
Access to Healthcare and Social Protection among Migrant Workers in Thailand before and during COVID-19 Era: A Qualitative Study

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
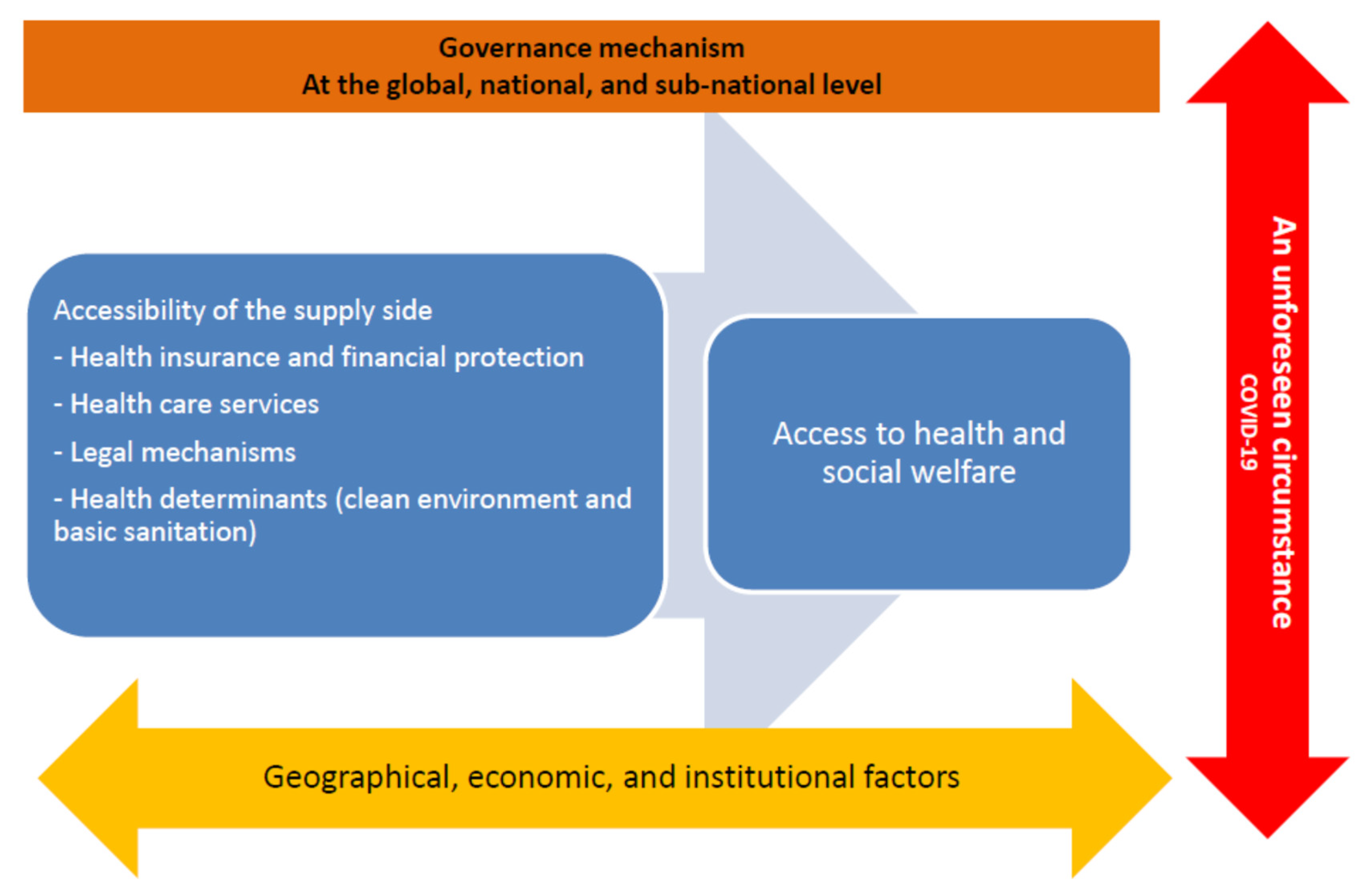
2.1. Study Design and Conceptual Framework
2.2. Samples and Data Collection
2.3. Data Analysis
2.4. Ethics Consideration
3. Results
3.1. Sustainability of the HICS
“I think there should be an independent body to manage the HICS funding which is not the MOPH. We should separate a provider from the funding manager (to prevent COI). The MOPH can be a provider to manage health care services and the health systems overall.”—Public Health Officer PA-5
“As the HICS funding is not that big, we can include more beneficiaries of high-skilled workers to maintain the sustainability of this funding pool. We can also inform them about advantages of HICS packages that cover health promotion and non-communicable diseases in order to compete with private health insurance.”—NGO PA-2
“To set up on a single health insurance system like the UK can be a way to improve health and social equity. For the operational cost, I think this approach could save more money too as the management of different health insurance schemes will become less complex. However, it can be difficult in practice because the UHC law includes only beneficiaries with Thai nationality only.”—Public Health Officer PA-5
3.2. People Dropping out of the SSS
“Some migrant workers stay in Thailand for a short period of time, and some of them often change their employers. So migrants’ employers would not be satisfied once their migrant workers move away and they do not want to pay for the SSS fund because somehow it is not cost effective (even it is legally binding).”—Public Health Officer PA-5
“There is inequity of access to the SSS information between migrant workers and the Thais. Some migrants they do not know once their payment will be sent to the SSS or not. And it is too late that they can use this SSS when they get sick and want to do medical reimbursement. So I would like to see the proper SSS information system to help them track their payment and know their right.”—NGO PA-7
3.3. Quality of Health Screening in MOU Migrants
“The prevalence of HIV and syphilis is more intense in cross-border migrants. It will be more problematic if they get infected from their countries. Also, it means that its transmissibility will be greater in Thailand. Additionally, surveillance system for these infectious diseases is critical and it should be more proactive.”—Health Professional PA-5
“We have already had the health checks from migrant workers’ countries of origin but practically the implementation is not good enough although this is a condition under the MOU. Sometimes our MOL does not care about the health check results. They try to urge them to have work permits at first and then the health check.”—Health Professional PA-17
3.4. Health Screening Problems and State Quarantine Management in Response to COVID-19
“There is a gap in the financial policy to identify who should be the key player responsible for the cost of COVID-19 screening. Currently, the Department of Disease Control is bearing this cost but some told us that the DHEHSF has a direct mission to take care of migrant people. However, the HICS reimbursement does not cover COVID-19. I am so worried about this situation as now the Department of Disease Control and some health facilities have to use their own finances for the screening during this crisis.”—Health Professional PA-17
