
Experiences of SENSory Relearning of the UPPer Limb (SENSUPP) after Stroke and Perceived Effects: A Qualitative Study

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Research Design
2.2. Participants
2.3. A Brief Description of the SENSUPP Protocol
2.4. Interviews
2.5. Data Analysis
2.6. Ethics
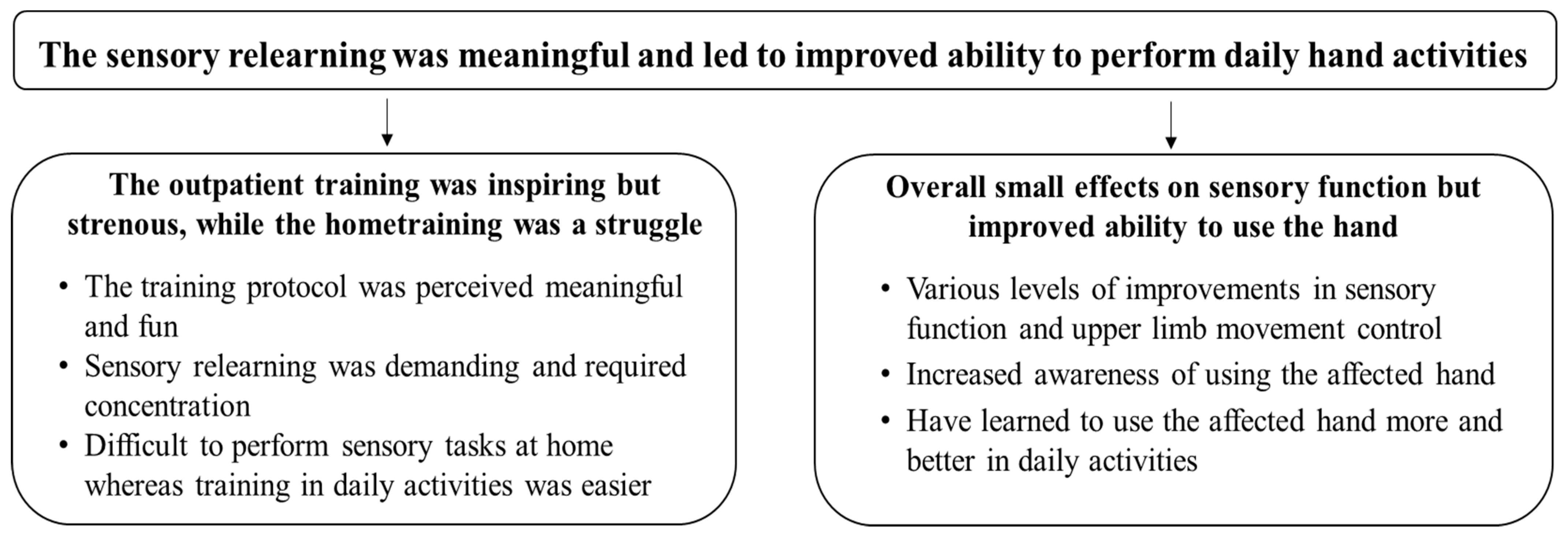
3. Results
3.1. The Outpatient Training Was Inspiring but Strenous, While the Home training Was a Struggle
3.1.1. The Training Protocol Was Perceived Meaningful and Fun
…I thought it was fun, it was fun to come here these days and then [do] the same at home. You feel like you have to keep it up… It was stimulating for the entire psyche and everything, it was…(P15)
Some exercises were more difficult than others and the level of difficulty gradually increased. As I managed the exercise a bit better, they increased it, so it was always at a level… challenging enough to try to feel what kind of object it was.(P4)
…along the way we were given plenty of reminders, I feel. Think about this, do you feel anything, is it heavy or light, is it hot or cold, how does the surface feel on this, we were constantly given reminders to like, raise our awareness…(P5)
3.1.2. Sensory Relearning Was Demanding and Required Concentration
It was strenuous for the brain, trying to categorize what kind of object it was… is it a soft or smooth surface… it was really difficult to push the brain like that, but it was really good.(P4)
…I got to have different objects in my hand without seeing what it was and had to try to identify what it was. It’s really difficult when you can’t manipulate the objects around in your hand and feel it.(P15)
3.1.3. Difficulty in Performing Sensory Tasks at Home, Whereas Training in Daily Activities Was Easier
…I felt like I had no motivation to do it (train at home). I couldn’t really relate it to being meaningful or not, I just felt like I’d rather do something else.(P14)
It should’ve been written down on a piece of paper, so you could see what kind of stuff (exercises) it was… (then) you would’ve put more effort into it to enjoy the training at home.(P9)
3.2. Small Effects Overall on Sensory Function but Improved Ability to Use the Hand
3.2.1. Various Levels of Improvements in Sensory Function and Upper Limb Movement Control
But [the training] has given me.., I could more easily feel things when I grab them. I can feel if I’m grabbing a glass or a loaf of bread, I can connect it in my brain somehow.(P12)
Now, when I’m at a restaurant cutting and such, I don’t need to think that much about how I’m cutting. But at first [before the sensory training], I just ripped it [the piece of meat] apart. …So, something about the training has made me feel like I have better control of how hard to grasp things…(P1)
3.2.2. Increased Awareness of Using the Affected Hand
It feels like the brain is more aware—that now you have to use the left hand too… For example when you grab a plate or turn on the faucet [and you think]: Can you use the left one? …and not only use the right one which is automatically preferred.(P2)
[I think about] making sure that I work a lot more with my right [hand]. I try to open doors with my right [hand], comb my hair with my right [hand], shave with my right [hand], so that I don’t just rely on my left [hand]… it could be better, but I’ve done it a lot more consciously since the training than I did before. But it’s not automatic.(P3)
3.2.3. Learning to Use the Affected Hand More and Better in Daily Activities
