
Evaluating the Psychometric Properties of the eHealth Literacy Scale (eHEALS) among Polish Social Media Users


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
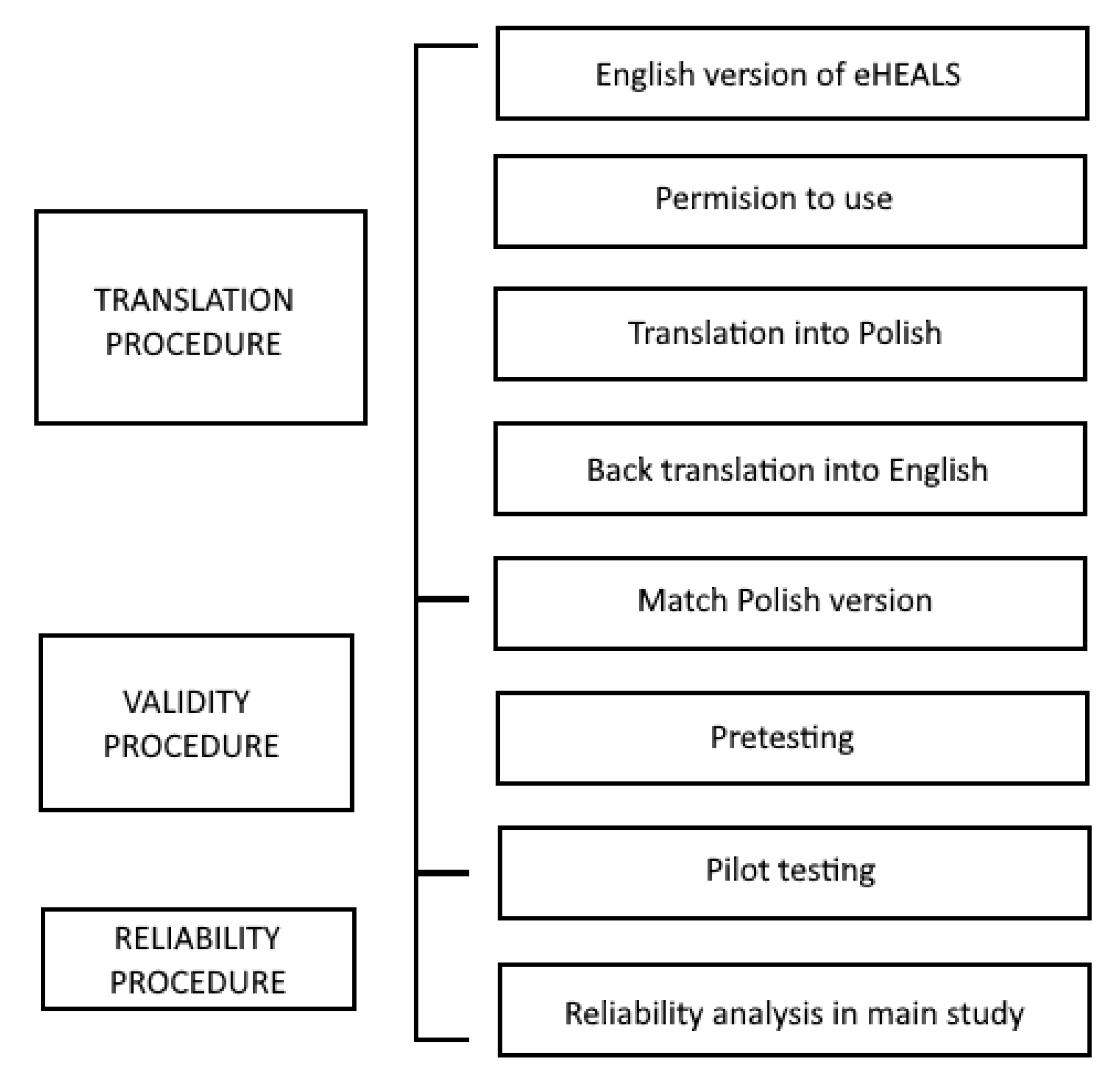
2.2. Instrument: eHEALS
2.3. Content Validity and Pilot Study
2.4. Recruitment and Participants
- -
- Facebook: (1) groups—the information about the survey was sent directly to administrators along with an active link to the electronic questionnaire; (2) fan pages—sending a message to the administrator, with the information about the study along with an active link referring to the electronic questionnaire;
- -
- Twitter: by posting information about the survey and marking accounts in tweets with an active link to the questionnaire;
- -
- Internet forums: (1) by publishing a post with the information about the conducted study directly in the stream of an active discussion; and/or (2) by sending a message to the forum administrator with a request to inform users about the conducted study;
- -
- blogs: through direct contact with authors—a message with information about the survey was sent via a contact form or post in the comments section;
- -
- YouTube channels: by publishing the information about the survey along with an active link to the questionnaire in the comments section.