“It is unclear about the appropriate settings for the state quarantine. Some people suggested that migrants can be quarantined at the factories but we cannot ensure the quality of that. Now there is a negotiation to reduce the cost of state quarantine with a shorter period.”—Health Professional PA-5
3.5. Managing Migration Quota and Dependency on Migrant Workers
“The NESDC should speak out about how many low-skilled migrants should be imported from neighbouring countries within 5 years. This number needs to be identified, along with how many of them can boost the national economy.”—Health Professional PA-1
“In fact we should accept that there are many undocumented migrants in Thailand. We need to know who they are, where they live, and how we can deal with them. The government needs to have a plan and policy to address this issue and report the accurate number of undocumented migrants. Big data system is absent in Thailand which is a way to report and track some personal information systematically such as their ID.”—International Organisation Officer PA-10
3.6. Influx of Migrants in the Backdrop of COVID-19
“COVID-19 is an opportunity to revise the regulation on undocumented migrants. Though this crisis remains in the country, we still need migrant workers. A long-term plan for addressing undocumented migrants should be developed, and it should be not only a 5-year plan but rather 10 years.”—International Organisation Officer PA-10
“Opponents of the military regime will definitely come to Thailand. I am not sure how the local health authorities could deal with it. Actually, there should be temporary camps to help people fleeing from Myanmar but I am not sure whether now it is in place.”—Government Officer PA-15
3.7. Poor Living Condition of Migrants and the Impact of COVID-19
“Our concern is about their poor living conditions. Actually, food and housing are even worse than for Thais. The Ministry of Interior needs to take action to improve their quality of life. Employers have to take care of them. However, many employers, I have heard, also seek decent rooms for their migrant workers. Many of them are living in a small room, and the water quality is also poor.”—Health Professional PA-5
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASEAN | Southeast Asia Nations |
| CLM | Cambodia, Lao PDR, and Myanmar |
| OSS | One Stop Service |
| MOPH | Ministry of Public Health of Thailand |
| MOI | Ministry of Interior |
| MOL | Ministry of Labor |
| MOU | Memorandum of Understanding |
| NV | Nationality Verification |
| UHC | Universal Health Coverage |
| UCS | Universal Coverage Scheme |
| CSMBS | Civil Servant Benefit Scheme |
| SSS | Social Security Scheme |
| HICS | Health Insurance Card Scheme |
| DHEHS | Division of Health Economics and Health Security |
| COI | Conflict of Interest |
| NESDC | National Economic and Social Development Council |
References
- Guinto, R.L.L.R.; Curran, U.Z.; Suphanchaimat, R.; Pocock, N.S. Universal health coverage in One ASEAN: Are migrants included? Glob. Health Action 2015, 8, 25749. [Google Scholar] [CrossRef] [PubMed]
- ASEAN. ASEAN Economic Community Blueprint; Association of Southeast Asian Nations: Jakarta, Indonesia, 2008.
