
Prevalence and Risk Factors Associated with Tumors and Other Structural Anomalies in Brain MRI Performed to Rule out Secondary Headache: A Multicenter Observational Study

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
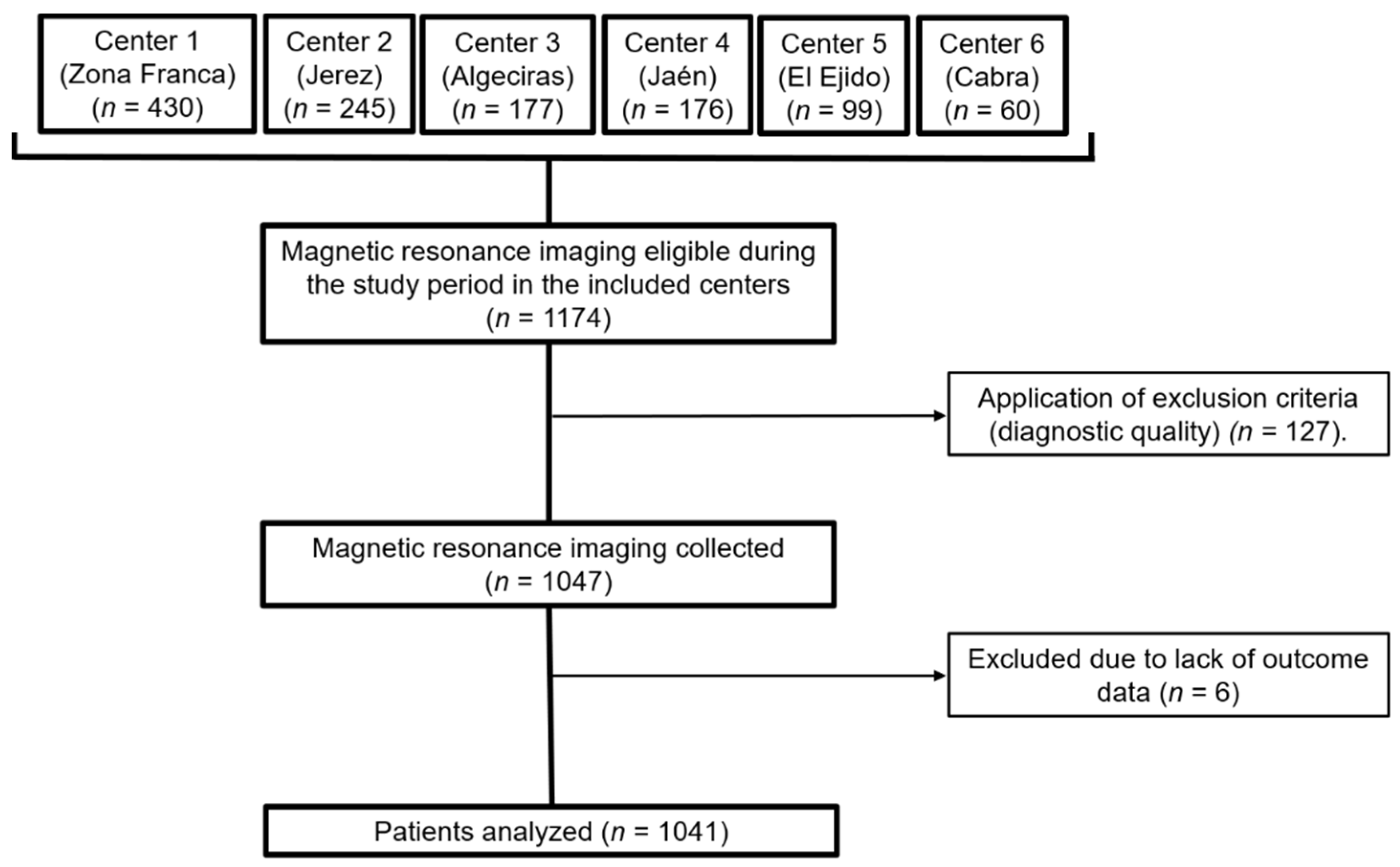
2.1. Study Design and Sample
2.2. Data Collection and Variables
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Headache Disorders; WHO: Rome, Italy, 2016. [Google Scholar]
- Ashina, M.; Katsarava, Z.; Do, T.P.; Buse, D.C.; Pozo-Rosich, P.; Özge, A.; Krymchantowski, A.V.; Lebedeva, E.R.; Ravishankar, K.; Yu, S.; et al. Migraine: Epidemiology and systems of care. Lancet 2021, 397, 1485–1495. [Google Scholar] [CrossRef]
- Negro, A.; Spuntarelli, V.; Sciattella, P.; Martelletti, P. Rapid referral for headache management from emergency department to headache centre: Four years data. J. Headache Pain 2020, 21, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Evans, R.W. Incidental Findings and Normal Anatomical Variants on MRI of the Brain in Adults for Primary Headaches. Headache J. Head Face Pain 2017, 57, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Zareie, A.; Sahebkar, A.; Khorvash, F.; Bagherniya, M.; Hasanzadeh, A.; Askari, G. Effect of cinnamon on migraine attacks and inflammatory markers: A randomized double-blind placebo-controlled trial. Phyther. Res. 2020, 34, 2945–2952. [Google Scholar] [CrossRef]
- Levin, M. Comprehensive Review of Headache Medicine, 1st ed.; Oxford University Press: Cambridge, UK, 2008. [Google Scholar]
- Paniagua Bravo, A.; Albillos Merino, J.C.; Ibáñez Sanz, L.; Alba De Cáceres, I. Análisis de la adecuación de las indicaciones clínicas en los estudios de neurorradiología. Radiologia 2013, 55, 37–45. [Google Scholar] [CrossRef]
- Carville, S.; Padhi, S.; Reason, T.; Underwood, M. Diagnosis and management of headaches in young people and adults: Summary of NICE guidance. BMJ 2012, 345, e5765. [Google Scholar] [CrossRef]
- Whitehead, M.T.; Cardenas, A.M.; Corey, A.S.; Policeni, B.; Burns, J.; Chakraborty, S.; Crowley, R.W.; Jabbour, P.; Ledbetter, L.N.; Lee, R.K.; et al. ACR Appropriateness Criteria® Headache. J. Am. Coll. Radiol. 2019, 16, S364–S377. [Google Scholar] [CrossRef] [Green Version]
- Bestué, M.; Gracia-Naya, M.; Santolaria, L. Reasons for indications neuroimaging studies in the evaluation of primary headache. Rev. Neurol. 2001, 33, 127–130. [Google Scholar] [CrossRef]
