
Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety at the Start of the Pandemic: Differences by Gender and Race


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Measures
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Demographics
3.2. Multiple Regression Model
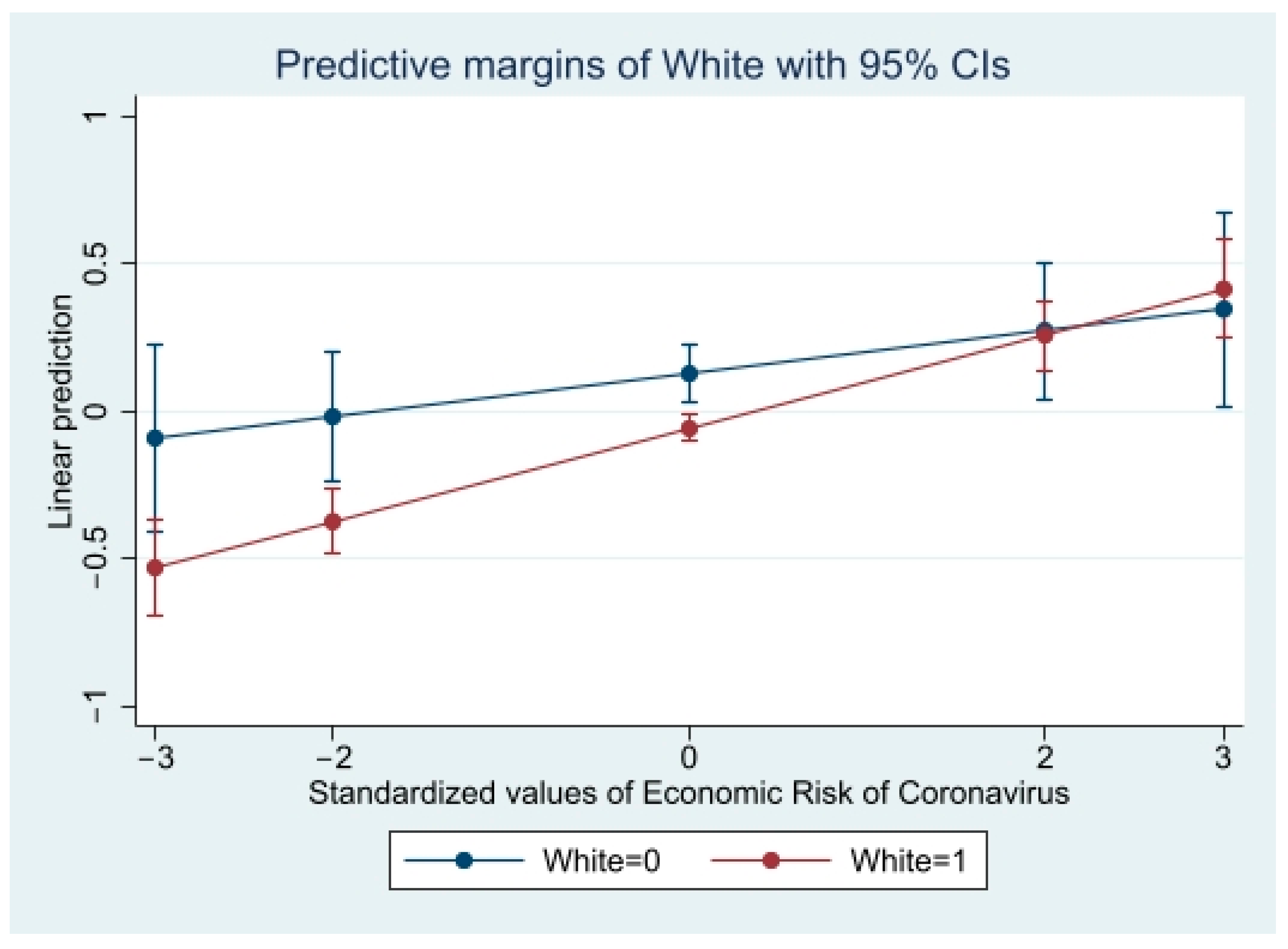
3.3. Interaction Models
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Twenge, J.M.; Joiner, T.E. US Census Bureau-assessed prevalence of anxiety and depressive symptoms in 2019 and during the 2020 COVID-19 pandemic. Depress. Anxiety 2020, 37, 954–956. [Google Scholar] [CrossRef]
- CDC Museum COVID-19 Timeline. Available online: https://www.cdc.gov/museum/timeline/covid19.html (accessed on 22 November 2021).
