
Low Use of Long-Acting Reversible Contraceptives in Tanzania: Evidence from the Tanzania Demographic and Health Survey

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Prevalence, Sociodemographic, Household, and Obstetric Characteristics with the Utilization of Long-Acting Family Planning (LARC)
3.2. Factors Associated with Utilization of Long-Acting Family Planning (LARC)
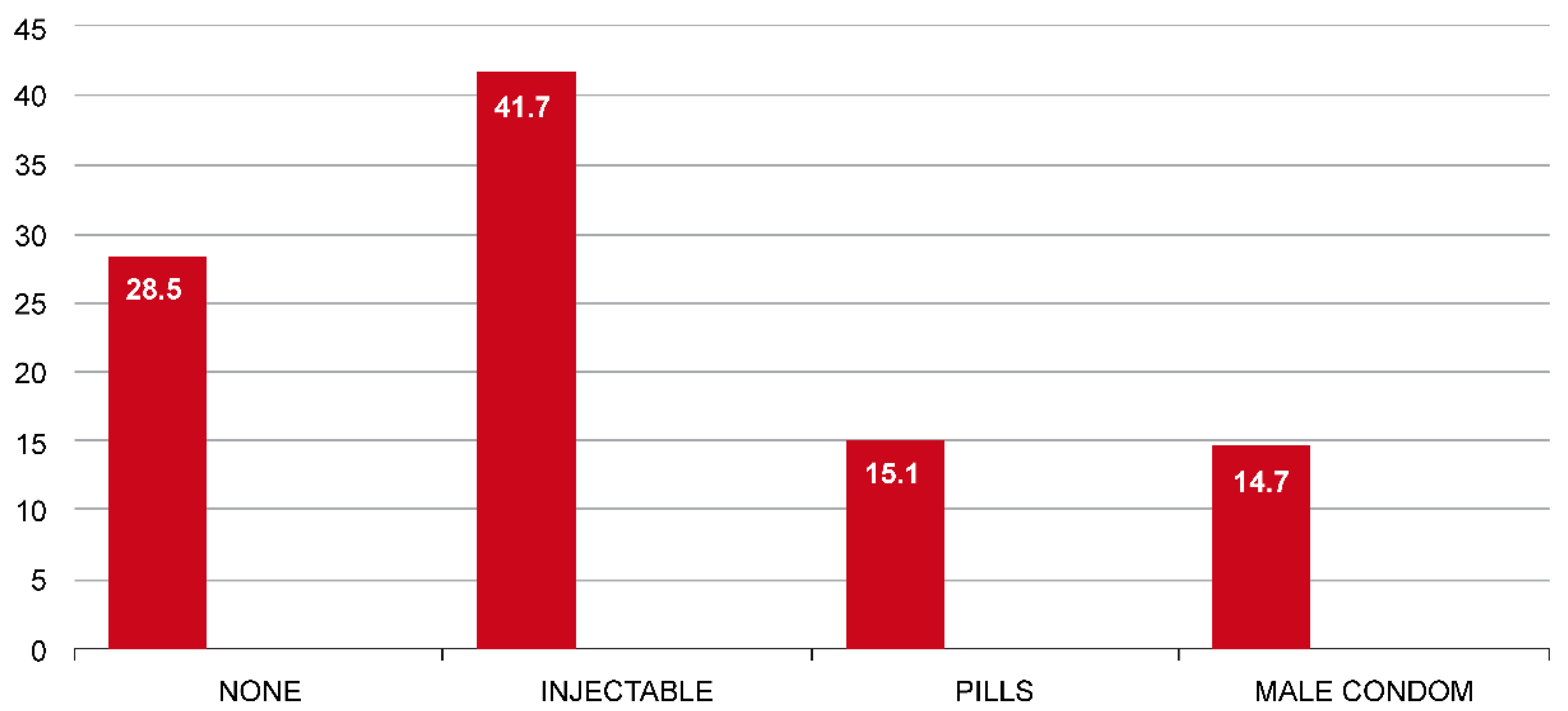
3.3. Current Contraceptive Methods
4. Discussion
Strength, Limitation and Recommend of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hubacher, D.; Trussell, J. A definition of modern contraceptive methods. Contraception 2015, 92, 420–421. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Department of Reproductive Health and Research (WHO/RHR) and Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs (CCP). Knowledge for Health Project. In Family Planning: A Global Handbook for Providers; CCP: Baltimore, MD, USA; WHO: Geneva, Switzerland, 2018.
