
Landscape of Molecular Crosstalk Perturbation between Lung Cancer and COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Gene Expression Data on COVID-19 and Lung Cancer
2.2. Bioinformatics Data Analysis
3. Results
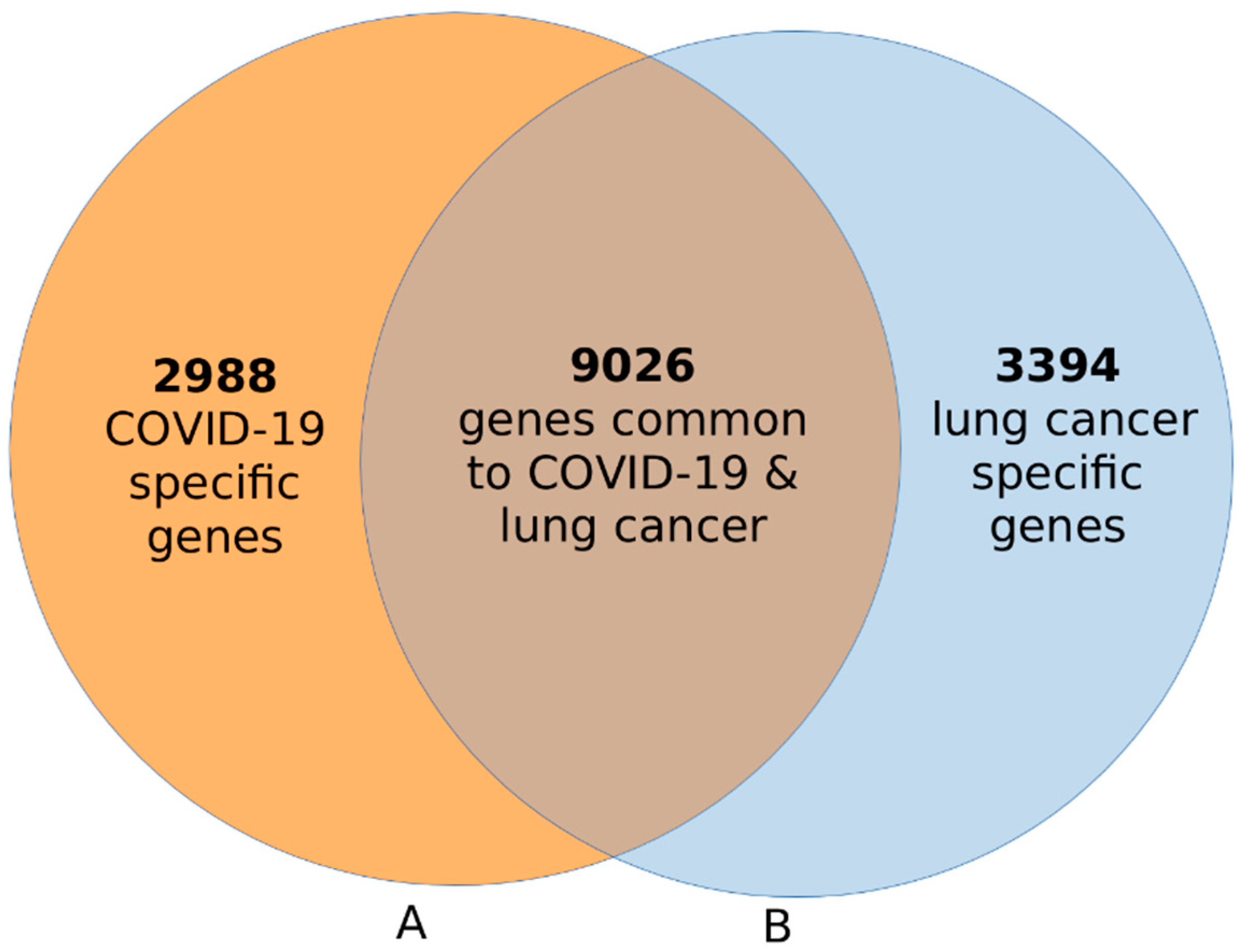
3.1. Discovery of Signatures of Genes Associated with COVID-19 and Lung Cancer
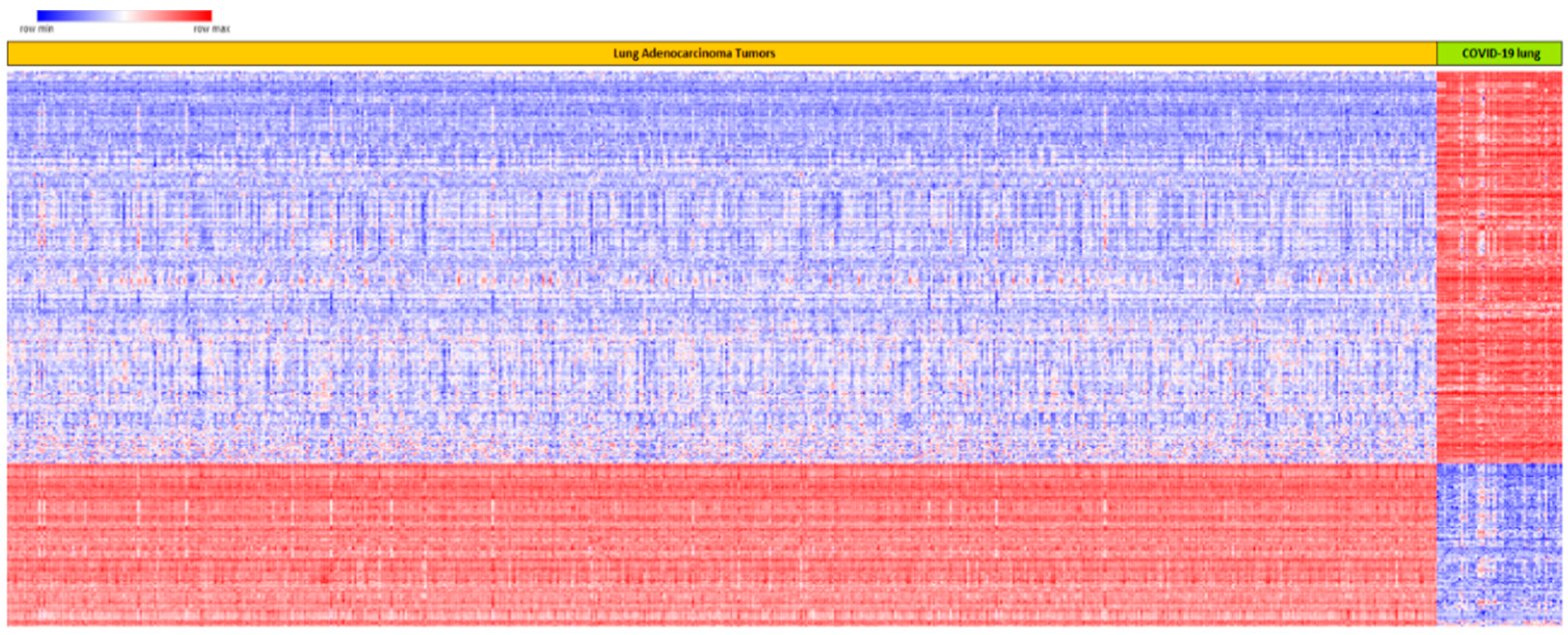