2.5. Data Analysis
2.6. Reliability
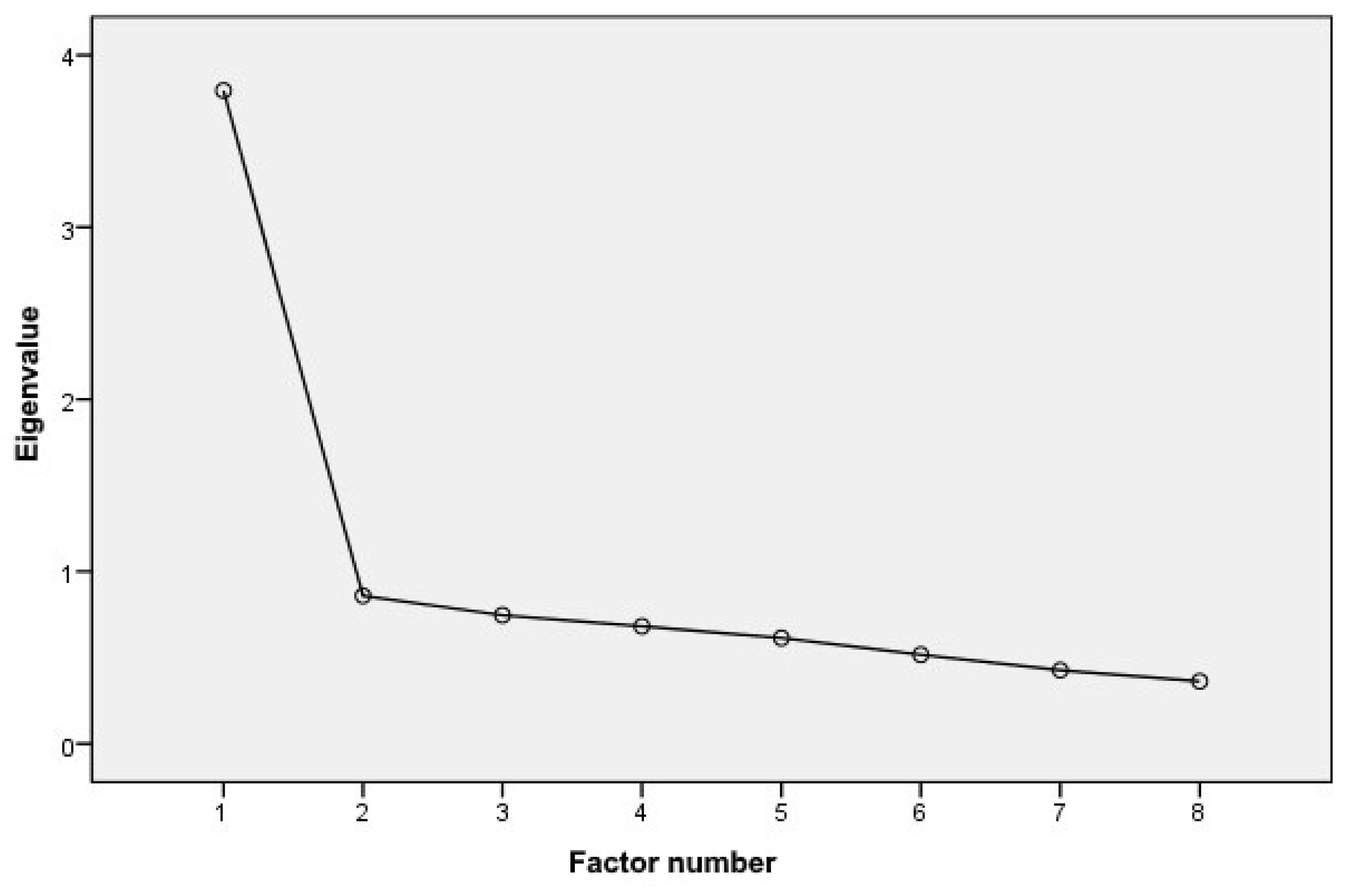
2.7. Construct Validity—Exploratory Factor Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Reliability
3.3. Construct Validity—Exploratory Factor Analysis
3.4. Construct Validity—Hypothesis Testing
3.5. Interpretation of eHEALS-Pl Scores
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Commission. Flash Eurobarometer 404: European Citizens’ Digital Health Literacy Survey. 2014. Available online: http://ec.europa.eu/commfrontoffice/publicopinion/flash/fl_404_en.pdf (accessed on 23 November 2021).
