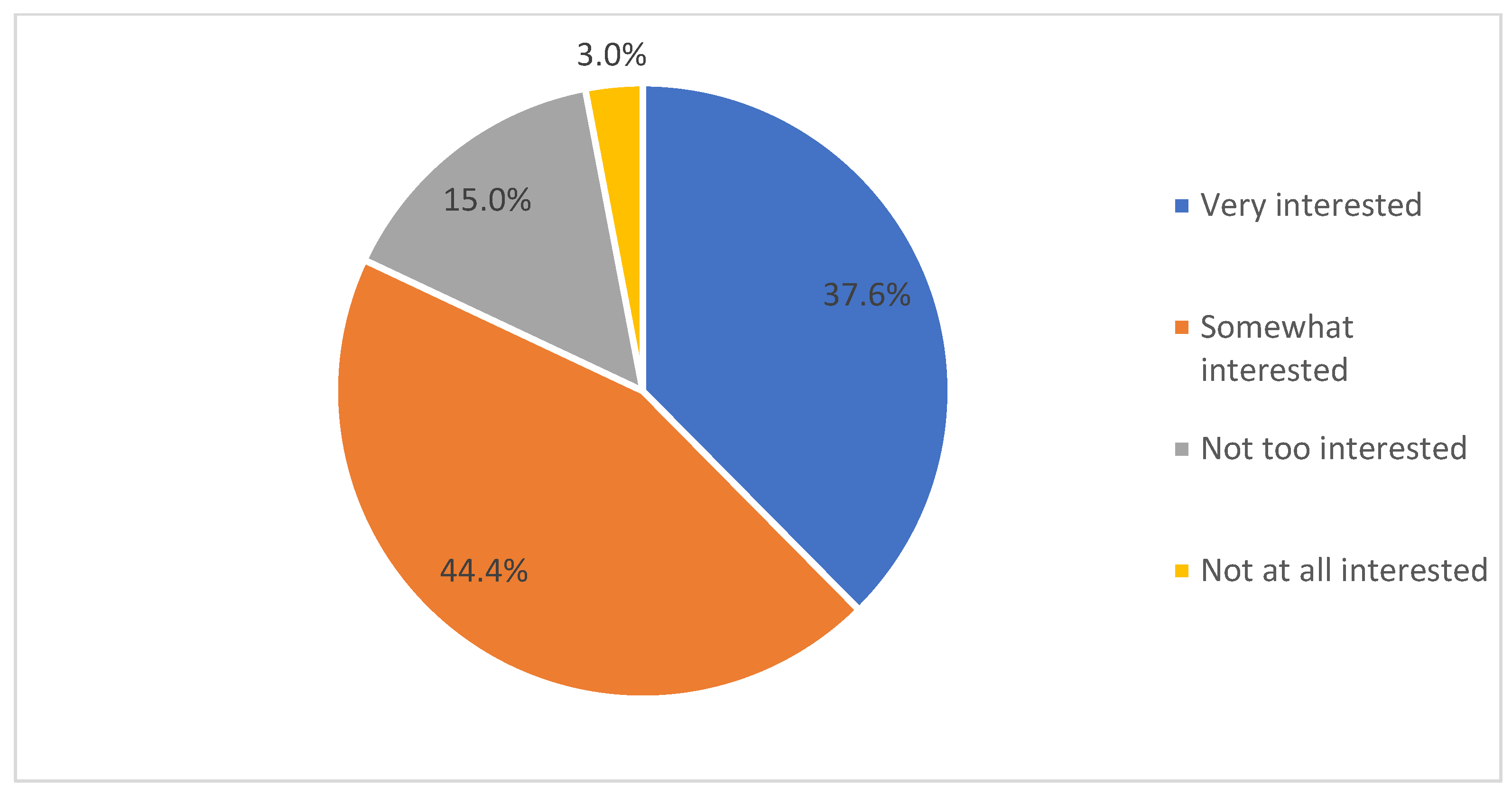
- How interested are you in using eHealth applications where you can get, keep, or update your health information?