3.2. Changes in Expression Profiles for Genes Associated with COVID-19 and Lung Cancer
3.3. Similarity in Expression Profiles for Genes Associated with Both COVID-19 and Lung Cancer
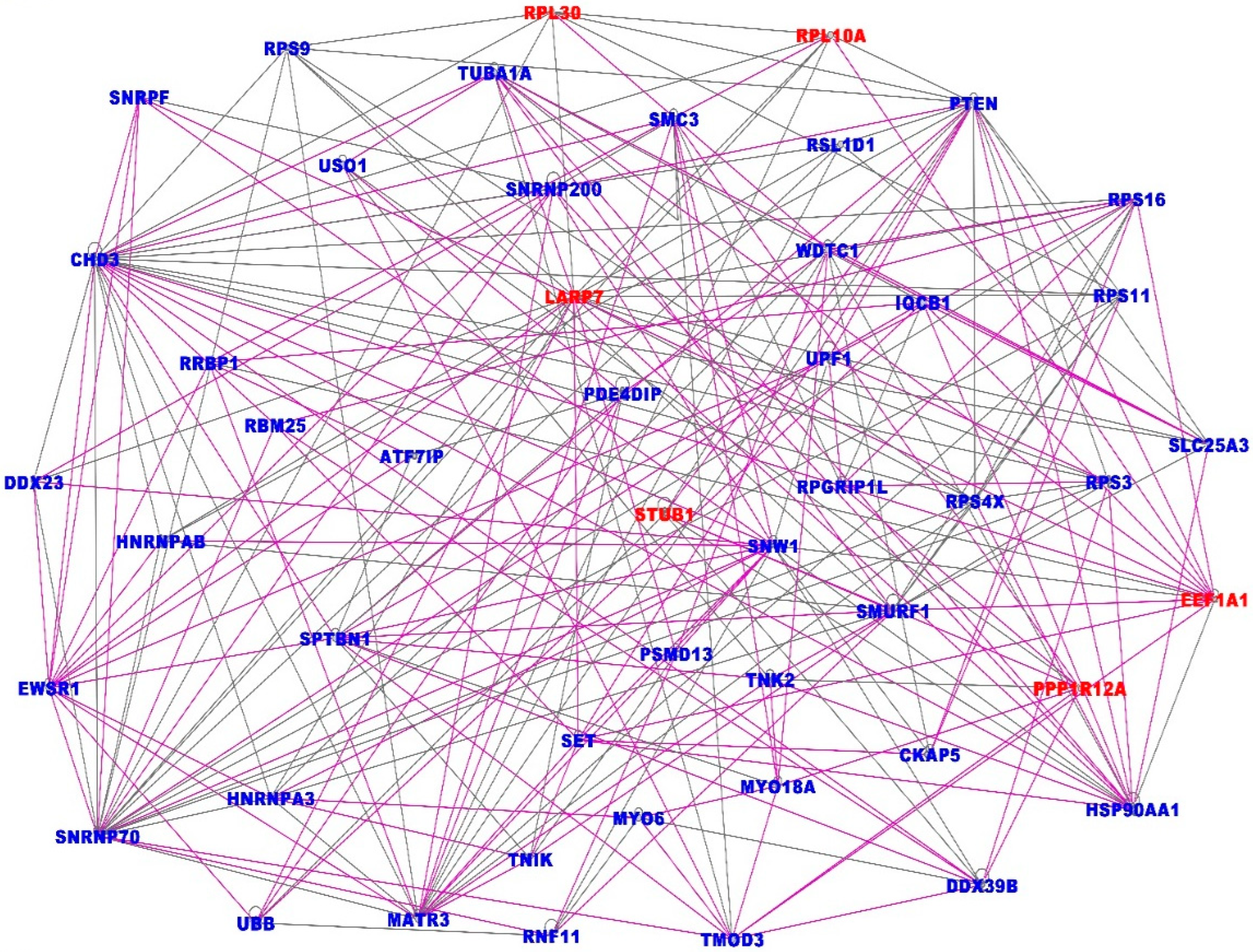