- Suphanchaimat, R.; Putthasri, W.; Prakongsai, P.; Tangcharoensathien, V. Evolution and complexity of government policies to protect the health of undocumented/illegal migrants in Thailand—The unsolved challenges. Risk Manag. Healthc. Policy 2017, 10, 49–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.S. A Theory of Migration. Demography 1966, 3, 47–57. [Google Scholar] [CrossRef]
- De Haas, H. A theory of migration: The aspirations-capabilities framework. Comput. Migr. Stud. 2021, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Castles, S. The Age of Migration: International Population Movements in the Modern World; Macmillan International Higher Education: London, UK, 1998. [Google Scholar]
- Paitoonpong, S.; Chalamwong, Y. Managing International Labor Migration in ASEAN: A Case of Thailand; Association of Southeast Asian Nations: Jakarta, Indonesia, 2012.
- Piore, M.J. Birds of Passage: Migrant Labor and Industrial Societies; Cambridge University Press: New York, NY, USA, 1979. [Google Scholar]
- Pasadilla, G.O. Social Security and Labor Migration in ASEAN; Association of Southeast Asian Nations: Jakarta, Indonesia, 2011.
- Harkins, B. Thailand Migration Report 2019; United Nations Thematic Working Group on Migration in Thailand: Bangkok, Thailand, 2019. [Google Scholar]
- Loganathan, T.; Rui, D.; Ng, C.-W.; Pocock, N.S. Breaking down the barriers: Understanding migrant workers’ access to healthcare in Malaysia. PLoS ONE 2019, 14, e0218669. [Google Scholar] [CrossRef] [Green Version]
- Orcutt, M.; Patel, P.; Burns, R.; Hiam, L.; Aldridge, R.; Devakumar, D.; Kumar, B.; Spiegel, G.; Abubakar, I. Global call to action for inclusion of migrants and refugees in the COVID-19 response. Lancet 2020, 395, 1482–1483. [Google Scholar] [CrossRef]
- Alahmad, B.; Kurdi, H.; Colonna, K.; Gasana, J.; Agnew, J.; Fox, M.A. COVID-19 stressors on migrant workers in Kuwait: Cumulative risk considerations. BMJ Glob. Health 2020, 5, e002995. [Google Scholar] [CrossRef]
- Koh, D. Migrant workers and COVID-19. Occup. Environ. Med. 2020, 77, 634–646. [Google Scholar] [CrossRef]
- Greenaway, C.; Hargreaves, S.; Barkati, S.; Coyle, C.M.; Gobbi, F.; Veizis, A.; Douglas, P. COVID-19: Exposing and addressing health disparities among ethnic minorities and migrants. J. Travel Med. 2020, 27, taaa113. [Google Scholar] [CrossRef]
- Suphanchaimat, R.; Pudpong, N.; Prakongsai, P.; Putthasri, W.; Hanefeld, J.; Mills, A. The Devil Is in the Detail-Understanding Divergence between Intention and Implementation of Health Policy for Undocumented Migrants in Thailand. Int. J. Environ. Res. Public Health 2019, 16, 1016. [Google Scholar] [CrossRef] [Green Version]
- WHO South-East Asia Region. Health of Refugees and Migrants: Parctices in Addressing the Health Needs of Refugees and Migrants. 2018. Available online: https://www.who.int/migrants/publications/PAHO-Practices.pdf (accessed on 30 June 2021).
- Posttoday, A Request from Illegal Migrant Workers for Nationality Verification. Available online: https://www.posttoday.com/social/general/645343 (accessed on 10 August 2021).
