
Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults

 , ,
, , 
 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instruments
2.2.1. Electromyostimulator
2.2.2. Muscle Thickness Assessment (Ultrasound)
2.3. Procedures
2.3.1. Strength Training Protocol
2.3.2. Electromyostimulation Protocol
2.3.3. Electromyostimulation Combined with Strength Training Protocol
2.4. Statistical Analyses
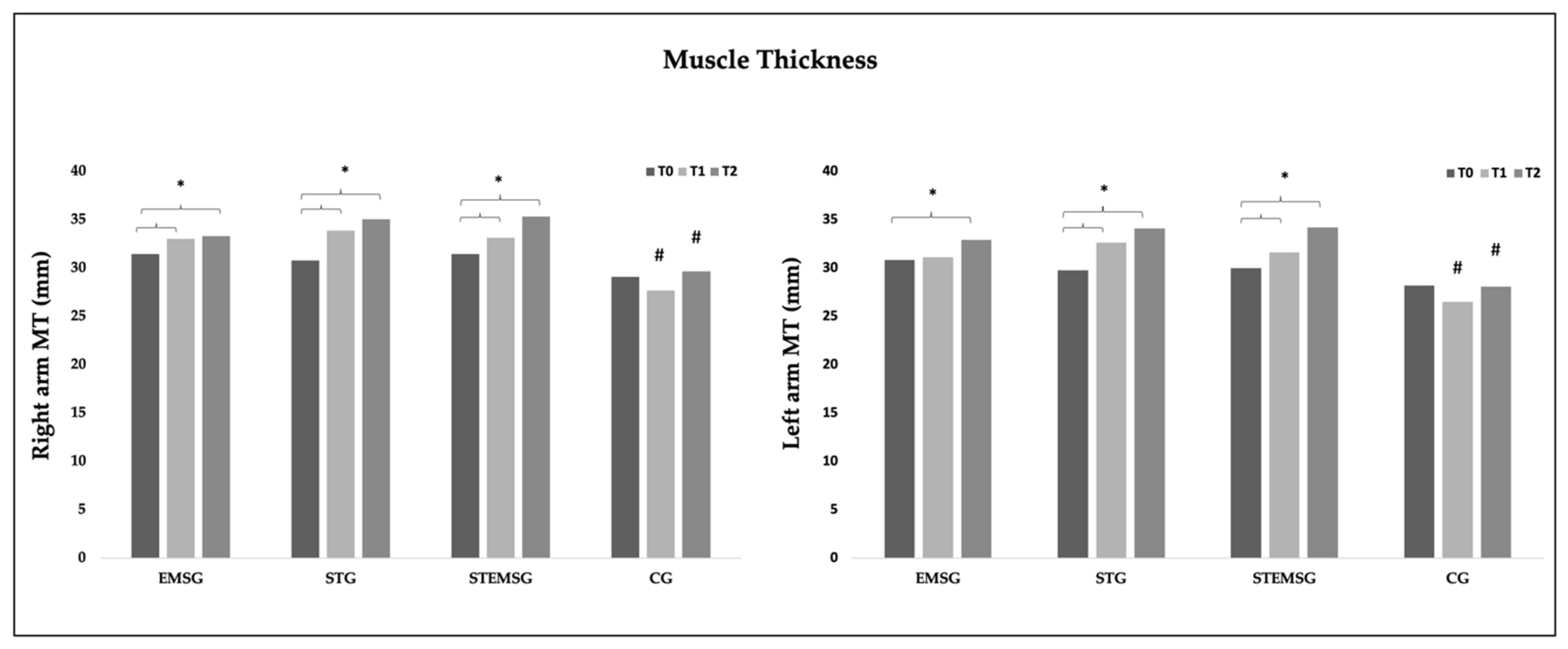
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grgic, J.; Lazinica, B.; Mikulic, P.; Krieger, J.W.; Schoenfeld, B.J. The Effects of Short versus Long Inter-Set Rest Intervals in Resistance Training on Measures of Muscle Hypertrophy: A Systematic Review. Eur. J. Sport Sci. 2017, 17, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and Hypertrophy Adaptations Between Low- vs. High-Load Resistance Training: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, D.S.; Simpson, S. Supplemental EMS and Dynamic Weight Training: Effects on Knee Extensor Strength and Vertical Jump of Female College Track & Field Athletes. J. Strength Cond. Res. 1998, 12, 131–137. [Google Scholar]
- Vanderthommen, M.; Duchateau, J. Electrical Stimulation as a Modality to Improve Performance of the Neuromuscular System. Exerc. Sport Sci. Rev. 2007, 35, 180. [Google Scholar] [CrossRef]
- Yanase, K.; Hasegawa, S.; Nakamura, M.; Yamauchi, T.; Nishishita, S.; Araki, K.; Umehara, J.; Fujita, K.; Sato, I.; Ibuki, S.; et al. Electrical Stimulation to the Infraspinatus on Hypertrophy and Strength of the Shoulder. Int. J. Sports Med. 2018, 39, 828–834. [Google Scholar] [CrossRef]
- Wirtz, N.; Dörmann, U.; Micke, F.; Filipovic, A.; Kleinöder, H.; Donath, L. Effects of Whole-Body Electromyostimulation on Strength-, Sprint-, and Jump Performance in Moderately Trained Young Adults: A Mini-Meta-Analysis of Five Homogenous RCTs of Our Work Group. Front. Physiol. 2019, 10, 1336. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Influence of Training Regimens and Stimulation Parameters on Effectiveness in Electromyostimulation Training of Selected Strength Parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef]
- Kemmler, W.; Schliffka, R.; Mayhew, J.L.; von Stengel, S. Effects of Whole-Body Electromyostimulation on Resting Metabolic Rate, Body Composition, and Maximum Strength in Postmenopausal Women: The Training and ElectroStimulation Trial. J. Strength Cond. Res. 2010, 24, 1880. [Google Scholar] [CrossRef]
- Kemmler, W.; Bebenek, M.; Engelke, K.; von Stengel, S. Impact of Whole-Body Electromyostimulation on Body Composition in Elderly Women at Risk for Sarcopenia: The Training and ElectroStimulation Trial (TEST-III). AGE 2014, 36, 395–406. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weißenfels, A.; Bebenek, M.; Fröhlich, M.; Kohl, M.; von Stengel, S. Effects of Whole-Body Electromyostimulation versus High-Intensity Resistance Exercise on Body Composition and Strength: A Randomized Controlled Study. Evid.-Based Complement. Altern. Med. 2016, 2016, 9236809. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Shojaa, M.; von Stengel, S.; Filipovic, A.; Kleinöder, H.; Berger, J.; Fröhlich, M. Efficacy and Safety of Low Frequency Whole-Body Electromyostimulation (WB-EMS) to Improve Health-Related Outcomes in Non-Athletic Adults. A Systematic Review. Front. Physiol. 2018, 9, 573. [Google Scholar] [CrossRef]
