
Nurses’ Knowledge about Delirium in the Group of Intensive Care Units Patients

 ,
,  ,
, 

{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
2.3. Participants
2.4. Inclusion and Exclusion Criteria
2.5. Data Analysis
2.6. Training Plan
- In the first part of the training, nurses were introduced to the problem of delirium in Poland and around the world, as well as the factors influencing the formation of delirium and its complications.
- In the second stage, the nurses watched a short 18 min video recording of a conversation with a patient who had experienced delirium at the ICU.
- Another element of the training included listening to a recording that was recorded during one of the CSICU night shifts. On the recording, you can hear conversations, laughter, shuffling chairs, alarms of cameras, closing lockers, etc.
- Nurses, after watching the film and listening to the recording, shared their own experiences of working with delirium patients. Nurses were informed that their statements were confidential in the group they were in.
- The next stage was related to making nurses aware of the consequences of decisions made in caring for a delirious patient.
- The effects and side-effects of sedative and analgesic drugs were discussed.
- During the training, they were presented with the legal consequences of using drugs without a doctor’s order. They were also presented with various tools that can be used to assess delirium in the ICU (CAM-ICU, 4AT, NuDesc).
- Particular attention was paid to how to talk to delirious patients and their families. At the end of the meeting, nurses received an information booklet, produced in collaboration with Health Improvement Scotland. The brochure is available at https://ptpaio.pl/dokumenty/96.pdf [6]. As a result of the training, there was a discussion that the training brought a lot of information about delirium, actions, and their consequences, about which nurses had not known so far.