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unützer, J.; Kimmel, R.J.; Snowden, M. Psychiatry in the age of COVID-19. World Psychiatry 2020, 19, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Yarrington, J.S.; Lasser, J.; Garcia, D.; Vargas, J.H.; Couto, D.D.; Marafon, T.; Craske, M.G.; Niles, A.N. Impact of the COVID-19 pandemic on mental health among 157,213 Americans. J. Affect. Disord. 2021, 286, 64–70. [Google Scholar] [CrossRef]
- Simpson, H.B.; Neria, Y.; Lewis-Fernández, R.; Schneier, F. Anxiety Disorders: Theory, Research and Clinical Perspectives; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germani, A.; Buratta, L.; Delvecchio, E.; Gizzi, G.; Mazzeschi, C. Anxiety severity, perceived risk of COVID-19 and individual functioning in emerging adults facing the pandemic. Front. Psychol. 2020, 11, 3384. [Google Scholar] [CrossRef]
- Faasse, K.; Newby, J. Public perceptions of COVID-19 in Australia: Perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front. Psychol. 2020, 11, 2553. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249–250. [Google Scholar] [CrossRef]
- Kan, F.P.; Raoofi, S.; Rafiei, S.; Khani, S.; Hosseinifard, H.; Tajik, F.; Raoofi, N.; Ahmadi, S.; Aghalou, S.; Torabi, F.; et al. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. J. Affect. Disord. 2021, 293, 391–398. [Google Scholar]
- Khubchandani, J.; Sharma, S.; Webb, F.J.; Wiblishauser, M.J.; Bowman, S.L. Post-lockdown depression and anxiety in the USA during the COVID-19 pandemic. J. Public Health 2021, 43, 246–253. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Hofmann, S.A. Racial disparities in COVID-19 anxiety and adversity. Traumatology 2021, 27, 465–470. [Google Scholar] [CrossRef]
- Mann, F.D.; Krueger, R.F.; Vohs, K.D. Personal economic anxiety in response to COVID-19. Personal. Individ. Differ. 2020, 167, 110233. [Google Scholar] [CrossRef] [PubMed]
- Schafer, K.M.; Lieberman, A.; Sever, A.C.; Joiner, T. Prevalence rates of anxiety, depressive, and eating pathology symptoms between the pre-and peri-COVID-19 eras: A meta-analysis. J. Affect. Disord. 2022, 298, 364–372. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders; Penguin: London, UK, 1979. [Google Scholar]
- Rimal, R.N.; Real, K. Perceived risk and efficacy beliefs as motivators of change: Use of the risk perception attitude (RPA) framework to understand health behaviors. Hum. Commun. Res. 2003, 29, 370–399. [Google Scholar] [CrossRef]
- Turner, M.M.; Rimal, R.N.; Morrison, D.; Kim, H. The role of anxiety in seeking and retaining risk information: Testing the risk perception attitude framework in two studies. Hum. Commun. Res. 2006, 32, 130–156. [Google Scholar] [CrossRef]
- Buchanan, T.; Selmon, N. Race and gender differences in self-efficacy: Assessing the role of gender role attitudes and family background. Sex Roles 2008, 58, 822–836. [Google Scholar] [CrossRef]
- Rodriguez-Besteiro, S.; Tornero-Aguilera, J.F.; Fernández-Lucas, J.; Clemente-Suárez, V.J. Gender differences in the covid-19 pandemic risk perception, psychology and behaviors of spanish university students. Int. J. Environ. Res. Public Health 2021, 18, 3908. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.-X.; Chen, Y.-M.; Chen, W.-Q. Association of psychosocial factors with anxiety and depressive symptoms in Chinese patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2008, 79, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Leppin, A.; Aro, A.R. Risk perceptions related to SARS and avian influenza: Theoretical foundations of current empirical research. Int. J. Behav. Med. 2009, 16, 7–29. [Google Scholar] [CrossRef] [Green Version]
- Frankham, C.; Richardson, T.; Maguire, N. Psychological factors associated with financial hardship and mental health: A systematic review. Clin. Psychol. Rev. 2020, 77, 101832. [Google Scholar] [CrossRef]
- US Census Bureau QuickFacts: United States. 2019. Available online: https://www.census.gov/quickfacts/fact/table/CA,US/PST045219 (accessed on 22 November 2021).
- Du, J.; Dong, L.; Wang, T.; Yuan, C.; Fu, R.; Zhang, L.; Liu, V.; Zhang, M.; Yin, Y.; Qin, J.; et al. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen. Hosp. Psychiatry 2020, 67, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline Nurses’ Burnout, Anxiety, Depression, and Fear Statuses and Their Associated Factors During the COVID-19 Outbreak in Wuhan, China: A Big-Scale Cross-Sectional Study. eClinicalMedicine 2020, 24, 100424. [Google Scholar]
- Personality, Attitudes, aNd Individual Differences Regarding the Coronavirus Pandemic (PANIC). Available online: https://osf.io/dkv2s/?view_only=e522a25ac66d484e9afaa2644af25e89 (accessed on 8 October 2021).