- Division of Health Economics and Health Security. Notification of the Ministry of Public Health of Thailand Re: Health Examination and Health Insurance for Migrant Workers 2019. Available online: https://dhes.moph.go.th/?p=4869 (accessed on 22 March 2021).
- Kunpeuk, W.; Teekasap, P.; Kosiyaporn, H.; Julchoo, S.; Phaiyarom, M.; Sinam, P.; Pudpong, N.; Suphanchaimat, R. Understanding the Problem of Access to Public Health Insurance Schemes among Cross-Border Migrants in Thailand through Systems Thinking. Int. J. Environ. Res. Public Health 2020, 17, 5113. [Google Scholar] [CrossRef] [PubMed]
- Tangcharoensathien, V.; Patcharanarumol, W. The Political Economy of UHC Reform in Thailand: Lessons for Low- and Middle-Income Countries. Health Syst. Reform 2019, 5, 195–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Employment. Ministry of Labour of Thailand. Guidelines for Documented Migrant Workers in Thailand. Available online: https://bit.ly/2WkFkFC (accessed on 1 July 2021).
- Bangkokpost. Don’t Leave Migrant Workers Behind. Available online: https://www.bangkokpost.com/business/2154731/dont-leave-migrant-workers-behind (accessed on 10 August 2021).
- Thailand Development Research Institute. The Impact of COVID-19 on the Mangement of Migrant Workers in Thailand. 2020. Available online: https://tdri.or.th/2020/08/covid-19-impact-on-migrant-workers/ (accessed on 23 March 2021).
- National News Bureau of Thailand. Infectious and High-Risk Areas in Greater Bangkok Will Be Closed Off. Available online: https://thainews.prd.go.th/en/news/detail/TCATG210626111504398 (accessed on 10 August 2021).
- Thairath. Cancellation on Active Case Finding in Documented Migrant Workers: Failure of the Thai Government with Ignorance of Migrant Workers in the Country. Available online: https://www.thairath.co.th/scoop/theissue/2141952 (accessed on 10 August 2021).
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Dhavan, P.; Fouad, J.M.; Groce, M.; Guo, Y.; et al. The UCL–Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef] [Green Version]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OHCHR. Principles and Guidelines, Supported by Practical Guidance, on the Human Rights Protection of Migrants in Vulnerable Situations Reports A/HRC/37/34 9. Available online: https://www.ohchr.org/Documents/Issues/Migration/OHCHR_slow_onset_of_Climate_Change_ENweb.pdf (accessed on 31 January 2022).
- Poungkanta, W.; Suphanchaimat, R. Health insurance for undocumented migrants: A literature review in developed countries. J. Med. Assoc. Thail. 2017, 100, 716–726. [Google Scholar]
- Witthayapipopsakul, W.; Kulthanmanusorn, A.; Vongmongkol, V.; Viriyathorn, S.; Wanwong, Y.; Tangcharoensathien, V. Achieving the targets for universal health coverage: How is Thailand monitoring progress? WHO South-East Asia J. Public Health. 2019, 8, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Prachachat, The Social Security Scheme for Migrant Workers in Thailand is the Same as the Thais. Available online: https://www.prachachat.net/csr-hr/news-325611 (accessed on 7 July 2021).
- Ministry of Labor of Thailand. New Normal during the COVID-19 and Labor of Thailand: Get through the COVID-19 Together. E-Mag. Min. Labor Thai. Bang. 2021, 36, 1–16. [Google Scholar]
- Thai Civil Rights and Investigate Journalism. Migrant Employers Asked for Subsidies on Health Screeing and State Quarantine before Importing Migrant Workers in Thailand. Available online: https://www.tcijthai.com/news/2020/7/scoop/10722 (accessed on 7 July 2021).
- The Ministry of Public Health of Thailand. Minute of the Meeting on Healthcare Intervention and Services for Migrants, Migrant Workers, Refugees, and Stateless Persons in Thailand during COVID-19 as of 29 April 2020. Available online: http://www.cbo.moph.go.th:8080/welfare/document_files/20200526-1590474881.pdf (accessed on 7 July 2021).
- Puey Ungphakorn Institute for Economic Research. Facts about Migrant Workers in Thailand: Chapter 1 Low-Skilled Workers through the Lens of the Social Security Fund. 2020. Available online: https://www.pier.or.th/abridged/2020/14/ (accessed on 22 March 2021).
- Hfocus. The Results of the Public Poll regarding Ilegal Migration and COVID-19. 2021. Available online: https://www.hfocus.org/content/2021/02/21049 (accessed on 22 March 2021).
