
Older People’s Help-Seeking Behaviors in Rural Contexts: A Systematic Review



Abstract
1. Introduction
2. Methods
2.1. Study Design and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Analysis
3. Results
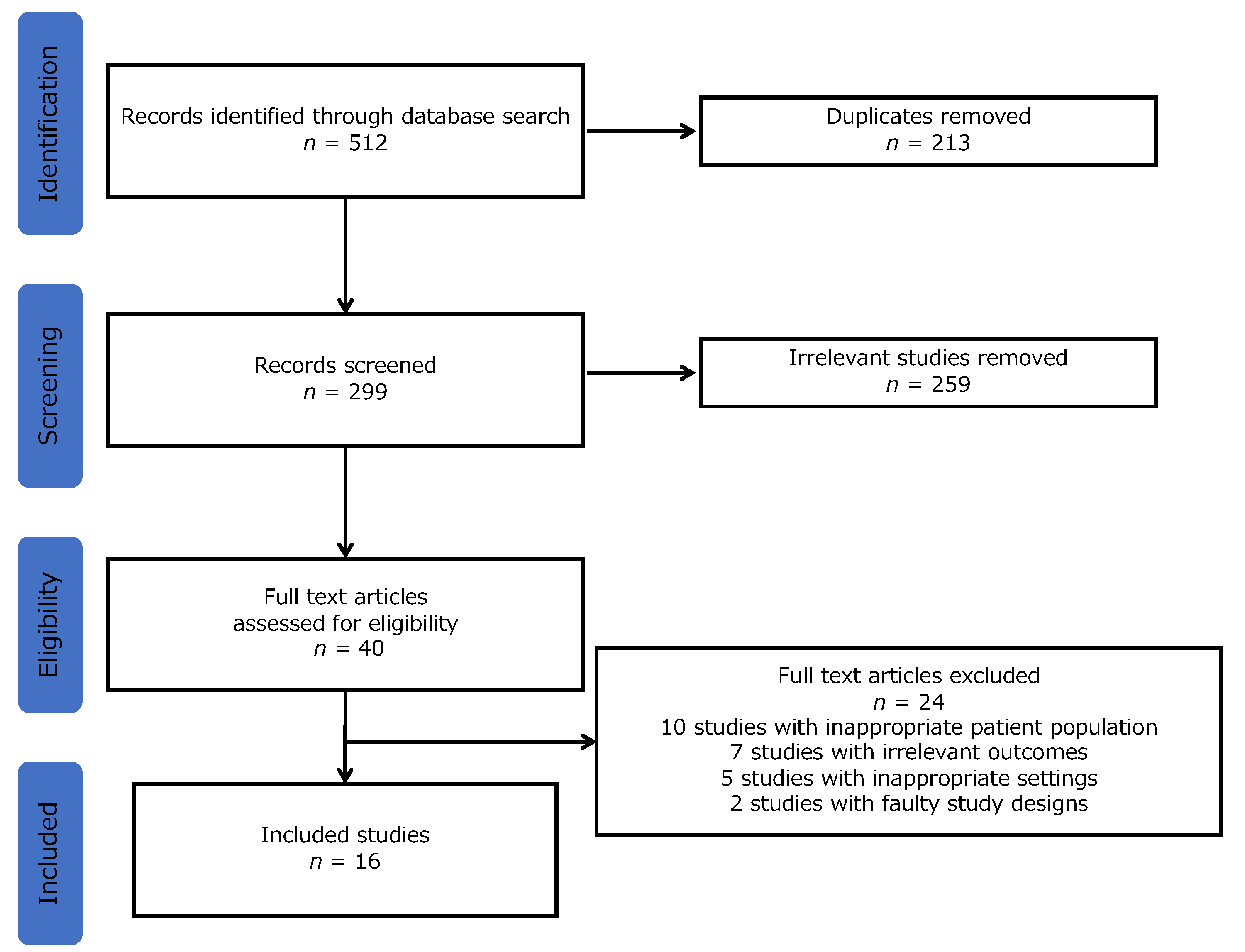
3.1. Search Results
3.2. Study Characteristics
3.3. The Causes of HSBs, Contents of HSBs, and Study’s Outcomes
3.4. Rural Older Patients’ HSBs and Outcomes
3.4.1. Associations with Backgrounds
3.4.2. Barriers
3.4.3. QOL, Diagnosis, and Perception of HSBs
3.4.4. Clarifying the Content of HSBs
3.4.5. Trend for Professional Care, SRH, and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rickwood, D.; Thomas, K. Conceptual measurement framework for help-seeking for mental health problems. Psychol. Res. Behav. Manag. 2012, 5, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Doshi, A.M.; Van Den Eeden, S.K.; Morrill, M.Y.; Schembri, M.; Thom, D.H.; Brown, J.S.; Reproductive Risks for Incontinence Study at Kaiser Research Group. Women with diabetes: Understanding urinary incontinence and help seeking behavior. J. Urol. 2010, 184, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Chinnakali, P.; Mohan, B.; Upadhyay, R.P.; Singh, A.K.; Srivastava, R.; Yadav, K. Hypertension in the elderly: Prevalence and health seeking behavior. N. Am. J. Med. Sci. 2012, 4, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Raymond, N.C.; Osman, W.; O’Brien, J.M.; Ali, N.; Kia, F.; Mohamed, F.; Mohamed, A.; Goldade, K.B.; Pratt, R.; Okuyemi, K. Culturally informed views on cancer screening: A qualitative research study of the differences between older and younger Somali immigrant women. BMC Public Health 2014, 14, 1188. [Google Scholar] [CrossRef]
- Shaw, C.; Brittain, K.; Tansey, R.; Williams, K. How people decide to seek health care: A qualitative study. Int. J. Nurs. Stud. 2008, 45, 1516–1524. [Google Scholar] [CrossRef]
- Bourne, P.A. Health status and medical care-seeking behaviour of the poorest 20% in Jamaica. Int. J. Collab. Res. Intern. Med. Public Health 2009, 1, 167–185. [Google Scholar]
- Pais-Ribeiro, J.L. Quality of life is a primary end-point in clinical settings. Clin. Nutrit. 2004, 23, 121–130. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Gomi, T.; Katsube, T. Challenges and solutions in the continuity of home care for rural older people: A thematic analysis. Home Health Care Serv. Q. 2020, 39, 126–139. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Sano, C.; Könings, K.D. Educational intervention to improve citizen’s healthcare participation perception in rural Japanese communities: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1782. [Google Scholar] [CrossRef]
- Cornally, N.; McCarthy, G. Help-seeking behaviour: A concept analysis. Int. J. Nurs. Pract. 2011, 17, 280–288. [Google Scholar] [CrossRef]
- Goins, R.T.; Williams, K.A.; Carter, M.W.; Spencer, M.; Solovieva, T. Perceived barriers to health care access among rural older adults: A qualitative study. J. Rural Health 2005, 21, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, K.; Osaka, W.; Togari, T.; Ishikawa, H.; Yonekura, Y.; Sekido, A.; Matsumoto, M. Comprehensive health literacy in Japan Is lower than in Europe: A validated Japanese-language assessment of health literacy. BMC Public Health 2015, 15, 505. [Google Scholar] [CrossRef] [PubMed]
- Beck, F.; Richard, J.; Nguyen-Thanh, V.; Montagni, I.; Parizot, I.; Renahy, E. Use of the internet as a health information resource among French young adults: Results from a nationally representative survey. J. Med. Internet Res. 2014, 16, e128. [Google Scholar] [CrossRef] [PubMed]