- Niepel, C.; Kranz, D.; Borgonovi, F.; Emslander, V.; Greiff, S. The coronavirus (COVID-19) fatality risk perception of US adult residents in March and April 2020. Br. J. Health Psychol. 2020, 25, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Sailer, M.; Stadler, M.; Botes, E.; Fischer, F.; Greiff, S. Science knowledge and trust in medicine affect individuals’ behavior in pandemic crises. Eur. J. Psychol. Educ. 2022, 37, 279–292. [Google Scholar] [CrossRef]
- Kranz, D.; Niepel, C.; Botes, E.; Greiff, S. Religiosity predicts unreasonable coping with COVID-19. Psychol. Relig. Spirit. 2020; Advance online publication. [Google Scholar]
- Schönbrodt, F.D.; Perugini, M. At what sample size do correlations stabilize? J. Res. Personal. 2013, 47, 609–612. [Google Scholar] [CrossRef] [Green Version]
- Prolific Team. Representative Samples FAQ. 2021. Available online: https://researcher-help.prolific.co/hc/en-gb/articles/360019238413-Representative-samples-FAQ (accessed on 22 November 2021).
- Grös, D.F.; Antony, M.M.; Simms, L.J.; McCabe, R.E. Psychometric properties of the state-trait inventory for cognitive and somatic anxiety (STICSA): Comparison to the state-trait anxiety inventory (STAI). Psychol. Assess. 2007, 19, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.E.; Davidson, R.J.; Goleman, D.J. Patterning of cognitive and somatic processes in the self-regulation of anxiety: Effects of meditation versus exercise. Psychosom. Med. 1978, 40, 321–328. [Google Scholar] [CrossRef]
- Chen, G.; Gully, S.M.; Eden, D. Validation of a new general self-efficacy scale. Organ. Res. Methods 2001, 4, 62–83. [Google Scholar] [CrossRef] [Green Version]
- Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety. Available online: https://osf.io/m759h/?view_only=d765fcd5713f43bd8fec0f8b5d42bce3 (accessed on 8 October 2021).
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: New York, NY, USA, 2007. [Google Scholar]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, A.; Shaw, E.; Lewis, K.V. The collaborative dynamic in social entrepreneurship. Am. J. Prev. Med. 2020, 59, 157–167. [Google Scholar]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A. Mental health characteristics associated with dysfunctional coronavirus anxiety. Psychol. Med. 2021, 51, 1403–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holingue, C.; Kalb, L.G.; Riehm, K.E.; Bennett, D.; Kapteyn, A.; Veldhuis, C.B.; Johnson, R.M.; Fallin, M.D.; Kreuter, F.; Stuart, E.A.; et al. Mental distress in the United States at the beginning of the COVID-19 pandemic. Am. J. Public Health 2020, 110, 1628–1634. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, M.; Li, Y.; Chung, J.E. Teens’ Social Media Engagement during the COVID-19 Pandemic: A Time Series Examination of Posting and Emotion on Reddit. Int. J. Environ. Res. Public Health 2021, 18, 10079. [Google Scholar] [CrossRef]
- Witte, K. A theory of cognition and negative affect: Extending Gudykunst and Hammer’s theory of uncertainty and anxiety reduction. Int. J. Intercult. Relat. 1993, 17, 197–215. [Google Scholar] [CrossRef]
- Witte, K.; Allen, M. A meta-analysis of fear appeals: Implications for effective public health campaigns. Health Educ. Behav. 2020, 27, 591–615. [Google Scholar] [CrossRef] [PubMed]
- Fetzer, T.; Hensel, L.; Hermle, J.; Roth, C. Coronavirus perceptions and economic anxiety. Rev. Econ. Stat. 2021, 103, 968–978. [Google Scholar] [CrossRef]
- Fitch, C.; Hamilton, S.; Bassett, P.; Davey, R. The relationship between personal debt and mental health: A systematic review. Ment. Health Rev. J. 2011, 16, 153–166. [Google Scholar] [CrossRef]
- Parmar, D.; Stavropoulou, C.; Ioannidis, J.P. Health outcomes during the 2008 financial crisis in Europe: Systematic literature review. BMJ 2016, 354, i4588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Measuring Better: Development of ‘True Rate of Unemployment’ Data as the Basis for Social and Economic Policy; The Ludwig Institute for Shared Economic Prosperity (LISEP): Washington, DC, USA, 2020; Available online: https://assets.website-files.com/5f67c16a6ca3251ecc11eca7/5fd77b946b8ccc555b8cc6e5_November%20White%20Paper%201220.pdf (accessed on 8 October 2021).