- Ministry of Interior of Thailand. Notification of the Ministry of Interior of Thailand Re: Permission on Visa Extension for Specific Grooups of Migrant Workers in Thailand during the Situation of COVID-19. Available online: http://www.ratchakitcha.soc.go.th/DATA/PDF/2563/E/305/T_0012.PDF (accessed on 22 March 2020).
- Bangkokpost. Myanmar Protests Pose Virus Threat. Available online: https://www.bangkokpost.com/thailand/general/2072171/myanmar-protests-pose-virus-threat (accessed on 16 June 2021).
- DW News. Thousands Flee Military to Thailand-Myanmar Border Region. Available online: https://www.dw.com/en/thousands-flee-military-to-thailand-myanmar-border-region/a-57007896 (accessed on 16 June 2021).
- International Organization for Migration. COVID-19 Rapid Needs Assessment: Mahachai Sub-District Samut Sakhon Province (Round 4). 2021. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/R4%20Needs%20Assessment_Mahachai_0.pdf (accessed on 23 March 2021).
- Ministry of Public Health of Thailand. Data on the HICS Registry with Valid Status. Available online: https://data.go.th/tr/dataset/dhesmoph (accessed on 21 July 2021).
- Herberholz, C. The Role of External Actors in Shaping Migrant Health Insurance in Thailand. PLoS ONE 2020, 15, e0234642. [Google Scholar] [CrossRef]
- Loganathan, T.; Chan, Z.X.; Pocock, N.S. Healthcare financing and social protection policies for migrant workers in Malaysia. PLoS ONE 2020, 15, e0243629. [Google Scholar] [CrossRef]
- Department of Statistics Malaysia. Key Statistics of Labour Force in Malaysia, July 2018; Department of Statistics Malaysia: Putrajaya, Malaysia, 2018.
- Hacker, K.; Anies, M.E.; Folb, B.; Zallman, L. Barriers to health care for undocumented immigrants: A literature review. Risk Manag. Health Policy 2015, 8, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Chuah, F.L.H.; Tan, S.T.; Yeo, J.; Legido-Quigley, H. Health System Responses to the Health Needs of Refugees and Asylum-seekers in Malaysia: A Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajaraman, N.; Yip, T.-W.; Kuan, B.Y.H.; Lim, J.F.Y. Exclusion of Migrant Workers from National UHC Systems—Perspectives from HealthServe, a Non-profit Organisation in Singapore. Asian Bioeth. Rev. 2020, 12, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Manpower. Foreign Workers Continue to Rate Working in Singapore Favourably in Latest Survey: Pay, Living Conditions, Safety and Security Commonly Cited Reasons. 2019. Available online: https://www.mom.gov.sg/newsroom/press-releases/2019/0609-foreign-workers-continue-to-rate-working-in-singaporefavourably-in-latest-survey (accessed on 8 July 2021).
- Ang, J.W.; Chia, C.; Koh, C.J.; Chua, B.W.B.; Narayanaswamy, S.; Wijaya, L.; Chan, L.G.; Goh, W.L.; Vasoo, S. Healthcare-seeking behaviour, barriers and mental health of non-domestic migrant workers in Singapore. BMJ Glob. Health 2017, 2, e000213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, J.; Koh, C.; Chua, B.; Narayanaswamy, S.; Wijaya, L.; Chan, L.; Soh, L.; Goh, W.; Vasoo, S. Are migrant workers in Singapore receiving adequate healthcare? A survey of doctors working in public tertiary healthcare institutions. Singap. Med. J. 2020, 61, 540–547. [Google Scholar] [CrossRef]
- Berger, Z.D.; Evans, N.G.; Phelan, A.; Silverman, R.D. COVID-19: Control measures must be equitable and inclusive. BMJ 2020, 368, m1141. [Google Scholar] [CrossRef] [Green Version]
- Hrynick, T.A.; Lorenzo, S.R.; Carter, S.E. COVID-19 response: Mitigating negative impacts on other areas of health. BMJ Glob. Health 2021, 6, e004110. [Google Scholar] [CrossRef]
- WHO. Neglected Tropical Diseases: Leveraging the New NTD Road Map to Build Back from COVID-19 Disruptions. 2020. Available online: https://www.who.int/news/item/19-06-2020-neglected-tropical-diseases-leveraging-the-new-ntd-road-map-to-build-back-from-covid-19-disruptions (accessed on 31 January 2022).