- Adams, V. Electromyostimulation to Fight Atrophy and to Build Muscle: Facts and Numbers: Editorial. J. Cachexia Sarcopenia Muscle 2018, 9, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, P.; Zhou, S.; Crowley, Z.; Brooks, L.; Hooper, A. Effects of Unilateral Electromyostimulation Superimposed on Voluntary Training on Strength and Cross-Sectional Area. Muscle Nerve 2009, 40, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Matsuse, H.; Shiba, N.; Umezu, Y.; Nago, T.; Tagawa, Y.; Kakuma, T.; Nagata, K.; Basford, J.R. Muscle Training by Means of Combined Electrical Stimulation and Volitional Contraction. Aviat. Space Environ. Med. 2006, 77, 6. [Google Scholar]
- Gondin, J.; Guette, M.; Ballay, Y.; Martin, A. Electromyostimulation Training Effects on Neural Drive and Muscle Architecture. Med. Sci. Sports Exerc. 2005, 37, 1291–1299. [Google Scholar] [CrossRef]
- Cabric, M.; Appell, H.-J.; Resic, A. Effects of Electrical Stimulation of Different Frequencies on the Myonuclei and Fiber Size in Human Muscle. Int. J. Sports Med. 1987, 8, 323–326. [Google Scholar] [CrossRef]
- Paillard, T. Training Based on Electrical Stimulation Superimposed Onto Voluntary Contraction Would Be Relevant Only as Part of Submaximal Contractions in Healthy Subjects. Front. Physiol. 2018, 9, 1428. [Google Scholar] [CrossRef]
- Micke, F.; Kleinöder, H.; Dörmann, U.; Wirtz, N.; Donath, L. Effects of an Eight-Week Superimposed Submaximal Dynamic Whole-Body Electromyostimulation Training on Strength and Power Parameters of the Leg Muscles: A Randomized Controlled Intervention Study. Front. Physiol. 2018, 9, 1719. [Google Scholar] [CrossRef]
- Ludwig, O.; Berger, J.; Becker, S.; Kemmler, W.; Fröhlich, M. The Impact of Whole-Body Electromyostimulation on Body Posture and Trunk Muscle Strength in Untrained Persons. Front. Physiol. 2019, 10, 1020. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Dugnani, S.; Folz, M.; Di Pierno, E.; Mauro, F. Effect of Combined Electrostimulation and Plyometric Training on Vertical Jump Height. Med. Sci. Sports Exerc. 2002, 34, 1638. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.A.; Izquierdo, M.; Maffiuletti, N.A.; García-López, J. Electromyostimulation and Plyometric Training Effects on Jumping and Sprint Time. Int. J. Sports Med. 2006, 27, 533–539. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cabric, M.; Appell, H.-J. Effect of Electrical Stimulation of High and Low Frequency on Maximum Isometric Force and Some Morphological Characteristics in Men. Int. J. Sports Med. 1987, 8, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, N.; Wahl, P.; Kleinöder, H.; Wechsler, K.; Achtzehn, S.; Mester, J. Acute Metabolic, Hormonal, and Psychological Responses to Strength Training with Superimposed EMS at the Beginning and the End of a 6 Week Training Period. J. Musculoskelet. Neuronal Interact. 