- Kobayashi, T.; Maeda, M.; Takebayashi, Y.; Sato, H. Traditional gender differences create gaps in the effect of COVID-19 on psychological distress of Japanese workers. Int. J. Environ. Res. Public Health 2021, 18, 8656. [Google Scholar] [CrossRef] [PubMed]
- Schönfeld, P.; Brailovskaia, J.; Bieda, A.; Zhang, X.C.; Margraf, J. The effects of daily stress on positive and negative mental health: Mediation through self-efficacy. Int. J. Clin. Health Psychol. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Rosenzweig, C.; Moss, A.J.; Litman, L. Tapped out or barely tapped? Recommendations for how to harness the vast and largely unused potential of the Mechanical Turk participant pool. PLoS ONE 2019, 14, e0226394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prolific. 2020. Available online: https://researcher-help.prolific.co/hc/en-gb/articles/360009501473-What-are-the-advantages-and-limitations-of-an-online-sample- (accessed on 2 November 2020).
- Kennedy, C.; Mercer, A.; Keeter, S.; Hatley, N.; McGeeney, K.; Gimenez, A. Evaluating Online Nonprobability Surveys; Pew Research Center: Washington, DC, USA, 2016; Available online: https://www.pewresearch.org/methods/2016/05/02/evaluating-online-nonprobability-surveys/ (accessed on 8 October 2021).
