
Evaluation of Sociodemographic Factors and Prevalence of Oral Lesions in People Living with HIV from Cacoal, Rondônia, Amazon Region of Brazil

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
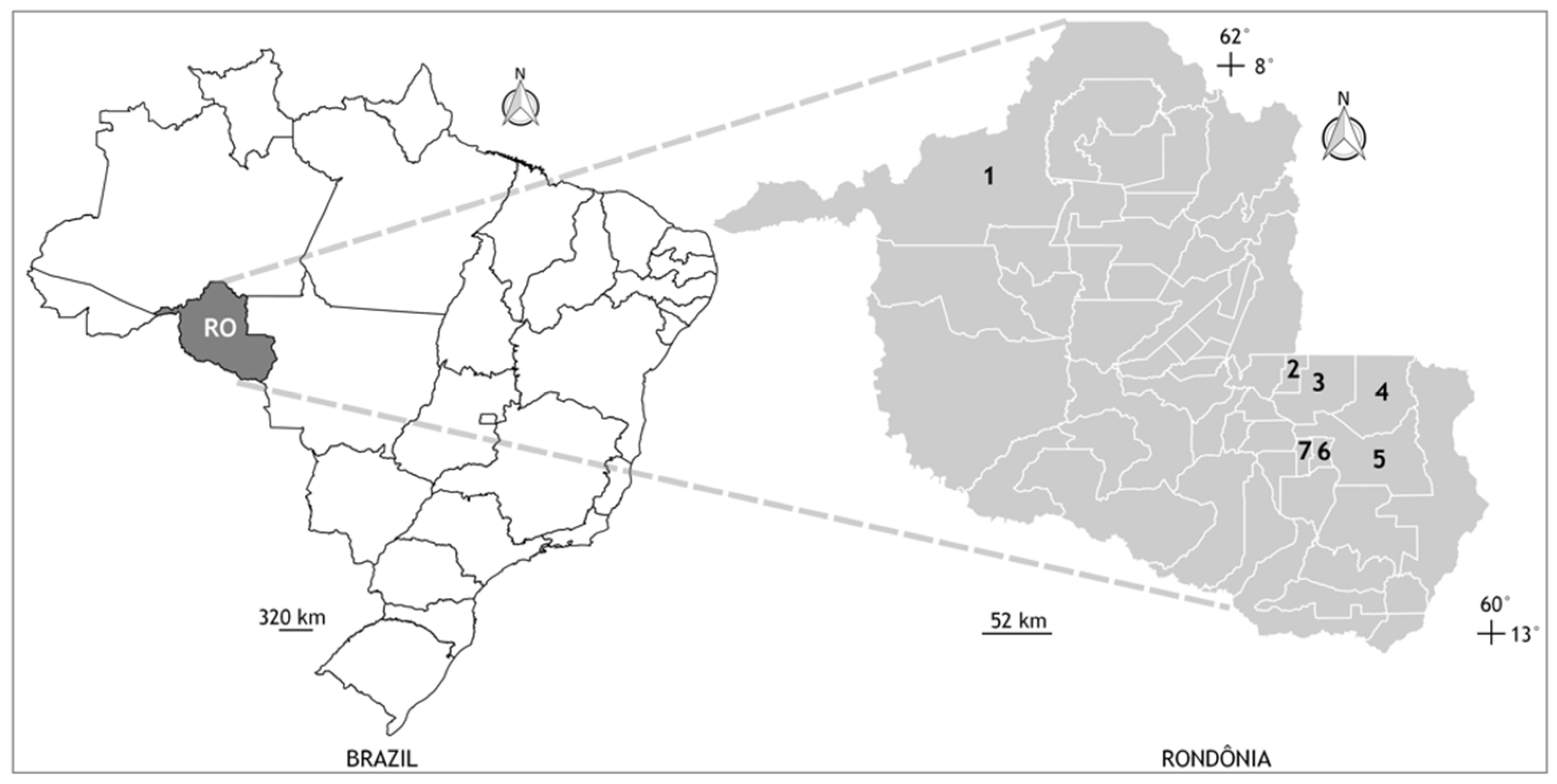
2.1. Study Design and Area Knowledge
2.2. Ethics
2.3. Clinical Parameters
2.4. Collection of Samples and Personal Data
2.5. Statistical Analysis
3. Results
3.1. Sample
3.2. Social, Behavioral and Health Characteristics of PLWH
3.3. Oral Manifestations Prevalence
3.4. Quantification of LTCD4+ and HIV-1 Plasmatic Viral Load
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crabtree-Ramírez, B.; Belaunzarán-Zamudio, P.F.; Cortes, C.P.; Morales, M.; Sued, O.; Sierra-Madero, J.; Cahn, P.; Pozniak, A.; Grinsztejn, B. The HIV epidemic in Latin America: A time to reflect on the history of success and the challenges ahead. J. Int. AIDS Soc. 2020, 23, e25468. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Report on New HIV Infections Rose More than 20% in Latin America in the Last Decade; Pan American Health Organization (PAHO): Washington, DC, USA, 2020; Available online: https://unaids.org.br/2020/12/opas-e-unaids-lancam-campanha-para-promover-o-autoteste-de-hiv-em-tempos-de-covid-19/ (accessed on 28 May 2021).