2015, 15, 325–332. [Google Scholar] [PubMed]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernández-González, V.; Reverter-Masia, J. Effects of Whole-Body ELECTROMYOSTIMULATION on Health and Performance: A Systematic Review. BMC Complement. Altern. Med. 2019, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Lima, K.M.M.; Carneiro, S.P.; de S. Alves, D.; Peixinho, C.C.; de Oliveira, L.F. Assessment of Muscle Architecture of the Biceps Femoris and Vastus Lateralis by Ultrasound After a Chronic Stretching Program. Clin. J. Sport Med. 2015, 25, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Paillard, T. Combined Application of Neuromuscular Electrical Stimulation and Voluntary Muscular Contractions. Sports Med. 2008, 38, 161–177. [Google Scholar] [CrossRef]
- Filipovic, A.; DeMarees, M.; Grau, M.; Hollinger, A.; Seeger, B.; Schiffer, T.; Bloch, W.; Gehlert, S. Superimposed Whole-Body Electrostimulation Augments Strength Adaptations and Type II Myofiber Growth in Soccer Players During a Competitive Season. Front. Physiol. 2019, 10, 1187. [Google Scholar] [CrossRef]
- Paillard, T. Muscle Plasticity of Aged Subjects in Response to Electrical Stimulation Training and Inversion and/or Limitation of the Sarcopenic Process. Ageing Res. Rev. 2018, 46, 1–13. [Google Scholar] [CrossRef]
- Wall, B.T.; Dirks, M.L.; Verdijk, L.B.; Snijders, T.; Hansen, D.; Vranckx, P.; Burd, N.A.; Dendale, P.; van Loon, L.J.C. Neuromuscular Electrical Stimulation Increases Muscle Protein Synthesis in Elderly Type 2 Diabetic Men. Am. J. Physiol.-Endocrinol. Metab. 2012, 303, E614–E623. [Google Scholar] [CrossRef]
- Di Filippo, E.S.; Mancinelli, R.; Marrone, M.; Doria, C.; Verratti, V.; Toniolo, L.; Dantas, J.L.; Fulle, S.; Pietrangelo, T. Neuromuscular Electrical Stimulation Improves Skeletal Muscle Regeneration through Satellite Cell Fusion with Myofibers in Healthy Elderly Subjects. J. Appl. Physiol. 2017, 123, 501–512. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | EMSG | STG | STEMSG | CG | |
|---|---|---|---|---|---|
| Age (years) | 24.5 ± 3.52 | 22.9 ± 2.08 | 25.3 ± 4.03 | 23.8 ± 3.43 | 25.8 ± 3.97 |
| Height (cm) | 176.9 ± 7.85 | 175.7 ± 8.76 | 177.4 ± 8.41 | 177.9 ± 6.82 | 175.7 ± 8.29 |
| BM (kg) | 73.1 ± 10.72 | 72.2 ± 18.12 | 73.5 ± 5.13 | 75.6 ± 9.23 | 71.0 ± 6.75 |
| EBF (%) | 17.9 ± 6.09 | 17.6 ± 8.29 | 16.9 ± 4.64 | 19.4 ± 5.51 | 17.6 ± 6.06 |
| Variables | Moment Effect | Interaction of Moment × Group | Group Effect | ||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | (ηp2) | F | p | (ηp2) | F | p | (ηp2) | |
| MTR50 | 33.324 | <0.0001 | 0.481 | 6.506 | <0.0001 | 0.352 | 5.515 | 0.003 | 0.315 |
| MTR60 | 35.600 | <0.0001 | 0.497 | 8.575 | <0.0001 | 0.417 | 7.547 | <0.0001 | 0.386 |
| MTL50 | 30.914 | <0.0001 | 0.462 | 5.163 | <0.0001 | 0.301 | 6.098 | 0.002 | 0.337 |
| MTL60 | 26.719 | <0.0001 | 0.426 | 5.863 | <0.0001 | 0.328 | 6.511 | 0.001 | 0.352 |
| EMSG | STG | STEMSG | CG | |
|---|---|---|---|---|
| T0 | ||||
