
Self-Reported Computer Vision Syndrome among Thai University Students in Virtual Classrooms during the COVID-19 Pandemic: Prevalence and Associated Factors

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Data
3.2. Characteristics of Screen Display and Usage Behavior
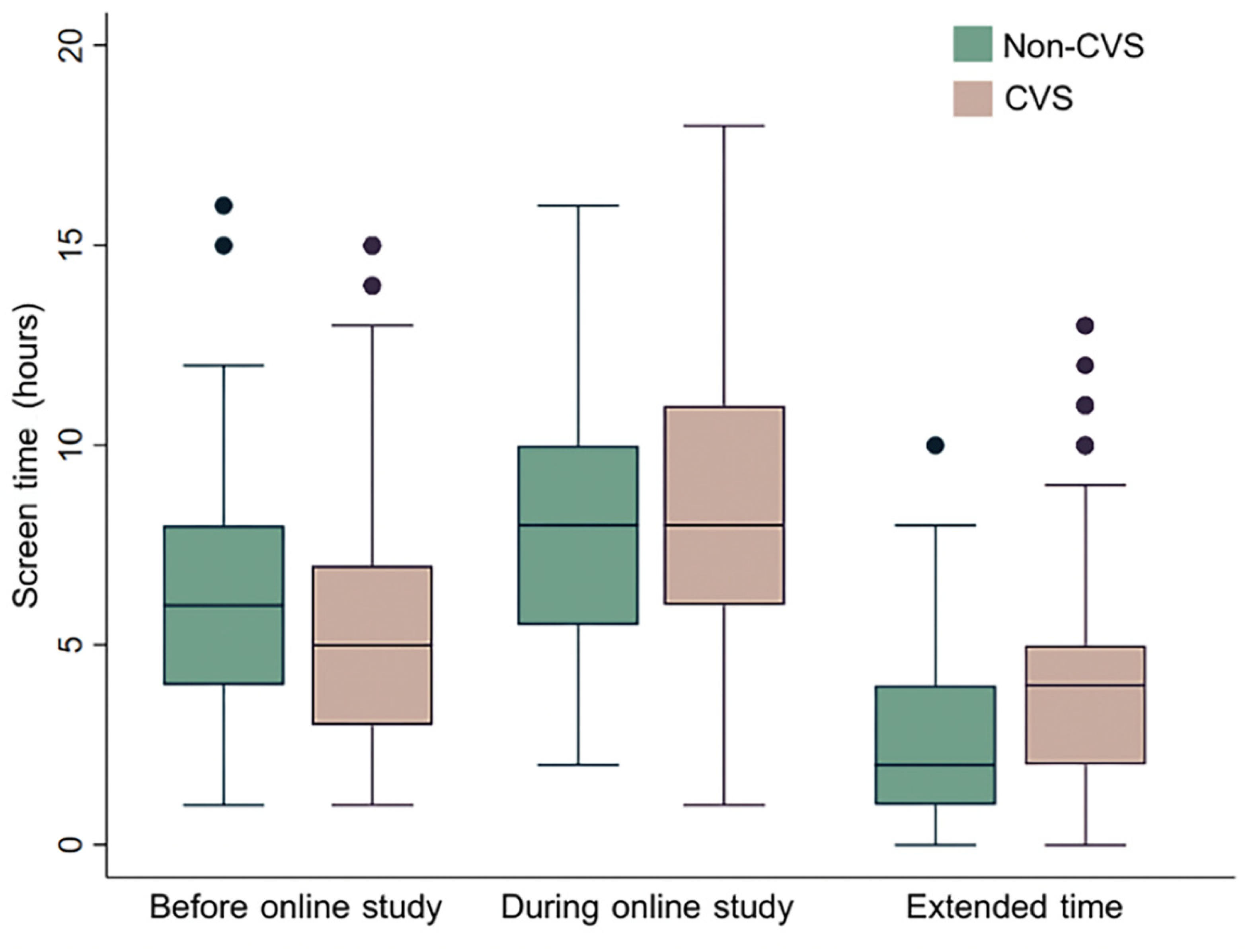
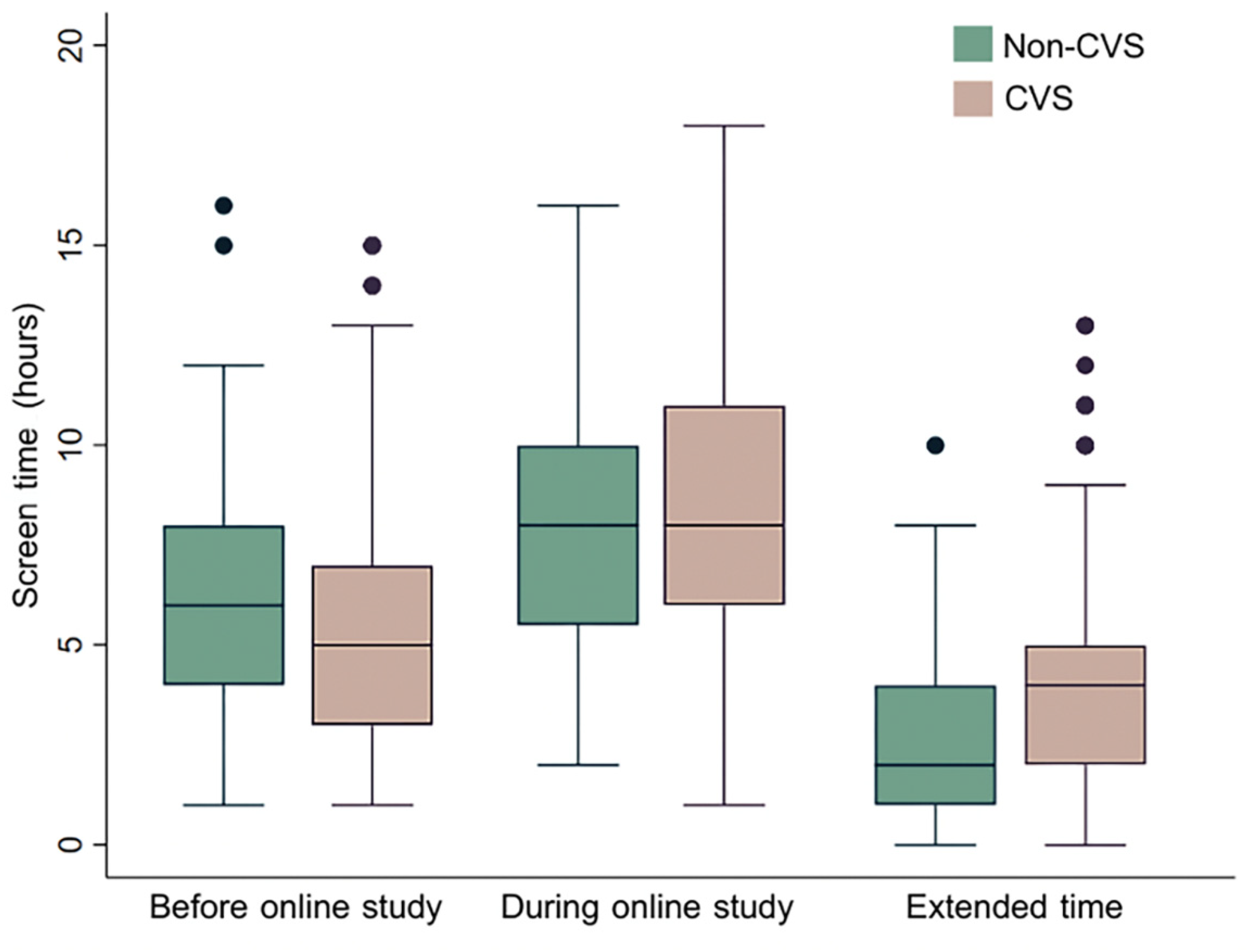
3.3. Screen Time and Rest Behaviors
3.4. Factors Associated with CVS
4. Discussion
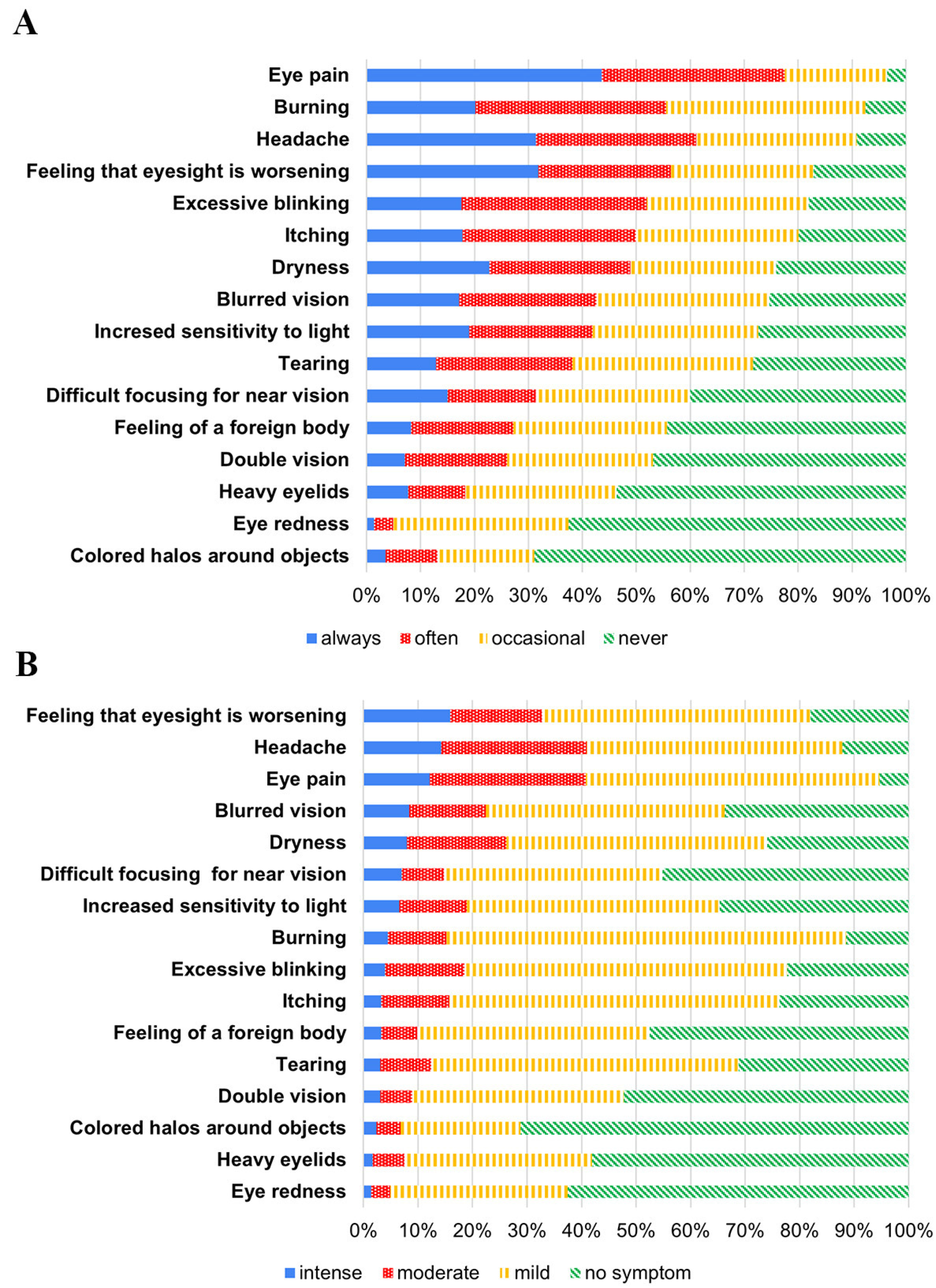
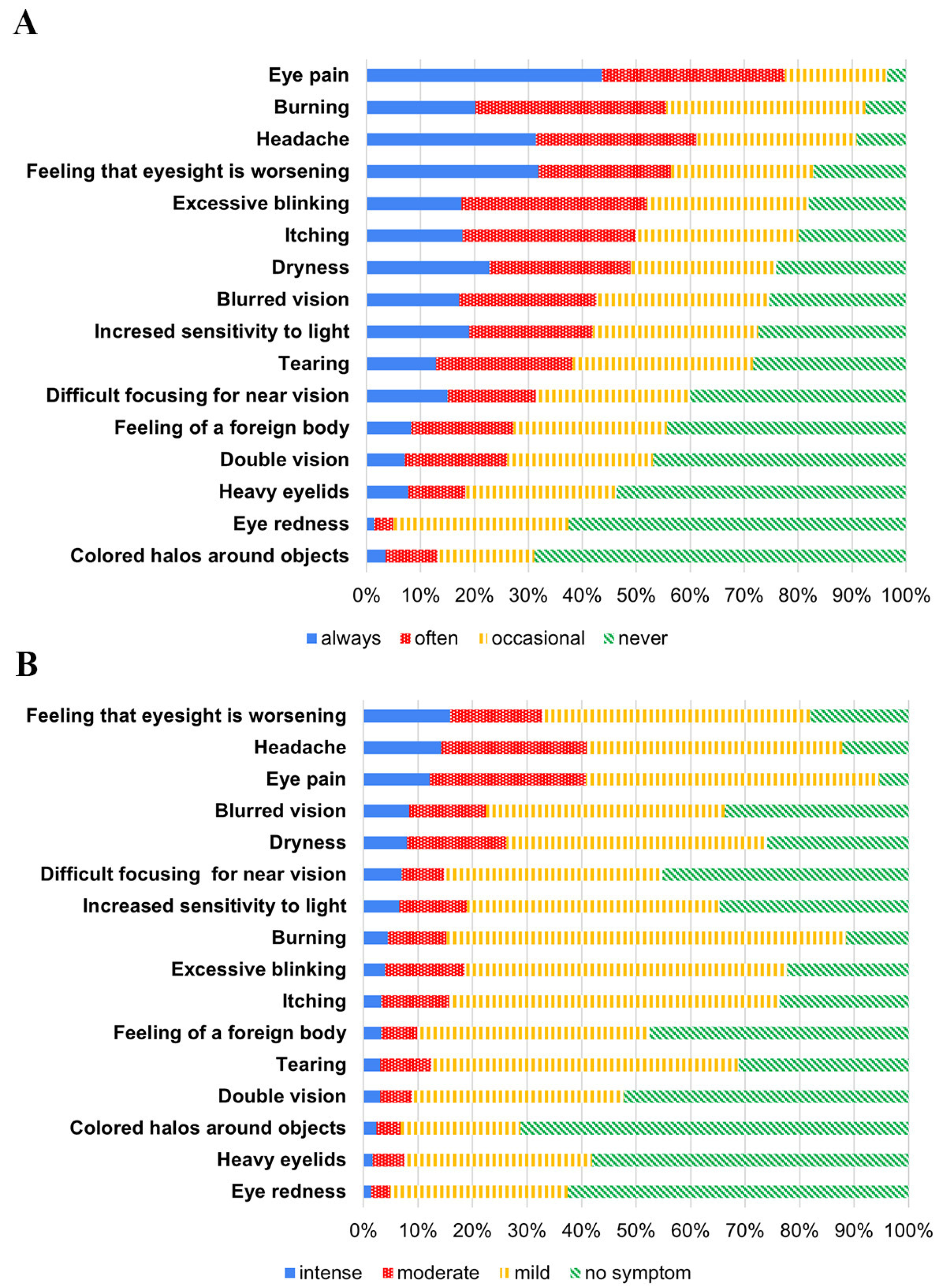
4.1. Reported Symptoms
4.2. Associated Factors
4.2.1. Gender
4.2.2. Age
4.2.3. Atopic Diseases
4.2.4. Prior Ocular Symptoms
4.2.5. Astigmatism
4.2.6. Distance from Display Less than 20 cm
4.2.7. Increased Screen Time
4.2.8. Environmental Factors
4.2.9. Sleeping Duration
4.2.10. Adequate Break Time between Classes
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Internet Users Statistics and 2021 World Population Stats (Blog). Available online: https://www.internetworldstats.com/stats.htm (accessed on 17 October 2021).
- Advice for the Public on COVID-19–World Health Organization (Blog). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 17 October 2021).
- The COVID-19 Pandemic Has Changed Education Forever. This Is How (Blog). World Economic Forum. Available online: https://www.weforum.org/agenda/2020/04/coronavirus-education-global-covid19-online-digital-learning (accessed on 18 October 2021).