- Very interested
- Somewhat interested
- Not too interested
- Not at all interested
- (8)
- There are applications that you can use to keep track of your health. Would you be interested in using a website to… (Mark all that apply)
- Track information about a chronic illness
- Track your diet and calories
- Track your exercise
- Remind you when to take prescriptions
- Remind you when you need tests
- Stay healthy
- Other
- (9)
- Please rate your acceptance on a scale of 5 (1: strongly reject; 2: reject; 3: neutral; 4: accept; 5: strongly accept) for the following activities using eHealth applications.
- Booking of appointments with physicians
- Access to laboratory test results
- Provision of educational resources
- Electronic renewal of prescriptions
- Personal repository of medical documentation
- Electronic diary for reporting symptoms
- Regular reporting of disease status to physician
- Contact with healthcare provider in case of disease exacerbation
- Online contact with healthcare professional (nurse or physician) on an as-needed basis
- Referral to physician
- Remote monitoring of physiological parameters
- (10)
- Many different groups have applications for people to get, keep, or update their health information. Would you be interested in using this type of website if it were from… (Mark all that apply)
- Your doctor
- The hospital you use
- Your health insurance plan
- A government group like Medicare
- Your employer
- A non-profit group like the American Cancer Society or AARP
- A company like Google or Apple
- (11)
- Here are some thoughts about using an application to get, keep, and update your health information. Do you agree or disagree with each one? (Options: strongly disagree; disagree; neutral; agree; strongly agree)
- I would be worried about the privacy of my health information if it were online (Mark all that apply)
- I don’t need this to handle my health needs
- I don’t like using computers/mobiles or the Internet
- It would take too much time
- This might cost too much
- I like to use, but depends on how easy to use the application
- I will use it anyway
- (12)
- In general, if your health information were online, how worried would you about the privacy and confidentiality of your information?
- Very worried
- Somewhat worried
- Not too worried
- Not at all worried
