
The Influence of Research Follow-Up during COVID-19 Pandemic on Mental Distress and Resilience: A Multicenter Cohort Study of Treatment-Resistant Depression

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Demographic Information
2.2.2. The Five-Item Brief Symptom Rating Scale (BSRS-5)
2.2.3. The Nine-Item Concise Mental Health Checklist (CMHC-9)
2.2.4. The Brief Resilient Coping Scale (BRCS)
2.3. Study Procedure
2.4. Statistical Analysis
3. Results
3.1. The Participants’ Demographics
3.2. Suicide Risk Factors of the Participants at Baseline Interview
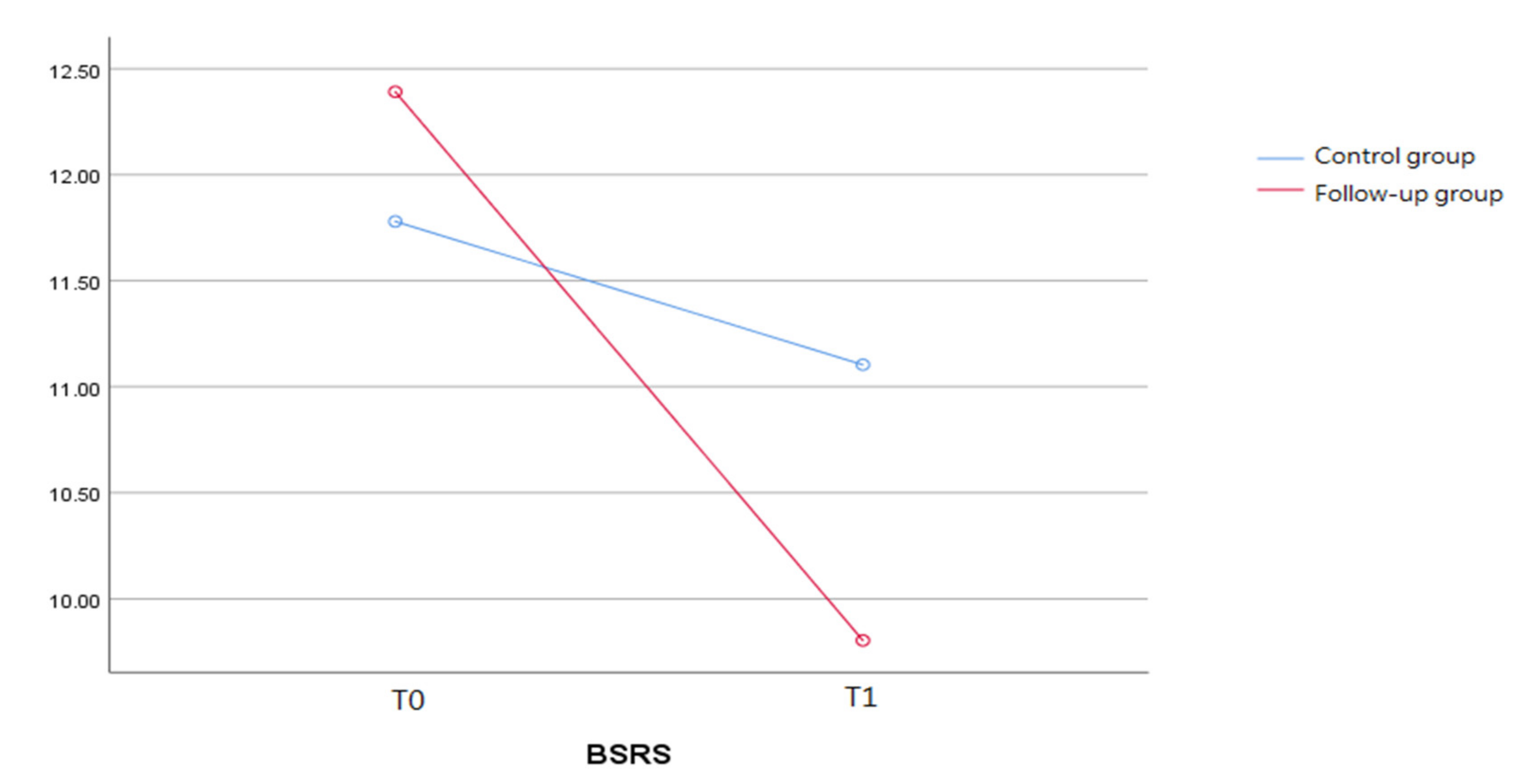
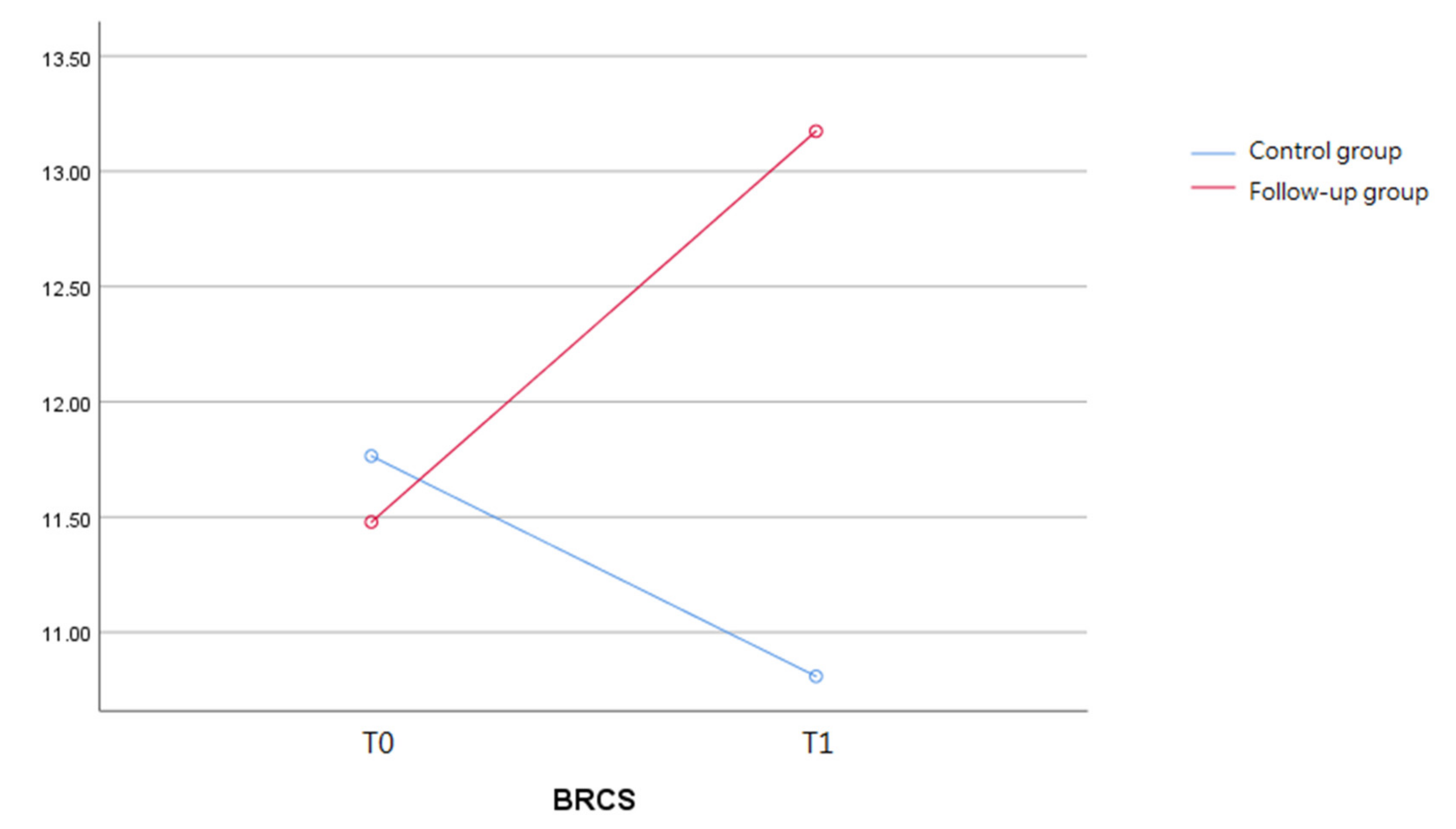
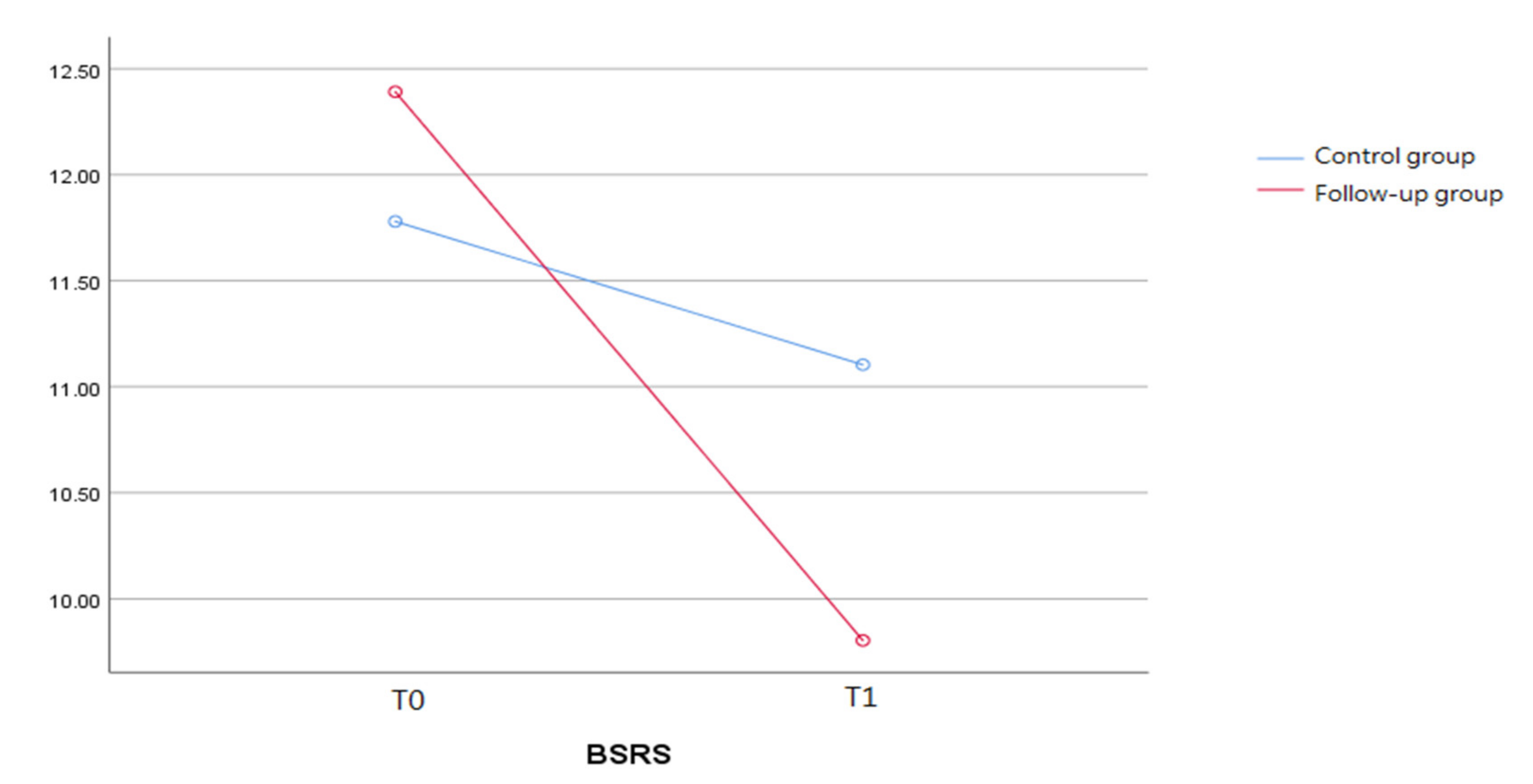
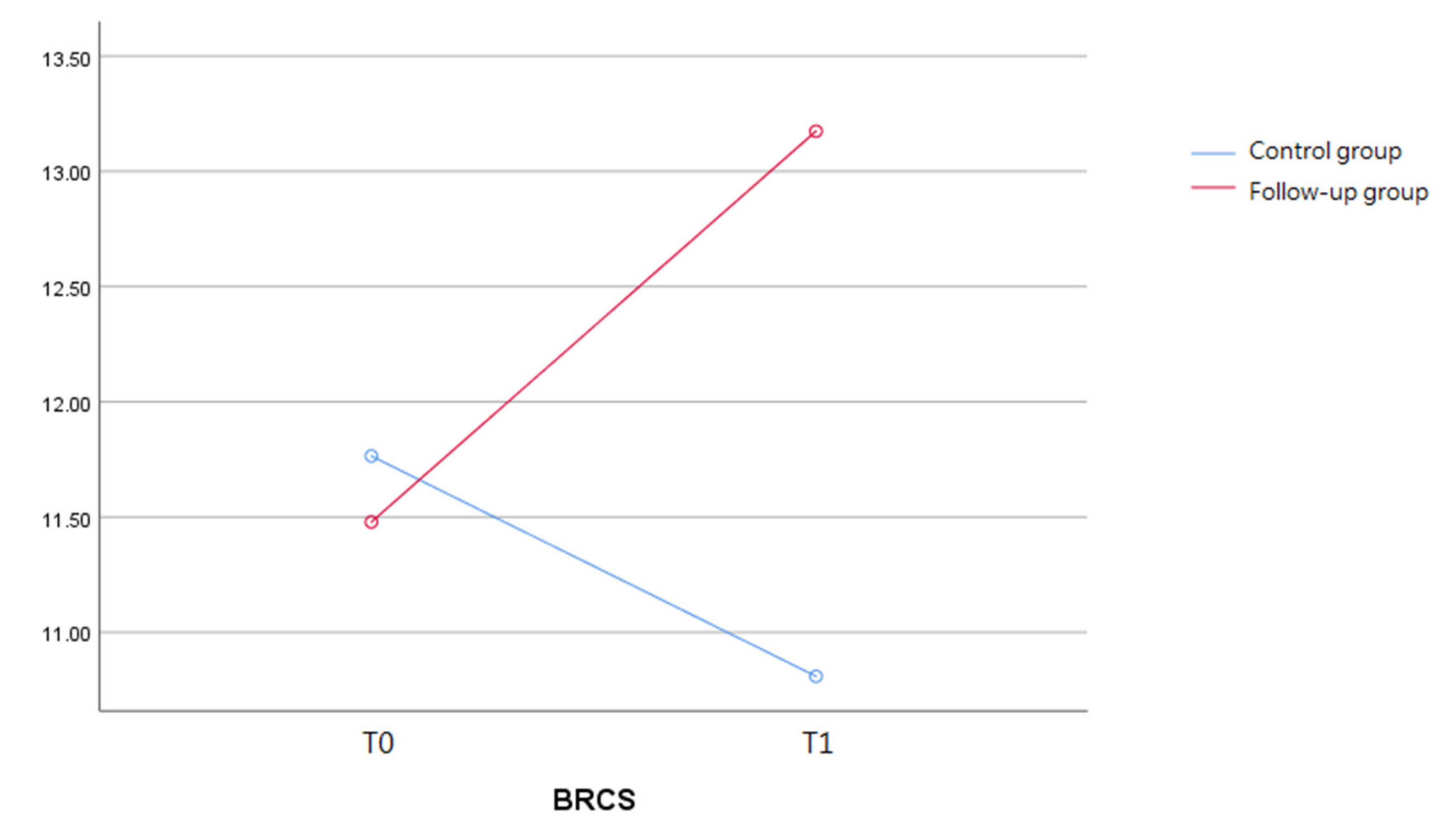
3.3. Trend of Mental Distress and Resilience before and after the COVID-19 Outbreak
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef]
- Tsay, S.F.; Kao, C.C.; Wang, H.H.; Lin, C.C. Nursing’s response to COVID-19: Lessons learned from SARS in Taiwan. Int. J. Nurs. 2020, 108, 103587. [Google Scholar] [CrossRef]
- Chen, Y.L.; Hsu, F.M.; Tsai, C.J.; Cheng, J.C.H. Efforts to reduce the impact of Coronavirus disease 2019 outbreak on radiation oncology in Taiwan. Adv. Radiat. Oncol. 2020, 5, 534–537. [Google Scholar] [CrossRef]
- Lee, I.K.; Wang, C.C.; Lin, M.C.; Kung, C.T.; Lan, K.C.; Lee, C.T. Effective strategies to prevent coronavirus disease-2019 (COVID-19) outbreak in hospital. J. Hosp. Infect. 2020, 105, 102–103. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, S.; Mendoza, J.; Tabatabaei-Jafari, H.; Pandemic-Mental Health International Network (Pan-MHIN); Salvador-Carulla, L. International experiences of the active period of COVID-19—Mental health care. Health Policy Technol. 