- van Deursen, A.J.A.M.; Helsper, E.J. A nuanced understanding of internet use and non-use among the elderly. Eur. J. Commun. 2015, 30, 171–187. [Google Scholar] [CrossRef]
- Hesse, B.W.; Nelson, D.E.; Kreps, G.L.; Croyle, R.T.; Arora, N.K.; Rimer, B.K.; Kasisomayajula, V. Trust and sources of health information: The impact of the internet and its implications for health care providers: Findings from the First Health Information National Trends Survey. Arch. Intern. Med. 2005, 165, 2618–2624. [Google Scholar] [CrossRef]
- Molokhia, M.; Majeed, A. Current and future perspectives on the management of polypharmacy. BMC Fam. Pract. 2017, 18, 70. [Google Scholar] [CrossRef]
- Freund, T.; Campbell, S.M.; Geissler, S.; Kunz, C.U.; Mahler, C.; Peters-Klimm, F.; Szecsenyi, J. Strategies for reducing potentially avoidable hospitalizations for ambulatory care-sensitive conditions. Ann. Fam. Med. 2013, 11, 363–370. [Google Scholar] [CrossRef]
- Irwan, A.M.; Kato, M.; Kitaoka, K.; Kido, T.; Taniguchi, Y.; Shogenji, M. Self-care practices and health-seeking behavior among older persons in a developing country: Theories-based research. Int. J. Nurs. Sci. 2016, 3, 11–23. [Google Scholar] [CrossRef][Green Version]
- Bennett, I.M.; Chen, J.; Soroui, J.S.; White, S. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann. Fam. Med. 2009, 7, 204–211. [Google Scholar] [CrossRef]
- Ford, J.A.; Turley, R.; Porter, T.; Shakespeare, T.; Wong, G.; Jones, A.P.; Steel, N. Access to primary care for socio-economically disadvantaged older people in rural areas: A qualitative study. PLoS ONE 2018, 13, e0193952. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kataoka, D.; Sano, C. Effectiveness and challenges in local self-governance: Multifunctional autonomy in Japan. Int. J. Environ. Res. Public Health 2021, 18, 574. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Makinen, M.; Lee, D.C.; Kidane, R.; Blanchet, N.; Liang, H.; Li, J.; Lindelow, M.; Wang, H.; Xie, S.; et al. Integrated care delivery and health care seeking by chronically-ill patients—A case-control study of rural Henan Province, China. Int. J. Equity Health 2015, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- von dem Knesebeck, O.; Geyer, S. Emotional support, education and self-rated health in 22 European countries. BMC Public Health 2007, 7, 272. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Ryu, Y.; Kitayuguchi, J.; Maeno, T.; Sano, C. What resources do elderly people choose for managing their symptoms? Clarification of rural older people’s choices of help-seeking behaviors in Japan. BMC Health Serv. Res. 2021, 21, 640. [Google Scholar] [CrossRef]
- Jett, K. Making the Connection: Seeking and receiving help by elderly African Americans. Qual. Health Res. 2002, 12, 373–387. [Google Scholar] [CrossRef]
- Sakamoto, S.; Tanaka, E.; Neichi, K.; Ono, Y. Where is help sought for depression or suicidal ideation in an elderly population living in a rural area of Japan? Psychiatry Clin. Neurosci. 2004, 58, 522–530. [Google Scholar] [CrossRef]
- Ma, X.; Xiang, Y.T.; Li, S.R.; Xiang, Y.Q.; Guo, H.L.; Hou, Y.Z.; Cai, Z.J.; Li, Z.B.; Li, Z.J.; Tao, Y.F.; et al. Prevalence and sociodemographic correlates of depression in an elderly population living with family members in Beijing, China. Psychol. Med. 2008, 38, 1723–1730. [Google Scholar] [CrossRef]