- (13)
- Please rate your frequency of using eHealth applications?
- many times a day
- at least once a day
- at least once a week
- at least once a month
- (14)
- Please tick the type of health service sought using eHealth applications
- Primary healthcare service (diagnosis, health advice and treatment)
- Specialized healthcare service (remote monitoring using wearables; treatment)
- health education/information
- (15)
- Effectiveness of using mobile phone for accessing healthcare
- Very effective
- effective
- not effective
- (16)
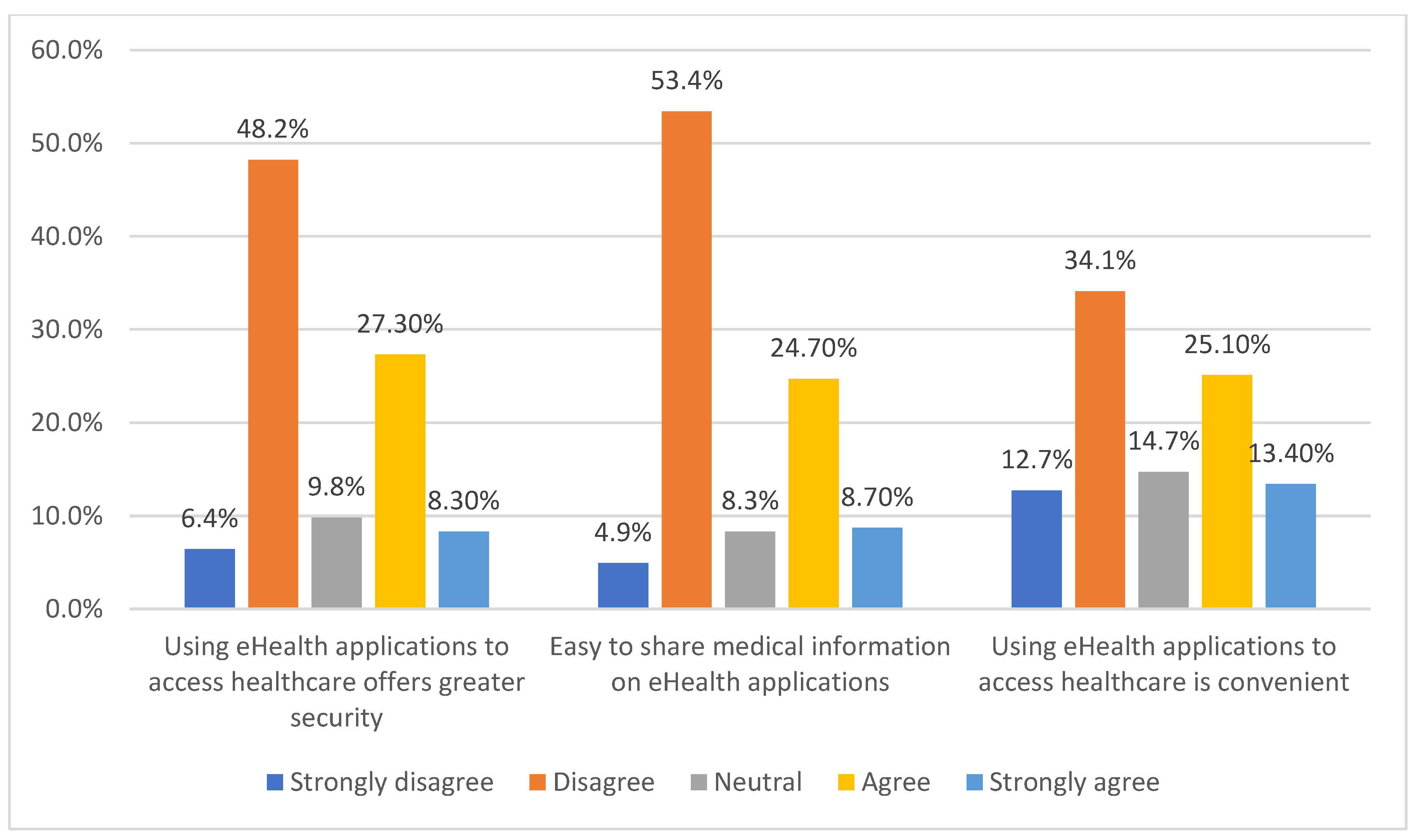
- Please rate the following items on a scale of 1-5 (1: strongly disagree; 2: disagree; 3: neutral; 4: agree; 5: strongly agree)
- Using eHealth applications to access healthcare offers greater security
- Easy to share medical information on eHealth applications
- Using eHealth applications to access healthcare is convenient
- (17)
- Please indicate the COVID-19 impact on your use and acceptance of eHealth applications? (Mark all that apply)
- Adopted eHealth applications out of necessity
- Adopted as no other services were available
- Adopted eHealth applications out of interest
- (18)
- Would you continue to use eHealth application after the pandemic ends?
- Very Probably
- Probably
- Possibly
- Probably Not
- Definitely Not
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Covid19.who.int. 2021. Available online: https://covid19.who.int/ (accessed on 16 December 2021).
- BBC. Covid: WHO Warns Europe Once Again at Epicentre of Pandemic. BBC News. 2021. Available online: https://www.bbc.com/news/world-europe-59160525 (accessed on 16 December 2021).
- World Health Organization. Saudi Arabia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Covid19.who.int. 2021. Available online: https://covid19.who.int/region/emro/country/sa (accessed on 16 December 2021).
- Alkhaldi, G.; Aljuraiban, G.S.; Alhurishi, S.; De Souza, R.; Lamahewa, K.; Lau, R.; Alshaikh, F. Perceptions towards COVID-19 and adoption of preventive measures among the public in Saudi Arabia: A cross sectional study. BMC Public Health 2021, 21, 1251. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. 2021. Available online: https://www.moh.gov.sa/en/Ministry/vro/Pages/Health-Transformation-Strategy.aspx (accessed on 16 December 2021).