2020, 9, 503–509. [Google Scholar] [CrossRef]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249–250. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Usher, K.; Durkin, J.; Bhullar, N. The COVID-19 pandemic and mental health impacts. Int. J. Ment. Health Nurs. 2020, 29, 315–318. [Google Scholar] [CrossRef] [Green Version]
- Dong, Z.; Ma, J.; Hao, Y.; Shen, X.; Liu, F.; Gao, Y.; Zhang, L. The social psychological impact of the COVID-19 pandemic on medical staff in China: A cross-sectional study. Eur. Psychiatry 2020, 63, e65. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polizzi, C.; Lynn, S.J.; Perry, A. Stress and coping in the time of COVID-19: Pathways to resilience and recovery. Clin. Neuropsychiatry 2020, 17, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Criss, M.; Pettit, G.; Bates, J.; Dodge, K.; Lapp, A. Family adversity, positive peer relationships & children’s externalising behavior: A longitudinal perspective on risk and resilience. Child Dev. 2002, 3, 1220–1237. [Google Scholar] [CrossRef]
- PeConga, E.K.; Gauthier, G.M.; Holloway, A.; Walker, R.S.W.; Rosencrans, P.L.; Zoellner, L.A.; Bedard-Gilligan, M. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychol. Trauma 2020, 12, S47–S48. [Google Scholar] [CrossRef]
- Shrivastava, A.; Desousa, A. Resilience: A psychobiological construct for psychiatric disorders. Ind. J. Psychiatry 2016, 58, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.; Wang, W.; Ai, M.; Kong, Y.; Chen, J.; Kuang, L. Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: A study of the general population in China at the peak of its epidemic. Soc. Sci. Med. 2020, 262, 113261. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Shi, J.; Ding, H.; Zhang, M.; Kang, C.; Wang, K.; Yu, Y.; Wei, J.; Wang, S.; Shao, N.; et al. Personality traits and depressive symptoms: The moderating and mediating effects of resilience in Chinese adolescents. J. Affect. Disord. 2020, 265, 611–617. [Google Scholar] [CrossRef]
- Kim, S.W.; Su, K.P. Using psychoneuroimmunity against COVID-19. Brain Behav. Immun. 2020, 87, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Zhang, J.; Ren, Y.; Huang, H.; Kauer, A.J.; Liu, Y.; Du, Q.; Jiang, T.; Du, B. Timely psychological care for patients with severe mental illness during COVID-19 epidemic. Asian J. Psychiatr. 2020, 52, 102178. [Google Scholar] [CrossRef]
- Gaynes, B.N.; Lux, L. Defining treatment-resistant depression. Depress Anxiety 2020, 37, 134–145. [Google Scholar] [CrossRef]
- Al-Harbi, K.S. Treatment-resistant depression: Therapeutic trends, challenges, and future directions. Patient Prefer. Adherence 2012, 6, 369–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dena, H.J.; Benoit, R.; Tom, R.D. The humanistic and economic burden of treatment-resistant depression in Europe: A cross-sectional study. BMC Psychiatry 2019, 19, 247. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Fife, D.; Wang, G.; Sheehan, J.J.; Bodén, R.; Brandt, L.; Brenner, P.; Reutfors, J.; DiBernardo, A. All-cause mortality in patients with treatment-resistant depression: A cohort study in the US population. Ann. Gen. Psychiatry 2019, 30, 18–23. [Google Scholar] [CrossRef]