- Brazilian Ministry of Health-Health Surveillance Secretary. Boletim Annual HIV/AIDS Epidemiological Bulletin; Brazilian Ministry of Health-Health Surveillance Secretary: Rio de Janeiro, Brazil, 2020. Available online: http://www.aids.gov.br/pt-br/pub/2020/boletim-epidemiologico-hivaids-2020 (accessed on 28 May 2021).
- Pedreira, E.N.; Cardoso, C.L.; Barroso, E.C.; Santos, J.A.; Fonseca, F.P.; Taveira, L.A. Epidemiological and oral manifestations of HIV-positive patients in a specialized service in Brazil. J. Appl. Oral Sci. 2008, 16, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Menezes, T.O.; Rodrigues, M.C.; Nogueira, B.M.; Menezes, S.A.; Silva, S.H.; Vallinoto, A.C. Oral and systemic manifestations in HIV-1 patients. Rev. Soc. Bras. Med. Trop. 2015, 48, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Patton, L.L.; Webster-Cyriaque, J.Y.; Greenspan, D.; Traboulsi, R.S.; Ghannoum, M.; Jurevic, R.; Phelan, J.A.; Reznik, D.; Greenspan, J.S.; et al. The Oral HIV/AIDS Research Alliance: Updated case definitions of oral disease endpoints. J. Oral Pathol. Med. 2009, 38, 481–488. [Google Scholar] [CrossRef]
- Araújo, J.F.; Oliveira, A.E.F.; Carvalho, H.L.C.C.; Roma, F.R.V.O.; Lopes, F.F. Most common oral manifestations in pediatric patients HIV positive and the effect of highly active antiretroviral therapy. Cienc. Saude Coletiva 2018, 23, 115–122. [Google Scholar] [CrossRef]
- Souza, A.J.; Gomes-Filho, I.S.; Silva, C.A.L.D.; Passos-Soares, J.S.; Cruz, S.S.D.; Trindade, S.C.; Figueiredo, A.C.M.G.; Buischi, Y.d.P.; Seymour, G.J.; de Moraes Marcílio Cerqueira, E. Factors associated with dental caries, periodontitis and intra-oral lesions in individuals with HIV/AIDS. AIDS Care 2018, 30, 578–585. [Google Scholar] [CrossRef]
- Vohra, P.; Jamatia, K.; Subhada, B.; Tiwari, R.V.C.; Althaf, M.N.; Jain, C. Correlation of CD4 counts with oral and systemic manifestations in HIV patients. J. Fam. Med. Prim. Care 2019, 31, 3247–3252. [Google Scholar] [CrossRef]
- Ratnam, M.; Nayyar, A.S.; Reddy, D.S.; Ruparani, B.; Chalapathi, K.V.; Azmi, S.M. CD4 cell counts and oral manifestations in HIV infected and AIDS patients. J. Oral Maxillofac. Pathol. 2018, 22, 282. [Google Scholar]
- Patton, L.L.; Phelan, J.A.; Ramos-Gomez, F.J.; Nittayananta, W.; Shiboski, C.H.; Mbuguye, T.L. Prevalence and classification of HIV-associated oral lesions. Oral Dis. 2002, 8, 98–109. [Google Scholar] [CrossRef]
- Mary, E.O.; Abiola, O.A.; Titilola, G.; Mojirayo, O.O.; Sulaimon, A.A. Prevalence of HIV related oral lesions in people living with HIV and on combined antiretroviral therapy: A Nigerian experience. Pan Afr. Med. J. 2018, 31, 180. [Google Scholar] [CrossRef]
- Ottria, L.; Lauritano, D.; Oberti, L.; Candotto, V.; Cura, F.; Tagliabue, A.; Tettamanti, L. Prevalence of HIV-related oral manifestations and their association with HAART and CD4+ T cell count: A review. J. Biol. Regul. Homeost. Agents 2018, 32, 51–59. [Google Scholar]