3. Results
3.1. First Round
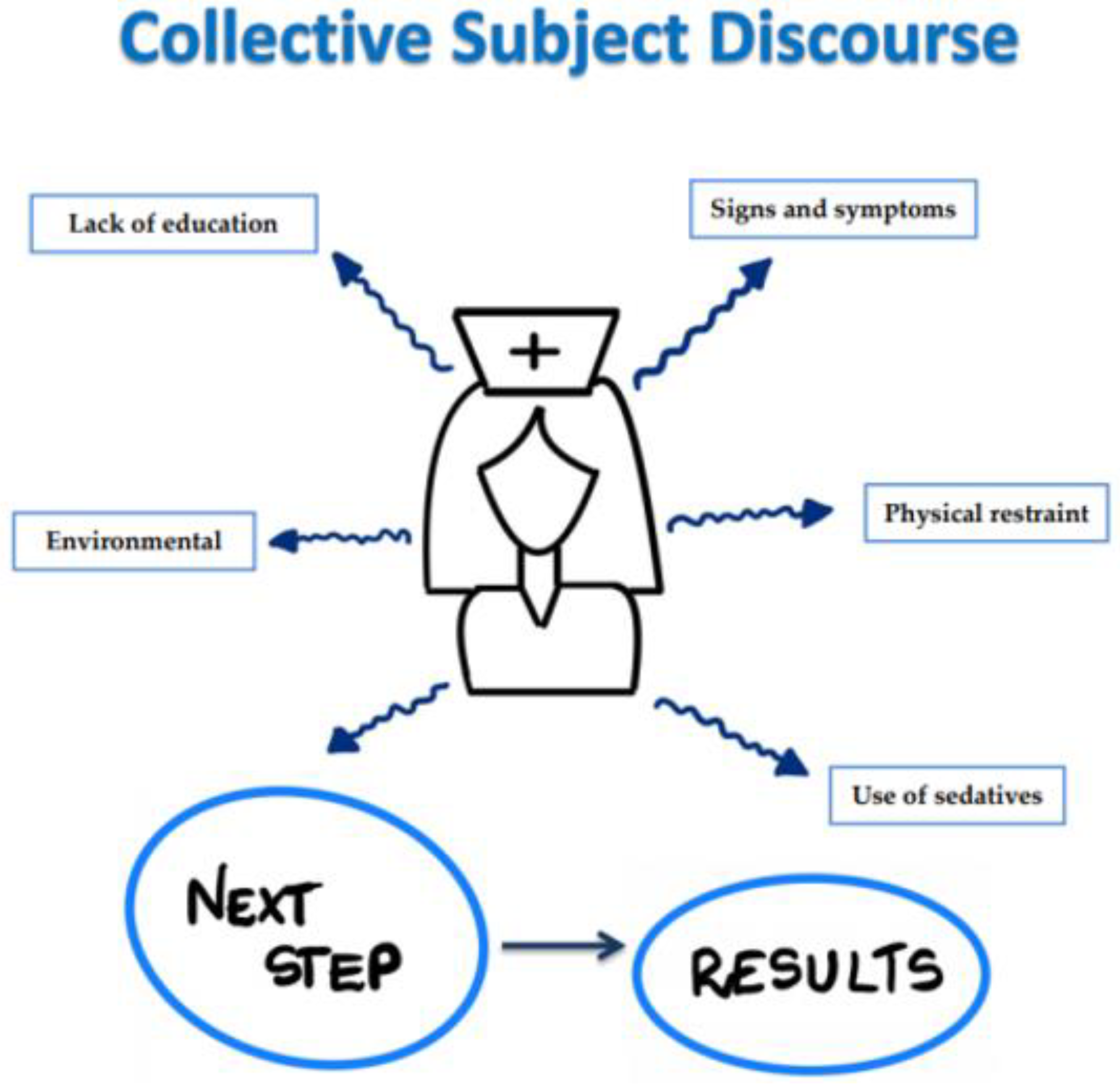
3.1.1. CSD 1. Signs and Symptoms
3.1.2. CSD 2. Physical Restraint
3.1.3. CSD 3. Use of Sedatives
3.1.4. CSD 4. Environmental
3.1.5. CSD 5. Lack of Education
3.2. Second Round
3.2.1. CSD 1. Signs and Symptoms
3.2.2. CSD 2. Physical Restraint
3.2.3. CSD 3. Use of Sedatives
3.2.4. CSD 4. Environmental
3.2.5. CSD 5. Lack of Education
4. Discussion
5. Study Limitations
6. Conclusions
7. Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed, Revision; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Carvalho, J.P.; Almeida, A.R.; Gusmao-Flores, D. Escalas de avaliação de delirium em pacientes graves: Revisão sistemática da literatura. Rev. Bras. Ter Intensiva 2013, 25, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Krupa, S.; Ozga, D. Review of the Literature on the Occurrence of Delirium after Veno-Venous and Veno-Arterial Extracorporeal Membrane Oxygenation: A Systematic Review. Dement Geriatr. Cogn. Dis. Extra 2019, 9, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Hickin, S.L.; White, S.; Knopp-Sihota, J. Nurses’ knowledge and perception of delirium screening and assessment in the intensive care unit: Long-term effectiveness of an education-based knowledge translation intervention. Intensive Crit. Care Nurs. 2017, 41, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Oliveria, P.F.P.; Marchiori, M.; Pacagnan, M.N. Contributions of the Collective Subject Discourse Methodology (CSD) for the Strategy Research as Practice. REBRAE 2015, 8, 37–52. [Google Scholar] [CrossRef]
- Delirum. Available online: https://ptpaio.pl/dokumenty/96.pdf (accessed on 29 December 2021).