- Reutfors, J.; Andersson, T.M.L.; Tanskanen, A.; DiBernardo, A.; Li, G.; Brandt, L.; Brenner, P. Risk factors for suicide and suicide attempts among patients with treatment-resistant depression: Nested case-control study. Arch. Suicide Res. 2021, 25, 424–438. [Google Scholar] [CrossRef] [Green Version]
- Edward, K.L. Resilience: A protector from depression. J. Am. Psychiatr. Nurses Assoc. 2005, 11, 241–243. [Google Scholar] [CrossRef]
- Chen, S.C.; Lai, Y.H.; Tsay, S.L. Nursing perspectives on the impacts of COVID-19. J. Nurs. Res. 2020, 28, e85. [Google Scholar] [CrossRef]
- Eagle, D.E.; Hybels, C.F.; Proeschold-Bell, R.J. Perceived social support, received social support, and depression among clergy. J. Soc. Pers. Relatsh. 2018, 36, 2055–2073. [Google Scholar] [CrossRef]
- Grey, I.; Arora, T.; Thomas, J.; Saneh, A.; Tomhe, P.; Abi-Habib, R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020, 293, 113452. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Lee, J.I.; Lee, M.B.; Liao, S.C.; Chang, C.M.; Chen, H.C.; Lung, F.W. Predictive validity of a five-item symptom checklist to screen psychiatric morbidity and suicide ideation in general population and psychiatric settings. J. Formos. Med. Assoc. 2016, 115, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.Y.; Lee, M.B.; Lin, Y.Y.; Liao, S.C. Development and validation of the 9-item Concise Mental Health Checklist (CMHC-9) for suicide risk assessment. J. Formos. Med. Assoc. 2019, 118, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, V.G.; Wallston, K.A. The Development and Psychometric Evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Albott, C.S.; Wozniak, J.R.; McGlinch, B.P.; Wall, M.H.; Gold, B.S.; Vinogradov, S. Battle buddies: Rapid deployment of a psychological resilience intervention for health care workers during the COVID-19 pandemic. Anesth. Analg. 