- Pérez-Pereda, S.; Madera, J.; González-Quintanilla, V.; Drake-Pérez, M.; Marzal Espí, C.N.; Serrano Munuera, C.; García, S.C.; Aguilella Linares, C.; Fernández Recio, M.; Velamazán Delgado, G.; et al. Is conventional brain MRI useful for the diagnosis of cluster headache in patients who meet ICHD-3 criteria? Experience in three hospitals in Spain. J. Neurol. Sci. 2021, 434, 120122. [Google Scholar] [CrossRef]
- Mullally, W.J.; Hall, K.E. Value of Patient-Directed Brain Magnetic Resonance Imaging Scan with a Diagnosis of Migraine. Am. J. Med. 2018, 131, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, P.; Friedman, D.I. Neuroimaging in Secondary Headache Disorders. Curr. Pain Headache Rep. 2015, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Okagaki, J.F. Practice parameter: The utility of neuroimaging in the evaluation of headache in patients with normal neurologic examinations (summary statement). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1994, 44, 1353–1354. [Google Scholar] [CrossRef]
- Pfund, Z.; Szapáry, L.; Jászberényi, O.; Nagy, F.; Czopf, J. Headache in intracranial tumors. Cephalalgia 1999, 19, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Cote, D.J.; Laws, E.R.; Chicoine, M.; Hawlasi, A.; Dacey, R.G. The Ethics of “Choosing Wisely”: The Use of Neuroimaging for Uncomplicated Headache. Neurosurgery 2017, 80, 816–819. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Howard, L.; Wessely, S.; Leese, M.; Page, L.; McCrone, P.; Husain, K.; Tong, J.; Dowson, A. Are investigations anxiolytic or anxiogenic? A randomised controlled trial of neuroimaging to provide reassurance in chronic daily headache. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1558–1564. [Google Scholar] [CrossRef]
- Kuruvilla, D.E.; Lipton, R.B. Appropriate Use of Neuroimaging in Headache. Curr. Pain Headache Rep. 2015, 19, 1–7. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Kerber, K.A.; Pace, R.J.; Skolarus, L.E.; Burke, J.F. Headaches and Neuroimaging: High Utilization and Costs Despite Guidelines. JAMA Intern. Med. 2014, 174, 819. [Google Scholar] [CrossRef] [Green Version]
- Eller, M.; Goadsby, P.J. MRI in headache. Expert Rev. Neurother. 2013, 13, 263–273. [Google Scholar] [CrossRef]
- Sempere, A.P.; Porta-Etessama, J.; Medrano, V.; Garcia-Morales, I.; Concepcións, L.; Ramos, A.; Florencio, I.; Bermejo, F.; Botella, C. Neuroimaging in the evaluation of patients with non-acute headache. Cephalalgia 2005, 25, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Z.; Simonson, T.M.; Greco, W.R.; Yuh, W.T.C. Brain MR imaging in the evaluation of chronic headache in patients without other neurologic symptoms. Acad. Radiol. 2001, 8, 405–408. [Google Scholar] [CrossRef]