- Farah, D.; de Moraes Andrade, T.R.; Sansone, D.; Batista Castello Girão, M.J.; Fonseca, M.C.M. A Cost Effectiveness Model of Long-Acting Reversible Contraceptive Methods in the Brazilian National Health System. Am. J. Prev. Med. 2022, 62, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Tanzania Could See Big Returns on Family Planning Investments. Available online: https://www.intrahealth.org/vital/tanzania-could-see-big-returns-family-planning-investments (accessed on 20 December 2020).
- Engstrand, S.; Kopp Kallner, H. Cost of unintended pregnancy in Sweden—A possibility to lower costs by increasing LARC usage. Contraception 2018, 97, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Increasing Access to Contraception Resources from States, Partners, and ASTHO. Available online: https://www.astho.org/Maternal-and-Child-Health/Increasing-Access-to-Contraception-Resources-from-States-Partners-and-ASTHO/ (accessed on 15 April 2020).
- Tanzania, Family Planning 2030. Available online: https://www.familyplanning2020.org/tanzania (accessed on 21 September 2020).
- Wilkinson, T.A.; Downs, S.M.; Tucker Edmonds, B. Cost minimization analysis of same-day long-acting reversible contraception for adolescents. JAMA Netw. Open 2019, 2, e1911063. [Google Scholar] [CrossRef]
- Abasiattai, A.M.; Bassey, E.A.; Udoma, E.J. Profile of intrauterine contraceptive device acceptors at the University of Uyo Teaching Hospital, Uyo, Nigeria. Ann. Afr. Med. 2008, 7, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branum, A.M.; Jones, J. Trends in long-acting reversible contraception use among U.S. Women aged 15–44. In NCHS Data Brief; National Center for Health Statistics: Atlanta, GA, USA, 2015; pp. 1–8. [Google Scholar]
- Adedini, S.A.; Omisakin, O.A.; Somefun, O.D. Trends, patterns and determinants of long-acting reversible methods of contraception among women in sub-Saharan Africa. PLoS ONE 2019, 14, e0217574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, K.; Abma, J.C. Current Contraceptive Status among Women Aged 15–49: United States, 2015–2017; NCHS Data Brief, No. 327; National Center for Health Statistics: Hyattsville, MD, USA, 2018. [Google Scholar]
- Gayatri, M. The utilization of long-acting reversible contraception and associated factors among women in Indonesia. Glob. J. Health Sci. 2020, 12, 110–120. [Google Scholar] [CrossRef]
- Female Education: A Solution for a Crowded Planet. Available online: https://www.thesolutionsjournal.com/article/female-education-a-solution-for-a-crowded-planet (accessed on 22 November 2020).
- Mason, K.O.; Smith, H.L. Husbands’ versus wives’ fertility goals and use of contraception: The influence of gender context in five Asian countries. Demography 2000, 37, 299–311. [Google Scholar] [CrossRef]
- Bhandari, R.; Pokhrel, K.N.; Gabrielle, N.; Amatya, A. Long acting reversible contraception use and associated factors among married women of reproductive age in Nepal. PLoS ONE 2019, 14, e0214590. [Google Scholar] [CrossRef]
- Mboane, R.; Bhatta, M.P. Influence of a husband’s healthcare decision making role on a woman’s intention to use contraceptives among Mozambican women. Reprod. Health 2015, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Community Development, Gender E and C (MoHCDGEC) [Tanzania Mainland]; Ministry of Health (MoH) [Zanzibar]; National Bureau of Statistics (NBS); Office of the Chief government Statistician (OCGS); ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016; MoHCDGEC/MoH/NBS/OCGS: Dar Es Salaam, Tanzania; ICF: Rockville, MD, USA, 2016.