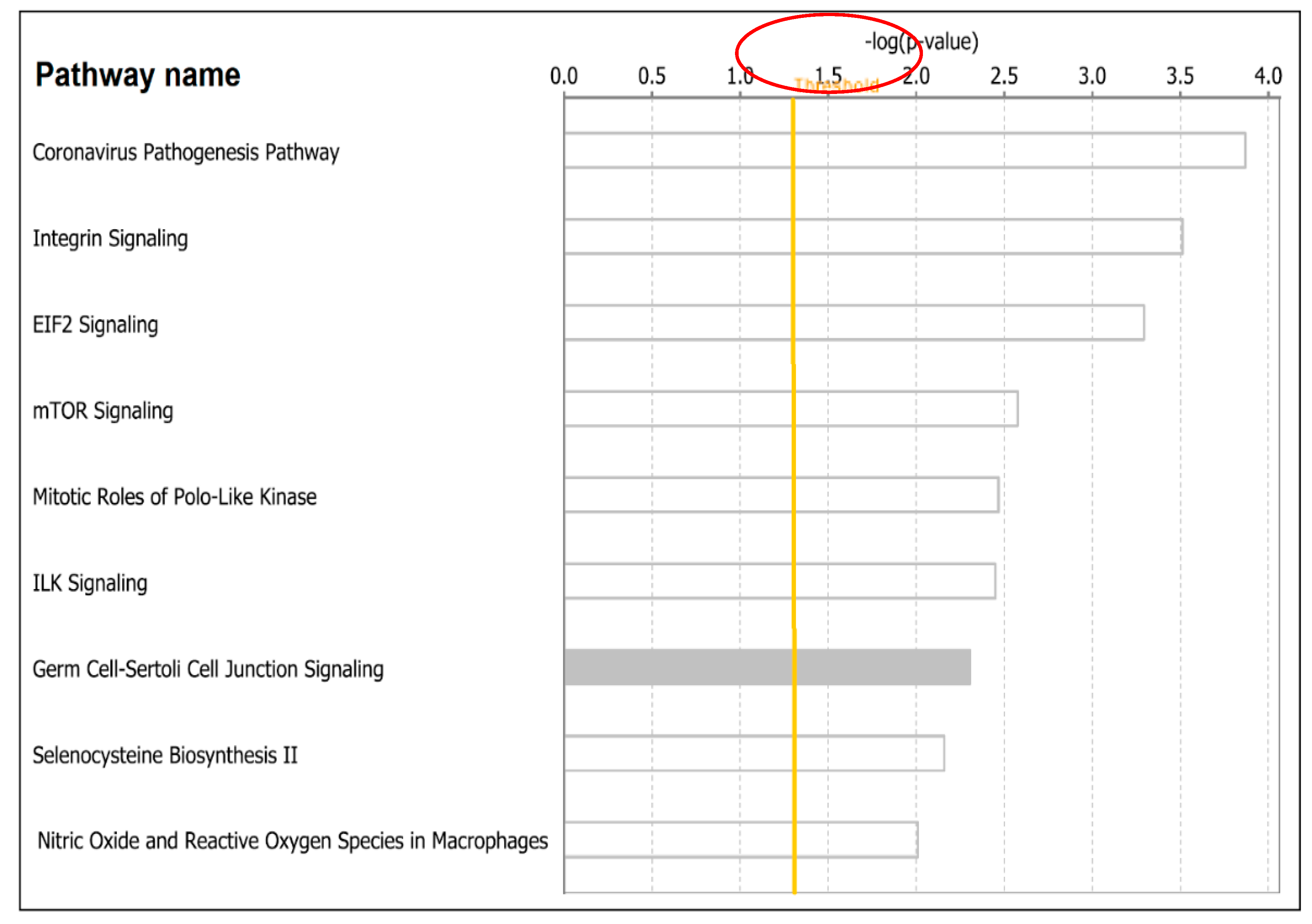
3.4. Discovery of Molecular Networks and Signaling Pathways Shared by the Two Diseases
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 10 February 2022).