- Loh, K.; Redd, S. Understanding and Preventing Computer Vision Syndrome. Malays. Fam. Physician 2008, 3, 128–130. [Google Scholar] [PubMed]
- Klamm, J.; Tarnow, K.G. Computer Vision Syndrome: A Review of Literature. Medsurg Nurs. 2015, 24, 89–93. [Google Scholar] [PubMed]
- Al Tawil, L.; Aldokhayel, S.; Zeitouni, L.; Qadoumi, T.; Hussein, S.; Ahamed, S.S. Prevalence of Self-Reported Computer Vision Syndrome Symptoms and Its Associated Factors Among University Students. Eur. J. Ophthalmol. 2020, 30, 189–195. [Google Scholar] [CrossRef]
- Rosenfield, M. Computer Vision Syndrome: A Review of Ocular Causes and Potential Treatments. Ophthalmic Physiol. Opt. 2011, 31, 502–515. [Google Scholar] [CrossRef]
- Altalhi, A.; Khayyat, W.; Khojah, O.; Alsalmi, M.; Almarzouki, H. Computer Vision Syndrome Among Health Sciences Students in Saudi Arabia: Prevalence and Risk Factors. Cureus 2020, 12, e7060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowatt, L.; Gordon, C.; Santosh, A.B.R.; Jones, T. Computer Vision Syndrome and Ergonomic Practices Among Undergraduate University Students. Int. J. Clin. Pract. 2018, 72, e13035. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Wathurapatha, W.S.; Perera, Y.S.; Lamabadusuriya, D.A.; Kulatunga, S.; Jayawardana, N.; Katulanda, P. Computer Vision Syndrome Among Computer Office Workers in a Developing Country: An Evaluation of Prevalence and Risk Factors. BMC Res. Notes 2016, 9, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wei, X.; Deng, Y. Computer Vision Syndrome During SARS-CoV-2 Outbreak in University Students: A Comparison Between Online Courses and Classroom Lectures. Front. Public Health 2021, 9, 696036. [Google Scholar] [CrossRef] [PubMed]
- OECD. Do Students Spend Enough Time Learning? PISA in Focus, No. 73; OECD Publishing: Paris, France, 2017; pp. 1–6. [Google Scholar]
- Akowuah, P.K.; Nti, A.N.; Ankamah-Lomotey, S.; Frimpong, A.A.; Fummey, J.; Boadi, P.; Osei-Poku, K.; Adjei-Anang, J. Digital Device Use, Computer Vision Syndrome, and Sleep Quality among an African Undergraduate Population. Adv. Public Health 2021, 2021, 6611348. [Google Scholar] [CrossRef]
- Hayes, J.R.; Sheedy, J.E.; Stelmack, J.A.; Heaney, C.A. Computer use, symptoms, and quality of life. Optom. Vis. Sci. 2007, 84, 738–744. [Google Scholar] [CrossRef]
- Li, R.; Ying, B.; Qian, Y.; Chen, D.; Li, X.; Zhu, H.; Liu, H. Prevalence of Self-Reported Symptoms of Computer Vision Syndrome and Associated Risk Factors among School Students in China during the COVID-19 Pandemic. Ophthalmic Epidemiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Sen, P.; Shah, C.; Jain, E.; Jain, S. Prevalence and Risk Factor Assessment of Digital Eye Strain Among Children Using Online E-Learning During the COVID-19 Pandemic: Digital Eye Strain Among Kids (DESK Study-1). Indian J. Ophthalmol. 