- Garapich, A. Internet a Decyzje Zakupowe—Rola Internetu w Procesie Zakupu Leków i Preparatów Zdrowotnych. 2012. Available online: https://www.slideshare.net/P_B_I/internet-a-decyzje-zakupowe-rola-internetu-w-procesie-zakupu-lekw-i-produktw-zdrowotnych (accessed on 23 November 2021).
- Fox, S.; Duggan, M. Health Online 2013; Pew Internet & American Life Project: Washington, DC, USA, 2013; Available online: http://www.pewinternet.org/files/old-media//Files/Reports/PIP_HealthOnline.pdf (accessed on 23 November 2021).
- Weiner, S.S.; Horbacewicz, J.; Rasberry, L.; Bensinger-Brody, Y. Improving the Quality of Consumer Health Information on Wikipedia: Case Series. J. Med. Internet Res. 2019, 21, e12450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GUS Społeczeńśtwo Informacyjne w Polsce—Wyniki Badań Statystycznych 2015–2019. 2019. Available online: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5497/1/13/1/spoleczenstwo_informacyjne_w_polsce_-_wyniki_badan_statystycznych_z_lat_2015-2019.pdf (accessed on 17 March 2022).
- CBOS Korzystanie z Internetu. Komunikat CBOS. 2019. Available online: https://cbos.pl/SPISKOM.POL/2019/K_095_19.PDF (accessed on 17 March 2022).
- Silver, L.; Smith, A.; Johnson, C.; Taylor, K.; Jiang, J.; Anderson, M.; Rainie, L. Use of Smartphones and Social Media is Common across Most Emerging Economies; Pew Internet & American Life Project: Washington, DC, USA, 2019; Available online: https://www.pewinternet.org/2019/03/07/use-of-smartphones-and-social-media-is-common-across-most-emerging-economies/#sortable-table (accessed on 23 November 2021).
- Lee, K.; Hoti, K.; Hughes, J.D.; Emmerton, L.M. Consumer Use of “Dr Google”: A Survey on Health Information-Seeking Behaviors and Navigational Needs. J. Med. Internet Res. 2015, 17, e288. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHealth literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Duplaga, M.; Sobecka, K.; Wójcik, S. The Reliability and Validity of the Telephone-Based and Online Polish eHealth Literacy Scale Based on Two Nationally Representative Samples. Int. J. Environ. Res. Public Health 2019, 16, 3216. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Kickbusch, I. Health literacy: An essential skill for the twenty-first century. Health Educ. 2008, 108, 101–104. [Google Scholar] [CrossRef]
- Parker, R.M.; Williams, M.V.; Weiss, B.D.; Baker, D.W.; Davis, T.C.; Doak, C.C.; Doak, L.G.; Hein, K.; Meade, C.D.; Dickinson, B.D.; et al. Health Literacy: Report of the Council on Scientific Affairs. Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. JAMA 1999, 281, 552–557. [Google Scholar]
- Nielsen-Bohlman, L.; Panzer, A.M.; Kindig, D.A. (Eds.) Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. Available online: https://pubmed.ncbi.nlm.nih.gov/25009856/ (accessed on 25 November 2021).