- Centers for Disease Control and Prevention (CDC). Available online: https://www.cdc.gov/coronavirus/2019-ncov/index.html (accessed on 10 February 2022).
- Johns Hopkins University of Medicine (JHU). The Johns Hopkins 30-Minute COVID-19 Briefing: Expert Insights on What You Need to Know Now. Available online: https://coronavirus.jhu.edu/ (accessed on 10 February 2022).
- Liao, Z.; del Campo, E.R.; Salem, A.; Pang, Q.; Liu, H.; Guerra, J.L.L. Optimizing lung cancer radiation treatment worldwide in COVID-19 outbreak. Lung Cancer 2020, 146, 230–235. [Google Scholar] [CrossRef]
- Flaherty, G.T.; Hession, P.; Liew, C.H.; Lim, B.C.W.; Leong, T.K.; Lim, V.; Sulaiman, L.H. COVID-19 in adult patients with pre-existing chronic cardiac, respiratory and metabolic disease: A critical literature review with clinical recommendations. Trop. Dis. Travel Med. Vaccines 2020, 6, 1–13. [Google Scholar] [CrossRef]
- Luo, J.; Rizvi, H.; Preeshagul, I.R.; Egger, J.V.; Hoyos, D.; Bandlamudi, C.; McCarthy, C.G.; Falcon, C.J.; Schoenfeld, A.J.; Arbour, K.C.; et al. COVID-19 in patients with lung cancer. Ann. Oncol. 2020, 31, 1386–1396. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, H.; Hu, K.; Wang, M. Clinical Management of Lung Cancer Patients during the Outbreak of 2019 Novel Coronavirus Disease (COVID-19). Zhongguo Fei Ai Za Zhi 2020, 23, 136–141. [Google Scholar] [PubMed]
- Burki, T.K. Coronavirus in China. Lancet Respir. Med. 2020, 8, 238. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it “typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Collange, O.; Tacquard, C.; Delabranche, X.; Leonard-Lorant, I.; Ohana, M.; Onea, M.; Anheim, M.; Solis, M.; Sauer, A.; Baloglu, S.; et al. Coronavirus Disease 2019: Associated Multiple Organ Damage. Open Forum Infect. Dis. 2020, 7, ofaa249. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, Z.; Chen, Z.; Huang, X.; Xu, M.; He, T.; Zhang, Z. The establishment of reference sequence for SARS-CoV-2 and variation analysis. J. Med. Virol. 2020, 92, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, J.Y.; Yang, J.S.; Kim, J.W.; Kim, V.N.; Chang, H. The Architecture of SARS-CoV-2 Transcriptome. Cell 2020, 181, 914–921.e10. [Google Scholar] [CrossRef]
- Pfitzer-BioNTech Corporation. Available online: https://www.pfizer.com/ (accessed on 10 February 2022).
- Moderna Corporation. Available online: https://www.modernatx.com/ (accessed on 10 February 2022).
- AstraZeneca Corporation. Available online: https://www.astrazeneca.com/ (accessed on 10 February 2022).
- Desai, N.; Neyaz, A.; Szabolcs, A.; Shih, A.R.; Chen, J.H.; Thapar, V.; Nieman, L.T.; Solovyov, A.; Mehta, A.; Lieb, D.J.; et al. Spectrum of Viral Load and Host Response Seen in Autopsies of SARS-CoV-2 Infected Lungs. medRxiv 2020. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Collisson, E.A.; Mills, G.B.; Shaw, K.R.M.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef]
- National CI Genomics Data Commons. Available online: https://gdc.cancer.gov/ (accessed on 17 December 2021).
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Wu, J.; Mamidi, T.K.K.; Zhang, L.; Hicks, C. Deconvolution of the Genomic and Epigen omicInteraction Landscape of Triple-Negative Breast Cancer. Cancers 2019, 11, 1692. [Google Scholar] [CrossRef] [Green Version]
- Benjamini, Y.; Yosef, H. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Morpheus. Available online: https://software.broadinstitute.org/morpheus/ (accessed on 17 December 2020).
