
Acute Effects of Electronic and Tobacco Cigarette Smoking on Sympathetic Nerve Activity and Blood Pressure in Humans


 ,
,  ,
,
Abstract
1. Introduction
2. Material and Methods
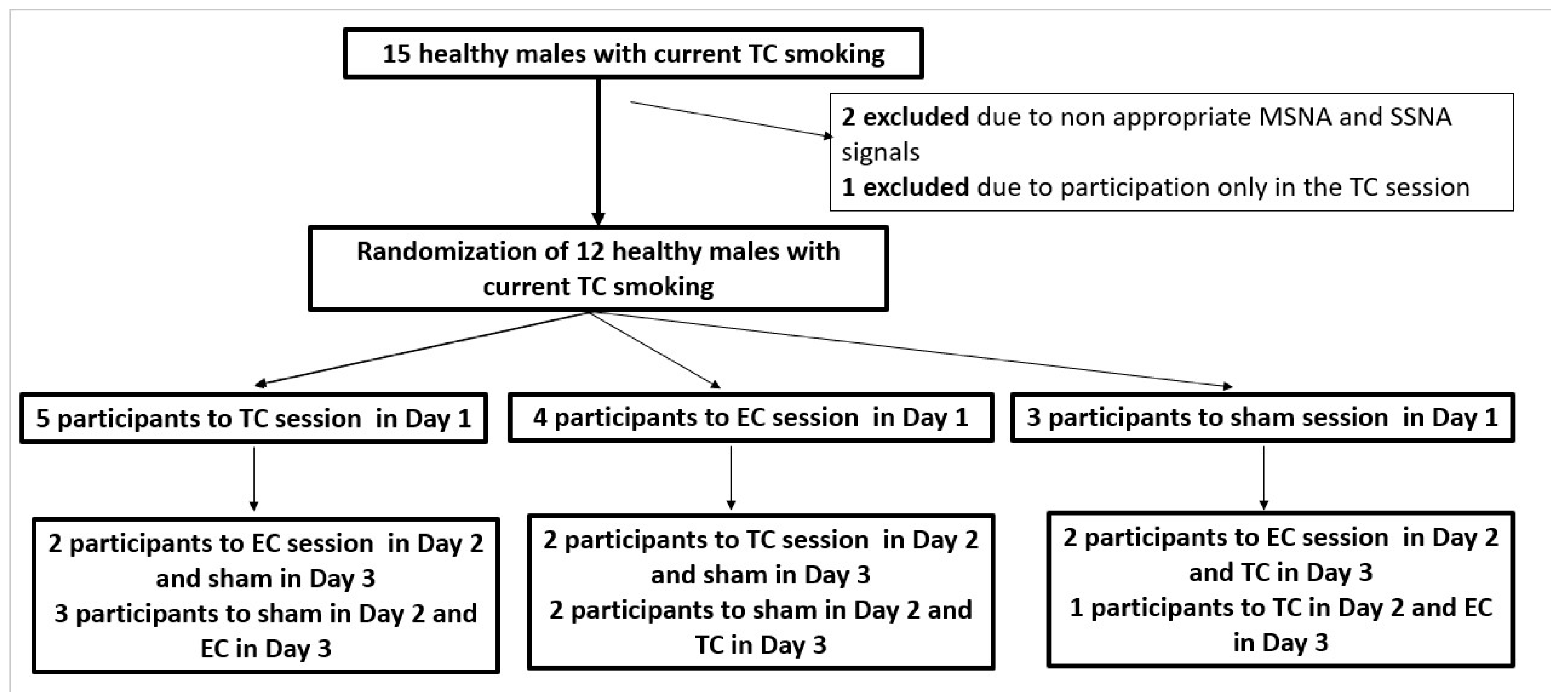
2.1. Subjects
2.2. Measurements
2.3. Experimental Session
2.4. Statistical Analysis
3. Results
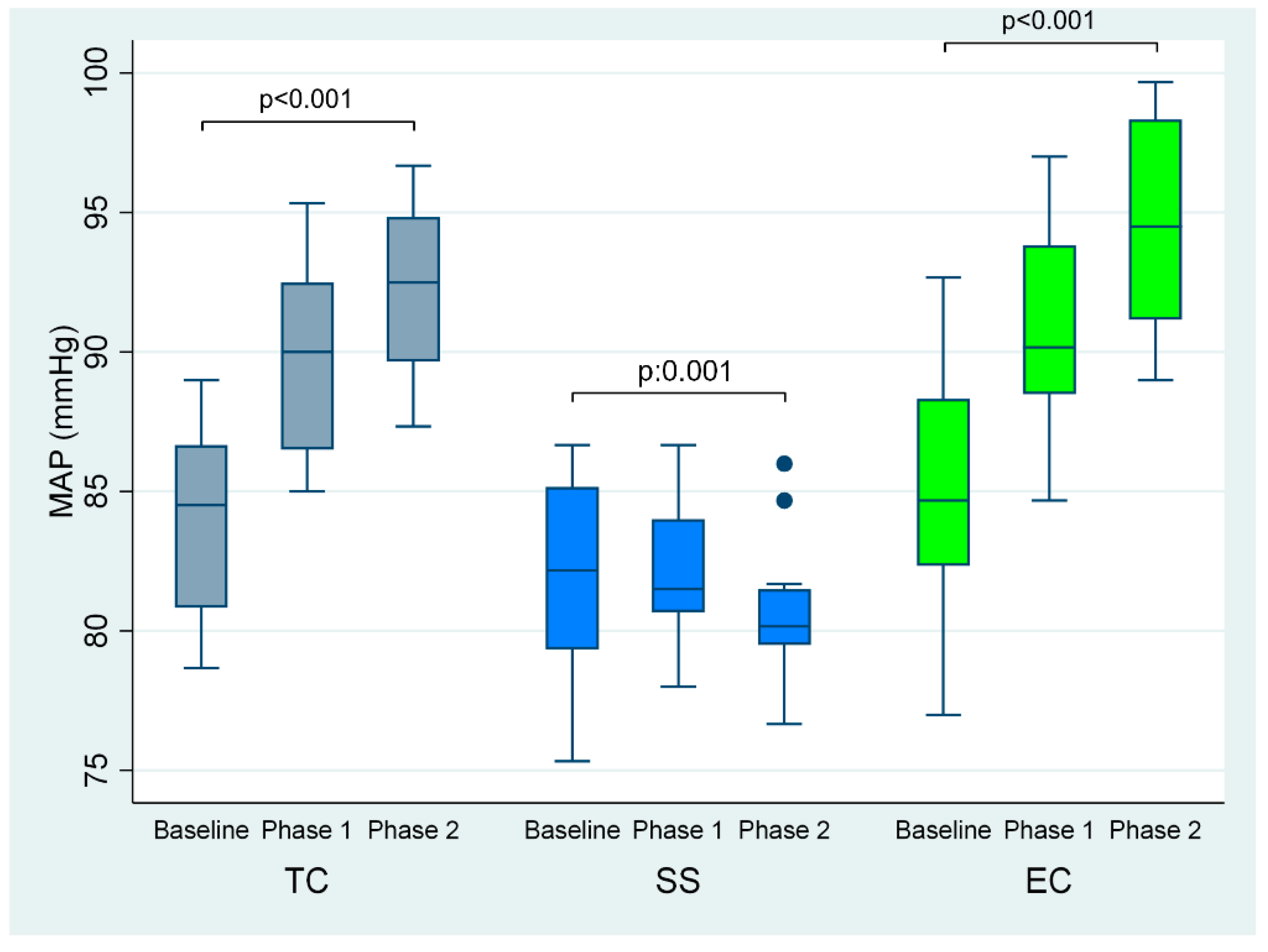
3.1. Effects of Smoking on Hemodynamic Parameters
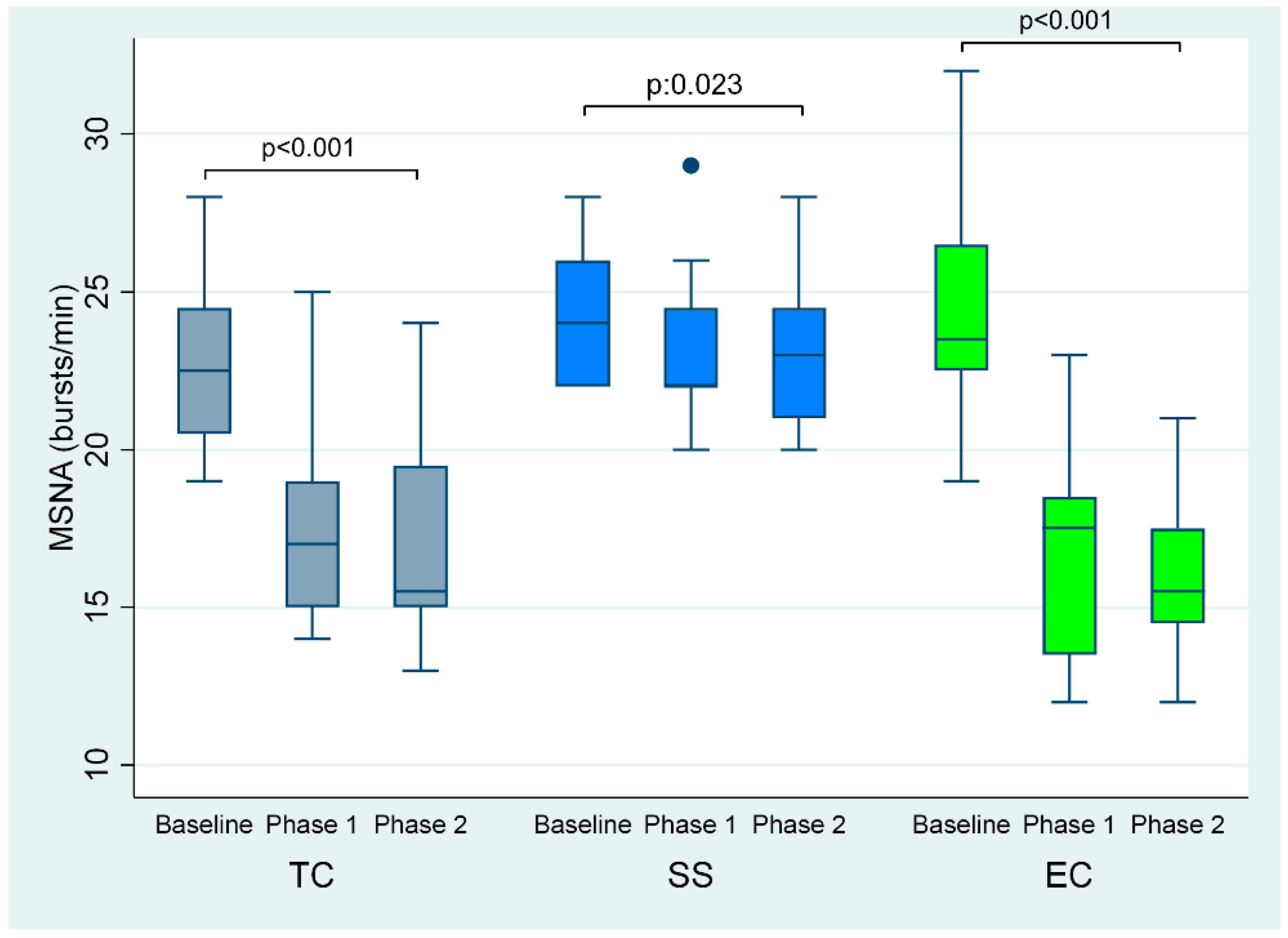
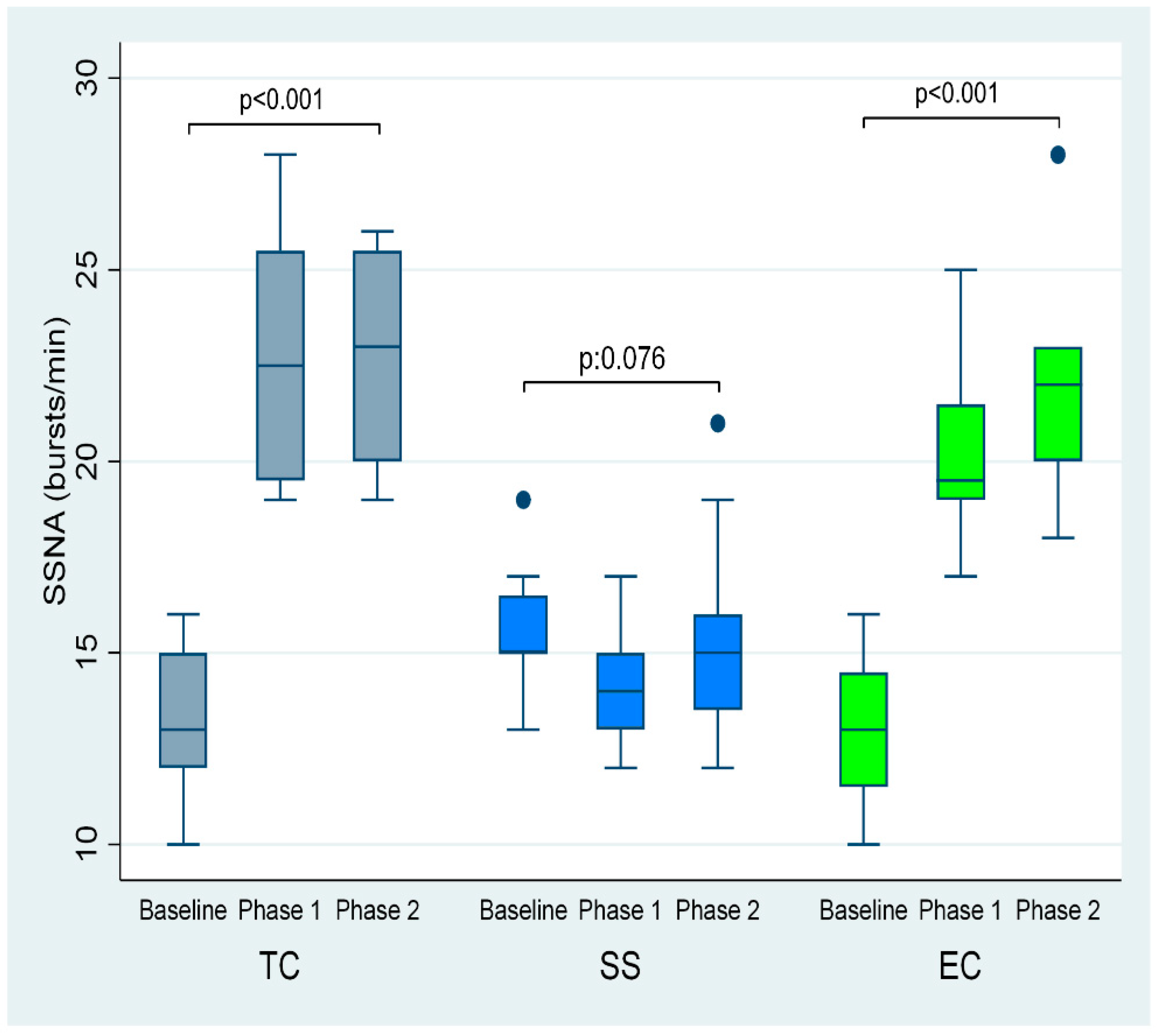
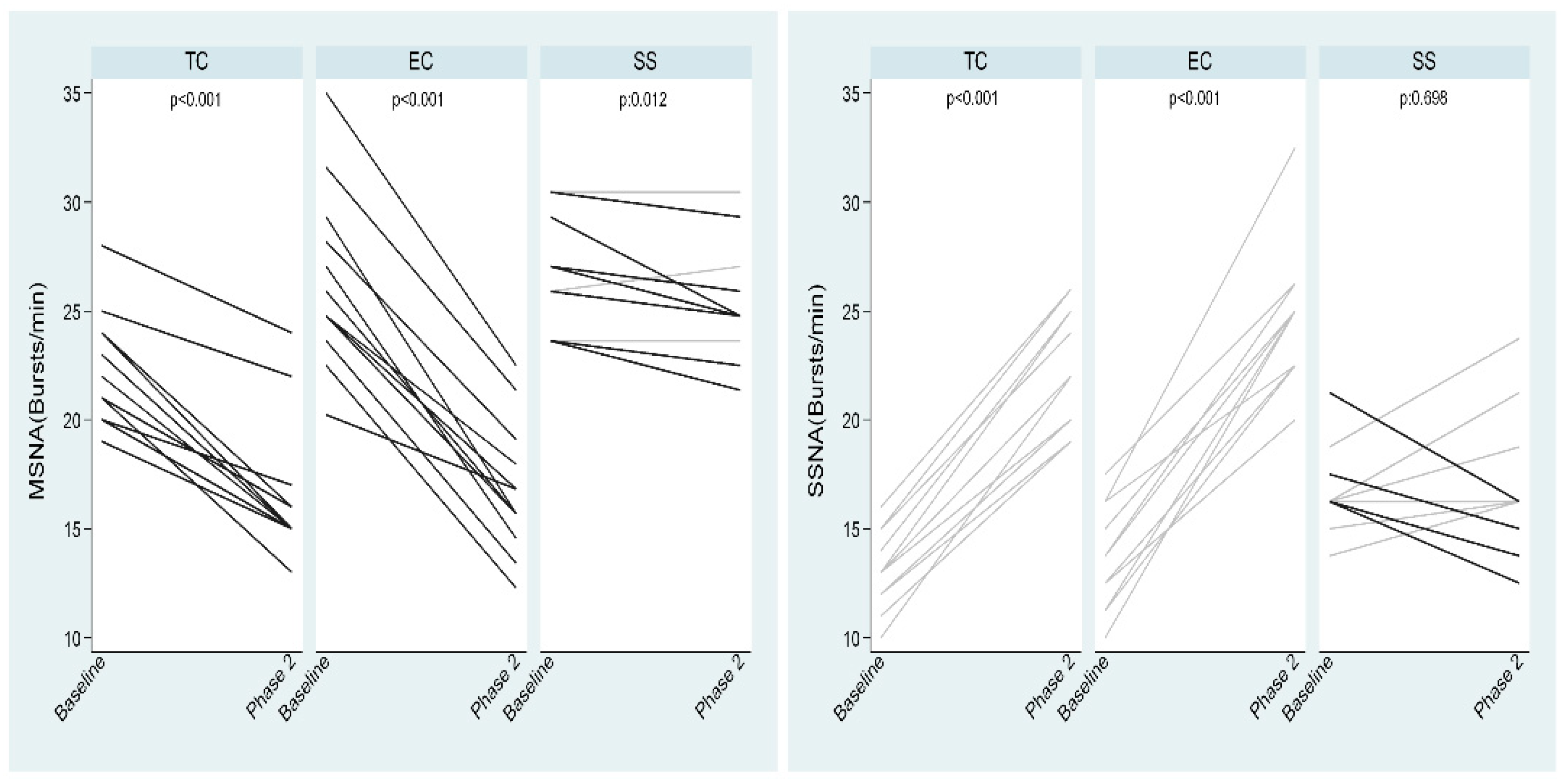
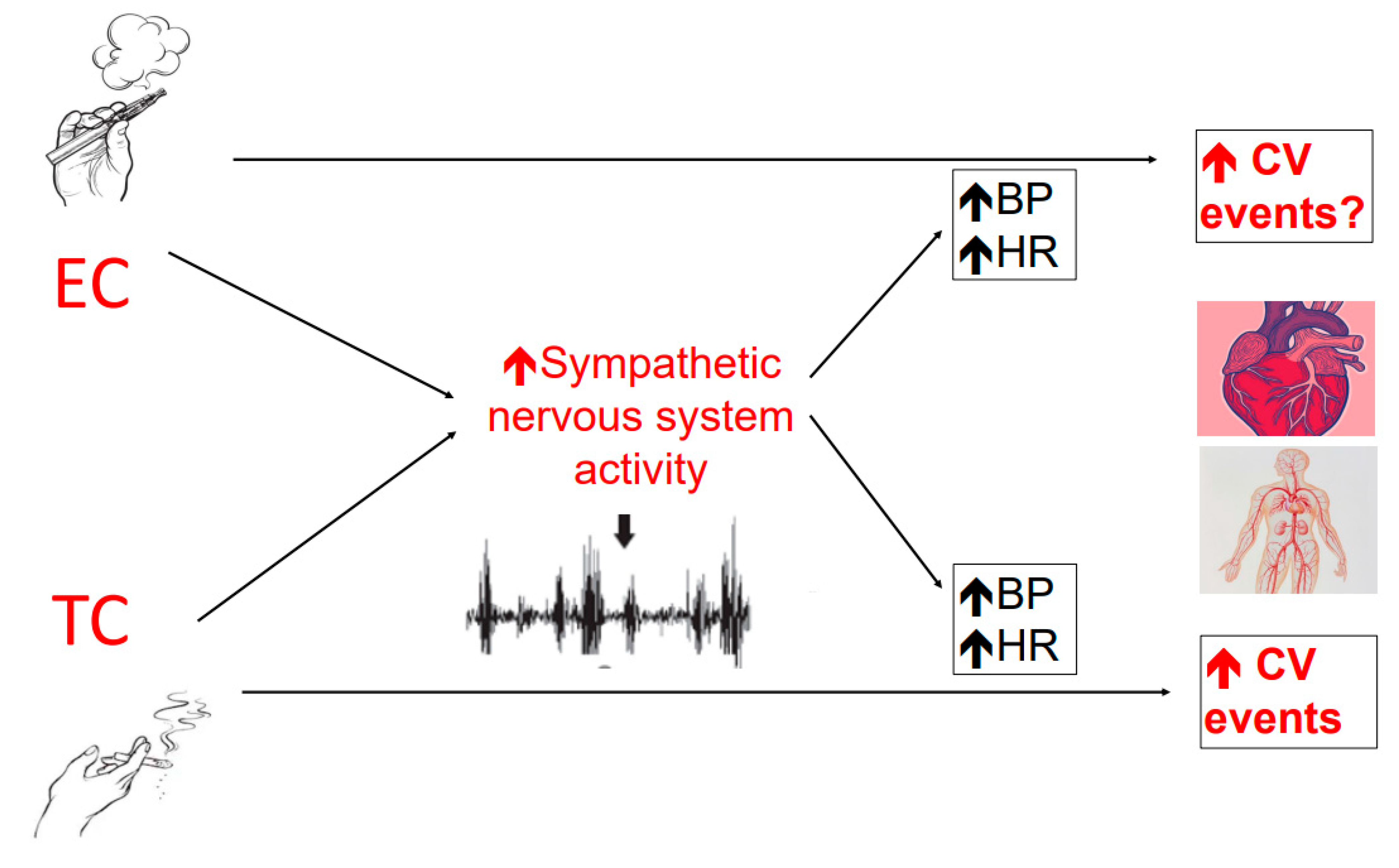
3.2. Effects of Smoking on Sympathetic Nervous System
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- D’Amario, D.; Migliaro, S.; Borovac, J.A.; Vergallo, R.; Galli, M.; Restivo, A.; Bonini, M.; Romagnoli, E.; Leone, A.M.; Crea, F. Electronic cigarettes and cardiovascular risk: Caution waiting for evidence. Eur. Cardiol. 2019, 14, 151–158. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef]
- Rippe, J.M. Lifestyle strategies for risk factor reduction, prevention, and treatment of cardiovascular disease. Am. J. Lifestyle Med. 2018, 13, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Middlekauff, H.R.; Park, J.; Moheimani, R.S. Adverse effects of cigarette and noncigarette smoke exposure on the autonomic nervous system: Mechanisms and implications for cardiovascular risk. J. Am. Coll. Cardiol. 2014, 64, 1740–1750. [Google Scholar] [CrossRef] [PubMed]