- Mazzotta, G.; Floridi, F.; Mattioni, A.; D’Angelo, R.; Gallai, B. The role of neuroimaging in the diagnosis of headache in childhood and adolescence: A multicentre study. Neurol. Sci. 2004, 25, s265–s266. [Google Scholar] [CrossRef] [PubMed]
- De Benedittis, G.; Lorenzetti, A.; Sina, C.; Bernasconi, V. Magnetic resonance imaging in migraine and tension-type headache. Headache 1995, 35, 264–268. [Google Scholar] [CrossRef]
- Aaseth, K.; Grande, R.B.; Kværner, K.J.; Gulbrandsen, P.; Lundqvist, C.; Russell, M.B. Prevalence of secondary chronic headaches in a population-based sample of 30-44-year-old persons. The Akershus study of chronic headache. Cephalalgia 2008, 28, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Morris, Z.; Whiteley, W.N.; Longstreth, W.T.; Weber, F.; Lee, Y.C.; Tsushima, Y.; Alphs, H.; Ladd, S.C.; Warlow, C.; Wardlaw, J.M.; et al. Incidental findings on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2009, 339, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartwigsen, G.; Siebner, H.R.; Deuschl, G.; Jansen, O.; Ulmer, S. Incidental findings are frequent in young healthy individuals undergoing magnetic resonance imaging in brain research imaging studies: A prospective single-center study. J. Comput. Assist. Tomogr. 2010, 34, 596–600. [Google Scholar] [CrossRef]
- Reneman, L.; De Win, M.M.L.; Booij, J.; Van Den Brink, W.; Den Heeten, G.J.; Freling, N.; Majoie, C.B.L.M. Incidental head and neck findings on MRI in young healthy volunteers: Prevalence and clinical implications. AJNR. Am. J. Neuroradiol. 2012, 33, 1971–1974. [Google Scholar] [CrossRef] [Green Version]
- Vernooij, M.W.; Ikram, M.A.; Tanghe, H.L.; Vincent, A.J.P.E.; Hofman, A.; Krestin, G.P.; Niessen, W.J.; Breteler, M.M.B.; van der Lugt, A. Incidental findings on brain MRI in the general population. N. Engl. J. Med. 2007, 357, 1821–1828. [Google Scholar] [CrossRef]
- Haberg, A.K.; Hammer, T.A.; Kvistad, K.A.; Rydland, J.; Möller, T.B.; Eikenes, L.; Garseth, M.; Stovner, L.J. Incidental Intracranial Findings and Their Clinical Impact; The HUNT MRI Study in a General Population of 1006 Participants between 50–66 Years. PLoS ONE 2016, 11, e0151080. [Google Scholar] [CrossRef]
- Neff, M. Evidence-Based Guidelines for Neuroimaging in Patients with Nonacute Headache. Am. Fam. Physician 2005, 71, 1219. [Google Scholar]
- Tsushima, Y.; Endo, K. MR imaging in the evaluation of chronic or recurrent headache. Radiology 2005, 235, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.; Mackay, I. Staging in rhinosinusitus. Rhinology 1993, 31, 183–184. [Google Scholar] [PubMed]
- Hopkins, C.; Browne, J.P.; Slack, R.; Lund, V.; Brown, P. The Lund-Mackay staging system for chronic rhinosinusitis: How is it used and what does it predict? Otolaryngol. Head. Neck Surg. 2007, 137, 555–561. [Google Scholar] [CrossRef]