2020, 131, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Ho, S.M.; Chan, J.C.; Kwong, R.S.; Cheung, C.K.; Wong, C.P.; Wong, V.C. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: A latent class approach. Health Psychol. 2008, 27, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Kandeğer, A.; Aydın, M.; Altınbaş, K.; Cansız, A.; Tan, Ö.; Tomar Bozkurt, H.; Eğilmez, Ü.; Tekdemir, R.; Şen, B.; Aktuğ Demir, N.; et al. Evaluation of the relationship between perceived social support, coping strategies, anxiety, and depression symptoms among hospitalized COVID-19 patients. Int. J. Psychiatry Med. 2021, 56, 240–254. [Google Scholar] [CrossRef]
- Guo, K.; Zhang, X.; Bai, S.; Minhat, H.S.; Nazan, A.I.N.M.; Feng, J.; Li, X.; Luo, G.; Zhang, X.; Feng, J.; et al. Assessing social support impact on depression, anxiety, and stress among undergraduate students in Shaanxi province during the COVID-19 pandemic of China. PLoS ONE 2021, 16, e0253891. [Google Scholar] [CrossRef]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [Green Version]
- McCambridge, J.; Day, M. Randomized controlled trial of the effects of completing the Alcohol Use Disorders Identification Test questionnaire on self-reported hazardous drinking. Addiction 2008, 103, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Koçak, O.; Koçak, Ö.E.; Younis, M.Z. The psychological consequences of COVID-19 fear and the moderator effects of individuals’ underlying illness and witnessing infected friends and family. Int. J. Environ. Res. Public Health 2021, 18, 1836. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and Coronavirus disease 2019—A perfect storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntyre, R.S.; Lee, Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry 2020, 19, 250–251. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| n (%)/Mean ± SD | Total | FG (n = 46) | CG (n = 68) | X2/t * |
|---|---|---|---|---|
| Age (years) | 56.9 ± 14.4 | 57.6 ± 12.0 | 56.4 ± 15.8 | −0.42 (ns) |
| Educational years | 11.9 ± 4.7 | 11.9 ± 4.3 | 11.9 ± 5.0 | −0.01 (ns) |
| Gender | ||||
| Male | 33 (28.9) | 14 (30.4) | 19 (27.9) | −0.29 (ns) |
| Female | 81 (71.1) | 32 (69.6) | 49 (72.1) | |
| Marital status | ||||
| Single | 22 (19.3) | 9 (19.6) | 13 (19.1) | 1.49 (ns) |
| Married/cohabited | 64 (56.1) | 28 (60.9) | 36 (52.9) | |
| Divorced/separate | 18 (15.8) | 5 (10.9) | 13 (19.1) | |
| Widow | 10 (8.8) | 4 (8.6) | 6 (8.8) | |
| Religion | ||||
| Yes | 86 (75.4) | 35 (76.1) | 51 (75.0) | 0.02 (ns) |
| No | 28 (24.6) | 11 (23.9) | 17 (25.0) | |
| Employment status | ||||
| Yes | 26 (22.8) | 11 (23.9) | 15 (22.1) | 0.05 (ns) |
| No | 88 (77.2) | 35 (76.1) | 53 (77.9) |
| n (%)/Mean ± SD | Total | FG (n = 46) | CG (n = 68) | X2/t * |
|---|---|---|---|---|
| Suicide ideation | ||||
| One Week | 48 (42.0) | 19 (41.3) | 29 (42.6) | 0.02 (ns) |
| Lifetime | 109 (95.6) | 44 (95.7) | 65 (95.6) | −0.02 (ns) |
| Suicide attempt | 0.28 (ns) | |||
| None | 48 (42.1) | 18 (39.1) | 30 (44.1) | |
| Once | 19 (16.7) | 8 (17.4) | 11 (16.2) | |
| Twice or more | 47 (41.2) | 20 (43.5) | 27 (39.7) | |
| Family suicide history | 4.87 (ns) | |||
| None | 80 (70.2) | 37 (80.4) | 43 (63.2) | |