- Barua, R.S.; Ambrose, J.A. Mechanisms of coronary thrombosis in cigarette smoke exposure. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, J.A.; Barua, R.S. The pathophysiology of cigarette smoking and cardiovascular disease: An update. J. Am. Coll. Cardiol. 2004, 43, 1731–1737. [Google Scholar] [CrossRef]
- Stokes, A.; Collins, J.M.; Berry, K.M.; Reynolds, L.M.; Fetterman, J.L.; Rodriguez, C.J.; Siegel, M.B.; Benjamin, E.J. Electronic cigarette prevalence and patterns of use in adults with a history of cardiovascular disease in the United States. J. Am. Heart Assoc. 2018, 7, e007602. [Google Scholar] [CrossRef]
- Pisinger, C.; Dossing, M. A systematic review of health effects of electronic cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef]
- Bullen, C.; McRobbie, H.; Thornley, S.; Glover, M.; Lin, R.; Laugesen, M. Effect of an electronic nicotine delivery device (e cigarette) on desire to smoke and withdrawal, user preferences and nicotine delivery: Randomised cross-over trial. Tob. Control 2010, 19, 98–103. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Green, S.H.; Bayer, R.; Fairchild, A.L. Evidence, policy, and E-cigarettes–will England reframe the debate? N. Engl. J. Med. 2016, 374, 1301–1303. [Google Scholar] [CrossRef] [PubMed]