…I get things out from the dishwasher, have started combing my hair [with the affected hand], I’m vacuuming with both my hands… I’ve started eating with cutlery in both hands… this thought hadn’t even struck me before, even trying these things.(P11)
4. Discussion
4.1. Methodological Considerations
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Connell, L.A.; Lincoln, N.B.; Radford, K.A. Somatosensory impairment after stroke: Frequency of different deficits and their recovery. Clin. Rehabil. 2008, 22, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Scalha, T.B.; Miyasaki, E.; Lima, N.M.; Borges, G. Correlations between motor and sensory functions in upper limb chronic hemiparetics after stroke. Arq. Neuropsiquiatr. 2011, 69, 624–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socialstyrelsen. Stroke Incidens in Sweden. Available online: http://www.socialstyrelsen.se/globalassets/share-point-dokument/artikelkatalog/statistik/2021-12-7643.pdf.2021 (accessed on 14 March 2022).
- Kessner, S.S.; Schlemm, E.; Cheng, B.; Bingel, U.; Fiehler, J.; Gerloff, C.; Thomalla, G. Somatosensory deficits after ischemic stroke. Stroke 2019, 50, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.A.; Hermsdorfer, J.; Topka, H. Deficits of predictive grip force control during object manipulation in acute stroke. J. Neurol. 2003, 250, 850–860. [Google Scholar] [CrossRef]
- Yekutiel, M. Sensory Re-Education of the Hand after Stroke; Whurr Publishers: London, UK, 2000. [Google Scholar]
- Sullivan, J.E.; Hedman, L.D. Sensory dysfunction following stroke: Incidence, significance, examination, and intervention. Top. Stroke Rehabil. 2008, 15, 200–217. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Baum, C. Effects of somatosensory impairment on participation after stroke. Am. J. Occup. Ther. 2018, 72, 7203205100p1–7203205100p10. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, H.; Gard, G.; Brogardh, C. Upper-limb sensory impairments after stroke: Self-reported experiences of daily life and rehabilitation. J. Rehabil. Med. 2018, 50, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Doyle, S.B.S.; Dudgeon, B.J. Sensory impairment after stroke: Exploring therapists clinical decision making. Can. J. Occup. Ther. 2014, 81, 215–225. [Google Scholar] [CrossRef]
- Connell, L.A.; McMahon, N.E.; Adams, N. Stroke survivors’ experiences of somatosensory impairment after stroke: An Interpretative Phenomenological Analysis. Physiotherapy 2014, 100, 150–155. [Google Scholar] [CrossRef]
- Gopaul, U. Combined somatosensory and motor training to improve upper limb function following stroke: Asystematic scoping review. Phys. Ther. Rev. 2018, 23, 355–375. [Google Scholar] [CrossRef]
- Carey, L.; Macdonell, R.; Matyas, T.A. SENSe: Study of the effectiveness of neurorehabilitation on sensation: A randomized controlled trial. Neurorehabilit. Neural Repair 2011, 25, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Turville, M.L.; Walker, J.; Blennerhassett, J.M.; Carey, L.M. Experiences of upper limb somatosensory retraining in persons with stroke: An interpretative phenomenological analysis. Front. Neurosci. 2019, 13, 756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purves, D. Neuroscience, 6th ed.; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Kessner, S.S.; Bingel, U.; Thomalla, G. Somatosensory deficits after stroke: A scoping review. Top. Stroke Rehabil. 2016, 23, 136–146. [Google Scholar] [CrossRef]
- Normann, B.; Fikke, H.K.; ØBerg, G.K. Somatosensory impairments and upper limb function following stroke: Extending the framework guiding neurological physiotherapy. Eur. J. Physiother. 2015, 17, 81–88. [Google Scholar] [CrossRef]