- Wright, K.B. Researching Internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J. Comput. Mediat. Commun. 2005, 10, JCMC1034. [Google Scholar] [CrossRef]
- Palan, S.; Schitter, C. Prolific. ac—A subject pool for online experiments. J. Behav. Exp. Financ. 2018, 17, 22–27. [Google Scholar] [CrossRef]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry 2020, 19, 406–407. [Google Scholar] [CrossRef]
- McDaid, D. Viewpoint: Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry 2021, 64, e32. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Sample Total (N = 1182) | β (p) |
|---|---|---|
| Coronavirus Anxiety | 2.49 ± 0.66 | - |
| Coronavirus crisis perception, a,b mean ± SD | 3.82 ± 0.83 | 0.42 (<0.001) |
| Perceived economic risk of Coronavirus, a,c mean ± SD | 3.89 ± 0.99 | 0.23 (<0.001) |
| General self-efficacy, a,d mean ± SD | 3.71 ± 0.72 | −0.12 (<0.001) |
| Gender, e n (%) | ||
| Female f | 596 (50.42) | 0.07 (0.04) |
| Male f | 574 (48.56) | −0.08 (0.01) |
| Other f | 12 (1.02) | 0.02 (0.43) |
| Race, g n (%) | −0.16 (<0.001) | |
| African American | 141 (11.93) | |
| Asian | 64 (5.41) | |
| Hispanic | 47 (3.98) | |
| Native American | 7 (0.59) | |
| Non-Hispanic White | 903 (76.40) | |
| Other | 20 (1.69) | |
| Annual Income, e,h n (%) | −0.01 (0.42) | |
| No personal income | 30 (2.54) | |
| Less than USD 20,000 | 179 (15.17) | |
| USD 20,000 to USD 34,999 | 190 (16.07) | |