- Population Reference Bureau. Youth Reproductive Health: Satisfying Unmet Need for Family Planning; Population Reference Bureau: Washington, DC, USA, 2015. [Google Scholar]
- Clifton, D.; Kaneda, T. Family Planning Worldwide 2013 Data Sheet; Population Reference Bureau: Washington, DC, USA, 2013. [Google Scholar]
- Staveteig, S.; Mallick, L.; Winter, R. Uptake and Discontinuation of Long—Acting Reversible Contraceptives (LARCs) in Low-Income Countries; DHS Analytical Studies No. 54; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- de Leon, R.G.P.; Ewerling, F.; Serruya, S.J.; Silveira, M.F.; Sanhueza, A.; Moazzam, A.; Becerra-Posada, F.; Coll, C.V.N.; Hellwig, F.; Victora, C.G.; et al. Contraceptive use in Latin America and the Caribbean with a focus on long-acting reversible contraceptives: Prevalence and inequalities in 23 countries. Lancet Glob. Health 2019, 7, E227–E235. [Google Scholar] [CrossRef] [Green Version]
- Use of Highly Effective Contraceptives in the U.S. Continues to Rise, with Likely Implications for Declines in Unintended Pregnancy and Abortion. Available online: https://www.guttmacher.org/article/2014/12/use-highly-effective-contraceptives-us-continues-rise-likely-implications-declines (accessed on 20 December 2020).
- Dempsey, A.R.; Billingsley, C.C.; Savage, A.H.; Korte, J.E. Predictors of long-acting reversible contraception use among unmarried young adults. Am. J. Obstet. Gynecol. 2012, 206, 526.e1–526.e5. [Google Scholar] [CrossRef] [PubMed]
- Neukom, J.; Chilambwe, J.; Mkandawire, J.; Mbewe, R.K.; Hubacher, D. Dedicated providers of long-acting reversible contraception: New approach in Zambia. Contraception 2011, 83, 447–452. [Google Scholar] [CrossRef]
- Smith, A.J.B.; Harney, K.F.; Singh, T.; Hurwitz, A.G. Provider and health system factors associated with usage of long-acting reversible contraception in adolescents. J. Pediatr. Adolesc. Gynecol. 2017, 30, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Blumenberg, C.; Hellwig, F.; Ewerling, F.; Barros, A.J.D. Socio-demographic and economic inequalities in modern contraception in 11 low- and middle-income countries: An analysis of the PMA2020 surveys. Reprod. Health 2020, 17, 82. [Google Scholar] [CrossRef] [PubMed]
- Larsson, C.; Stanfors, M. Women’s education, empowerment, and contraceptive use in sub-Saharan Africa: Findings from recent demographic and health surveys. Afr. Popul. Stud. 2014, 28, 1022–1034. [Google Scholar] [CrossRef] [Green Version]
- Measure Evaluation. Women and Girls’ Status and Empowerment. Available online: https://measureevaluation.org/prh/rh_indicators/gender/wgse (accessed on 20 December 2020).
- Bolarinwa, O.A.; Olagunju, O.S. Knowledge and factors influencing long-acting reversible contraceptives use among women of reproductive age in Nigeria. Gates Open Res. 2020, 3, 1–4. [Google Scholar] [CrossRef]
- Moreau, C. Trends and determinants of use of long-acting reversible contraception use amonyoung women in France: Results from three national surveys conducted between 2000 and 2010. Fertil. Steril. 2013, 100, 451–458. [Google Scholar] [CrossRef]