- Ingenuity Pathways Analysis (IPA) System Redwood, CA: Ingenuity Systems. Available online: http://www.ingenuity.com/ (accessed on 4 January 2021).
- Ashburner, M.; Ball, C.A.; Blake, J.A.; Botstein, D.; Butler, H.; Cherry, J.M.; Davis, A.P.; Dolinski, K.; Dwight, S.S.; Eppig, J.T.; et al. Gene ontology: Tool for the unification of biology. The Gene Ontology Consortium. Nat. Genet. 2000, 25, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Rogado, J.; Pangua, C.; Serrano-Montero, G.; Obispo, B.; Marino, A.M.; Pérez-Pérez, M.; López-Alfonso, A.; Gullón, P.; ÁngelLara, M. COVID-19 and lung cancer: A greater fatality rate? Lung Cancer 2020, 146, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.-Y.; Chen, Z.; Leng, Y.; Wu, M.; Liu, Y.; Zhou, F.; Ming, C.; Shao, N.; Liu, M.; Cai, H. Patients With Lung Cancer Have High Susceptibility of COVID-19: A Retrospective Study in Wuhan, China. Cancer Control 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.Z.; Chan, Y.F.Z.; Leong, W.Y.; Lee, N.M.Y.; Kalimuddin, S.; Mohideen, S.M.H.; Chan, K.S.; Tan, A.T.; Bertoletti, A.; Ooi, E.E.; et al. A Dynamic Immune Response Shapes COVID-19 Progression. Cell Host Microbe 2020, 27, 879–882.e2. [Google Scholar] [CrossRef] [PubMed]
- Sagkan, R.I.; Akin-Bali, D.F. Structural variations and expression profiles of the SARS-CoV-2 host invasion genes in lung cancer. J. Med. Virol. 2020, 92, 2637–2647. [Google Scholar] [CrossRef] [PubMed]
- Cava, C.; Bertoli, G.; Castiglioni, I. In Silico Discovery of Candidate Drugs against COVID-19. Viruses 2020, 12, 404. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Duan, X.; Yang, L.; Nilsson-Payant, B.E.; Wang, P.; Duan, F.; Tang, X.; Yaron, T.M.; Zhang, T.; Uhl, S.; et al. Identification of SARS-CoV-2 inhibitors using lung and colonic organoids. Nature 2021, 589, 270–275. [Google Scholar] [CrossRef]
- Jia, Z.; Song, X.; Shi, J.; Wang, W.; He, K. Transcriptome-based drug repositioning for coro-navirus disease 2019 (COVID-19). Pathog. Dis. 2020, 78, ftaa036. [Google Scholar] [CrossRef]
- Karunakaran, K.B.; Balakrishnan, N.; Ganapathiraju, M. Potentially repurposable drugs for COVID-19 identified from SARS-CoV-2 Host Protein Interactome. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L.; et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.-H.; Feng, G.; Liu, W.; Targher, G.; Byrne, C.D.; Zheng, M. Extrapulmonary complications of COVID-19: A multisystem disease? J. Med. Virol. 2020, 93, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Abobaker, A.; Raba, A.A.; Alzwi, A. Extrapulmonary and atypical clinical presentations of COVID-19. J. Med. Virol. 2020, 92. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0238215. [Google Scholar] [CrossRef] [PubMed]