- Valentinis, L.; Tuniz, F.; Valent, F.; Mucchiut, M.; Little, D.; Skrap, M.; Bergonzi, P.; Zanchin, G. Headache attributed to intracranial tumours: A prospective cohort study. Cephalalgia 2010, 30, 389–398. [Google Scholar] [CrossRef]
- Ravn Munkvold, B.K.; Sagberg, L.M.; Jakola, A.S.; Solheim, O. Preoperative and Postoperative Headache in Patients with Intracranial Tumors. World Neurosurg. 2018, 115, e322–e330. [Google Scholar] [CrossRef]
- Kurth, T.; Buring, J.E.; Rist, P.M. Headache, migraine and risk of brain tumors in women: Prospective cohort study. J. Headache Pain 2015, 16, 17–501. [Google Scholar] [CrossRef] [Green Version]
- Palmieri, A.; Valentinis, L.; Zanchin, G. Update on headache and brain tumors. Cephalalgia 2021, 41, 431–437. [Google Scholar] [CrossRef]
- Christiaans, M.H.; Kelder, J.C.; Arnoldus, E.P.J.; Tijssen, C.C. Prediction of intracranial metastases in cancer patients with headache. Cancer 2002, 94, 2063–2068. [Google Scholar] [CrossRef] [Green Version]
- Ozawa, M.; Brennan, P.M.; Zienius, K.; Kurian, K.M.; Hollingworth, W.; Weller, D.; Grant, R.; Hamilton, W.; Ben-Shlomo, Y. The usefulness of symptoms alone or combined for general practitioners in considering the diagnosis of a brain tumour: A case-control study using the clinical practice research database (CPRD) (2000–2014). BMJ Open 2019, 9, e029686. [Google Scholar] [CrossRef] [Green Version]
- Butowski, N.A. Epidemiology and diagnosis of brain tumors. Contin. Lifelong Learn. Neurol. 2015, 21, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Wermuth, P.J.; Jimenez, S.A. Nephrogenic Systemic Fibrosis. Scleroderma Pathog. Compr. Manag. 2021, 137–159. [Google Scholar] [CrossRef]
- Olchowy, C.; Cebulski, K.; Łasecki, M.; Chaber, R.; Olchowy, A.; Kałwak, K.; Zaleska-Dorobisz, U. The presence of the gadolinium-based contrast agent depositions in the brain and symptoms of gadolinium neurotoxicity-A systematic review. PLoS ONE 2017, 12, e0171704. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Characteristic | Total Sample | Structural Finding Explaining Headache | No Structural Finding Explaining Headache | p-Value 1 |
|---|---|---|---|---|
| Total | 1041 (100.0%) | 224 (21.5%) | 817 (78.5%) | - |
| Sex, n (%) | 0.080 | |||
| Women | 728 (69.9%) | 146 (20.1%) | 582 (79.9%) | |
| Men | 313 (30.1%) | 78 (24.9%) | 235 (75.1%) | |
| Age, x (sd) | 38.6 (18.9) | 38.6 (18.8) | 38.6 (18.9) | 0.980 |
| Province, n (%) | 0.200 | |||
| Almería | 88 (8.5%) | 22 (25.0%) | 66 (75.0%) | |
| Cádiz | 748 (71.9%) | 159 (21.3%) | 589 (78.7%) | |