- Dinas, P.C.; Koutedakis, Y.; Flouris, A.D. Effects of active and passive tobacco cigarette smoking on heart rate variability. Int. J. Cardiol. 2013, 163, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., 3rd; Eatough, D.J.; Gold, D.R.; Pang, Y.; Nielsen, K.R.; Nath, P.; Verrier, R.L.; Kanner, R.E. Acute exposure to environmental tobacco smoke and heart rate variability. Environ. Health Perspect. 2001, 109, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E.; Haymond, M.W.; Santiago, J.V.; Shah, S.D. Norepinephrine and epinephrine release and adrenergic mediation of smoking-associated hemodynamic and metabolic events. N. Engl. J. Med. 1976, 295, 573–577. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Calhoun, D.A.; Bolla, G.B.; Giannattasio, C.; Marabini, M.; Del Bo, A.; Mancia, G. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994, 90, 248–253. [Google Scholar] [CrossRef]
- Narkiewicz, K.; van de Borne, P.J.; Hausberg, M.; Cooley, R.L.; Winniford, M.D.; Davison, D.E.; Somers, V.K. Cigarette smoking increases sympathetic outflow in humans. Circulation 1998, 98, 528–534. [Google Scholar] [CrossRef]
- Hering, D.; Somers, V.K.; Kara, T.; Kucharska, W.; Jurak, P.; Bieniaszewski, L.; Narkiewicz, K. Sympathetic neural responses to smoking are age dependent. J. Hypertens. 2006, 24, 691–695. [Google Scholar] [CrossRef]