- Carlsson, H.; Rosen, B.; Pessah-Rasmussen, H.; Bjorkman, A.; Brogardh, C. SENSory re-learning of the UPPer limb after stroke (SENSUPP): Study protocol for a pilot randomized controlled trial. Trials 2018, 19, 229. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, H.; Rosén, B.; Björkman, A.; Pessah-Rasmussen, H.; Brogårdh, C. SENSory re-learning of the UPPer limb (SENSUPP) after stroke: Development and description of a novel intervention using the TIDieR checklist. Trials 2021, 22, 430. [Google Scholar] [CrossRef]
- Carlsson, H.; Rosén, B.; Björkman, A.; Pessah-Rasmussen, H.; Brogårdh, C. Efficacy and feasibility of SENSory relearning of the UPPer limb (SENSUPP) in people with chronic stroke: A pilot randomized controlled trial. PM&R 2022, 1–13. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lindgren, B.M.; Lundman, B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Educ. Today 2017, 56, 29–34. [Google Scholar] [CrossRef]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitago, T.; Krakauer, J.W. Motor learning principles for neurorehabilitation. Handb. Clin. Neurol. 2013, 110, 93–103. [Google Scholar] [PubMed]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Mulder, T.; Hochstenbach, J. Adaptability and flexibility of the human motor system: Implications for neurological rehabilitation. Neural Plast. 2001, 8, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shumway-Cook, A.; Woollacott, M. Motor Control: Translating Research into Clinical Practice, 4th ed.; Lippincott Williams & Wilkins: Philadeplhia, PA, USA, 2012. [Google Scholar]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Levin, M.F.; Demers, M. Motor learning in neurological rehabilitation. Disabil. Rehabil. 2020, 43, 3445–3453. [Google Scholar] [CrossRef]
- Carey, L.M.; Lamp, G.; Turville, M. The state-of-the-science on somatosensory function and its impact on daily life in adults and older adults, and following stroke: A scoping review. OTJR 2016, 36, 27s–41s. [Google Scholar] [CrossRef]
- Merlo, A.R.; Goodman, A.; McClenaghan, B.A.; Fritz, S.L. Participants’ perspectives on the feasibility of a novel, intensive, task-specific intervention for individuals with chronic stroke: A qualitative analysis. Phys. Ther. 2013, 93, 147–157. [Google Scholar] [CrossRef] [Green Version]
- De Bruyn, N.; Saenen, L.; Thijs, L.; van Gils, A.; Ceulemans, E.; Essers, B.; Lafosse, C.; Michielsen, M.; Beyens, H.; Schillebeeckx, F.; et al. Sensorimotor vs. motor upper limb therapy for patients with motor and somatosensory deficits: A randomized controlled trial in the early rehabilitation phase after stroke. Front. Neurol. 2020, 11, 597666. [Google Scholar] [CrossRef]
- De Diego, C.; Puig, S.; Navarro, X. A sensorimotor stimulation program for rehabilitation of chronic stroke patients. Restor. Neurol. Neurosci. 2013, 31, 361–371. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Meads, H. Stroke survivors’ experiences of upper limb recovery: A systematic review of qualitative studies. Phys. Ther. Rev. 2020, 25, 316–330. [Google Scholar] [CrossRef]
- Bennett, L.; Luker, J.; English, C.; Hillier, S. Stroke survivors’ perspectives on two novel models of inpatient rehabilitation: Seven-day a week individual therapy or five-day a week circuit class therapy. Disabil. Rehabil. 2016, 38, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Mangset, M.; Erling, D.T.; Førde, R.; Wyller, T.B. ‘We’re just sick people, nothing else’: ... factors contributing to elderly stroke patients’ satisfaction with rehabilitation. Clin. Rehabil. 2008, 22, 825–835. [Google Scholar] [CrossRef]