- Gilmore, K.; Hoopes, A.J.; Cady, J.; Amies Oelschlager, A.M.; Prager, S.; Vander Stoep, A. Providing long-acting reversible contraception services in Seattle school-based health centers: Key themes for facilitating implementation. J. Adolesc. Health 2015, 56, 658–665. [Google Scholar] [CrossRef]
- Anguzu, R.; Sempeera, H.; Sekandi, J.N. High parity predicts use of long-acting reversible contraceptives in the extended postpartum period among women in rural Uganda. Contracept. Reprod. Med. 2018, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Alemayehu, M.; Kalayu, A.; Desta, A.; Gebremichael, H.; Hagos, T.; Yebyo, H. Rural women are more likely to use long acting contraceptive in Tigray region, Northern Ethiopia: A comparative community-based cross sectional study. BMC Women’ Health 2015, 15, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, K.; Reddy, S.; Getachew, B. Unmet need of long-acting and permanent family planning methods among women in the reproductive age group in shashemene town, Oromia region, Ethiopia: A cross sectional study. BMC Women’ Health 2015, 15, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teferra, A.S.; Wondifraw, A.A. Determinants of long acting contraceptive use among reproductive age women in Ethiopia: Evidence from EDHS 2011. Sci. J. Public Health 2015, 3, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Tekelab, T.; Sufa, A.; Wirtu, D. Factors affecting intention to use long acting and permanent contraceptive methods among married women of reproductive age groups in Western Ethiopia: A community based cross sectional study. Fam. Med. Med. Sci. Res. 2015, 4, 2. [Google Scholar]


{kind=link}
| Variable | Total | Using LARCs | Not Using LARCs | p-Value |
|---|---|---|---|---|
| Woman’s age (years) | N | n (%) | n (%) | |
| 15–19 | 619 | 17 (2.75) | 602 (97.25) | |
| 20–35 | 4788 | 422 (8.81) | 4366 (91.19) | <0.0001 |
| >35 | 2782 | 156 (5.61) | 2626 (94.39) | |
| Husbands/Partners age (years) | ||||
| 17–24 | 624 | 36 (5.769) | 588 (94.23) | |
| 25–34 | 2590 | 226 (8.726) | 2364 (91.27) | <0.0001 |
| 35–44 | 2629 | 212 (8.064) | 2417 (91.94) | |
| >44 | 2345 | 121 (5.16) | 2224 (94.84) | |
| Woman’s occupation status | ||||
| Not working | 1388 | 77 (5.55) | 1311 (94.45) | |
| Professional | 281 | 21 (7.47) | 260 (92.56) | |
| Clerical | 34 | 1 (2.94) | 33 (97.06) | |
| Agricultural—Self-employed | 4101 | 300 (7.32) | 3801 (92.68) | |
| Agricultural—Employee | 237 | 17 (7.17) | 220 (92.83) | 0.1676 |
| Household and domestic | 263 | 20 (7.61) | 243 (92.4) | |
| Services | 285 | 27 (9.47) | 258 (90.53) | |
| Skilled manual | 337 | 28 (8.31) | 309 (91.69) | |
| Unskilled manual | 1263 | 104 (8.23) | 1159 (91.77) | |
| Woman’s education level | ||||
| No education | 1610 | 80 (4.97) | 1530 (95.03) | |
| Incomplete primary | 1026 | 73 (7.12) | 953 (92.88) | |
| Complete primary | 4022 | 323 (8.03) | 3699 (91.97) | 0.001 |
| Incomplete secondary | 643 | 39 (6.07) | 604 (93.93) | |
| Complete secondary | 810 | 75 (9.26) | 735 (90.74) | |
| Higher | 78 | 5 (6.41) | 73 (93.59) | |
| Husband’s/Partner’s education status | ||||
| No education/don’t know | 1093 | 36 (3.294) | 1057 (96.71) | |
| Primary | 5292 | 428 (8.088) | 4864 (91.91) | <0.0001 |
| Secondary and higher | 1804 | 131 (7.262) | 1673 (92.74) | |
| Residence | ||||