2021, 69, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Wayne, W.D. Biostatistics: A Foundation of Analysis in the Health Sciences, 6th ed.; John Wiley & Sons: Hoboken, NJ, USA, 1995; p. 180. [Google Scholar]
- Tubtimhin, S.; Puthaburi, N. Prevalence and Severity of Computer Vision Syndrome of Supporting Staff in Ubon Ratchathani University. Srinagarind Med. J. 2019, 34, 173–177. [Google Scholar]
- Chaiear, N.; Buranruk, O.; Pinitsoonthom, S.; Boonma, M.; Leelathanapipat, S.; Sujinprum, C.; Durongkhadet, P.; Leelamanotham, S.; Moonthawee, K. Health Effects of Computer Use Among Thai Commercial Bank Workers, Khon Kaen, Thailand. Srinagarind Med. J. 2005, 20, 3–10. [Google Scholar]
- Sornboot, J.; Phakthongsuk, P.; Thangtrison, S. Prevalence of Visual Fatigue and Its Determinants Among Computer Users in the Faculty of Medicine, Prince of Songkla University. J. Health Sci. Med. Res. 2009, 27, 22–27. [Google Scholar]
- del Mar Seguí, M.; Cabrero-García, J.; Crespo, A.; Verdú, J.; Ronda, E. A Reliable and Valid Questionnaire Was Developed to Measure Computer Vision Syndrome at the Workplace. J. Clin. Epidemiol. 