- Hering, D.; Kucharska, W.; Kara, T.; Somers, V.K.; Narkiewicz, K. Smoking is associated with chronic sympathetic activation in hypertension. Blood Press. 2010, 19, 152–155. [Google Scholar] [CrossRef]
- Niedermaier, O.N.; Smith, M.L.; Beightol, L.A.; Zukowska-Grojec, Z.; Goldstein, D.S.; Eckberg, D.L. Influence of cigarette smoking on human autonomic function. Circulation 1993, 88, 562–571. [Google Scholar] [CrossRef]
- Moheimani, R.S.; Bhetraratana, M.; Yin, F.; Peters, K.M.; Gornbein, J.; Araujo, J.A.; Middlekauff, H.R. Increased cardiac sympathetic activity and oxidative stress in habitual electronic cigarette users: Implications for cardiovascular risk. JAMA Cardiol. 2017, 2, 278–284. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Ioakeimidis, N.; Abdelrasoul, M.; Terentes-Printzios, D.; Georgakopoulos, C.; Pietri, P.; Stefanadis, C.; Tousoulis, D. Electronic Cigarette Smoking Increases Aortic Stiffness and Blood Pressure in Young Smokers. J. Am. Coll. Cardiol. 2016, 67, 2802–2803. [Google Scholar] [CrossRef] [PubMed]
- Moheimani, R.S.; Bhetraratana, M.; Peters, K.M.; Yang, B.K.; Yin, F.; Gornbein, J.; Araujo, J.A.; Middlekauff, H.R. Sympathomimetic Effects of Acute E-Cigarette Use: Role of Nicotine and Non-Nicotine Constituents. J. Am. Heart Assoc. 2017, 6, e006579. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.E.; Cooke, W.H. Acute effects of electronic cigarettes on arterial pressure and peripheral sympathetic activity in young nonsmokers. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H248–H255. [Google Scholar] [CrossRef] [PubMed]
- Seravalle, G.; Dimitriadis, K.; Dell’Oro, R.; Grassi, G. How to assess sympathetic nervous system activity in clinical practice. Curr. Clin. Pharmacol. 2013, 8, 182–188. [Google Scholar] [CrossRef]
- Tsioufis, C.; Dimitriadis, K.; Kasiakogias, A.; Kalos, T.; Liatakis, I.; Koutra, E.; Nikolopoulou, L.; Kordalis, A.; Ella, R.O.; Lau, E.O.; et al. Effects of multielectrode renal denervation on elevated sympathetic nerve activity and insulin resistance in metabolic syndrome. J. Hypertens. 2017, 35, 1100–1108. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Buzzi, S.; Magni, L.; Brambilla, G.; Quarti-Trevano, F.; Dell’Oro, R.; Mancia, G. Muscle and skin sympathetic nerve traffic during physician and nurse blood pressure measurement. J. Hypertens. 2013, 31, 1131–1135. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Kosmopoulou, F.; Panagiotakos, D.; Ioakeimidis, N.; Alexopoulos, N.; Pitsavos, C.; Stefanadis, C. Smoking and caffeine have a synergistic detrimental effect on aortic stiffness and wave reflections. J. Am. Coll. Cardiol. 2004, 44, 1911–1917. [Google Scholar] [CrossRef][Green Version]