| Urban | 2183 | 176 (8.06) | 2007 (91.94) | |
| Rural | 6006 | 419 (6.98) | 5587 (93.02) | 0.1321 |
| Wealth index | ||||
| Poorest | 1587 | 86 (5.42) | 1501 (94.58) | |
| Poorer | 1455 | 97 (6.67) | 1358 (93.33) | |
| Middle | 1586 | 126 (7.95) | 1460 (92.06) | 0.005 |
| Richer | 1835 | 164 (8.94) | 1671 (91.06) | |
| Richest | 1726 | 122 (7.07) | 1604 (92.93) | |
| Variable | Total | Using LARCs | Not Using LARCs | p-Value |
|---|---|---|---|---|
| Age at first birth (years) | ||||
| ≤13 | 94 | 89 (94.68) | 5 (5.32) | |
| 15–19 | 4492 | 4121 (91.74) | 371 (8.26) | |
| 20–24 | 2420 | 2244 (92.73) | 176 (7.27) | |
| 25–29 | 508 | 466 (92.46) | 38 (7.54) | |
| ≥30 | 108 | 105 (97.22) | 3 (2.78) | 0.141 |
| Parity | ||||
| 0 | 646 | 3 (.46) | 646 (99.54) | |
| 1–4 | 5149 | 428 (8.31) | 4721 (91.69) | <0.0001 |
| >4 | 2394 | 164 (6.85) | 2230 (93.15) | |
| Desire for the last child | ||||
| Wanted then | 3983 | 311 (7.81) | 3672 (92.19) | |
| Wanted later | 1519 | 220 (10.82) | 1362 (89.66) | 0.0112 |
| Wanted no more | 248 | 25 (10.08) | 223 (89.92) | |
| Desire for more children | ||||
| Wants within 2 years | 1862 | 58 (3.12) | 1804 (96.89) | |
| Wants after 2 years | 3507 | 328 (9.35) | 3179 (90.65) | |
| Wants, unsure timing | 81 | 3 (3.70) | 78 (96.30) | <0.0001 |
| Undecided | 242 | 10 (4.13) | 232 (95.87) | |
| Wants no more | 2056 | 193 (9.39) | 1863 (90.61) | |
| Sterilized/Declared infecund | 438 | 3 (0.68) | 435 (99.32) | |
| Visited health facility in the last 12 months | ||||
| Yes | 5669 | 5246 (92.54) | 423 (7.46) | |
| No | 2518 | 2346 (93.17) | 172 (6.83) | 0.316 |
| Information on family planning provided | ||||
| Yes | 2184 | 200 (9.16) | 1984 (90.84) | |
| No | 3485 | 223 (6.40) | 3262 (93.6) | 0.0003 |
| Knowledge of family planning methods | ||||
| Knows modern methods | 8122 | 595 (7.33) | 7527 (92.67) | |
| Don’t know | 67 | 0 | 67 (100) | 0.1115 |
| Variable | N | COR (CI 95%) | AOR (CI 95%) |
|---|---|---|---|
| Woman’s age (years) | |||
| 15–19 | 619 | 1 | 1 |
| 20–35 | 4788 | 3.42 (2.09–5.61) | 2.66 (1.39–5.07) * |
| 36–49 | 2782 | 2.10 (1.25–3.54) | 2.29 (1.08–4.87) * |
| Husband/Partner age (years) | |||
| 17–24 | 624 | 1 | 1 |
| 25–34 | 2590 | 1.56 (1.09–2.25) | 0.99 (0.60–1.63) |
| 35–44 | 2629 | 1.43 (0.97–2.11) | 1.04 (0.59–1.81) |
| >44 | 2345 | 0.89 (0.60–1.32) | 0.79 (0.41–1.51) |
| Parity | |||
| 0 | 646 | 1 | 1 |
| 1–4 | 5149 | 19.43 (6.27–60.17) | 2.71 (0.37–20.07) |
| >4 | 1394 | 15.76 (5.07–49.03) | 2.56 (0.33–19.64) |
| Desire for more children (woman) | |||
| Wants within 2 years | 1862 | 1 | 1 |
| Wants after 2 years | 3507 | 2.85 (2.18–3.72) | 2.27 (1.51–3.42) * |
| Wants, unsure timing | 81 | 0.45 (0.28–0.73) | - |
| Undecided | 242 | 1.21 (0.75–1.96) | 1.11 (0.46–2.69) |
| Wants no more | 2056 | 3.21 (2.41–4.28) | 2.42 (1.51–3.86) * |
| Sterilized/Declared infecund | 438 | 0.47 (0.18–1.28) | - |
| Desire for the last child | |||
| Wanted then | 3983 | 1 | 1 |
| Wanted later | 1519 | 1.36 (1.10–1.68) | 1.10 (0.85–1.42) |
| Wanted no more | 248 | 1.32 (0.84–2.08) | 1.16 (0.64–2.09) |
| Woman’s occupation status | |||
| Unemployed | 1388 | 1.38 (0.82–2.29) | 0.93 (0.43–2.02) |
| Professional | 281 | 0.52 (0.07–3.58) | 1.03 (0.15–7.10) |