2015, 68, 662–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chidnayee, S.C.J. Risk Factors for Computer Visual Syndrome and Prevalence of Vision Problems in Nursing Students at Borommarajonani College of Nursing, Uttaradit. Nurs. Public Health Educ. J. 2015, 16, 13–22. [Google Scholar]
- Bahkir, F.A.; Grandee, S.S. Impact of the COVID-19 Lockdown on Digital Device-Related Ocular Health. Indian J. Ophthalmol. 2020, 68, 2378–2383. [Google Scholar] [CrossRef]
- Galindo-Romero, C.; Ruiz-Porras, A.; García-Ayuso, D.; Di Pierdomenico, J.; Sobrado-Calvo, P.; Valiente-Soriano, F.J. Computer Vision Syndrome in the Spanish Population during the COVID-19 Lockdown. Optom. Vis. Sci. 2021, 98, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-M.; Chang, D.S.-T.; Wu, P.-C. The Association between Near Work Activities and Myopia in Children-A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140419. [Google Scholar] [CrossRef] [Green Version]
- Pärssinen, O.; Kauppinen, M.; Viljanen, A. The Progression of Myopia from Its Onset at Age 8–12 to Adulthood and the Influence of Heredity and External Factors on Myopic Progression: A 23-Year Follow-up Study. Acta Ophthalmol. 2014, 92, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Computers, Digital Devices and Eye Strain (Blog). American Academy of Ophthalmology. 2020. Available online: https://www.aao.org/eye-health/tips-prevention/computer-usage (accessed on 17 October 2021).