| Suicide attempt | 13 (11.4) | 2 (4.3) | 11 (16.2) | |
| Death from suicide | 21 (18.4) | 7 (15.2) | 14 (20.6) | |
| CMHC-9 | ||||
| Item 1: Insomnia, past week | 53 (46.5) | 23 (50.0) | 30 (44.1) | −0.61 (ns) |
| Item 2: Anxiety, past week | 47 (41.2) | 20 (43.5) | 27 (39.7) | −0.40 (ns) |
| Item 3: Irritability, past week | 54 (47.4) | 21 (45.7) | 33 (48.5) | 0.30 (ns) |
| Item 4: Depressed mood, past week | 62 (54.4) | 23 (50.0) | 39 (57.4) | 0.77 (ns) |
| Item 5: Inferiority, past week | 58 (50.9) | 25 (54.3) | 33 (48.5) | −0.61 (ns) |
| Item 6: Suicide attempt/self-harm, lifetime | 68 (59.6) | 30 (65.2) | 38 (55.9) | −0.99 (ns) |
| Item 7: Alcohol/drug abuse, lifetime | 42 (36.8) | 14 (30.4) | 28 (41.2) | 1.16 (ns) |
| Item 8: Stated future suicide intent | 21 (18.4) | 6 (13.0) | 15 (22.1) | 1.22 (ns) |
| Item 9: Lack of social support | 55 (48.2) | 23 (50.0) | 32 (47.1) | −0.31 (ns) |
| Total | 4.04 ± 2.60 | 4.02 ± 2.85 | 4.04 ± 2.44 | 0.05 (ns) |
| T0 a | T1 | |||||
|---|---|---|---|---|---|---|
| n (%)/Mean ± SD | FG b (n = 46) | CG (n = 68) | X2/t | FG (n = 46) | CG (n = 68) | X2/t |
| BSRS-5 | ||||||
| Total scores | 12.4 ± 6.6 | 11.8 ± 5.9 | −0.52 | 9.8 ± 6.7 | 11.1 ± 7.2 | 0.97 |
| Mental distress levels | ||||||
| Low (0–5) | 8 (17.4) | 11 (16.2) | 0.04 | 15 (32.6) | 21 (30.9) | 7.32 * |
| Moderate (6–9) | 7 (15.2) | 11 (16.2) | 9 (19.6) | 3 (4.4) | ||
| Severe (≥10) | 31 (67.4) | 46 (67.6) | 22 (47.8) | 44 (64.7) | ||
| BRCS | ||||||
| Total scores | 11.5 ± 3.9 | 11.8 ± 3.8 | 3.92 | 13.2 ± 3.3 | 10.8 ± 4.2 | −3.18 ** |
| Resilience levels (tertiles) | ||||||
| Low (4–10) | 18 (39.1) | 25 (36.8) | 0.12 | 10 (21.7) | 30 (44.1) | 6.08 * |