| Clerical | 34 | 1 | 1 |
| Agricultural—Self-employed | 4101 | 1.34 (1.04–1.74) | 1.21 (0.84–1.73) |
| Agricultural—employee | 237 | 1.32 (0.74–2.33) | 1.74 (0.83–3.66) |
| Household and domestic | 263 | 1.40 (0.88–2.24) | 1.25 (0.65–2.38) |
| Services | 285 | 1.78 (1.15–2.77) | 1.26 (0.69–2.29) |
| Skilled manual | 337 | 1.54 (0.97–2.45) | 1.16 (0.65–2.08) |
| Unskilled manual | 1263 | 1.53 (1.51–2.03) | 1.40 (0.98–2.01) |
| Wealth index | |||
| Poorest | 1587 | 1 | 1 |
| Poorer | 1455 | 1.25 (0.91–1.72) | 1.28 (0.88–1.86) |
| Middle | 1586 | 1.51 (1.08–2.10) | 1.16 (0.75–1.78) |
| Richer | 1835 | 1.71 (1.28–2.28) | 1.37 (1.92–2.06) * |
| Richest | 1726 | 1.33 (0.98–1.80) | 0.93 (0.58–1.50) |
| Husband/Partner desire for children | |||
| Both want the same | 2966 | 1 | 1 |
| Husband wants more | 2138 | 0.69 (0.56–0.86) | 0.67 (0.49–0.91) * |
| Husband wants fewer | 444 | 1.26 (0.89–1.79) | 1.35 (0.89–2.05) |
| Don’t know | 2390 | 0.54 (0.44–0.68) | 1.35 (0.89–2.05) |
| Partner/Husband education status | |||
| No education | 1093 | 1 | 1 |
| Primary | 5292 | 2.58 (1.82–3.67) | 2.29 (1.8–3.81) * |
| Secondary and higher | 1804 | 2.30 (1.55–3.41) | 2.40 (1.37–4.21) * |
| Woman’s education level | |||
| No education | 1610 | 1 | 1 |
| Incomplete primary | 1026 | 1.33 (0.96–1.84) | 1.36 (0.89–2.08) |
| Complete primary | 4022 | 1.59 (1.23–2.07) | 1.37 (0.99–1.88) |
| Incomplete secondary | 643 | 0.76 (0.53–1.09) | 1.05 (0.65–1.70) |
| Complete secondary | 810 | 1.18 (0.85–1.65) | 1.64 (1.05–2.55) * |
| Higher | 78 | 1.09 (0.49–2.44) | 1.32 (0.43–4.15) |
| Residence | |||
| Urban | 2183 | 1 | |
| Rural | 6006 | 0.86 (0.69–1.05) | - |
| Knowledge of family planning methods | |||
| Knows modern methods | 8122 | 0.63 (0.06–0.07) | |
| Don’t know | 67 | 1 | - |
| Information on family planning provided | |||
| Yes | 2184 | 1.47 (1.19–1.82) | 1.17 (0.93–1.47) |
| No | 3485 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikula, A.I.; Moshiro, C.; Makoko, N.; Park, E.; Pembe, A.B. Low Use of Long-Acting Reversible Contraceptives in Tanzania: Evidence from the Tanzania Demographic and Health Survey. Int. J. Environ. Res. Public Health 2022, 19, 4206. https://doi.org/10.3390/ijerph19074206
Kikula AI, Moshiro C, Makoko N, Park E, Pembe AB. Low Use of Long-Acting Reversible Contraceptives in Tanzania: Evidence from the Tanzania Demographic and Health Survey. International Journal of Environmental Research and Public Health. 2022; 19(7):4206. https://doi.org/10.3390/ijerph19074206
Chicago/Turabian StyleKikula, Amani Idris, Candida Moshiro, Naku Makoko, Eunyoung Park, and Andrea Barnabas Pembe. 2022. "Low Use of Long-Acting Reversible Contraceptives in Tanzania: Evidence from the Tanzania Demographic and Health Survey" International Journal of Environmental Research and Public Health 19, no. 7: 4206. https://doi.org/10.3390/ijerph19074206
APA StyleKikula, A. I., Moshiro, C., Makoko, N., Park, E., & Pembe, A. B. (2022). Low Use of Long-Acting Reversible Contraceptives in Tanzania: Evidence from the Tanzania Demographic and Health Survey. International Journal of Environmental Research and Public Health, 19(7), 4206. https://doi.org/10.3390/ijerph19074206