- Tsioufis, C.; Dimitriadis, K. Sympathetic System-Related Artery Stiffness. Hypertension 2019, 73, 975–976. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Burnett, R.T.; Krewski, D.; Jerrett, M.; Shi, Y.; Calle, E.E.; Thun, M.J. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke: Shape of the exposure-response relationship. Circulation 2009, 120, 941–948. [Google Scholar] [CrossRef]
- Munch, P.A.; Thoren, P.N.; Brown, A.M. Dual effects of norepinephrine and mechanisms of baroreceptor stimulation. Circ. Res. 1987, 61, 409–419. [Google Scholar] [CrossRef]
- Waeber, B.; Schaller, M.D.; Nussberger, J.; Bussien, J.P.; Hofbauer, K.G.; Brunner, H.R. Skin blood flow reduction induced by cigarette smoking: Role of vasopressin. Am. J. Physiol. 1984, 247, H895–H901. [Google Scholar] [CrossRef] [PubMed]
- Hagbarth, K.E.; Hallin, R.G.; Hongell, A.; Torebjork, H.E.; Wallin, B.G. General characteristics of sympathetic activity in human skin nerves. Acta Physiol. Scand. 1972, 84, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Gawron, M.; Goniewicz, M.L. Changes in puffing behavior among smokers who switched from tobacco to electronic cigarettes. Addict. Behav. 2015, 48, 1–4. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline | TC Phase 1 | TC Phase 2 | p | Baseline | EC Phase 1 | EC Phase 2 | p |
|---|---|---|---|---|---|---|---|---|