- Ranner, M.; Guidetti, S.; von Koch, L.; Tham, K. Experiences of participating in a client-centred ADL intervention after stroke. Disabil. Rehabil. 2019, 41, 3025–3033. [Google Scholar] [CrossRef] [Green Version]
- Peoples, H.; Satink, T.; Steultjens, E. Stroke survivors’ experiences of rehabilitation: A systematic review of qualitative studies. Scand. J. Occup. Ther. 2011, 18, 163–171. [Google Scholar] [CrossRef]
- Byl, N.; Roderick, J.; Mohamed, O.; Hanny, M.; Kotler, J.; Smith, A.; Tang, M.; Abrams, G. Effectiveness of sensory and motor rehabilitation of the upper limb following the principles of neuroplasticity: Patients stable poststroke. Neurorehabilit. Neural Repair 2003, 17, 176–191. [Google Scholar] [CrossRef]
- Reunanen, M.A.; Järvikoski, A.; Talvitie, U.; Pyöriä, O.; Härkäpää, K. Individualised home-based rehabilitation after stroke in eastern Finland—The client’s perspective. Health Soc. Care Community 2016, 24, 77–85. [Google Scholar] [CrossRef]
- Taule, T.; Strand, L.I.; Skouen, J.S.; Råheim, M. Striving for a life worth living: Stroke survivors’ experiences of home rehabilitation. Scand. J. Caring Sci. 2015, 29, 651–661. [Google Scholar] [CrossRef] [Green Version]
- Van der Lee, J.H.; Wagenaar, R.C.; Lankhorst, G.J.; Vogelaar, T.W.; Deville, W.L.; Bouter, L.M. Forced use of the upper extremity in chronic stroke patients: Results from a single-blind randomized clinical trial. Stroke 1999, 30, 2369–2375. [Google Scholar] [CrossRef]
- Smania, N.; Montagnana, B.; Faccioli, S.; Fiaschi, A.; Aglioti, S.M. Rehabilitation of somatic sensation and related deficit of motor control in patients with pure sensory stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1692–1702. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variables | Values |
|---|---|
| Age | |
| Years; mean (SD) | 59 (11.9) |
| Gender | |
| Male (n) | 10 |
| Female (n) | 5 |
| Time since stroke | |
| Months; mean (SD) | 26.5 (27.5) |
| Type of stroke | |
| Ischemic (n) | 11 |
| Hemorrhage (n) | 4 |
| Side of paresis | |
| Right | 9 |
| Left | 6 |
| Dominant hand affected | |
| Yes | 9 |
| No | 6 |
| Discriminative touch | |
| STI; median (min-max) | 0 (0–4) |
| Gross manual dexterity | |
| BBT; median (min-max) | 28 (1–48) |
| Ability to use the hand in daily activities | |
| MAL AOU; median (min-max) | 2.1 (0.8–4.5) |
| MAL QOM; median (min-max) | 1.7 (0.6–4.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlsson, H.; Lindgren, I.; Rosén, B.; Björkman, A.; Pessah-Rasmussen, H.; Brogårdh, C. Experiences of SENSory Relearning of the UPPer Limb (SENSUPP) after Stroke and Perceived Effects: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 3636. https://doi.org/10.3390/ijerph19063636
Carlsson H, Lindgren I, Rosén B, Björkman A, Pessah-Rasmussen H, Brogårdh C. Experiences of SENSory Relearning of the UPPer Limb (SENSUPP) after Stroke and Perceived Effects: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3636. https://doi.org/10.3390/ijerph19063636
Chicago/Turabian StyleCarlsson, Håkan, Ingrid Lindgren, Birgitta Rosén, Anders Björkman, Hélène Pessah-Rasmussen, and Christina Brogårdh. 2022. "Experiences of SENSory Relearning of the UPPer Limb (SENSUPP) after Stroke and Perceived Effects: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 6: 3636. https://doi.org/10.3390/ijerph19063636
APA StyleCarlsson, H., Lindgren, I., Rosén, B., Björkman, A., Pessah-Rasmussen, H., & Brogårdh, C. (2022). Experiences of SENSory Relearning of the UPPer Limb (SENSUPP) after Stroke and Perceived Effects: A Qualitative Study. International Journal of Environmental Research and Public Health, 19(6), 3636. https://doi.org/10.3390/ijerph19063636