| Córdoba | 53 (5.1%) | 6 (11.3%) | 47 (88.7%) | |
| Jaén | 152 (14.6%) | 37 (24.3%) | 115 (75.7%) | |
| Specialty of ordering physician, n (%) | 0.017 * | |||
| Neurology | 738 (71.0%) | 148 (20.1%) | 590 (79.9%) | |
| Pediatrics | 112 (10.8%) | 29 (25.9%) | 83 (74.1%) | |
| Internal Medicine | 64 (6.2%) | 10 (25.0%) | 54 (75.0%) | |
| Oncology | 29 (2.8%) | 12 (41.4%) | 17 (58.7%) | |
| Primary Care | 24 (2.3%) | 6 (25.0%) | 18 (75.0%) | |
| Neurosurgery | 22 (2.1%) | 9 (40.9) | 13 (59.1%) | |
| Others | 51 (4.9%) | 10 (19.6%) | 41 (80.4%) | |
| Type of headache, n (%) | 0.085 | |||
| Migraine | 225 (21.6%) | 39 (17.3%) | 186 (82.7%) | |
| Other | 816 (78.4%) | 185 (22.7%) | 631 (77.3%) | |
| Contrast (Gadolinium), n (%) | 0.001 * | |||
| Yes | 176 (16.9%) | 55 (31.3%) | 121 (68.8%) | |
| No | 865 (83.1%) | 169 (19.5%) | 696 (80.5%) | |
| New (incident) headache, n (%) | 0.211 | |||
| Yes | 131 (12.6%) | 34 (26.0%) | 97 (74.0%) | |
| No | 910 (87.4%) | 190 (20.9%) | 720 (79.1%) | |
| Concomitant symptoms, n (%) | 0.163 | |||
| Yes | 304 (29.2%) | 57 (18.8%) | 247 (81.3%) | |
| No | 737 (70.8%) | 167 (22.7%) | 570 (77.3%) | |
| Previous trauma, n (%) | 0.572 | |||
| Yes | 27 (2.6%) | 7 (25.9%) | 20 (74.1%) | |
| No | 1104 (97.4%) | 217 (21.4%) | 797 (78.6%) | |
| Previous MRI, n (%) | 0.024 * | |||
| Yes | 151 (14.5%) | 43 (28.5%) | 108 (71.5%) | |
| No | 890 (85.5%) | 181 (20.3%) | 709 (79.7%) | |
| Previous known condition that may justify headache, n (%) | <0.001 * | |||
| Yes | 106 (10.2%) | 41 (38.7%) | 65 (61.3%) | |
| No | 934 (89.8%) | 183 (19.6%) | 751 (80.4%) |
| Characteristic | Presence of SOL | Absence of SOL | p-Value 1 | Presence of IT | Absence of IT | p-Value 2 |
|---|---|---|---|---|---|---|
| Total | 71 (6.8%) | 970 (93.2%) | - | 16 (22.5%) | 55 (77.5%) | - |
| Sex, n (%) | 0.718 | |||||
| Women | 51 (7.0%) | 677 (93.0%) | 13 (25.5%) | 38 (74.5%) | 0.048 * | |
| Men | 20 (6.4%) | 293 (96.3%) | 3 (15.0%) | 17 (85.0%) | ||
| Age, x (sd) | 39.5 (19.3) | 38.5 (18.9) | 0.688 | 40.7 (23.4) | 39.1 (18.2) | 0.778 |
| Province, n (%) | 0.752 | 0.636 | ||||
| Almería | 5 (5.7%) | 83 (94.3%) | 2 (25.0%) | 6 (75.0%) | ||
| Cádiz | 55 (7.4%) | 693 (92.6%) | 12 (21.8%) | 43 (78.2%) | ||
| Córdoba | 3 (5.7%) | 50 (94.3%) | 0 (0.0%) | 3 (100.0%) | ||
| Jaén | 8 (5.3%) | 144 (94.7%) | 2 (25.05%) | 6 (75.0%) | ||
| Specialty of ordering physician, n (%) | 0.493 | 0.241 | ||||
| Neurology | 50 (6.8%) | 688 (93.8%) | 12 (24.0%) | 38 (76.0%) | ||
| Pediatrics | 9 (8.0%) | 103 (92.0%) | 3 (33.3%) | 6 (66.7%) | ||
| Internal Medicine | 5 (7.8%) | 59 (92.2%) | 0 (0.0%) | 5 (100.0%) | ||