- Lourenço, A.G.; Ribeiro, A.E.R.A.; Nakao, C.; Motta, A.C.F.; Antonio, L.G.L.; Machado, A.A. Oral Candida spp carriage and periodontal diseases in HIV-infected patients in Ribeirao Preto, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e29. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, A.; Marcenes, W.; Zakrzewska, J.M.; Robinson, P.G. Dental and oral lesions in HIV infected patients: A study in Brazil. Int. Dent. J. 2004, 54, 131–137. [Google Scholar] [CrossRef]
- Indrastiti, R.K.; Wardhany, I.I.; Soegyanto, A.I. Oral manifestations of HIV: Can they be an indicator of disease severity? (A systematic review). Oral Dis. 2020, 26, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Patton, L.L.; Ranganathan, K.; Naidoo, S.; Bhayat, A.; Balasundaram, S.; Adeyemi, O.; Taiwo, O.; Speicher, D.J.; Chandra, L. Oral lesions, HIV phenotypes, and management of HIV-related disease: Workshop 4A. Adv. Dent. Res. 2011, 23, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Blignaut, E.; Patton, L.L.; Nittayananta, W.; Ramirez-Amador, V.; Ranganathan, K.; Chattopadhyay, A. (A3) HIV Phenotypes, oral lesions, and management of HIV-related disease. Adv. Dent. Res. 2006, 19, 122–129. [Google Scholar] [CrossRef]
- Tappuni, A.R. The global changing pattern of the oral manifestations of HIV. Oral Dis. 2020, 26, 22–27. [Google Scholar] [CrossRef]
- El Howati, A.; Tappuni, A. Systematic review of the changing pattern of the oral manifestations of HIV. J. Investig. Clin. Dent. 2018, 9, e12351. [Google Scholar] [CrossRef]
- Heron, S.E.; Elahi, S. HIV Infection and Compromised Mucosal Immunity: Oral Manifestations and Systemic Inflammation. Front. Immunol. 2017, 8, 241. [Google Scholar] [CrossRef]
- Bodhade, A.S.; Ganvir, S.M.; Hazarey, V.K. Oral manifestations of HIV infection and their correlation with CD4 count. J. Oral Sci. 2011, 53, 203–211. [Google Scholar] [CrossRef][Green Version]
- Gliosca, L.A.; Eramo, L.R.; Bozza, F.L.; Soken, L.; Abusamra, L.; Salgado, P.A.; Squassi, A.F.; Molgatini, S.L. Microbiological study of the subgingival biofilm in HIV+/HAART patients at a specialized dental service. Acta Odontol. Latinoam. 2019, 32, 147–155. [Google Scholar] [PubMed]
- Vidal, F.; Peres, R.V.; de Souza, R.C.; Gonçalves, C.; Pavan, P.; Gonçalves, L.S. Dental implants in individuals living with HIV-1: Results from a prospective study in patients undergoing highly active antiretroviral therapy. Spec. Care Dent. 2021, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Perla, N.; Kumar, S.; Jadhav, A.; Bhalinge, P.; Dadpe, M.; Acharya, S. Quantification of Oral Candidal Carriage Rate and Prevalence of Oral Candidal Species in HIV Patients with and Without Highly Active Antiretroviral Therapy. J. Microsc. Ultrastruct. 2021, 9, 145–153. [Google Scholar]