- Han, C.C.; Liu, R.; Liu, R.R.; Zhu, Z.H.; Yu, R.B.; Ma, L. Prevalence of Asthenopia and Its Risk Factors in Chinese College Students. Int. J. Ophthalmol. 2013, 6, 718–722. [Google Scholar] [PubMed] [Green Version]
- Alabdulkader, B. Effect of Digital Device use During COVID-19 on Digital Eye Strain. Clin. Exp. Optom. 2021, 104, 698–704. [Google Scholar] [CrossRef]
- Zayed, H.A.M.; Saied, S.M.; Younis, E.A.; Atlam, S.A. Digital Eye Strain: Prevalence and Associated Factors Among Information Technology Professionals, Egypt. Environ. Sci. Pollut. Res. 2021, 28, 25187–25195. [Google Scholar] [CrossRef] [PubMed]
- Sheedy, J.E.; Smith, R.; Hayes, J. Visual Effects Of The Luminance Surrounding a Computer Display. Ergonomics 2005, 48, 1114–1128. [Google Scholar] [CrossRef] [PubMed]
- Hultgren, G.V.; Knave, B. Discomfort Glare and Disturbances from Light Reflections in an Office Landscape with CRT Display Terminals. Appl. Ergon. 1974, 5, 2–8. [Google Scholar] [CrossRef]
- Sheedy, J.E.; Hayes, J.N.; Engle, J. Is all Asthenopia the Same? Optom. Vis. Sci. 2003, 80, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Gowrisankaran, S.; Sheedy, J.E.; Hayes, J.R. Eyelid Squint Response to Asthenopia-Inducing Conditions. Optom. Vis. Sci. 2007, 84, 611–619. [Google Scholar] [CrossRef]
- Miyao, M.; Hacisalihzade, S.S.; Allen, J.S.; Stark, L.W. Effects of VDT Resolution on Visual Fatigue and Readability: An Eye Movement Approach. Ergonomics 1989, 32, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Matossian, C.; McDonald, M.; Donaldson, K.E.; Nichols, K.K.; MacIver, S.; Gupta, P.K. Dry Eye Disease: Consideration for Women’s Health. J. Women’s Health 2019, 28, 502–514. [Google Scholar] [CrossRef]
- Lurati, A.R. Computer Vision Syndrome: Implications for the Occupational Health Nurse. Workplace Health Saf. 2018, 66, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A.; Modugno, R.L.; Salami, E. Allergy and Dry Eye Disease. Ocul. Immunol. Inflamm. 2021, 29, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Ruktrakulvitaya, T.; Silawan, T.; Chaoratanakavi, S.; Tongkeo, T.; Santiparp, P. The Prevalence of Refractive Errors and Corrected Refractive Errors of Secondary School Students in Muang District, Pathumthani Province. Acad. J. Community Public Health 2021, 7, 60–73. [Google Scholar]
- Jenchitr, W.; Raiyawa, S. Refractive Errors: The Major Visual Impairment in Thailand. Rangsit J. Arts Sci. 2012, 2, 133–141. [Google Scholar]
- Wiggins, N.P.; Daum, K.M. Visual Discomfort and Astigmatic Refractive Errors in VDT Use. J. Am. Optom. Assoc. 1991, 62, 680–684. [Google Scholar]
- Wiggins, N.P.; Daum, K.M.; Snyder, C.A. Effects of Residual Astigmatism in Contact Lens Wear on Visual Discomfort in VDT Use. J. Am. Optom. Assoc. 1992, 63, 177–181. [Google Scholar]
- Rosenfield, M.; Hue, J.E.; Huang, R.R.; Bababekova, Y. The Effects of Induced Oblique Astigmatism on Symptoms and Reading Performance While Viewing a Computer Screen. Ophthalmic Physiol. Opt. 2012, 32, 142–148. [Google Scholar] [CrossRef]
- Wang, L.L.; Wang, W.; Han, X.T.; He, M.G. Influence of Severity and Types of Astigmatism on Visual Acuity in School-Aged Children in Southern China. Int. J. Ophthalmol. 2018, 11, 1377–1383. [Google Scholar] [PubMed]
- Bababekova, Y.; Rosenfield, M.; Hue, J.E.; Huang, R.R. Font Size and Viewing Distance of Handheld Smart Phones. Optom. Vis. Sci. 2011, 88, 795–797. [Google Scholar] [CrossRef] [Green Version]
- Bilton, N. I Live in the Future & Here’s How It Works; Crown Business: New York, NY, USA, 2010. [Google Scholar]
- Long, J.; Cheung, R.; Duong, S.; Paynter, R.; Asper, L. Viewing Distance and Eyestrain Symptoms with Prolonged Viewing of Smartphones. Clin. Exp. Optom. 2017, 100, 133–137. [Google Scholar] [CrossRef]
- Tribley, J.; McClain, S.; Karbasi, A.; Kaldenberg, J. Tips For Computer Vision Syndrome Relief and Prevention. Work 2011, 39, 85–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blehm, C.; Vishnu, S.; Khattak, A.; Mitra, S.; Yee, R.W. Computer Vision Syndrome: A Review. Surv. Ophthalmol. 2005, 50, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Osterhaus, W.K.E.; Bailey, I.L. Large area glare sources and their effect on discomfort and visual performance at computer workstations. In Proceedings of the 1992 IEEE Industry Applications Society Annual Meeting, Houston, TX, USA, 4–9 October 1992; pp. 1–5. [Google Scholar]
- eTools: Computer Workstations-Workstation Environment|Occupational Safety and Health Administration (Blog). Available online: https://www.osha.gov/etools/computer-workstations/workstation-environment (accessed on 13 January 2022).