- Eysenbach, G. Improving the quality of web surveys: The checklist for reporting results of internet e-surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Van der Vaart, R.; van Deursen, A.J.; Drossaert, C.H.; Taal, E.; van Dijk, J.A.; van de Laar, M.A. Does the eHealth Literacy Scale (eHEALS) Measure What it Intends to Measure? Validation of a Dutch Version of the eHEALS in Two Adult Populations. J. Med. Internet Res. 2011, 13, e86. [Google Scholar]
- Mitsutake, S.; Shibata, A.; Ishii, K.; Okazaki, K.; Oka, K. Developing Japanese version of the eHealth Literacy Scale (eHEALS). Nihon Koshu Eisei Zasshi 2011, 58, 361–371. [Google Scholar] [PubMed]
- Pérez, G.P.; Almagro, B.J.; Gómez, Á.H.; Gómez, A.; Gómez, J.I.A. Validación de la escala eHealth Literacy Scale (eHEALS) en población universitaria Española. Rev. Esp. Salud Publica 2015, 89, 329–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diviani, N.; Dima, A.L.; Schulz, P.J. A Psychometric Analysis of the Italian Version of the eHealth Literacy Scale Using Item Response and Classical Test Theory Methods. J. Med. Internet Res. 2017, 19, e114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soellner, R.; Huber, S.; Reder, M. The concept of eHealth literacy and its measurement: German translation of the eHEALS. J. Media Psychol. 2014, 26, 29–38. [Google Scholar] [CrossRef]
- Bazm, S.; Mirzaei, M.; Fallahzadeh, H.; Bazm, R. Validity and Reliability of the Iranian Version of eHealth Literacy Scale. J. Community Health Res. 2016, 5, 121–130. [Google Scholar]
- World Health Organization. Process of Translation and Adaptation of Instruments. 2011. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/index.html (accessed on 25 November 2021).
- Eysenbach, G.; Wyatt, J. Using the Internet for surveys and health research. J. Med. Internet Res. 2002, 4, e13. [Google Scholar] [CrossRef]
- Peterson, R.A. A meta-analysis of Cronbach’s coefficient alpha. J. Consum. Res. 1994, 21, 381–391. [Google Scholar] [CrossRef]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994; pp. 34–35. [Google Scholar]
- Loewen, S.; Gonulal, T. Exploratory Factor Analysis and Principal Components Analysis. In Advancing Quantitative Methods in Second Language Research; Plonsky, L., Ed.; Routledge: New York, NY, USA, 2015; pp. 182–212. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- De Caro, W.; Corvo, E.; Marucci, A.R.; Mitello, L.; Lancia, L.; Sansoni, J. eHealth Literacy Scale: An Nursing Analisys and Italian Validation. Stud. Health Technol. Inform. 2016, 225, 949. [Google Scholar]
- Tomás, C.C.; Queirós, P.J.P.; Ferreira, T.D.J.R. Analysis of the psychometric properties of the Portuguese version of an ehealth literacy assessment tool. Rev. Enferm. Ref. 2014, 2, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.; Park, B.K.; Nahm, E.S. The Korean eHealth Literacy Scale (K-eHEALS): Reliability and Validity Testing in Younger Adults Recruited Online. J. Med. Internet Res. 2018, 20, e138. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.; Schultz, P.J. The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China. Int. J. Environ. Res. Public Health 2018, 15, 1553. [Google Scholar] [CrossRef] [Green Version]
- Koo, M.; Norman, C.D.; Hsiao-Mei, C. Psychometric Evaluation of a Chinese Version of the eHealth Literacy Scale in school age children. Int. Electron. J. Health Educ. 2012, 15, 29–36. [Google Scholar]
- Coskun, S.; Bebis, H. Psychometric evaluation of a Turkish version of the e-health literacy scale (e-heals) in adolescents. Gulhane Med. J. 2015, 57, 378. [Google Scholar] [CrossRef]