| Oncology | 2 (6.9%) | 27 (93.1%) | 1 (50.0%) | 1 (50.0%) | ||
| Primary Care | 1 (4.2%) | 23 (95.8%) | 0 (0.0%) | 1 (100.0%) | ||
| Neurosurgery | 1 (4.5%) | 21 (93.2%) | 0 (0.0%) | 1 (100.0%) | ||
| Others | 3 (5.9%) | 48 (94.1%) | 0 (0.0%) | 3 (100.0%) | ||
| Type of headache, n (%) | 0.918 | 0.452 | ||||
| Migraine | 15 (6.7%) | 210 (93.3%) | 4 (26.7%) | 11 (73.3%) | ||
| Others | 56 (6.9%) | 760 (93.1%) | 12 (21.4%) | 44 (78.6%) | ||
| Contrast (Gadolinium), n (%) | 0.511 | 0.836 | ||||
| Yes | 10 (5.7%) | 166 (94.3%) | 2 (20.0%) | 8 (80.0%) | ||
| No | 61 (7.1%) | 804 (92.9%) | 14 (23.0%) | 47 (77.0%) | ||
| New (incident) headache, n (%) | 0.981 | 0.981 | ||||
| Yes | 9 (6.9%) | 122 (93.1%) | 2 (22.2%) | 7 (77.8%) | ||
| No | 62 (6.8%) | 848 (93.2%) | 14 (22.6%) | 48 (77.4%) | ||
| Concomitant symptoms, n (%) | 0.249 | 0.417 | ||||
| Yes | 25 (8.2%) | 279 (91.8%) | 9 (36.0%) | 16 (64.0%) | 0.033 * | |
| No | 46 (6.2%) | 691 (93.8%) | 7 (15.2%) | 39 (84.8%) | ||
| Trauma, n (%) | 0.439 | 0.225 | ||||
| Yes | 1 (3.7%) | 26 (96.3%) | 1 (100.0%) | 0 (0.0%) | ||
| No | 70 (6.9%) | 944 (93.1%) | 15 (21.4%) | 55 (78.6%) | ||
| Previous MRI, n (%) | 0.133 | 0.719 | ||||
| Yes | 6 (4.0%) | 145 (96.0%) | 1 (16.7%) | 5 (83.3%) | ||
| No | 65 (7.3%) | 825 (92.7%) | 15 (23.1%) | 50 (76.9%) | ||
| Previous known condition that may justify the headache, n (%) | 0.188 | 0.903 | ||||
| Yes | 4 (3.8%) | 102 (96.2%) | 1 (25.0%) | 3 (75.0%) | ||
| No | 67 (7.2%) | 867 (92.8%) | 15 (22.4%) | 52 (77.6%) |
| Concomitant Symptoms | n (%) from the Total Sample (n = 1041) | % from the Patients with Concomitant Symptoms (n = 100) | * |
|---|---|---|---|
| None | 737 (70.8) | - | 0.184 |
| ≥1 symptom | 304 (29.2) | - | |
| Visual disturbances | 89 (8.9) | 29.3 | 0.594 |
| Vertigo or dizziness | 58 (5.6) | 19.1 | 0.324 |
| Paresthesia | 58 (5.6) | 19.1 | 0.407 |
| Instability | 28 (2.7) | 9.2 | 0.372 |
| Non-cardiogenic syncope | 18 (1.7) | 5.9 | - |
| Disorientation or memory disturbance | 17 (1.6) | 5.6 | - |
| Motor impairment or movement disorders | 13 (1.3) | 4.3 | - |
| Tinnitus | 12 (1.1) | 3.9 | - |
| Epileptic seizures | 10 (1.0) | 3.3 | - |
| Hypoacusis | 1 (0.1) | 0.3 | - |
| Variables | Crude OR (95% CI) | Adjusted OR 1 (95% CI) |
|---|---|---|
| Sex (female) | 1.32 (0.97–1.81) | 1.35 (1.02–1.85) * |
| Age | 1.00 (0.99–1.01) | 0.99 (0.98–1.01) |
| Type of headache (non-migraine) | 1.40 (0.95–2.05) | 1.27 (0.86–1.88) |
| Use of contrast (gadolinium) | 1.88 (1.31–2.68) | 1.89 (1.31–2.72) * |
| Presence of accompanying symptoms | 1.27 (0.91–1.78) | 1.34 (1.05–1.89) * |