| USD 35,000 to USD 49,999 | 190 (16.07) | |
| USD 50,000 to USD 74,999 | 215 (18.19) | |
| USD 75,000 to USD 99,999 | 144 (12.18) | |
| USD 100,000 up to USD 114,999 | 77 (6.51) | |
| USD 115,000 up to USD 129,999 | 45 (3.81) | |
| USD 130,000 or more | 95 (8.04) | |
| Do not wish to respond | 17 (1.44) | |
| Education level, f,i n (%) | −0.01 (0.80) | |
| Less than a high school diploma | 6 (0.51) | |
| High school diploma or equivalent | 124 (10.49) | |
| Some college, no degree | 269 (22.76) | |
| Associate’s degree | 139 (11.76) | |
| Bachelor’s degree | 414 (35.03) | |
| Master’s degree | 155 (13.11) | |
| Professional degree | 33 (2.79) | |
| Doctorate degree | 33 (2.79) | |
| Vocational training/trade | 7 (0.59) | |
| Other; specify | 2 (0.17) | |
| Age (years), f mean ± SD | 45.6 ± 15.7 | −0.001 (0.08) |
| Employment, f,j n (%) | −0.03 (0.38) | |
| Employed full time (≥40 h/week) | 428 (36.21) | |
| Employed part time (<40 h/week) | 157 (13.28) | |
| Unemployed and currently looking for work | 78 (6.60) | |
| Unemployed and currently not looking for work | 12 (1.02) | |
| Student | 61 (5.16) | |
| Retired | 176 (14.89) | |
| Homemaker | 63 (5.33) | |
| Self-employed | 161 (13.62) | |
| Unable to work | 46 (3.89) |
| Coronavirus Anxiety ab | ||
|---|---|---|
| β (95% CI) | p-Value | |