- Rajnay, Z.W.; Hochstetter, R.L. Immediate placement of an endosseous root-form implant in an HIV-positive patient: Report of a case. J. Periodontol. 1998, 69, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.F.; Capparé, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. Implant Prosthetic Rehabilitation in Controlled HIV-Positive Patients: A Prospective Longitudinal Study with 1-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2016, 18, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Capparé, P.; Teté, G.; Romanos, G.E.; Nagni, M.; Sannino, G.; Gherlone, E.F. The ‘All-on-four’ protocol in HIV-positive patients: A prospective, longitudinal 7-year clinical study. Int. J. Oral Implantol. 2019, 12, 501–510. [Google Scholar]


{kind=link}
| Parameters | HIV | |
|---|---|---|
| n | % | |
| Age (Years) | ||
| 4–20 | 4 | 3.5 |
| 20–36 | 36 | 31.9 |
| 36–52 | 53 | 46.9 |
| 52–68 | 16 | 14.2 |
| 68–84 | 4 | 3.5 |
| Gender | ||
| Male | 54 | 47.8 |
| Female | 59 | 52.2 |
| Colour/race (self-identified) | ||
| White | 52 | 46 |
| Black | 52 | 46 |
| Pardo (mixed race) | 8 | 7.1 |
| Indigenous | 1 | 0.9 |
| Marital status * | ||
| Single | 37 | 32.7 |
| Married | 52 | 46 |
| Separated | 10 | 8.8 |
| Widowed | 6 | 5.3 |
| Not informed | 8 | 7.1 |
| Monthly income (Brazilian minimum wage) * | ||
| Up to one wage | 14 | 12.4 |
| 1–3 wages | 66 | 58.4 |
| 4–6 wages | 15 | 13.3 |
| 7–11 wages | 3 | 2.6 |
| Not informed | 15 | 13.3 |
| Sexual orientation | ||
| Homosexual | 12 | 10.7 |
| Heterosexual | 95 | 84.1 |
| Bisexual | 3 | 2.6 |
| Not informed | 3 | 2.6 |
| Source | ||
| Capital city | 96 | 85 |
| Countryside | 17 | 15 |
| Length of education * | ||
| No formal education (including illiterates) | 43 | 38 |
| Up to elementary school | 27 | 23.9 |
| Up to high school | 29 | 25.7 |
| College graduation | 8 | 7.1 |
| Not informed | 6 | 5.3 |
| Condom use ** | ||
| Rarely | 7 | 6.2 |
| Never | 18 | 15.9 |
| Sometimes | 52 | 46 |
| Always | 36 | 31.9 |
| Number of sexual partners ** | ||
| 0–1 | 56 | 49.6 |
| 2–5 | 46 | 40.7 |
| Up to 5 | 11 | 9.7 |
| STI History | ||
| Yes | 38 | 33.7 |
| No | 75 | 66.3 |
| Illicit drug use ** | ||
| Yes | 59 | 52.3 |
| No | 54 | 47.7 |
| Alcohol use ** | ||
| Yes | 38 | 33.7 |
| No | 75 | 66.3 |
| Tobacco use ** | ||
| Yes | 50 | 44.2 |
| No | 63 | 55.7 |
| ART use * | ||
| Yes | 90 | 79.6 |
| No | 23 | 20.4 |
| Tattoos | ||
| Yes | 24 | 21.2 |
| No | 89 | 78.8 |
| Parameters | Oral Lesion Types (n/%) | |||||
|---|---|---|---|---|---|---|
| Fungal Infections | Viral Infections | Idiopathic Conditions | Bacterial Infections | Salivary Gland Diseases | Neoplasms | |
| Anatomic region | ||||||
| Maxilla | - | 2 (12.5%) ‡ | - | 1 (50%) ¶ | - | - |
| Mandible | - | 3 (18.75%) ‡ | - | 1 (50%) # | - | - |
| Tongue | 4 (57.1%) * | 4 (25%) † | 1 (14.3%) ** | - | - | - |
| Lips and buccal mucosa | 3 (42.9%) * | 5 (31.25%) ¥ | 6 (85.7%) ** | - | - | - |
| Oropharynx | - | 2 (12.5%) † | - | - | - | - |