- Chiemeke, S.C.; Akhahowa, A.E.; Ajayi, O.B. Evaluation of Vision-Related Problems amongst Computer Users: A Case Study of University of Benin, Nigeria. In Proceedings of the World Congress on Engineering, London, UK, 2–4 July 2007. [Google Scholar]
- Photihung, P. Factors related to computer vision syndrome in working group, Thailand: A systematic review of the literature. J. Fac. Nurs. Burapha Univ. 2016, 24, 1–14. [Google Scholar]
- Magno, M.S.; Utheim, T.P.; Snieder, H.; Hammond, C.J.; Vehof, J. The Relationship Between Dry Eye and Sleep Quality. Ocul. Surf. 2021, 20, 13–19. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Factors | CVS (n = 427) | Non-CVS (n = 100) | p-Value | ||
|---|---|---|---|---|---|
| Age, years (mean ± SD) | 19.98 ± 1.62 | 20.55 ± 2.35 | 0.004 ** | ||
| Sex, n (%) | |||||
| Male | 110 | (25.8) | 46 | (46.0) | <0.001 ** |
| Female | 317 | (74.2) | 54 | (54.0) | |
| Atopic diseases, n (%) | 76 | (17.8) | 8 | (8.0) | 0.015 * |
| Prior ocular symptoms, n (%) | 195 | (45.7) | 24 | (24.0) | <0.001 ** |
| Use of dry-eye-associated systemic medications, n (%) | 21 | (4.9) | 2 | (2.0) | 0.279 |
| History of laser refractive surgery, n (%) | 2 | (0.5) | 2 | (2.0) | 0.165 |
| Myopia, n (%) | 275 | (64.4) | 63 | (63.0) | 0.817 |
| Hyperopia, n (%) | 4 | (0.9) | 0 | (0.0) | 0.081 |
| Astigmatism, n (%) | 141 | (33.0) | 22 | (22.0) | 0.041 * |
| All types of refractive error, n (%) | 295 | (69.1) | 65 | (65.0) | 0.474 |
| Glasses wear, n (%) | 273 | (63.9) | 64 | (64.0) | 1.000 |
| Contact lens wear, n (%) | 59 | (13.8) | 17 | (17.0) | 0.430 |
| Artificial tears use, n (%) | 74 | (17.3) | 11 | (11.0) | 0.133 |
| Variables | CVS (n = 427) | Non-CVS (n = 100) | p-Value | ||
|---|---|---|---|---|---|
| Most frequently used types of display, n (%) | |||||
| Tablet | 208 | (48.7) | 57 | (57.0) | 0.086 |
| Mobile phone | 176 | (41.2) | 31 | (31.0) | |
| Laptop | 31 | (7.3) | 6 | (6.0) | |
| Computer | 10 | (2.3) | 5 | (5.0) | |
| Projector | 0 | (0.0) | 1 | (1.0) | |
| Television | 2 | (0.5) | 0 | (0.0) | |
| Distance from display < 20 cm, n (%) | 225 | (52.7) | 40 | (40.0) | 0.026 * |
| Improper display and eye level, n (%) | 238 | (55.7) | 50 | (50.0) | 0.317 |
| Low Screen brightness, n (%) | 63 | (14.8) | 7 | (7.0) | 0.048 * |
| Glare or reflection on display, n (%) | 204 | (47.8) | 29 | (29.0) | 0.001 ** |
| Improper environmental brightness, n (%) | 109 | (25.5) | 23 | (23.0) | 0.701 |
| Difference of brightness between display and surroundings, n (%) | 41 | (9.6) | 5 | (5.0) | 0.170 |
| Unchanging of posture during study, n (%) | 262 | (61.4) | 67 | (67.0) | 0.305 |
| Characteristics | CVS (n = 427) | Non-CVS (n = 100) | p Value |
|---|---|---|---|
| Screen time during online study, hours (mean ± SD) | 8.58 ± 3.81 | 7.92 ± 3.32 | 0.102 |
| Screen time before online study, hours (mean ± SD) | 5.55 ± 2.86 | 6.26 ± 3.31 | 0.031 * |
| Increment of screen usage time during online study, hours (median, IQR) | 3 (0–3) | 2 (1–5) | <0.001 ** |
| Rest interval during study, minutes (median, IQR) | 10 (3–20) | 10 (5–15) | 0.372 |
| Rest frequency during study, times (median, IQR) | 2 (0–3) | 2 (0–3) | 0.962 |
| Feeling adequate of break time between classes, n (%) | 55 (12.9) | 39 (39.0) | <0.001 ** |
| Sleep duration per day, hours (mean ± SD) | 6.33 ± 1.17 | 6.63 ± 1.33 | 0.027 * |