- Alshammari, M. Electronic-health in Saudi Arabia: A review. Int. J. Adv. Appl. Sci. 2021, 8, 9942873. [Google Scholar] [CrossRef]
- Noor, A. The Utilization of E-Health in the Kingdom of Saudi Arabia. Int. Res. J. Eng. Technol. 2019, 6, 1229–1239. [Google Scholar]
- Alharbi, F. The Use of Digital Healthcare Platforms During the COVID-19 Pandemic: The Consumer Perspective. Acta Inform. Med. 2021, 29, 51. [Google Scholar] [CrossRef] [PubMed]
- Alhodaib, H.; Alanzi, T. Understanding the Impact of Digital Health Strategies During the COVID-19 Outbreak in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 4581–4594. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Yokota, F.; Sultana, N.; Ahmed, A. Factors Influencing Rural End-Users’ Acceptance of e-Health in Developing Countries: A Study on Portable Health Clinic in Bangladesh. Telemed. e-Health 2019, 25, 221–229. [Google Scholar] [CrossRef]
- Purwanto, E.; Budiman, V. Applying the Technology Acceptance Model to Investigate the Intention to Use E-health: A Conceptual Framework. Technol. Rep. Kansai Univ. 2020, 62, 2569–2580. [Google Scholar]
- Hayotte, M.; Thérouanne, P.; Gray, L.; Corrion, K.; D’Arripe-Longueville, F. The French eHealth Acceptability Scale Using the Unified Theory of Acceptance and Use of Technology 2 Model: Instrument Validation Study. J. Med. Internet. Res. 2020, 22, e16520. [Google Scholar] [CrossRef]
- Arfi, W.; Nasr, I.; Kondrateva, G.; Hikkerova, L. The role of trust in intention to use the IoT in eHealth: Application of the modified UTAUT in a consumer context. Technol. Forecast. Soc. Change 2021, 167, 120688. [Google Scholar] [CrossRef]
- Sahin, E.; Kefeli, U.; Cabuk, D.; Ozden, E.; Cakmak, Y.; Kaypak, M.A.; Seyyar, M.; Uygun, K. Perceptions and acceptance of telemedicine among medical oncologists before and during the COVID-19 pandemic in Turkey. Support. Care Cancer 2021, 29, 7497–7503. [Google Scholar] [CrossRef]
- Singh, A.; Ravi, P. Adoption of E-health platforms by medical practitioners: Mediating effect of attitude on E-health platforms usage. Health Mark. Q. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Klaver, N.S.; van de Klundert, J.; van den Broek, R.J.G.M.; Askari, M. Relationship Between Perceived Risks of Using mHealth Applications and the Intention to Use Them Among Older Adults in the Netherlands: Cross-sectional Study. JMIR Mhealth Uhealth 2021, 9, e26845. [Google Scholar] [CrossRef]
- Wang, J.; Fu, Y.; Lou, V.; Tan, S.; Chui, E. A systematic review of factors influencing attitudes towards and intention to use the long-distance caregiving technologies for older adults. Int. J. Med. Inform. 2021, 153, 104536. [Google Scholar] [CrossRef] [PubMed]
- Bondzie-Micah, V.; Qigui, S.; Arkorful, V.; Lugu, B.; Bentum-Micah, G.; Ayi-Bonte, A. Predicting consumer intention to use electronic health service: An empirical structural equation modeling approach. J. Public Aff. 2021, e2677. [Google Scholar] [CrossRef]
- Alsharif, A. Applying eHealth for Pandemic Management in Saudi Arabia in the Context of COVID-19: Survey Study and Framework Proposal. JMIR Med. Inform. 2020, 8, e19524. [Google Scholar] [CrossRef]
- Al Bar, A.; Hoque, M. Patient Acceptance of e-Health Services in Saudi Arabia: An Integrative Perspective. Telemed. e-Health 2019, 25, 847–852. [Google Scholar] [CrossRef]
- Thapa, S.; Nielsen, J.B.; Aldahmash, A.M.; Qadri, F.R.; Leppin, A. Willingness to Use Digital Health Tools in Patient Care Among Health Care Professionals and Students at a University Hospital in Saudi Arabia: Quantitative Cross-sectional Survey. JMIR Med. Educ. 2021, 7, e18590. [Google Scholar] [CrossRef]
- Chikhaoui, E.; Sarabdeen, J.; Parveen, R. Privacy and Security Issues in the Use of Clouds in e-Health in the Kingdom of Saudi Arabia. Commun. IBIMA 2017, 2017, 369309. [Google Scholar] [CrossRef][Green Version]
- Alsswey, A.; Al-Samarraie, H.; Bervell, B. mHealth technology utilization in the Arab world: A systematic review of systems, usage, and challenges. Health Technol. 2021, 11, 895–907. [Google Scholar] [CrossRef]
- Alanezi, F. Factors affecting the adoption of e-health system in the Kingdom of Saudi Arabia. Int. Health 2020, 13, 456–470. [Google Scholar] [CrossRef]
- Chandran, D.; Aljohani, N. The Role of Cultural Factors on Mobile Health Adoption: The Case of Saudi Arabia. AMCIS 2020 Proc. 3. Available online: https://aisel.aisnet.org/amcis2020/culture_in_is/culture_in_is/3 (accessed on 24 March 2022).