| Salivary glands | - | - | - | - | - | - |
| Parameters | Oral Manifestations | |||||
|---|---|---|---|---|---|---|
| Yes | No | p | ||||
| n | % | n | % | |||
| Gender | ||||||
| Female | 13 | 40.6 | 46 | 56.8 | 0.122 | |
| Male | 19 | 59.4 | 35 | 43.2 | ||
| Total | 32 | 100.0 | 81 | 100.0 | ||
| Age | ||||||
| 4–20 | 3 | 9.4 | 1 | 1.2 | 0.024 | |
| 20–36 | 6 | 18.8 | 35 | 43.2 | ||
| 36–52 | 16 | 50.0 | 32 | 39.5 | ||
| 52–68 | 7 | 21.9 | 10 | 12.3 | ||
| 68–84 | 0 | 0.0 | 3 | 3.7 | ||
| Total | 32 | 100.0 | 81 | 100.0 | ||
| Sexual orientation | ||||||
| Homosexual | 0 | 0 | 3 | 3.7 | 0.298 | |
| Heterosexual | 25 | 78.1 | 70 | 86.4 | ||
| Bisexual | 5 | 15.6 | 7 | 8.6 | ||
| Not informed | 2 | 6.3 | 1 | 1.2 | ||
| Total | 32 | 100.0 | 81 | 100.0 | ||
| Condom use | ||||||
| Rarely | 4 | 12.5 | 3 | 3.7 | 0.347 | |
| Never | 4 | 12.5 | 14 | 17.3 | ||
| Sometimes | 17 | 53.1 | 35 | 43.2 | ||
| Always | 7 | 21.9 | 29 | 35.8 | ||
| Total | 32 | 100.0 | 81 | 100.0 | ||
| Number of sexual partners | ||||||
| 0–1 | 16 | 50 | 40 | 49.4 | 0.853 | |
| 2–5 | 13 | 40.6 | 33 | 40.7 | ||
| Up to 5 | 3 | 9.4 | 8 | 9.9 | ||
| Total | 32 | 100.0 | 81 | 100.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Rocha, G.d.C.T.; Fonseca, R.R.d.S.; Oliveira-Filho, A.B.; Ribeiro, A.L.R.; de Menezes, S.A.F.; Laurentino, R.V.; Machado, L.F.A. Evaluation of Sociodemographic Factors and Prevalence of Oral Lesions in People Living with HIV from Cacoal, Rondônia, Amazon Region of Brazil. Int. J. Environ. Res. Public Health 2022, 19, 2614. https://doi.org/10.3390/ijerph19052614
da Rocha GdCT, Fonseca RRdS, Oliveira-Filho AB, Ribeiro ALR, de Menezes SAF, Laurentino RV, Machado LFA. Evaluation of Sociodemographic Factors and Prevalence of Oral Lesions in People Living with HIV from Cacoal, Rondônia, Amazon Region of Brazil. International Journal of Environmental Research and Public Health. 2022; 19(5):2614. https://doi.org/10.3390/ijerph19052614
Chicago/Turabian Styleda Rocha, Graziela de Carvalho Tavares, Ricardo Roberto de Souza Fonseca, Aldemir Branco Oliveira-Filho, Andre Luis Ribeiro Ribeiro, Silvio Augusto Fernandes de Menezes, Rogério Valois Laurentino, and Luiz Fernando Almeida Machado. 2022. "Evaluation of Sociodemographic Factors and Prevalence of Oral Lesions in People Living with HIV from Cacoal, Rondônia, Amazon Region of Brazil" International Journal of Environmental Research and Public Health 19, no. 5: 2614. https://doi.org/10.3390/ijerph19052614
APA Styleda Rocha, G. d. C. T., Fonseca, R. R. d. S., Oliveira-Filho, A. B., Ribeiro, A. L. R., de Menezes, S. A. F., Laurentino, R. V., & Machado, L. F. A. (2022). Evaluation of Sociodemographic Factors and Prevalence of Oral Lesions in People Living with HIV from Cacoal, Rondônia, Amazon Region of Brazil. International Journal of Environmental Research and Public Health, 19(5), 2614. https://doi.org/10.3390/ijerph19052614