- Goh, O.Q.; Islam, A.M.; Lim, J.C.; Chow, W.-C. Towards health market systems changes for migrant workers based on the COVID-19 experience in Singapore. BMJ Glob. Health 2020, 5, e003054. [Google Scholar] [CrossRef]
- Yi, H.; Ng, S.T.; Farwin, A.; Low, A.P.T.; Chang, C.M.; Lim, J. Health equity considerations in COVID-19: Geospatial network analysis of the COVID-19 outbreak in the migrant population in Singapore. J. Travel Med. 2020, 28, taaa159. [Google Scholar] [CrossRef]
- Chiew, C.J.; Li, Z.; Lee, V.J. Reducing onward spread of COVID-19 from imported cases: Quarantine and stay at home measures for travellers and returning residents to Singapore. J. Travel Med. 2020, 27, e003054. [Google Scholar] [CrossRef] [Green Version]
- Archuleta, S.; Cross, G.; Somani, J.; Lum, L.; Santosa, A.; Alagha, R.A.; Allen, D.M.; Ang, A.; Beh, D.; Chai, L.; et al. Responding to COVID-19: How an academic infectious diseases division mobilized in Singapore. BMC Med. 2020, 18, 179. [Google Scholar] [CrossRef]
- Lee, V.J.; Chiew, C.J.; Khong, W.X. Interrupting transmission of COVID-19: Lessons from containment efforts in Singapore. J. Travel Med. 2020, 27, taaa039. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Code | Gender | Experience (Years) | Career Level | Organization |
|---|---|---|---|---|
| PA-1 | Male | >10 | Senior | Health sector (beyond the government) |
| PA-2 | Male | >10 | Middle | NGOs 1 (migrant working group) |
| PA-3 | Female | 5–10 | Middle | MOPH 2 |
| PA-4 | Male | >10 | Senior | MOPH 2 |
| PA-5 | Male | >10 | Senior | MOPH 2 |
| PA-6 | Male | >10 | Senior | Government |
| PA-7 | Male | >10 | Middle | NGOs 1 (migrant working group) |
| PA-8 | Female | >10 | Senior | NGOs 1 (Thai social foundation) |
| PA-9 | Male | >10 | Senior | Government |
| PA-10 | Female | >10 | Middle | NGOs 1 (international) |
| PA-11 | Female | >10 | Middle | NGOs 1 (international) |
| PA-12 | Female | >10 | Senior | NGOs 1 (international) |
| PA-13 | Female | 5–10 | Middle | NGOs 1 (migrant working group) |
| PA-14 | Female | <5 | Middle | MOPH 2 |
| PA-15 | Female | >10 | Senior | Health sector (beyond the government) |
| PA-16 | Female | >10 | Middle | Academic |
| PA-17 | Male | 5–10 | Senior | MOPH 2 |
| PA-18 | Male | >10 | Senior | Academic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunpeuk, W.; Julchoo, S.; Phaiyarom, M.; Sinam, P.; Pudpong, N.; Loganathan, T.; Yi, H.; Suphanchaimat, R. Access to Healthcare and Social Protection among Migrant Workers in Thailand before and during COVID-19 Era: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 3083. https://doi.org/10.3390/ijerph19053083
Kunpeuk W, Julchoo S, Phaiyarom M, Sinam P, Pudpong N, Loganathan T, Yi H, Suphanchaimat R. Access to Healthcare and Social Protection among Migrant Workers in Thailand before and during COVID-19 Era: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(5):3083. https://doi.org/10.3390/ijerph19053083
Chicago/Turabian StyleKunpeuk, Watinee, Sataporn Julchoo, Mathudara Phaiyarom, Pigunkaew Sinam, Nareerut Pudpong, Tharani Loganathan, Huso Yi, and Rapeepong Suphanchaimat. 2022. "Access to Healthcare and Social Protection among Migrant Workers in Thailand before and during COVID-19 Era: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 5: 3083. https://doi.org/10.3390/ijerph19053083
APA StyleKunpeuk, W., Julchoo, S., Phaiyarom, M., Sinam, P., Pudpong, N., Loganathan, T., Yi, H., & Suphanchaimat, R. (2022). Access to Healthcare and Social Protection among Migrant Workers in Thailand before and during COVID-19 Era: A Qualitative Study. International Journal of Environmental Research and Public Health, 19(5), 3083. https://doi.org/10.3390/ijerph19053083