- Vagenas, D.; McLaughlin, D.; Dobson, A. Regional variation in the survival and health of older Australian women: A prospective cohort study. Aust. N. Z. J. Public Health 2009, 33, 119–125. [Google Scholar] [CrossRef]
- Romay-Barja, M.; Jarrin, I.; Ncogo, P.; Nseng, G.; Sagrado, M.J.; Santana-Morales, M.A.; Aparicio, P.; Valladares, B.; Riloha, M.; Benito, A. Rural-urban differences in household treatment-seeking behaviour for suspected malaria in children at Bata District, Equatorial Guinea. PLoS ONE 2015, 10, e0135887. [Google Scholar] [CrossRef]
- Brenes, G.A.; Danhauer, S.C.; Lyles, M.F.; Hogan, P.E.; Miller, M.E. Barriers to mental health treatment in rural older adults. Am. J. Geriatr. Psychiatry. 2015, 23, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Nguyen, N.T.T.; ChieuTo, S.B.; Pham, T.L.; Nguyen, T.X.; Nguyen, H.T.T.; Nguyen, T.N.; Nguyen, T.H.T.; Nguyen, Q.N.; Tran, B.X.; et al. Sex differences in quality of life and health services utilization among elderly people in rural Vietnam. Int. J. Environ. Res. Public Health 2018, 16, 69. [Google Scholar] [CrossRef]
- Zhang, T.; Liu, C.; Ni, Z. Association of access to healthcare with self-assessed health and quality of life among old adults with chronic disease in China: Urban versus rural populations. Int. J. Environ. Res. Public Health 2019, 16, 2592. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Li, Z.; Pan, Z.; He, R.; Zhang, L. Prevalence and associated factors of self-treatment behaviour among different elder subgroups in Rural China: A cross-sectional study. Int. J. Equity Health 2020, 19, 32. [Google Scholar] [CrossRef]
- Srivastava, S.; Gill, A. Untreated morbidity and treatment-seeking behaviour among the elderly in India: Analysis based on national sample survey 2004 and 2014. SSM Popul. Health 2020, 10, 100557. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Sulaiman, K.M.; Drishti, D.; Muhammad, T. Factors associated with psychiatric disorders and Treatment Seeking Behaviour among Older Adults in India. Sci. Rep. 2021, 11, 24085. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. The association between the self-management of mild symptoms and quality of life of elderly populations in rural communities: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 8857. [Google Scholar] [CrossRef]
- Chauhan, S.; Gupte, S.S.; Kumar, S.; Patel, R. Urban–rural differential in diabetes and hypertension among elderly in India: A study of prevalence, factors, and treatment-seeking. Diabetes Metab. Syndr. 2021, 15, 102201. [Google Scholar] [CrossRef]
- Korman, M.; Felkle, D.; Korman, T. Are rural patients aware of myocardial infarction’s risk factors, symptoms, and management? A survey study in the COVID-19 pandemic era. Folia Med. Cracov. 2021, 61, 103–115. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. Potential help-seeking behaviors associated with better self-rated health among rural older patients: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 9116. [Google Scholar] [CrossRef]
- Ogbolu, Y.; Scrandis, D.A.; Fitzpatrick, G. Barriers and facilitators of care for diverse patients: Nurse leader perspectives and nurse manager implications. J. Nurs. Manag. 2018, 26, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Barcham, R.; Silas, E.; Irie, J. Health promotion and empowerment in Henganofi district, Papua New Guinea. Rural Remote Health 2016, 16, 3553. [Google Scholar] [CrossRef] [PubMed]
- Saint Arnault, D. Cultural determinants of help seeking: A model for research and practice. Res. Theory Nurs. Pract. 2009, 23, 259–278. [Google Scholar] [CrossRef] [PubMed]