- Sudbury-Riley, L.; FitzPatrick, M.; Schulz, P.J. Exploring the Measurement Properties of the eHealth Literacy Scale (eHEALS) Among Baby Boomers: A Multinational Test of Measurement Invariance. J. Med. Internet Res. 2017, 19, e53. [Google Scholar] [CrossRef] [Green Version]
- Stellefson, M.; Paige, S.R.; Tennant, B.; Alber, J.M.; Chaney, B.H.; Chaney, D.; Grossman, S. Reliability and Validity of the Telephone-Based eHealth Literacy Scale Among Older Adults: Cross-Sectional Survey. J. Med. Internet Res. 2017, 19, e362. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.Y.; Nahm, E.S. Testing reliability and validity of the eHealth Literacy Scale (eHEALS) for older adults recruited online. Comput. Inform. Nurs. 2015, 33, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Neter, E.; Brainin, E. eHealth Literacy: Extending the Digital Divide to the Realm of Health Information. J. Med. Internet Res. 2012, 14, e19. [Google Scholar] [CrossRef]
- Hyde, L.L.; Boyes, A.W.; Evans, T.J.; Mackenzie, L.J.; Sanson-Fisher, R. Three-Factor Structure of the eHealth Literacy Scale Among Magnetic Resonance Imaging and Computed Tomography Outpatients: A Confirmatory Factor Analysis. JMIR Hum. Factors 2018, 5, e6. [Google Scholar] [CrossRef]
- James, D.C.; Harville, C., II. eHealth Literacy, Online Help-Seeking Behavior, and Willingness to Participate in mHealth Chronic Disease Research Among African Americans, Florida, 2014–2015. Prev. Chronic Dis. 2016, 13, 160210. [Google Scholar] [CrossRef] [Green Version]
- Wångdahl, J.; Jaensson, M.; Dahlberg, K.; Nilsson, U. The Swedish Version of the Electronic Health Literacy Scale: Prospective Psychometric Evaluation Study Including Thresholds Levels. JMIR mHealth uHealth 2020, 8, e16316. [Google Scholar] [CrossRef]
- Li, X.; Liu, Q. Social Media Use, eHealth Literacy, Disease Knowledge, and Preventive Behaviors in the COVID-19 Pandemic: Cross-Sectional Study on Chinese Netizens. J. Med. Internet Res. 2020, 22, e19684. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| eHEALS-Pl Items | Mean (SD a) | Mean, If Item Deleted | α, If Item Deleted | Variance of the Scale, If Item Deleted | Item-to-Total Correlation b |
|---|---|---|---|---|---|
| item 1 | 3.61 (0.946) | 27.08 | 0.814 | 14.920 | 0.634 |
| item 2 | 3.69 (0.985) | 27.00 | 0.809 | 14.482 | 0.666 |
| item 3 | 3.91 (0.731) | 26.78 | 0.829 | 16.831 | 0.514 |
| item 4 | 3.87 (0.798) | 26.82 | 0.815 | 15.828 | 0.626 |
| item 5 | 3.98 (0.756) | 26.71 | 0.830 | 16.738 | 0.506 |
| item 6 | 3.93 (0.722) | 26.76 | 0.828 | 16.852 | 0.518 |
| item 7 | 4.00 (0.677) | 26.69 | 0.829 | 17.094 | 0.516 |
| item 8 | 3.71 (0.906) | 26.97 | 0.817 | 15.327 | 0.605 |
| Mean (SD) sum score | 30.69 (4.52) |
| Variable | α | Items |
|---|---|---|
| Gender | ||
| female | 0.834 | 8 |
| male | 0.869 | 8 |
| Age (years) | ||
| <17 | 0.799 | 8 |
| 17–24 | 0.789 | 8 |
| 25–34 | 0.808 | 8 |
| 35–44 | 0.809 | 8 |
| 45–59 | 0.837 | 8 |
| 60–64 | 0.807 | 8 |
| <64 | 0.847 | 8 |
| Item | Age (Years) | Gender | |||||||
|---|---|---|---|---|---|---|---|---|---|
| <17 | 17–24 | 25–34 | 35–44 | 45–59 | 60–64 | 64+ | Females | Males | |
| item 1 | 0.777 | 0.744 | 0.768 | 0.793 | 0.779 | 0.776 | 0.804 | 0.807 | 0.841 |
| item 2 | 0.737 | 0.762 | 0.764 | 0.769 | 0.804 | 0.805 | 0.820 | 0.802 | 0.843 |
| item 3 | 0.759 | 0.770 | 0.788 | 0.800 | 0.784 | 0.811 | 0.850 | 0.821 | 0.861 |
| item 4 | 0.745 | 0.752 | 0.779 | 0.780 | 0.808 | 0.763 | 0.818 | 0.808 | 0.844 |
| item 5 | 0.753 | 0.782 | 0.792 | 0.789 | 0.815 | 0.751 | 0.837 | 0.822 | 0.864 |