- Statista. eHealth-Saudi Arabia|Statista Market Forecast. 2021. Available online: https://www.statista.com/outlook/dmo/digital-health/ehealth/saudi-arabia#global-comparison (accessed on 16 December 2021).
- Alshahrani, A.; Stewart, D.; MacLure, K. A systematic review of the adoption and acceptance of eHealth in Saudi Arabia: Views of multiple stakeholders. Int. J. Med. Inform. 2019, 128, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Shati, A. Mhealth Applications Developed by The Ministry of Health for Public Users in Ksa: A Persuasive Systems Design Evaluation. Health Inform. Int. J. 2020, 9, 1–14. [Google Scholar] [CrossRef]
- Alharbi, A.; Alzuwaed, J.; Qasem, H. Evaluation of e-health (Seha) application: A cross-sectional study in Saudi Arabia. BMC Med. Inform. Decis. Mak. 2021, 21, 103. [Google Scholar] [CrossRef] [PubMed]
- Algumzi, A. Evolving factors influencing consumers’ attitudes towards the use of eHealth applications: Implications on the future of Neom. Int. Health 2021, 14, 152–160. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Sedgwick, P. Convenience sampling. BMJ 2013, 347, f6304. [Google Scholar] [CrossRef]
- Cochran, W.G. Sampling Techniques, 2nd ed.; John Wiley and Sons, Inc.: New York, NY, USA, 1963. [Google Scholar]
- Alduraywish, S.; Altamimi, L.; Aldhuwayhi, R.; AlZamil, L.; Alzeghayer, L.; Alsaleh, F.; Aldakheel, F.M.; Tharkar, S. Sources of Health Information and Their Impacts on Medical Knowledge Perception Among the Saudi Arabian Population: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e14414. [Google Scholar] [CrossRef]
- Abdulaziz, A.; Ronald, R. Factors Affecting Electronic Health Record Adoption in Developing Countries: A Case of Saudi Arabia. AMCIS 2020 Proc. 2020, 33, 1–15. [Google Scholar]
- Alsahafi, Y.; Gay, V.; Khwaji, A. Factors affecting the acceptance of integrated electronic personal health records in Saudi Arabia: The impact of e-health literacy. Health Inf. Manag. J. 2022, 51, 98–109. [Google Scholar] [CrossRef]
- Al-Anezi, F.M. Evaluating the Readiness of Mobile Technology with Respect to e-Heath for Medication in Saudi Arabia: An Integrative Perspective. J. Multidiscip. Healthc. 2021, 14, 59–66. [Google Scholar] [CrossRef]
- Alsulame, K.; Khalifa, M.; Househ, M. eHealth in Saudi Arabia: Current Trends, Challenges and Recommendations. Stud. Health Technol. Inform. 2015, 213, 233–236. [Google Scholar] [PubMed]
- Jonker, L.; Haveman, M.; de Bock, G.; van Leeuwen, B.; Lahr, M. Feasibility of Perioperative eHealth Interventions for Older Surgical Patients: A Systematic Review. J. Am. Med. Dir. Assoc. 2020, 21, 1844–1851.e2. [Google Scholar] [CrossRef] [PubMed]
- Wildenbos, G.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | N | Relative Frequency |
|---|---|---|
| Gender | ||
| Male | 125 | 53.4% |
| Female | 109 | 46.6% |
| Education | ||
| High School/Diploma | 58 | 24.8% |
| Bachelor’s degree | 131 | 55.9% |
| Master’s degree | 27 | 11.5% |
| Doctorate | 18 | 7.7% |
| Age (years) | ||
| 18–24 | 129 | 55.1% |
| 25–34 | 35 | 14.9% |
| 35–44 | 45 | 19.2% |
| 45–54 | 16 | 6.8% |
| ≥55 | 9 | 3.8% |
| Online Activities | Frequency |