- McCutchan, G.M.; Wood, F.; Edwards, A.; Richards, R.; Brain, K.E. Influences of cancer symptom knowledge, beliefs and barriers on cancer symptom presentation in relation to socioeconomic deprivation: A systematic review. BMC Cancer 2015, 15, 1000. [Google Scholar] [CrossRef]
- Begashaw, B.; Tessema, F.; Gesesew, H.A. Health care seeking behavior in southwest Ethiopia. PLoS ONE 2016, 11, e0161014. [Google Scholar] [CrossRef]
- Alberts, J.F.; Sanderman, R.; Gerstenbluth, I.; van den Heuvel, W.J. Sociocultural variations in help-seeking behavior for everyday symptoms and chronic disorders. Health Policy 1998, 44, 57–72. [Google Scholar] [CrossRef]
- Elliott, A.M.; McAteer, A.; Hannaford, P.C. Revisiting the symptom iceberg in today’s primary care: Results from a UK population survey. BMC Fam. Pract. 2011, 12, 16. [Google Scholar] [CrossRef]
- Takahashi, O.; Ohde, S. The ecology of medical care in Japan revisited. Value Health 2014, 17, A434. [Google Scholar] [CrossRef][Green Version]
- Fukui, T.; Rahman, M.; Ohde, S.; Hoshino, E.; Kimura, T.; Urayama, K.Y.; Omata, F.; Deshpande, G.A.; Takahashi, O. Reassessing the ecology of medical care in Japan. J. Commun. Health 2017, 42, 935–941. [Google Scholar] [CrossRef]
- Yun, K.; Paul, P.; Subedi, P.; Kuikel, L.; Nguyen, G.T.; Barg, F.K. Help-seeking behavior and health care navigation by Bhutanese refugees. J. Commun. Health 2016, 41, 526–534. [Google Scholar] [CrossRef]
- Willems, S.; Peersman, W.; De Maeyer, P.; Buylaert, W.; De Maeseneer, J.; De Paepe, P. The impact of Neighborhood deprivation on patients’ unscheduled out-of-hours healthcare seeking behavior: A cross-sectional study. BMC Fam. Pract. 2013, 14, 136. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Carver, L.F.; Beamish, R.; Phillips, S.P.; Villeneuve, M. A scoping review: Social participation as a cornerstone of successful aging in place among rural older adults. Geriatrics 2018, 3, 75. [Google Scholar] [CrossRef] [PubMed]
- Ocloo, J.; Matthews, R. From tokenism to empowerment: Progressing patient and public involvement in healthcare improvement. BMJ Qual. Saf. 2016, 25, 626–632. [Google Scholar] [CrossRef] [PubMed]
- von Faber, M.; Tavy, Z.; van der Pas, S. Engaging older people in age-friendly cities through participatory video design. Int. J. Environ. Res. Public Health 2020, 17, 8977. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, J.H.; Sychareun, V.; Kang, M. Recovering Disrupted Social capital: Insights from Lao DPR rural villagers’ perceptions of local leadership. BMC Public Health 2016, 16, 1189. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Rana, A.K.; Kabir, Z.N. Social capital and quality of life in old age: Results from a cross-sectional study in rural Bangladesh. J. Aging Health 2006, 18, 419–434. [Google Scholar] [CrossRef]
- Aslani, P. Patient empowerment and informed decision-making. Int. J. Pharm. Pract. 2013, 21, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Sirri, L.; Fava, G.A.; Sonino, N. The Unifying Concept of Illness Behavior. Psychother. Psychosom. 2013, 82, 74–81. [Google Scholar] [CrossRef]


{kind=link}
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Population | Rural older people/the rural elderly | Other age groups |
| Setting | Rural areas | Not rural areas |
| Types of study | Qualitative, quantitative, mixed-methods | Non-empirical studies (editorial, news) |
| Outcome | Outcomes associated with HSBs | Outcomes not associated with HSBs |
| Other | Abstract available Full text available in English | Abstract not available Full text not available in English |