| Coronavirus crisis perception c | 0.46 (0.41, 1.00) | <0.001 |
| Perceived economic crisis of Coronavirus d | 0.14 (0.09, 1.00) | <0.001 |
| Self-efficacy e | −0.15 (−1.00, −0.11) | <0.001 |
| Coronavirus Anxiety ab | ||
|---|---|---|
| β (95% CI) | p-Value | |
| Interaction Model by Gender | ||
| Coronavirus crisis perception c | 0.40 (0.34, 1.00) | <0.001 |
| Perceived economic crisis of Coronavirus d | 0.14 (0.10, 1.00) | <0.001 |
| Self-efficacy e | −0.15 (−1.00, −0.10) | <0.001 |
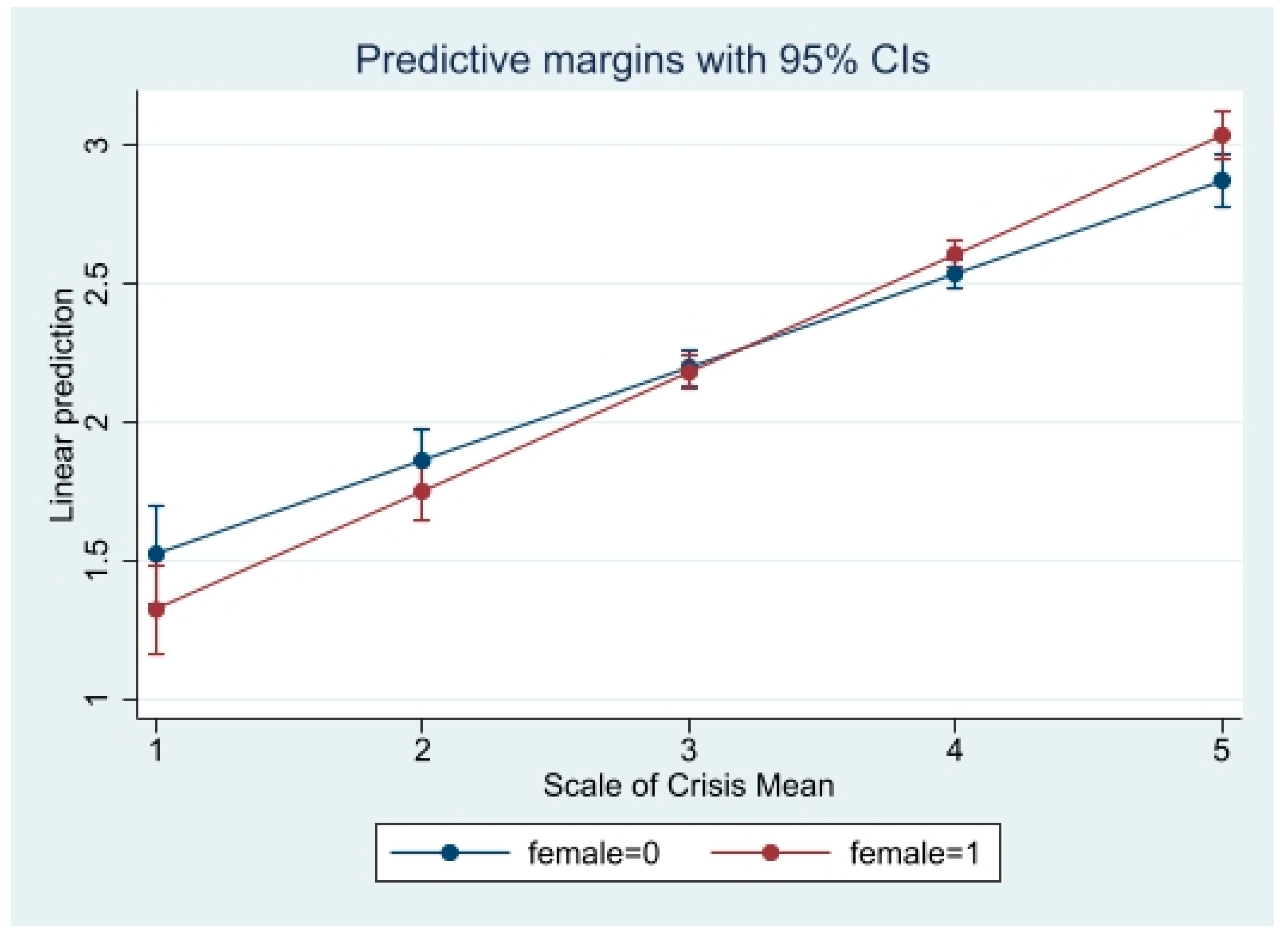
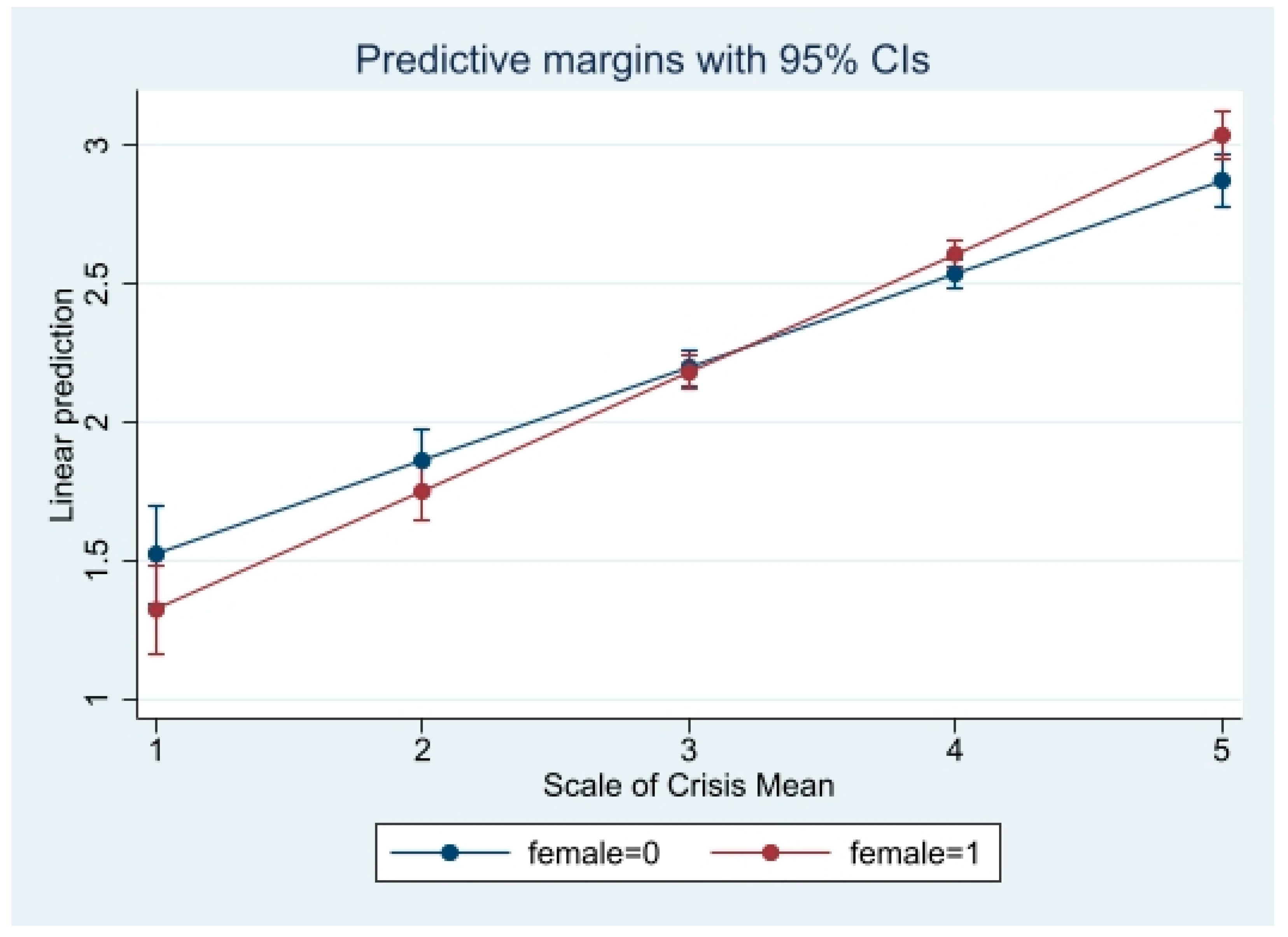
| Coronavirus crisis perception c * gender (female = ref) | 0.11 (0.03, 1.00) | 0.01 |
| Interaction Model by Race | ||
| Coronavirus crisis perception c | 0.32 (0.19, 1.00) | <0.001 |
| Perceived economic crisis of Coronavirus d | 0.14 (0.09, 1.00) | <0.001 |
| Self-efficacy e | −0.15 (−1.00, −0.11) | <0.001 |
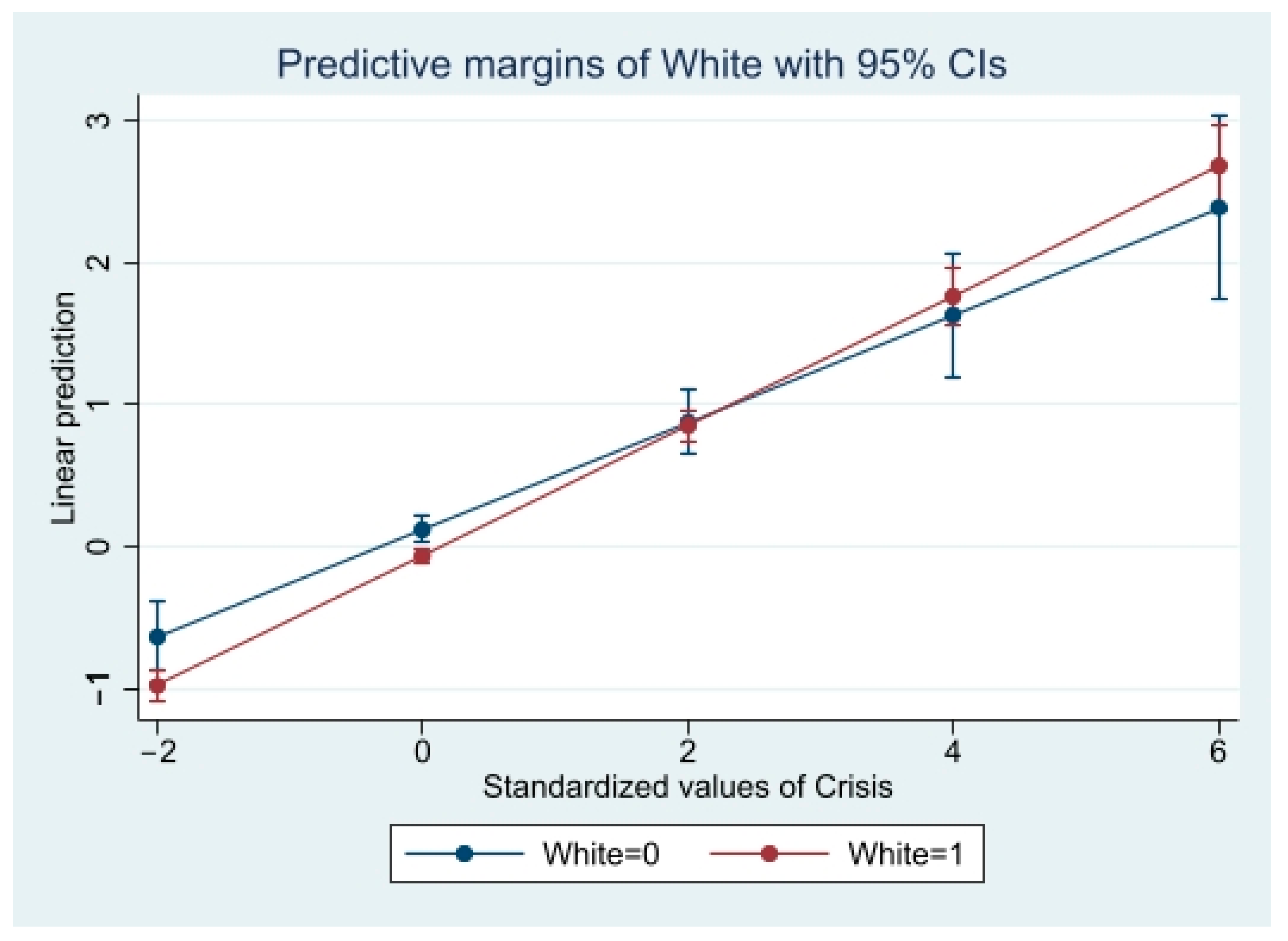
| Coronavirus crisis perception c * race (White = ref) | 0.17 (0.03, 1.00) | 0.02 |
| Interaction Model by Race | ||
| Coronavirus crisis perception c | 0.46 (0.41, 1.00) | <0.001 |
| Perceived economic crisis of Coronavirus d | 0.05 (−0.04, 1.00) | 0.35 |
| Self-efficacy e | −0.16 (−1.00, −0.10) | <0.001 |
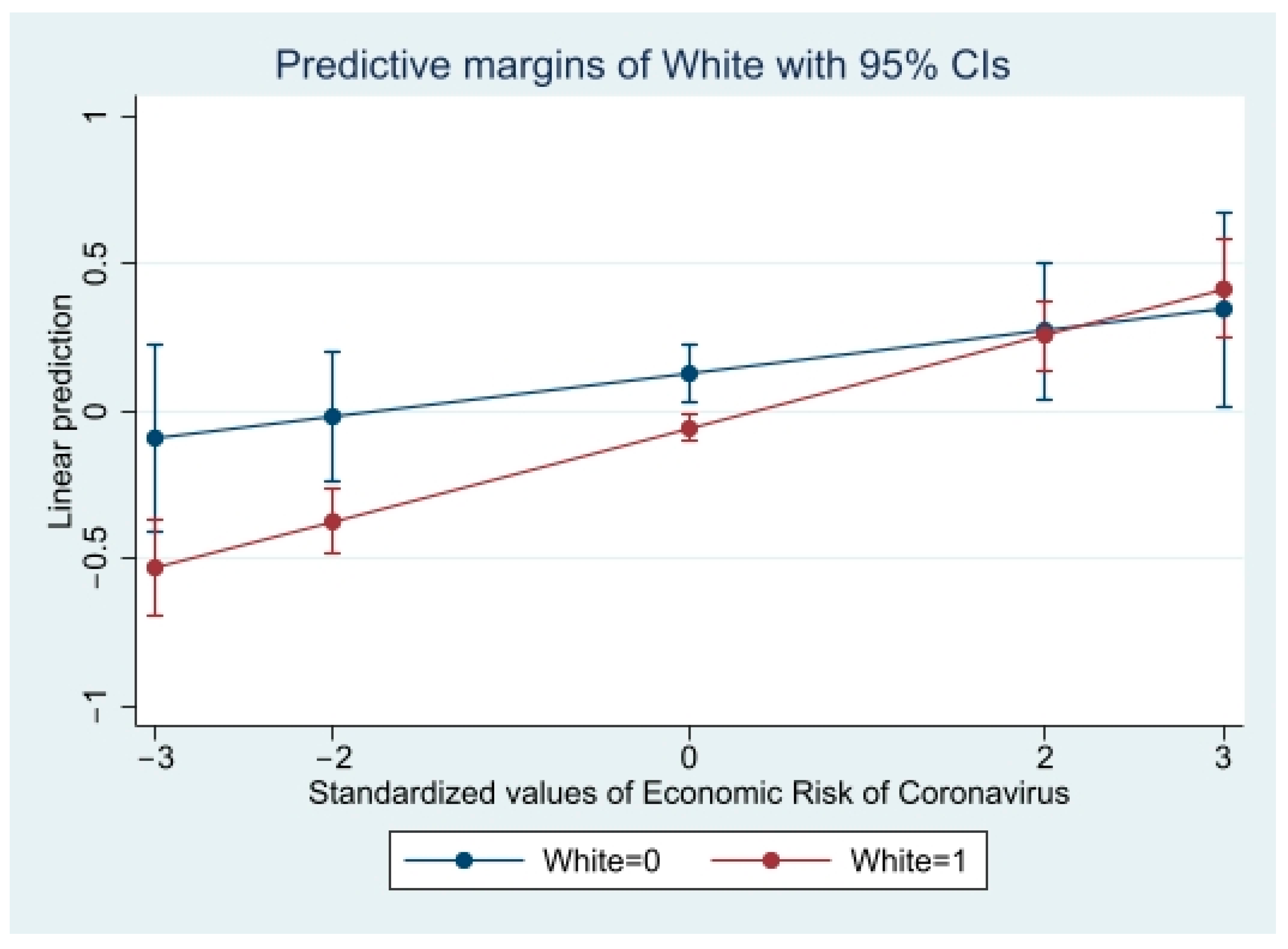