|---|---|
| Searched online for information about a disease or medical problem | 64.2% |
| Searched online for information about a doctor | 28.7% |
| Typed information on an application about what you eat, how much you exercise, or your weight | 38.7% |
| Typed information on an application about a chronic illness you have | 37.2% |
| Renewed a prescription online | 57.6% |
| Consulted your doctor | 63.5% |
| Used a personal health record | 29.4% |
| Looked at a test result online | 54.1% |
| Used a device that measures health information (like blood pressure; blood glucose levels) that connects to your mobile/website application | 56.3% |
| Posted anything online about your health or health care | 49.9% |
| Joined an online group that is for a health issue that you or your family member has | 34.6% |
| Booked appointment with doctors | 53.8% |
| Activities | Mean |
|---|---|
| Booking of appointments with physicians | 4.34 |
| Access to laboratory test results | 4.25 |
| Provision of educational resources | 4.21 |
| Electronic renewal of prescriptions | 4.21 |
| Personal repository of medical documentation | 4.22 |
| Regular reporting of disease status to physician | 4.23 |
| Contact with healthcare provider in case of disease exacerbation | 4.26 |
| Online contact with healthcare professional (nurse or physician) on an as-needed basis | 4.19 |
| Referral to physician | 4.30 |
| N | Mean | Standard Deviation | df | T-Value | p-Value | |
|---|---|---|---|---|---|---|
| By gender | ||||||
| Male | 125 | 2.4 | 3.14 | 232 | 0.7782 | 0.4372 |
| Female | 109 | 2.65 | 1.26 | |||
| By age | ||||||
| <35 years | 164 | 2.55 | 1.68 | 232 | 0.1501 | 0.8808 |
| ≥35 years | 70 | 2.5 | 3.41 | |||
| N | Mean | Standard Deviation | df | T-Value | p-Value | |
|---|---|---|---|---|---|---|
| By gender | ||||||
| Male | 125 | 2.04 | 0.43 | 232 | 2.4458 | 0.0152 (p < 0.05) * |
| Female | 109 | 1.84 | 0.79 | |||
| By age | ||||||
| <35 years | 164 | 1.99 | 0.38 | 232 | 2.0230 | 0.0442 (p < 0.05) * |
| ≥35 years | 70 | 1.85 | 0.67 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
ALsharif, A.H. Attitudes of Patients with Chronic Diseases toward Management eHealth Applications Systems in Post-COVID-19 Times. Int. J. Environ. Res. Public Health 2022, 19, 4289. https://doi.org/10.3390/ijerph19074289
ALsharif AH. Attitudes of Patients with Chronic Diseases toward Management eHealth Applications Systems in Post-COVID-19 Times. International Journal of Environmental Research and Public Health. 2022; 19(7):4289. https://doi.org/10.3390/ijerph19074289
Chicago/Turabian StyleALsharif, Abdullah H. 2022. "Attitudes of Patients with Chronic Diseases toward Management eHealth Applications Systems in Post-COVID-19 Times" International Journal of Environmental Research and Public Health 19, no. 7: 4289. https://doi.org/10.3390/ijerph19074289
APA StyleALsharif, A. H. (2022). Attitudes of Patients with Chronic Diseases toward Management eHealth Applications Systems in Post-COVID-19 Times. International Journal of Environmental Research and Public Health, 19(7), 4289. https://doi.org/10.3390/ijerph19074289