| item 6 | 0.812 | 0.780 | 0.800 | 0.792 | 0.857 | 0.787 | 0.796 | 0.822 | 0.853 |
| item 7 | 0.836 | 0.763 | 0.804 | 0.796 | 0.825 | 0.790 | 0.857 | 0.821 | 0.864 |
| item 8 | 0.761 | 0.771 | 0.785 | 0.777 | 0.844 | 0.794 | 0.828 | 0.810 | 0.851 |
| Pl-eHEALS | 1 |
|---|---|
| (Q1) I know which health resources are available on the Internet | 0.769 |
| (Q2) I know where to find helpful health resources on the Internet | 0.741 |
| (Q3) I know how to use the health information I find on the Internet to help me | 0.736 |
| (Q4) I know how to find helpful health resources on the Internet | 0.721 |
| (Q5) I have the skills I need to evaluate the health resources I find on the Internet | 0.634 |
| (Q6) I know how to use the Internet to answer my questions about health | 0.633 |
| (Q7) I can perceive which health resources are of high quality and which are of low quality on the Internet | 0.633 |
| (Q8) I feel confident in using information from the Internet to make health decisions | 0.623 |
| % of variance explained | 47.426 |
| N = 1527 | eHEALS-Pl Overall | |
|---|---|---|
| Social media usage—overall | rho | 0.141 |
| p | <0.001 | |
| rho | 0.069 | |
| p | <0.001 | |
| YouTube | rho | 0.027 |
| p | 0.290 | |
| rho | 0.029 | |
| p | 0.252 | |
| rho | 0.092 | |
| p | <0.001 | |
| Snapchat | rho | −0.123 |
| p | <0.001 | |
| rho | −0.29 | |
| p | 0.250 | |
| Wikipedia | rho | 0.037 |
| p | 0.147 | |
| Blogs | rho | 0.243 |
| p | <0.001 | |
| Online forums | rho | 0.187 |
| p | <0.001 | |
| eHEALS-Pl Items | eHEALS-Pl Overall | |
|---|---|---|
| ra | ρb | |
| (Q1) I know what health resources are available on the Internet | 0.750 ** | 0.719 ** |
| (Q2) I know where to find helpful health resources on the Internet | 0.778 ** | 0.744 ** |
| (Q3) I know how to use the health information I find on the Internet to help me | 0.628 ** | 0.599 ** |
| (Q4) I know how to find helpful health resources on the Internet | 0.728 ** | 0.677 ** |
| (Q5) I have the skills I need to evaluate the health resources I find on the Internet | 0.625 ** | 0.600 ** |
| (Q6) I know how to use the Internet to answer my questions about health | 0.630 ** | 0.591 ** |
| (Q7) I can perceive which health resources are of high quality and which are of low quality on the Internet | 0.622 ** | 0.603 ** |
| (Q8) I feel confident in using information from the Internet to make health decisions | 0.725 ** | 0.691 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burzyńska, J.; Rękas, M.; Januszewicz, P. Evaluating the Psychometric Properties of the eHealth Literacy Scale (eHEALS) among Polish Social Media Users. Int. J. Environ. Res. Public Health 2022, 19, 4067. https://doi.org/10.3390/ijerph19074067
Burzyńska J, Rękas M, Januszewicz P. Evaluating the Psychometric Properties of the eHealth Literacy Scale (eHEALS) among Polish Social Media Users. International Journal of Environmental Research and Public Health. 2022; 19(7):4067. https://doi.org/10.3390/ijerph19074067
Chicago/Turabian StyleBurzyńska, Joanna, Magdalena Rękas, and Paweł Januszewicz. 2022. "Evaluating the Psychometric Properties of the eHealth Literacy Scale (eHEALS) among Polish Social Media Users" International Journal of Environmental Research and Public Health 19, no. 7: 4067. https://doi.org/10.3390/ijerph19074067
APA StyleBurzyńska, J., Rękas, M., & Januszewicz, P. (2022). Evaluating the Psychometric Properties of the eHealth Literacy Scale (eHEALS) among Polish Social Media Users. International Journal of Environmental Research and Public Health, 19(7), 4067. https://doi.org/10.3390/ijerph19074067