| Study | Country | Study Design | Participants | Causes of HSB | HSB | Outcome | Results |
|---|---|---|---|---|---|---|---|
| Jett 2002, [26] | United States | Qualitative research | n = 41; M and F | General symptoms | Professional care | Perception of HSB | Older individuals believe that receiving help in late life is a reward for a good life. By understanding and following the rules of help-seeking, formal helpers might more efficiently and effectively meet their needs. |
| Sakamoto 2004, [27] | Japan | Cross-sectional study | n = 285; M and F | Depression | Professional care | Associations with backgrounds | Participation in mental health workshops was associated with frequent consultation with professional care. |
| Ma 2008, [28] | China | Cohort | n = 127; M and F | Depression | Professional care | Associations with backgrounds | Female sex, lower educational level, monthly income, and the presence of one or more major medical conditions were associated with lower use of professional care with the symptoms of depression. |
| Vagenas 2009, [29] | Australia | Cohort | n = 12,778; F | General symptoms | Professional care | Mortality | Mortality was higher in rural than in urban women. Rural women reported fewer visits to general practitioners and medical specialists. |
| Iloh 2012, [30] | Nigeria | Cross-sectional | n = 216; M and F | Acute symptoms | Professional care | Diagnosis | The three most common causes of geriatric emergencies were acute malaria (33.8%), hypertensive crises syndrome (19.0%), and acute hypertensive heart failure (18.1%). |
| Brenes 2015, [31] | United States | Cross-sectional | n = 478; M and F | General anxiety disorder | Professional care | Associations with backgrounds | The most reported barrier to treatment was the personal belief that “I should not need help”. Other commonly reported barriers included practical barriers (cost, not knowing where to go, distance), mistrust of mental health providers, not thinking treatment would help, stigma, and not wanting to talk with a stranger about private matters. |
| Pham 2018, [32] | Vietnam | Cross-sectional | n = 523; M and F | General symptoms | Professional care | QOL | People with higher QOL were less likely to use inpatient services. |
| Zhang 2019, [33] | China | Cross-sectional | n = 31,464; M and F | Chronic diseases | Professional care | QOL | One-year and two-week access to healthcare was found to be associated with QOL scores at the 10th and 90th quantiles, respectively. Access to healthcare affects the self-assessed health and QOL of the elderly. |
| Xu 2020, [34] | China | Cross-sectional | n = 216; M and F | General symptoms | Lay care | Associations with backgrounds | The factors associated with self-treatment were better health status, no recent alcohol consumption, and no utilization of family practice. |
| Srivastava 2020, [35] | India | Cross-sectional | n = 9973; M and F | Chronic diseases | Professional care | Associations with backgrounds | Older individuals living with a spouse in comparison to those living alone had a lower likelihood to have untreated morbidities. Additionally, the elderly from rural areas and having lower levels of education had a higher likelihood of untreated morbidity. |
| Ohta 2021, [25] | Japan | Mixed-method | n = 267; M and F | Acute symptoms | Lay and professional care | Clarifying contents of HSB | The most common behavior with mild symptoms was consulting with primary care physicians, followed by self-care and using home medicine. The test–retest reliability for mild symptoms revealed kappa values of 0.836 for lay care and 0.808 for professional care. |