| Previous MRI | 1.56 (1.06–2.30) | 1.25 (0.82–1.90) |
| Previously known condition potentially explaining headache | 2.59 (1.70–3.95) | 2.44 (1.55–3.84) * |
| Structural Abnormalities | n (%) |
|---|---|
| Total | 224 (100.0) |
| Non-space-occupying lesions | 153 (68.3) |
| Sinusitis | 119 (53.1) |
| Chiari malformation | 10 (4.5) |
| Non-communicating hydrocephalus | 8 (3.6) |
| Pseudotumor cerebri | 7 (3.1) |
| Dural sinus thrombosis | 5 (2.2) |
| Arteriovenous malformation | 2 (0.9) |
| Subacute stroke | 2 (0.9) |
| Space-occupying lesions | 71 (31.7) |
| Arachnoid cyst | 32 (14.3) |
| Subdural hygroma | 8 (3.6) |
| Aneurism | 4 (1.8) |
| Cavernoma | 4 (1.8) |
| Epidermoid cyst | 3 (1.3) |
| Chronic subdural hematoma | 2 (0.9) |
| Intraparenchymal hematoma | 1 (0.4) |
| Subdural empyema | 1 (0.4) |
| Intracranial tumors | 16 (7.1) |
| Meningioma | 7 (3.1) |
| Metastasis | 7 (3.1) |
| Glioma | 2 (0.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez Barbero, J.P.; Láinez Ramos-Bossini, A.J.; Rivera-Izquierdo, M.; Sendra-Portero, F.; Benítez-Sánchez, J.M.; Cervilla, J.A. Prevalence and Risk Factors Associated with Tumors and Other Structural Anomalies in Brain MRI Performed to Rule out Secondary Headache: A Multicenter Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 3521. https://doi.org/10.3390/ijerph19063521
Martínez Barbero JP, Láinez Ramos-Bossini AJ, Rivera-Izquierdo M, Sendra-Portero F, Benítez-Sánchez JM, Cervilla JA. Prevalence and Risk Factors Associated with Tumors and Other Structural Anomalies in Brain MRI Performed to Rule out Secondary Headache: A Multicenter Observational Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3521. https://doi.org/10.3390/ijerph19063521
Chicago/Turabian StyleMartínez Barbero, José Pablo, Antonio Jesús Láinez Ramos-Bossini, Mario Rivera-Izquierdo, Francisco Sendra-Portero, José Manuel Benítez-Sánchez, and Jorge A. Cervilla. 2022. "Prevalence and Risk Factors Associated with Tumors and Other Structural Anomalies in Brain MRI Performed to Rule out Secondary Headache: A Multicenter Observational Study" International Journal of Environmental Research and Public Health 19, no. 6: 3521. https://doi.org/10.3390/ijerph19063521
APA StyleMartínez Barbero, J. P., Láinez Ramos-Bossini, A. J., Rivera-Izquierdo, M., Sendra-Portero, F., Benítez-Sánchez, J. M., & Cervilla, J. A. (2022). Prevalence and Risk Factors Associated with Tumors and Other Structural Anomalies in Brain MRI Performed to Rule out Secondary Headache: A Multicenter Observational Study. International Journal of Environmental Research and Public Health, 19(6), 3521. https://doi.org/10.3390/ijerph19063521