| Systolic BP (mmHg) | 117 ± 5 | 126 ± 6 | 129 ± 5 | <0.001 | 119 ± 5 | 127 ± 6 | 133 ± 5 | <0.001 |
| Diastolic BP (mmHg) | 67 ± 3 | 71 ± 3 | 73 ± 3 | <0.001 | 68 ± 4 | 72 ± 4 | 75 ± 5 | <0.001 |
| Heart rate (bpm) | 64 ± 5 | 72 ± 6 | 76 ± 5 | <0.001 | 66 ± 6 | 71 ± 6 | 75 ± 8 | <0.001 |
| MAP (mmHg) | 84 ± 3 | 90 ± 3 | 92 ± 3 | <0.001 | 84 ± 3 | 90 ± 3 | 94 ± 4 | <0.001 |
| MSNA (bursts/min) | 23 ± 3 | 17 ± 3 | 17 ± 4 | <0.001 | 24 ± 3 | 16 ± 4 | 16 ± 3 | <0.001 |
| SSNA (bursts/min) | 13 ± 2 | 22 ± 3 | 23 ± 3 | <0.001 | 13 ± 2 | 20 ± 2 | 22 ± 2 | <0.001 |
| Plasma NE (pg/mL) | 168 ± 19 | 170 ± 22 | 182 ± 27 | 0.002 | 173 ± 22 | 185 ± 17 | 231 ± 30 | 0.003 |
| Parameter | Baseline | Sham Smoking Phase 1 | Sham Smoking Phase 2 | p |
|---|---|---|---|---|
| Systolic BP (mmHg) | 114 ± 5 | 113 ± 4 | 112 ± 5 | 0.135 |
| Diastolic BP (mmHg) | 65 ± 3 | 66 ± 3 | 64 ± 3 | 0.094 |
| Heart rate (bpm) | 63 ± 4 | 64 ± 5 | 64 ± 5 | 0.041 |
| MAP (mmHg) | 84 ± 3 | 82 ± 3 | 80 ± 3 | 0.001 |
| MSNA (bursts/min) | 24 ± 2 | 23 ± 2 | 23 ± 3 | 0.023 |
| SSNA (bursts/min) | 15 ± 2 | 14 ± 2 | 15 ± 3 | 0.076 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitriadis, K.; Narkiewicz, K.; Leontsinis, I.; Konstantinidis, D.; Mihas, C.; Andrikou, I.; Thomopoulos, C.; Tousoulis, D.; Tsioufis, K. Acute Effects of Electronic and Tobacco Cigarette Smoking on Sympathetic Nerve Activity and Blood Pressure in Humans. Int. J. Environ. Res. Public Health 2022, 19, 3237. https://doi.org/10.3390/ijerph19063237