| Factors | Crude OR | 95% CI | p Value |
|---|---|---|---|
| Systemic factors | |||
| Female | 2.45 | 1.57–3.85 | <0.001 ** |
| Age | 0.86 | 0.76–0.96 | 0.010 * |
| Atopic diseases | 2.49 | 1.16–5.34 | 0.020 * |
| Administration of systemic-medication related dry eye | 2.53 | 0.58–10.99 | 0.214 |
| Ocular factors | |||
| Prior ocular symptoms | 2.66 | 1.62–4.37 | <0.001 ** |
| Laser refractive surgery | 0.23 | 0.03–1.66 | 0.145 |
| Artificial tears use | 1.70 | 0.86–3.33 | 0.125 |
| Myopia | 1.06 | 0.68–1.67 | 0.792 |
| Astigmatism | 1.75 | 1.05–2.92 | 0.033 * |
| Eyeglasses use | 1.00 | 0.63–1.57 | 0.990 |
| Contact lenses use | 0.78 | 0.43–1.41 | 0.416 |
| Display and environment | |||
| Mobile phone use | 1.56 | 0.98–2.49 | 0.061 |
| Glare or reflection on screen | 2.24 | 1.40–3.59 | <0.001 ** |
| Improper environmental brightness | 1.15 | 0.69–1.92 | 0.600 |
| Low screen brightness | 2.30 | 1.02–5.19 | 0.045 * |
| Different brightness between display and surrounding | 2.02 | 0.78–5.24 | 0.150 |
| Behaviors | |||
| Distance from screen < 20 cm | 1.67 | 1.07–2.60 | 0.023 * |
| Proper display and eye level | 1.26 | 0.81–1.95 | 0.300 |
| Changing body posture | 1.28 | 0.81–2.03 | 0.295 |
| Duration of rest during study | 1.00 | 0.99–1.01 | 0.703 |
| Sleeping duration | 0.82 | 0.68–0.98 | 0.030 * |
| Inadequate break time between classes | 4.32 | 2.65–7.07 | <0.001 ** |
| Increased screen time usage during online study | 1.12 | 1.06–1.20 | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wangsan, K.; Upaphong, P.; Assavanopakun, P.; Sapbamrer, R.; Sirikul, W.; Kitro, A.; Sirimaharaj, N.; Kuanprasert, S.; Saenpo, M.; Saetiao, S.; et al. Self-Reported Computer Vision Syndrome among Thai University Students in Virtual Classrooms during the COVID-19 Pandemic: Prevalence and Associated Factors. Int. J. Environ. Res. Public Health 2022, 19, 3996. https://doi.org/10.3390/ijerph19073996
Wangsan K, Upaphong P, Assavanopakun P, Sapbamrer R, Sirikul W, Kitro A, Sirimaharaj N, Kuanprasert S, Saenpo M, Saetiao S, et al. Self-Reported Computer Vision Syndrome among Thai University Students in Virtual Classrooms during the COVID-19 Pandemic: Prevalence and Associated Factors. International Journal of Environmental Research and Public Health. 2022; 19(7):3996. https://doi.org/10.3390/ijerph19073996
Chicago/Turabian StyleWangsan, Kampanat, Phit Upaphong, Pheerasak Assavanopakun, Ratana Sapbamrer, Wachiranun Sirikul, Amornphat Kitro, Naphasorn Sirimaharaj, Sawita Kuanprasert, Maneekarn Saenpo, Suchada Saetiao, and et al. 2022. "Self-Reported Computer Vision Syndrome among Thai University Students in Virtual Classrooms during the COVID-19 Pandemic: Prevalence and Associated Factors" International Journal of Environmental Research and Public Health 19, no. 7: 3996. https://doi.org/10.3390/ijerph19073996
APA StyleWangsan, K., Upaphong, P., Assavanopakun, P., Sapbamrer, R., Sirikul, W., Kitro, A., Sirimaharaj, N., Kuanprasert, S., Saenpo, M., Saetiao, S., & Khamphichai, T. (2022). Self-Reported Computer Vision Syndrome among Thai University Students in Virtual Classrooms during the COVID-19 Pandemic: Prevalence and Associated Factors. International Journal of Environmental Research and Public Health, 19(7), 3996. https://doi.org/10.3390/ijerph19073996