- Voyer, P.; Richard, S.; McCusker, J.; Cole, M.G.; Monette, J.; Champoux, N.; Ciampi, A.; Belzile, E. Detection of delirium and its symptoms by nurses working in a long term care facility. J. Am. Med. Dir. Assoc. 2012, 13, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Salluh, J.I.F.; Pandharipande, P. Prevenção do delirium em pacientes críticos: Um recomeço? Rev. Bras. Ter. Intensiva 2012, 24, 1–3. [Google Scholar] [CrossRef]
- Ribeiro, S.C.L.; Nascimento, E.R.P.; Lazzari, D.D.; Jung, W.; Boes, A.A.; Bertoncello, K. Cilene. Knowledge of nurses about delirium in critical patients: Collective subject discourse. Texto Contexto Enferm. 2015, 24, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Bourne, R.S. Delirium and use of sedation agents in intensive care. Nurs. Crit. Care 2008, 13, 195–202. [Google Scholar] [CrossRef]
- Svenningsen, H.; Tonnesen, E. Delirium incidents in three Danish intensive care units. Nurs. Crit. Care 2011, 16, 186–192. [Google Scholar] [CrossRef]
- Alexander, E. Delirium in the intensive care unit: Medications as risk factors. Crit. Care Nurse 2009, 29, 85–87. [Google Scholar] [CrossRef]
- Lewandowska, K.; Weisbrot, M.; Cieloszyk, A.; Mędrzycka-Dąbrowska, W.; Krupa, S.; Ozga, D. Impact of Alarm Fatigue on the Work of Nurses in an Intensive Care Environment—A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8409. [Google Scholar] [CrossRef]
- Macedo, I.S.C.; Mateus, D.C.; Costa, E.M.G.C.; Asprino, A.C.F.; Lourenço, E.A. Avaliação do ruído em unidades de terapia intensiva. Braz. J. Otorhinolaryngol. 2009, 75, 844–846. [Google Scholar] [CrossRef]
- Silva, C.L.; Firmino, J.S.; Knopfholz, J.; Roznowski, K.C. Delirium: Emergência clínica de difícil diagnóstico e os cuidados de enfermagem aos pacientes. Publ. UEPG Ci. Biol. Saúde 2011, 17, 91–97. [Google Scholar] [CrossRef]
- Devlin, J.W.; Fong, J.J.; Howard, E.P.; Skrobik, Y.; McCoy, N.; Yasuda, C.; Marshall, J. Assessment of delirium in the intensive care unit: Nursing practices and perceptions. Am. J. Crit. Care 2008, 17, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Forsgren, L.M.; Eriksson, M. Delirium—Awareness, observation and interventions in intensive care units: A national survey of Swedish ICU head nurses. Intensive Crit. Care Nurs. 2010, 26, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Faria, R.S.B.; Moreno, R.P. Delirium na unidade de terapia intensiva. In Delirium: Uma Síndrome Mental Orgânica; Editora Atheneu: São Paulo, Brazil, 2013; Volume 25, pp. 137–147. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Fisher, J.; Wand, A.P.F.; Milisen, K.; Detroyer, E.; Sockalingam, S.; Agar, M.; Hosie, A.; Teodorczuk, A. Developing delirium best practice: A systematic review of education interventions for healthcare professionals working in inpatient settings. Eur. Geriatr. Med. 2020, 11, 1–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Velthuijsen, E.L.; Zwakhalen, S.M.G.; Warnier, R.M.J.; Ambergen, T.; Mulder, W.J.; Verhey, F.R.J.; Kempen, G.I.J.M. Can education improve clinical practice concerning delirium in older hospitalised patients? Results of a pre-test post-test study on an educational intervention for nursing staff. BMC Med. Educ. 2018, 18, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krupa, S.; Friganović, A.; Oomen, B.; Benko, S.; Mędrzycka-Dąbrowska, W. Nurses’ Knowledge about Delirium in the Group of Intensive Care Units Patients. Int. J. Environ. Res. Public Health 2022, 19, 2758. https://doi.org/10.3390/ijerph19052758
Krupa S, Friganović A, Oomen B, Benko S, Mędrzycka-Dąbrowska W. Nurses’ Knowledge about Delirium in the Group of Intensive Care Units Patients. International Journal of Environmental Research and Public Health. 2022; 19(5):2758. https://doi.org/10.3390/ijerph19052758
Chicago/Turabian StyleKrupa, Sabina, Adriano Friganović, Ber Oomen, Snježana Benko, and Wioletta Mędrzycka-Dąbrowska. 2022. "Nurses’ Knowledge about Delirium in the Group of Intensive Care Units Patients" International Journal of Environmental Research and Public Health 19, no. 5: 2758. https://doi.org/10.3390/ijerph19052758
APA StyleKrupa, S., Friganović, A., Oomen, B., Benko, S., & Mędrzycka-Dąbrowska, W. (2022). Nurses’ Knowledge about Delirium in the Group of Intensive Care Units Patients. International Journal of Environmental Research and Public Health, 19(5), 2758. https://doi.org/10.3390/ijerph19052758