| Medium (11–14) | 19 (41.3) | 28 (41.2) | 19 (41.3) | 21 (30.9) | ||
| High (≥15) | 9 (19.6) | 15 (22.0) | 17 (37.0) | 17 (25.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huong, P.T.T.; Wu, C.-Y.; Lee, M.-B.; Hung, W.-C.; Chen, I.-M.; Chen, H.-C. The Influence of Research Follow-Up during COVID-19 Pandemic on Mental Distress and Resilience: A Multicenter Cohort Study of Treatment-Resistant Depression. Int. J. Environ. Res. Public Health 2022, 19, 3738. https://doi.org/10.3390/ijerph19063738
Huong PTT, Wu C-Y, Lee M-B, Hung W-C, Chen I-M, Chen H-C. The Influence of Research Follow-Up during COVID-19 Pandemic on Mental Distress and Resilience: A Multicenter Cohort Study of Treatment-Resistant Depression. International Journal of Environmental Research and Public Health. 2022; 19(6):3738. https://doi.org/10.3390/ijerph19063738
Chicago/Turabian StyleHuong, Pham Thi Thu, Chia-Yi Wu, Ming-Been Lee, Wei-Chieh Hung, I-Ming Chen, and Hsi-Chung Chen. 2022. "The Influence of Research Follow-Up during COVID-19 Pandemic on Mental Distress and Resilience: A Multicenter Cohort Study of Treatment-Resistant Depression" International Journal of Environmental Research and Public Health 19, no. 6: 3738. https://doi.org/10.3390/ijerph19063738
APA StyleHuong, P. T. T., Wu, C.-Y., Lee, M.-B., Hung, W.-C., Chen, I.-M., & Chen, H.-C. (2022). The Influence of Research Follow-Up during COVID-19 Pandemic on Mental Distress and Resilience: A Multicenter Cohort Study of Treatment-Resistant Depression. International Journal of Environmental Research and Public Health, 19(6), 3738. https://doi.org/10.3390/ijerph19063738