- Moni, M.A.; Quinn, J.M.W.; Sinmaz, N.; Summers, A.M. Gene expression profiling of SARS-CoV-2 infections reveal distinct primary lung cell and systemic immune infection responses that identify pathways relevant in COVID-19 disease. Briefings Bioinform. 2020, 22, 1324–1337. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Wu, S.; Yu, Z.; Huang, J.; Zhong, X.; Liu, X.; Zhu, H.; Xiao, L.; Deng, Q.; Sun, W. Transcriptomic analysis reveals novel mechanisms of SARS-CoV-2 infection in human lung cells. Immun. Inflamm. Dis. 2020, 8, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.S.; Liu, D.X. Human Coronavirus: Host-Pathogen Interaction. Annu. Rev. Microbiol. 2019, 73, 529–557. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.; Giancotti, F.G. Integrin Signaling in Cancer: Mechanotransduction, Stemness, Epithelial Plasticity, and Therapeutic Resistance. Cancer Cell 2019, 35, 347–367. [Google Scholar] [CrossRef]
- Barrett, H.H.; Caucci, L. Stochastic models for objects and images in oncology and virology: Application to PI3K-Akt-mTOR signaling and COVID-19 disease. J. Med. Imaging 2021, 8 (Suppl. 1), S16001. [Google Scholar] [CrossRef]
- Bolourian, A.; Mojtahedi, Z. Obesity and COVID-19: The mTOR pathway as a possible culprit. Obes. Rev. 2020, 21, e13084. [Google Scholar] [CrossRef]
- Azar, W.; Njeim, R.; Fares, A.H.; Azar, N.S.; Azar, S.T.; El Sayed, M.; Eid, A.A. COVID-19 and diabetes mellitus: How one pandemic worsens the other. Rev. Endocr. Metab. Disord. 2020, 21, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary recovery after COVID-19: An observational prospective multicentre trial. Eur. Respir. J. 2020, 57, 2003481. [Google Scholar] [CrossRef] [PubMed]
- Honavar, S.; Sen, M.; Sharma, N.; Sachdev, M. COVID-19 and Eye: A Review of Ophthalmic Manifestations of COVID-19. Indian J. Ophthalmol. 2021, 69, 488–509. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Name | Chromosome | logFC | p-Value | Up/Downregulated |
|---|---|---|---|---|
| SNRNP200 | 2q11.2 | −7.66807 | 1.00 × 10−300 | Down |
| MT-CO1 | 9q21.31 | −7.45498 | 1.00 × 10−300 | Down |
| MT-CO2 | 20q13.33 | −6.52755 | 1.00 × 10−300 | Down |
| SHOC2 | 10q25.2 | −7.37305 | 1.69 × 10−300 | Down |
| KRT19 | 17q21.2 | −8.23486 | 6.20 × 10−290 | Down |
| RPS3 | 11q13.4 | −9.84811 | 2.78 × 10−289 | Down |
| ZSWIM6 | 5q12.1 | −6.9536 | 3.27 × 10−275 | Down |
| SFPQ | 1p34.3 | −10.5243 | 4.12 × 10−274 | Down |
| SERPINA1 | 14q32.13 | −8.07982 | 1.13 × 10−273 | Down |
| PAK2 | 3q29 | −5.11624 | 9.35 × 10−267 | Down |
| VPS35 | 16q11.2 | −5.93836 | 1.86 × 10−264 | Down |
| ANKLE2 | 12q24.33 | −7.79146 | 1.73 × 10−260 | Down |
| WDR1 | 4p16.1 | −5.53354 | 5.42 × 10−260 | Down |
| SORL1 | 11q24.1 | −7.31638 | 2.00 × 10−258 | Down |
| ZC3H11A | 1q32.1 | −4.42734 | 4.58 × 10−257 | Down |
| ZCCHC2 | 18q21.33 | −7.37741 | 5.73 × 10−255 | Down |