| Perceived economic crisis of Coronavirus d * race (White = ref) | 0.11 (0.01, 1.00) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, S.; Hopfer, S.; Botes, E.; Greiff, S. Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety at the Start of the Pandemic: Differences by Gender and Race. Int. J. Environ. Res. Public Health 2022, 19, 2872. https://doi.org/10.3390/ijerph19052872
Garcia S, Hopfer S, Botes E, Greiff S. Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety at the Start of the Pandemic: Differences by Gender and Race. International Journal of Environmental Research and Public Health. 2022; 19(5):2872. https://doi.org/10.3390/ijerph19052872
Chicago/Turabian StyleGarcia, Samantha, Suellen Hopfer, Elouise Botes, and Samuel Greiff. 2022. "Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety at the Start of the Pandemic: Differences by Gender and Race" International Journal of Environmental Research and Public Health 19, no. 5: 2872. https://doi.org/10.3390/ijerph19052872
APA StyleGarcia, S., Hopfer, S., Botes, E., & Greiff, S. (2022). Associations between Coronavirus Crisis Perception, Perceived Economic Risk of Coronavirus, General Self-Efficacy, and Coronavirus Anxiety at the Start of the Pandemic: Differences by Gender and Race. International Journal of Environmental Research and Public Health, 19(5), 2872. https://doi.org/10.3390/ijerph19052872