| Srivastava 2021, [36] | India | Cross-sectional | n = 31,464; M and F | Psychiatric disorders | Professional care | Associations with backgrounds | Older adults, who were females and with a lower socioeconomic background had a lower probability of seeking treatment for a psychiatric disorder. |
| Ohta 2021, [37] | Japan | Cross-sectional | n = 1066; M and F | Acute symptoms | Lay care | QOL | The HSBs with a trend of using self-management were related to a high QOL. |
| Chauhan 2021, [38] | India | Cross-sectional | n = 31,464; M and F | Chronic diseases | Professional care | Associations with backgrounds | Treatment-seeking is relatively low among the elderly in low-income households. |
| Korman 2021, [39] | Poland | Cross-sectional | n = 194; M and F | Myocardial infarction | Professional care | Trend for professional care | 76.2% would call an ambulance in response to chest pain. Merely 80% were able to recall the emergency phone number. Among respondents who declared they would not call an ambulance, 38.7% were afraid of in-hospital COVID-19 infection or healthcare system collapse. |
| Ohta 2021, [40] | Japan | Cross-sectional | n = 169; M and F | Acute symptoms | Lay and professional care | Self-rated health | Using both lay and professional care was significantly associated with high self-rated health. |
| Variable | Number of Studies | Percentage |
|---|---|---|
| Countries | ||
| United States | 2 | 12.5% |
| China | 3 | 18.8% |
| Japan | 4 | 25% |
| India | 3 | 18.8% |
| Vietnam | 1 | 6.25% |
| Poland | 1 | 6.25% |
| Nigeria | 1 | 6.25% |
| Australia | 1 | 6.25% |
| Study design | ||
| Cross-sectional | 12 | 75% |
| Cohort | 2 | 12.5% |
| Qualitative | 1 | 6.25% |
| Mixed-method | 1 | 6.25% |
| Variable | Number of Studies | Percentage |
|---|---|---|
| Cause of HSB | ||
| General symptoms | 4 | 25% |
| Acute symptoms | 4 | 25% |
| Chronic diseases | 3 | 18.8% |
| Depression | 2 | 12.5% |
| General anxiety disorder | 1 | 6.25% |
| Psychiatric diseases | 1 | 6.25% |
| Myocardial infarction | 1 | 6.25% |
| Content of HSBs | ||
| Professional care | 12 | 75% |
| Lay care | 2 | 12.5% |
| Lay and professional care | 2 | 12.5% |
| Study outcomes | ||
| Associations with backgrounds | 7 | 43.8% |
| Quality of life | 3 | 18.8% |
| Perception of HSB | 1 | 6.25% |
| Diagnosis | 1 | 6.25% |
| Clarifying contents of HSB | 1 | 6.25% |
| Trend for professional care | 1 | 6.25% |
| Self-rated health | 1 | 6.25% |
| Mortality | 1 | 6.25% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohta, R.; Ryu, Y.; Sano, C. Older People’s Help-Seeking Behaviors in Rural Contexts: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3233. https://doi.org/10.3390/ijerph19063233
Ohta R, Ryu Y, Sano C. Older People’s Help-Seeking Behaviors in Rural Contexts: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(6):3233. https://doi.org/10.3390/ijerph19063233
Chicago/Turabian StyleOhta, Ryuichi, Yoshinori Ryu, and Chiaki Sano. 2022. "Older People’s Help-Seeking Behaviors in Rural Contexts: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 6: 3233. https://doi.org/10.3390/ijerph19063233
APA StyleOhta, R., Ryu, Y., & Sano, C. (2022). Older People’s Help-Seeking Behaviors in Rural Contexts: A Systematic Review. International Journal of Environmental Research and Public Health, 19(6), 3233. https://doi.org/10.3390/ijerph19063233