| GOLGB1 | 3q13.33 | −10.4188 | 1.95 × 10−251 | Down |
| ZFHX3 | 16q22.2 | −7.58576 | 1.35 × 10−247 | Down |
| MIER1 | 1p31.3 | −7.31554 | 1.16 × 10−246 | Down |
| P4HB | 17q25.3 | −6.7194 | 1.90 × 10−246 | Down |
| TBC1D2B | 15q24.3 | −8.07794 | 3.29 × 10−246 | Down |
| SIPA1L1 | 14q24.1 | −7.41523 | 6.22 × 10−244 | Down |
| CRTAP | 3p22.3 | −7.55263 | 5.75 × 10−240 | Down |
| LITAF | 16p13.13 | −6.36823 | 1.43 × 10−239 | Down |
| TANC1 | 2q24.2 | −4.77239 | 5.00 × 10−234 | Down |
| PCDHB13 | 5q31.3 | 6.96034 | 1.94 × 10−161 | Up |
| SYNDIG1 | 20p11.21 | 6.746343 | 1.70 × 10−160 | Up |
| LINC00324 | 17p13.1 | 6.797806 | 1.38 × 10−157 | Up |
| LEKR1 | 3q25.31 | 9.303897 | 1.01 × 10−150 | Up |
| TMEM59L | 19p12 | 7.908565 | 2.29 × 10−143 | Up |
| SERP2 | 13q14.11 | 7.323597 | 1.24 × 10−141 | Up |
| RTN4IP1 | 6q21 | 6.36925 | 6.08 × 10−139 | Up |
| ZDHHC19 | 3q29 | 7.455968 | 1.05 × 10−136 | Up |
| SEC61A2 | 10p14 | 5.899905 | 1.34 × 10−133 | Up |
| TPT1-AS1 | 13q14.13 | 7.189802 | 3.80 × 10−133 | Up |
| EGFL6 | Xp22.2 | 7.885459 | 2.92 × 10−128 | Up |
| SPDEF | 6p21.31 | 6.341318 | 2.09 × 10−124 | Up |
| SARS2 | 19q13.2 | 6.014209 | 3.10 × 10−122 | Up |
| MUC13 | 3q21.2 | 7.0324 | 3.30 × 10−120 | Up |
| SNX32 | 11q13.1 | 5.567126 | 8.27 × 10−119 | Up |
| RPS13P2 | 1p32.3 | 7.698321 | 4.21 × 10−118 | Up |
| ZNF208 | 19p12 | 4.720081 | 2.03 × 10−117 | Up |
| UBASH3A | 21q22.3 | 6.09295 | 1.18 × 10−114 | Up |
| TMEM128 | 4p16.3 | 5.123725 | 4.21 × 10−110 | Up |
| SEC31B | 10q24.31 | 4.168494 | 4.12 × 10−106 | Up |
| PRC1 | 15q26.1 | 7.932253 | 2.82 × 10−104 | Up |
| SNRNP25 | 16p13.3 | 5.221731 | 2.26 × 10−103 | Up |
| PCSK9 | 1p32.3 | 4.906412 | 5.31 × 10−103 | Up |
| TCF15 | 20p13 | 5.559709 | 1.73 × 10−100 | Up |
| GREB1 | 2p25.1 | 6.243165 | 1.08 × 10−99 | Up |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuchi, A.; Wu, J.; Fuloria, J.; Hicks, C. Landscape of Molecular Crosstalk Perturbation between Lung Cancer and COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 3454. https://doi.org/10.3390/ijerph19063454
Kuchi A, Wu J, Fuloria J, Hicks C. Landscape of Molecular Crosstalk Perturbation between Lung Cancer and COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(6):3454. https://doi.org/10.3390/ijerph19063454
Chicago/Turabian StyleKuchi, Aditi, Jiande Wu, Jyotsna Fuloria, and Chindo Hicks. 2022. "Landscape of Molecular Crosstalk Perturbation between Lung Cancer and COVID-19" International Journal of Environmental Research and Public Health 19, no. 6: 3454. https://doi.org/10.3390/ijerph19063454
APA StyleKuchi, A., Wu, J., Fuloria, J., & Hicks, C. (2022). Landscape of Molecular Crosstalk Perturbation between Lung Cancer and COVID-19. International Journal of Environmental Research and Public Health, 19(6), 3454. https://doi.org/10.3390/ijerph19063454