Dimitriadis K, Narkiewicz K, Leontsinis I, Konstantinidis D, Mihas C, Andrikou I, Thomopoulos C, Tousoulis D, Tsioufis K. Acute Effects of Electronic and Tobacco Cigarette Smoking on Sympathetic Nerve Activity and Blood Pressure in Humans. International Journal of Environmental Research and Public Health. 2022; 19(6):3237. https://doi.org/10.3390/ijerph19063237
Chicago/Turabian StyleDimitriadis, Kyriakos, Krzysztof Narkiewicz, Ioannis Leontsinis, Dimitris Konstantinidis, Costas Mihas, Ioannis Andrikou, Costas Thomopoulos, Dimitrios Tousoulis, and Konstantinos Tsioufis. 2022. "Acute Effects of Electronic and Tobacco Cigarette Smoking on Sympathetic Nerve Activity and Blood Pressure in Humans" International Journal of Environmental Research and Public Health 19, no. 6: 3237. https://doi.org/10.3390/ijerph19063237
APA StyleDimitriadis, K., Narkiewicz, K., Leontsinis, I., Konstantinidis, D., Mihas, C., Andrikou, I., Thomopoulos, C., Tousoulis, D., & Tsioufis, K. (2022). Acute Effects of Electronic and Tobacco Cigarette Smoking on Sympathetic Nerve Activity and Blood Pressure in Humans. International Journal of Environmental Research and Public Health, 19(6), 3237. https://doi.org/10.3390/ijerph19063237