| MTR50 | 30.12 ± 4.56 (27.94–32.30) | 28.81 ± 3.70 (26.63–30.99) | 30.00 ± 2.48 (27.82–32.18) | 27.62 ± 2.39 (25.44–29.80) |
| MTR60 | 32.82 ± 3.95 (31.01–34.63) | 32.76 ± 2.57 (30.95–34.57) | 32.88 ± 2.59 (31.07–34.69) | 30.61 ± 1.71 (28.80–32.42) |
| MTL50 | 29.49 ± 3.99 (27.53–31.45) | 27.78 ± 3.44 (25.82–29.74) | 28.95 ± 2.50 (26.99–30.91) | 26.48 ± 1.84 (24.52–28.44) |
| MTL60 | 32.18 ± 4.35 (29.99–34.37) | 31.78 ± 3.23 (29.59–33.97) | 31.02 ± 2.59 (28.83–33.21) | 29.97 ± 3.20 (27.78–32.16) |
| T1 | ||||
| MTR50 | 31.84 ± 3.81 (29.84–33.85) * | 31.95 ± 3.92 (29.95–33.96) * | 31.79 ± 2.28 (29.79–33.80) * | 25.96 ± 1.99 (23.96–27.97) & |
| MTR60 | 34.23 ± 3.45 (32.16–36.30) * | 35.78 ± 3.70 (33.71–37.85) * | 34.49 ± 3.31 (32.42–36.56) * | 29.39 ± 2.24 (27.32–31.46) *& |
| MTL50 | 31.14 ± 3.34 (29.22–33.06) | 30.98 ± 3.42 (29.06–32.90) * | 30.26 ± 2.60 (28.34–32.18) * | 25.11 ± 2.46 (23.19–27.03) & |
| MTL60 | 31.04 ± 2.88 (32.15–35.93) | 34.28 ± 3.64 (32.39–36.17) & | 33.03 ± 2.53 (31.14–34.92) * | 27.95 ± 2.60 (26.06–29.84) & |
| T2 | ||||
| MTR50 | 31.98 ± 3.68 (30.00–33.95) * | 33.56 ± 3.54 (31.59–35.53) * | 34.06 ± 2.18 (32.09–34.63) *† | 28.06 ± 2.66 (26.09–30.03) & |
| MTR60 | 34.65 ± 3.00 (32.87–36.43) * | 36.53 ± 3.23 (34.75–38.31) * | 36.64 ± 2.43 (34.86–38.42) *† | 31.22 ± 2.32 (29.44–33.00) & |
| MTL50 | 31.38 ± 3.49 (29.22–33.06) * | 32.59 ± 2.80 (30.85–34.33) * | 32.96 ± 2.32 (31.22–34.70) *† | 26.21 ± 2.03 (24.47–27.95) & |
| MTL60 | 34.44 ± 2.94 (32.87–36.02) * | 35.55 ± 2.59 (33.98–37.13) * | 35.50 ± 2.17 (33.93–37.08) *† | 29.95 ± 2.01 (28.38–31.53) & |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matos, F.; Amaral, J.; Martinez, E.; Canário-Lemos, R.; Moreira, T.; Cavalcante, J.; Peixoto, R.; Pinheiro, B.N.; Junior, L.S.; Uchoa, P.; et al. Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 3184. https://doi.org/10.3390/ijerph19063184
Matos F, Amaral J, Martinez E, Canário-Lemos R, Moreira T, Cavalcante J, Peixoto R, Pinheiro BN, Junior LS, Uchoa P, et al. Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults. International Journal of Environmental Research and Public Health. 2022; 19(6):3184. https://doi.org/10.3390/ijerph19063184
Chicago/Turabian StyleMatos, Filipe, João Amaral, Eduardo Martinez, Rui Canário-Lemos, Tiago Moreira, Jurandir Cavalcante, Rafael Peixoto, Bruno Nobre Pinheiro, Lino Scipião Junior, Paulo Uchoa, and et al. 2022. "Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults" International Journal of Environmental Research and Public Health 19, no. 6: 3184. https://doi.org/10.3390/ijerph19063184
APA StyleMatos, F., Amaral, J., Martinez, E., Canário-Lemos, R., Moreira, T., Cavalcante, J., Peixoto, R., Pinheiro, B. N., Junior, L. S., Uchoa, P., Garrido, N., Reis, V. M., Monteiro, G. M., & Vilaça-Alves, J. (2022). Changes in Muscle Thickness after 8 Weeks of Strength Training, Electromyostimulation, and Both Combined in Healthy Young Adults. International Journal of Environmental Research and Public Health, 19(6), 3184. https://doi.org/10.3390/ijerph19063184